
Abstract
Introduction:
Gestational diabetes mellitus (GDM) is defined as glucose intolerance first recognized during pregnancy. Insertion/deletion (I/D) polymorphism of a 287 bp Alu repetitive sequence in intron 16 of the angiotensin-converting enzyme (ACE) gene has been widely investigated in Asian Indian populations with different ethnic origins. The present study examined possible association between I/D polymorphism of the ACE gene and GDM in Asian Indian pregnant women.
Methods:
A total of 200 pregnant women (100 GDM and 100 non-GDM) were recruited in this study and I/D polymorphism of a 287 bp Alu1 element inside intron 16 of the ACE gene was examined by polymerase chain reaction (PCR)-based gel electrophoresis.
Result:
The distribution of the variants like II, ID, and DD genotypes of ACE gene showed differences between normal GDM versus non-GDM subjects, and the frequency of the ID+ DD Vs II genotype was significant (p=0.0002) in the GDM group.
Conclusion:
ACE gene polymorphism was associated with GDM in Asian Indian pregnant women.
Keywords
Introduction
Gestational diabetes mellitus (GDM), defined as any glucose intolerance detected during pregnancy, has evolved into clinical conditions associated with higher risks for maternal and perinatal morbidity. 1 Epidemiological studies have confirmed that GDM is associated with increased feto-maternal morbidity and long-term complications in mothers and offspring. However, the pathogenesis of GDM is still largely unknown. Given the fact that women with a history of GDM are at an increased risk of developing type 2 diabetes mellitus (T2DM) later in their lives, women with a family history of diabetes may be predisposed to an increased risk of GDM and may polymorphism refers to the presence or absence share the same risk factors and genetic susceptibilities with T2DM. It has been reported that the pathophysiological changes of GDM are similar to those observed in T2DM, which are characterized by peripheral insulin resistance accompanied by an insulin secretory defect.1,2
Angiotensin-converting enzyme (ACE) plays an important role in the renin-angiotensin system (RAS) cascade by converting angiotensin I to angiotensin II. There are studies suggesting ACE polymorphism may be involved in the etiology of renal disease in T2DM. The ACE gene insertion/ deletion (I/D) polymorphism refers to the presence or absence of Alu Sequence i.e. 287 base pair sequence in intron16. 3 The goal of the present study was to scrutinize the relationship of ACE I/D gene polymorphism with GDM in Asian Indian women.
Materials and methodology
The present study was carried out on 200 pregnant women: 100 women had developed GDM during pregnancy and 100 women had normal glucose levels during pregnancy. Blood samples of 2 mL were collected from the pregnant women in Ethylene Diamine Tetra Acetic acid (EDTA) tubes. The study protocol was approved by the institutional ethical committee. All selected GDM women had a 60% family history of T2DM. Screening and management of diabetes during pregnancy were done by a qualified physician according to the American Diabetes Association (ADA) guidelines. 4 Women with type 1 diabetes mellitus (T1DM), T2DM or any other diabetes diagnosed before the pregnancy were excluded.
Glucose and diagnostic criteria for GDM
GDM cases were identified after a glucose challenge test (GCT) between 24th–28th week of gestation, 50 g of glucose was given to pregnant women fasting plasma glucose value exceeded 130 mg/dL otherwise standard the oral glucose tolerance test (OGTT) was performed using 100 g of glucose for women after overnight fasting and three days of unrestricted diet. Fasting plasma samples were drawn after 1, 2 and 3 h of administration of glucose. In this study GDM cases were those which showed two or more glucose values that met or exceeded the threshold values as shown in Table 1. 5
Diagnosis of GDM with a 100g oral glucose load.

Determination of ACE I/D polymorphism
Genomic DNA was extracted from EDTA-blood samples using the salting out technique 6 . The ACE I/D gene was analyzed using polymerase chain reaction (PCR) and primers specified by Movva et al. 6 The sequences of the primers were chosen such that they flank the targeted region of the genome on the intron 16 of ACE gene (17q23). The template DNA (0.5 µL) was amplified by following primers: (forward) 5’-CTG GAG ACC ACT CCC ATC CTT TCT 3’, and (reverse) 5’-GAT GTG GCC ATC ACA TTC GTC AGA T 3’. PCR products (190 bp for deletion or 490 bp with 287 bp Alu insertion) were detected by electrophoresis on agarose gel containing ethidium bromide (Figure 1). The PCR profile consisted of 35 cycles denaturation (at 94 °C for 5 min), annealing (at 58 °C for 30 s) and extension at (72 °C for 5 min). Presence or absent from 490 bp and 190 bp fragments were monitored by an ultraviolet transilluminator.
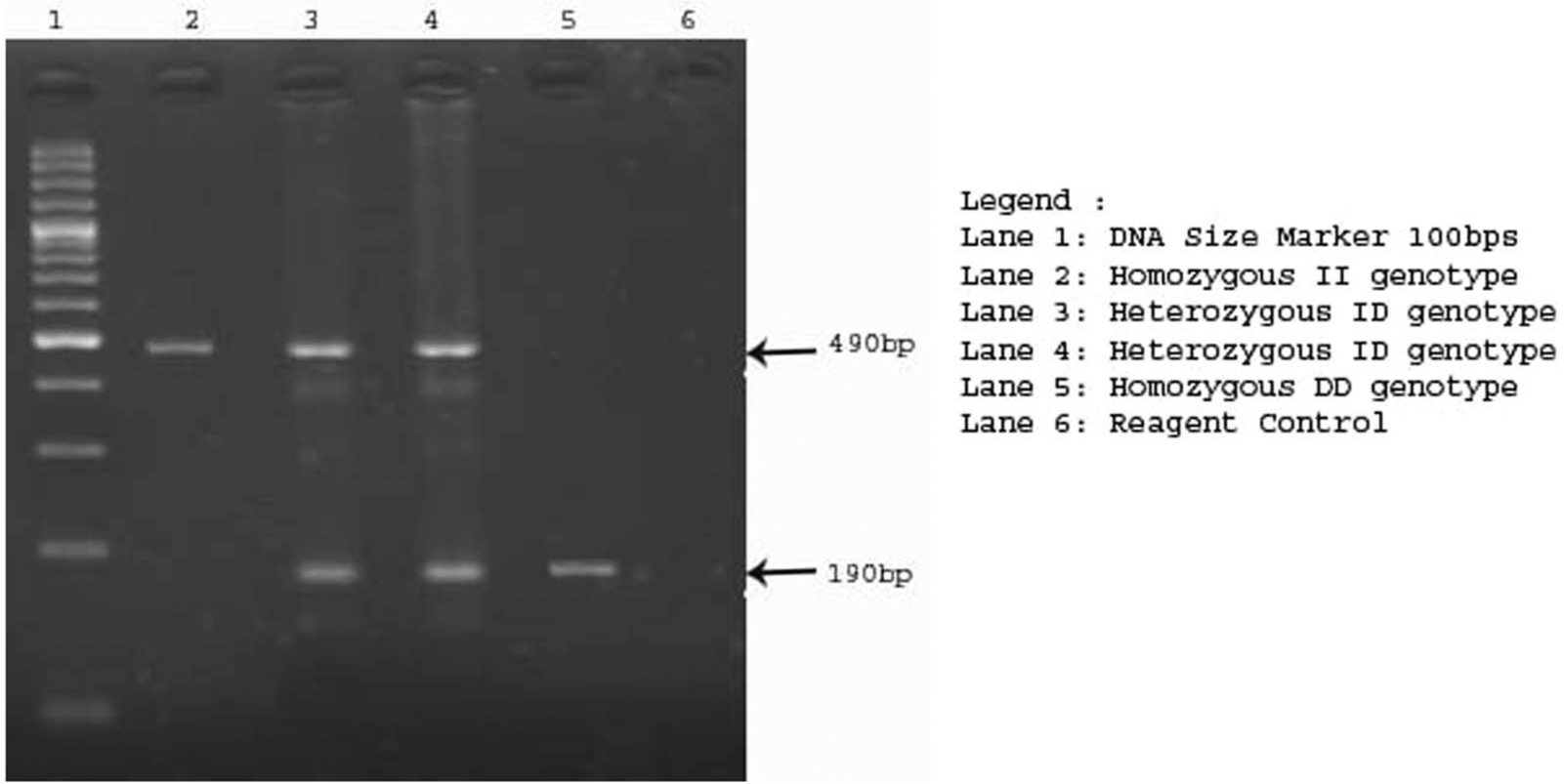
Electrophoresis on agarose gel and polymerase chain reaction (PCR) products. Illustrative 3% agarose gel picture of ACE gene I/D polymorphism.
Statistical analysis
Data are presented as mean±standard deviation (SD). Chi-square test was used for the comparison of expected and observed frequencies of categorical variables. A value of p < 0.05 (two-tailed) was considered statistically significant. The odds ratio (OR) was calculated. Statistical analysis was performed using SPSS, version 19.0 (Chicago, USA). The t-test was also performed with SPSS software.
Result
The clinical characteristics of GDM cases and non-GDM subjects are given in Table 2. GDM cases (n=100) had an age range of 22–38 years, 31% of them were primigravida, thus 69% were multigravida. The pre-pregnancy body mass index (BMI) range of the GDM cases was 19.8–35.6 kg/m2 with a mean±SD of 27.08±3.93 kg/m2 versus 19–31.1 kg/m2 for control women with a mean±SD of 24.10±3.55 kg/m2 (p = 0.31). Fasting Blood Sugar (FBS) values were not significantly different (p = 0.13) between the GDM cases andnon-GDM subjects. However, 41% of individuals managed diabetes with appropriate diet and exercise, while 59% of the patients required 4–8 units of insulin for the entire antenatal period.
Clinical details of gestational diabetes mellitus (GDM) cases and non-GDM involved in the study.

BMI: body mass index; NA: not analyzed/ not applicable.
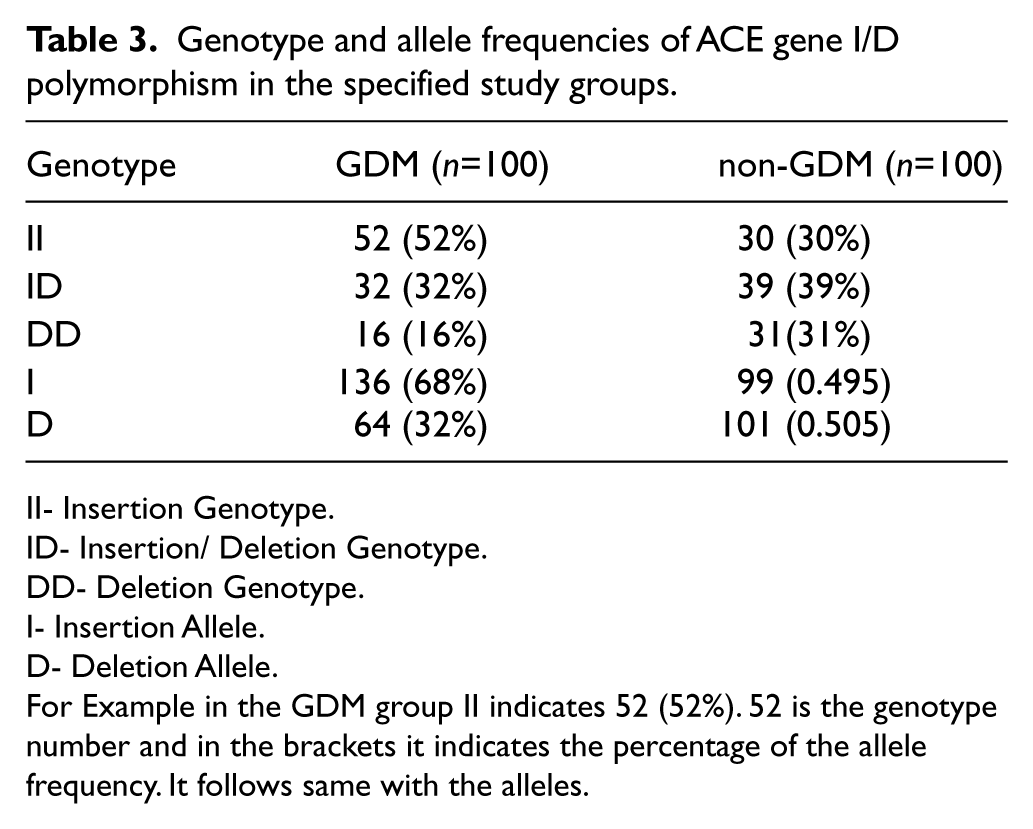
The genotype frequency for ACE I/D polymorphism differed significantly between the GDM and non-GDM (Tables 3 and 4). The frequencies of DD, ID and II genotypes among GDM patients were 16%, 32% and 52% respectively, versus 30%, 39% and 31% for the non-GDM subjects, respectively. The ID+DD Vs II genotype appeared to be strong association (OR-2.979; 95%CI = 1.784-4.975; p = 0.0002) with GDM.
Genotype and allele frequencies of ACE gene I/D polymorphism in the specified study groups.
II- Insertion Genotype.
ID- Insertion/ Deletion Genotype.
DD- Deletion Genotype.
I- Insertion Allele.
D- Deletion Allele.
For Example in the GDM group II indicates 52 (52%). 52 is the genotype number and in the brackets it indicates the percentage of the allele frequency. It follows same with the alleles.
Statistical Analysis of ACE genotypes and alleles in the specified groups.

The genotypes distributions of GDM patients were in Hardy-Weinberg equilibrium. Table 5 shows clinical data versus genotype for GDM patients. Women of ID genotype were older, lighter in weight and had a higher FBS than the other two genotypes (67.2±11.23 and 114.76±25.90). The highest Post Prandial Blood Glucose (PPBG) was observed with women of II genotype, 63.4% of whom having the family history and were on insulin treatment more frequently than woman of ID or DD genotypes.
Analysis of the risk in GDM subjects according to the ACE II, ID and DD genotypes.

BMI: body mass index.
Discussion
ACE is a zinc metalloprotease that is widely distributed on the surface of epithelial and endothelial cells. The ACE gene is one of the most intensely studied genes because of the key role it plays in the RAS. An I/D polymorphism in intron 16 of ACE gene, may serve as a suitable marker for studying genetic variation in human populations. 3 Table 6 summarizes previous studies that are related to ACE genotype associations.7 –24
Angiotensin-converting enzyme (ACE) insertion/deletion (I/D) gene polymorphism studies in certain diseases.

In the present study, we investigated the possible association of ACE I/D polymorphisms with the development of GDM among selected individuals from the Asian Indian population. The study was carried out between two groups (GDM cases and non-GDM subjects) and showed significant differences with respect to age, weight and PPBG. The results suggest a possible positive association between ID+DD polymorphism and the development of GDM in women of the Asian Indian population.
Women with GDM had significantly higher frequencies of II genotype (p = 0.002) than non-GDM women. This is the first report to show a significant association between ACE I/D polymorphism and GDM in India. The ACE I/D gene polymorphism has been associated with different diseases (Table 6). There is only a solitary study by Dostalova et al. 9 in which ACE gene polymorphism has been found not to be associated with GDM. During the past decade, there has been a growing interest in the study of the ACE gene I/D polymorphism as a potential risk factor for diabetic retinopathy (DR) after a report that more than half of the plasma ACE variation levels between individuals were under the influence of the I/D polymorphism.25,26 Confirmation of genetic association has been difficult for many reasons. Among widely cited explanations are the multifactorial nature of the diseases, insufficient sample size, and criteria of selection which may lead to false negative results. The interaction between genes and environment makes it difficult to assess the GDM risk of specific individuals since environmental background influences the penetrance of many genes.
GDM, T2DM and its complications are complex diseases; hence the gene polymorphisms individually or in combination will help in identifying those who are at increased risk of T2DM and GDM and ensure thereby a better prognosis for these multifactorial diseases. Most common forms of GDM are believed to be multifactorial and the result of many genes with small individual effects. The identification of these genes and their variation would be very helpful for the prediction, prevention, and management of GDM. Genetic risk scores derived from several functional single nucleotide polymorphisms or haplotypes in multiple genes may improve the prediction of GDM. In early gestation, FBS is lower and insulin sensitivity decreases slightly. This is followed by progressively increasing insulin resistance in the second and third trimesters with a borderline increase of insulin production or hyperinsulinemia. Furthermore, insulin resistance occurs as a result of placental hormones that antagonize insulin, estrogen, progesterone, human placental lactogen, human placental growth hormone, cortisol, prolactin and tumor necrosis factor-alpha. The above different pathophysiologic mechanisms accompanying pregnancy result in metabolic changes that allow for higher postprandial maternal glucose. Ongoing studies will address important gaps in the literature. 27
Conclusions
Our results showed that the ACE I/D gene polymorphism had a role in the development of GDM in Asian Indian women. Given the inherent limitations of case-control studies and the complex nature of genetic susceptibility in chronic degenerative diseases, prospective and interventional clinical studies with larger sample sizes are required in individual ethnic groups to confirm our observations and for the identification of molecular predisposing factors for GDM that may help in the development of new treatments.
Footnotes
Conflicts of interest
The authors declare that there are no conflicts of interest.
Funding
The authors would like to thank the Indian Council for Medical Research for the funding of this work (Sanction no. 5-3-8-39-2007; RHN).