
Abstract
Introduction:
Malfunctioning of the cardiovascular system during pregnancy may be responsible for adverse effects on the ‘mother-fetus’ system. The cardiovascular system of a pregnant woman develops adaptation to the increased load. Angiotensin-converting enzyme (ACE) is known to play an important role in the adaptation. The present study was designed to investigate whether the insertion-deletion (I/D) polymorphism of the ACE gene is associated with the level of arterial blood pressure in women before and during pregnancy.
Materials and methods:
The level of blood pressure was measured in 591 Russian women (Central Russia) before and during (37–40 weeks term) pregnancy. The women were divided into three groups which were hypertensive, hypotensive, and normotensive according to blood pressure level. Genotyping of the ACE I/D polymorphism was performed using polymerase chain reaction (PCR) and amplified fragment length polymorphism assay.
Results:
Women with genotype DD showed the highest blood pressure level both during and at the end of pregnancy (p<0.05). The highest frequencies of allele D and genotype DD were found in pregnant women in the hypertensive group.
Conclusions:
The deletion variant of the ACE gene is associated with high blood pressure level at the end of pregnancy.
Keywords
Introduction
Pregnancy is one of the physiological conditions that requires lengthy and significant restructuring of many systems of an organism to properly maintain homeostasis.1,2 Therefore, studying changes in the functions of the cardiovascular system (CVS) during pregnancy and the factors responsible for these changes, is an important medical challenge. These functional changes may result in an increased load on the cardiovascular system of a woman. 3 Impairments of the cardiovascular system during pregnancy may cause preeclampsia4,5 and, thereby, lead to chronic intrauterine hypoxia and placental failure. 6
The renin-angiotensin-aldosterone system and, in particular, angiotensin-converting enzyme (ACE) is known to play an important regulatory role in the function of the CVS. The enzyme hydrolyses angiotensin I into angiotensin II, a powerful vasoconstrictor. 7 Several polymorphisms of the ACE gene have been studied with respect to the association with CVS functioning under normal and diseased conditions.8–10 One of these polymorphisms is an insertion-deletion (I/D) of the 287-bp Alu repetitive element in intron 16 of the gene. 11 The polymorphism does not affect the protein structure but apparently influences expression of this gene.
Several studies reported that blood ACE levels in healthy individuals with the DD genotype were twice as high as those in the II homozygotes, with the heterozygotes having an intermediate value.11–13 The studies reporting the association of the I/D polymorphism of the ACE gene with the blood pressure (BP) level in pregnant women are contradictory. This prompts further research on the role of the I/D polymorphism of ACE gene in the regulation of BP during pregnancy.
Materials and methods
Study subjects
The study population included 591 unrelated women of Russian descent living in Central Russia (Belgorod region). The age of the women varied from 20–43 years (mean age 27.98±4.50 years). The study was approved by the Regional Ethics Committee at Belgorod State University. All women signed an informed consent form prior to the recruitment for this study.
Clinical and laboratory examinations of women were conducted at the Perinatal Center (Division of Pathological Pregnancy) of the Belgorod Regional Clinical Hospital. The criteria for inclusion in the study group were (a) Russian nationality; (b) pregnancy at 37–40 weeks of gestation; and (с) signed informed consent for the study. Pregnant women with diabetes mellitus, hepatic or renal failure, and those at a gestation <37 weeks and >40 weeks were excluded from the study. A general outline is shown in Figure 1. BP level was measured three times by experienced obstetricians according to the American Heart Association recommendations. 14 The measurements were done in the morning (between 0700–0900 hours) and evening (between 1900–2100 hours). The data on BP level before pregnancy were obtained from the medical records of each woman. The mean arterial pressure (MAP, mm Hg) was calculated as follows:

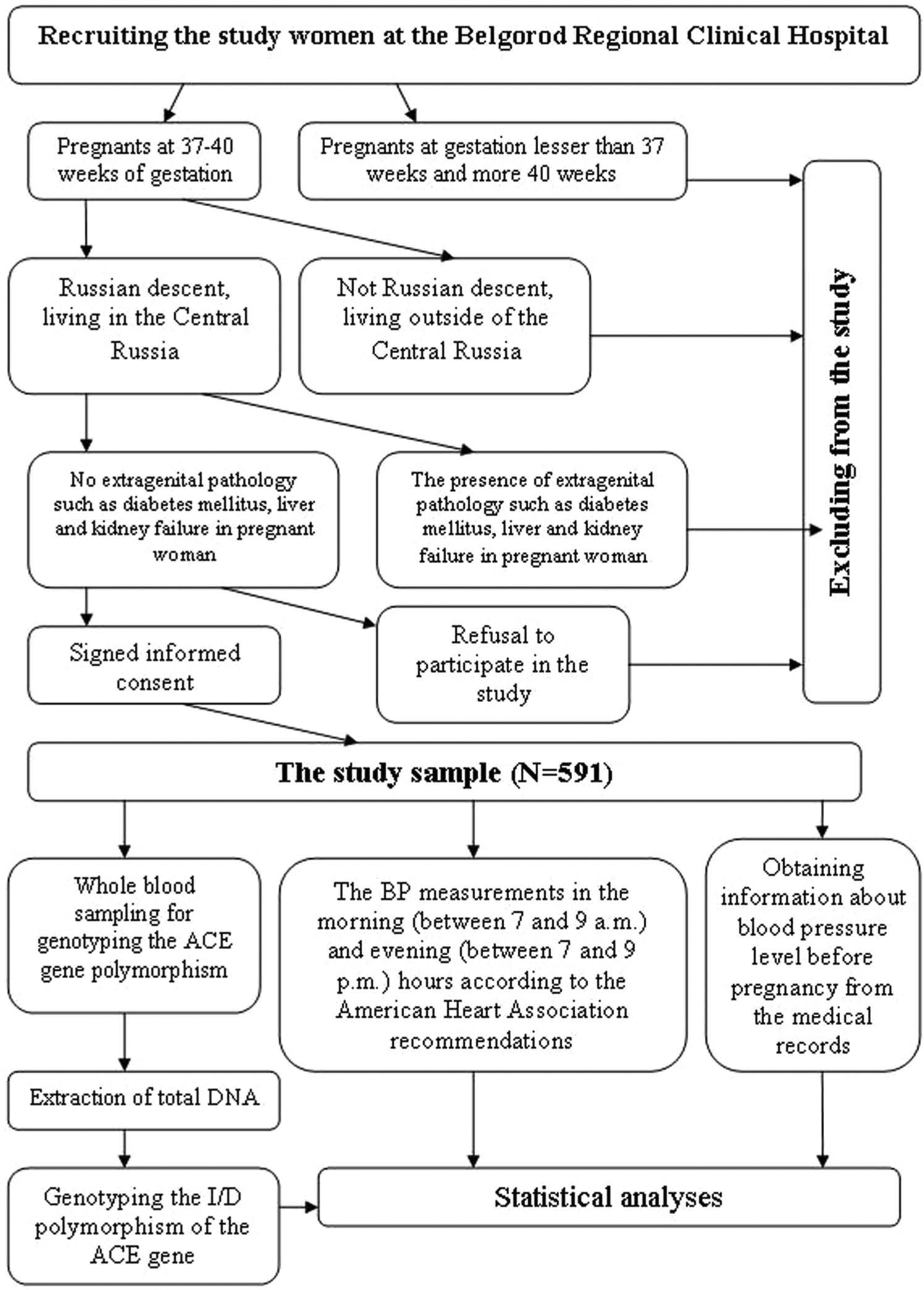
The general outline of the investigation.
All study participants were divided into three groups depending on the BP level at the end of pregnancy. The groups included normotensive women (SBP from 90–140 mm Hg and/or DBP from 60–90 mm Hg), hypotensive women (SBP<90 mm Hg and/or DBP<60 mm Hg), and hypertensive women (SBP>140 mm Hg and/or DBP>90 mm Hg). 16
DNA extraction and genotyping
Venous blood (8–9 ml) was drawn from the ulnar vein of each woman. Genomic DNA was isolated using the method proposed Miller and et al. 17 Genotyping of the insertion-deletion polymorphism (rs4646994) of the ACE gene was performed using a polymerase chain reaction (PCR) and amplified fragment length polymorphism (AFLP) assay according to the protocol described elsewhere. 18
Statistical analysis
Allele frequencies of the ACE gene polymorphism were estimated by the gene counting method, and the chi-squire test was used to identify significant departure from Hardy–Weinberg equilibrium (HWE). The distribution of allele and genotype frequencies between the study groups was compared by the chi-squire test for 2×2 contingency tables. The p-values were adjusted for multiple testing using the Bonferroni correction (pcor). The distribution of the quantitative traits such as SBP, DBP, MAP and pulse pressure (the pressure difference between the systolic and diastolic pressures) before and at the end of pregnancy were analyzed by the Shapiro-Wilk’s test. 19 Because the values of the quantitative traits did not follow the normal distribution, median (Me) and interquartile range (Q25–Q75) were used for their description and intergroup comparisons were done using the Mann-Whitney test. 20 Linear regression analysis was used to estimate the impact of age, weight, and ACE genotypes on the BP parameters in women. All statistical analyses were performed using STATISTICA for Windows v. 6.0 (StatSoft, USA).
Results
The biomedical and clinical characteristics of the study women are shown in Table 1. As can be seen from Table 1, the prevalence of hypertension among women before and at the end of pregnancy was 10.3% and 51.7%, respectively. The prevalence of hypotension dropped from 19.1% prior to pregnancy to 4.1% at the end of pregnancy. Moreover the values of BP increased significantly in women to the end of pregnancy in comparison with women prior to pregnancy. Obesity was found in 20.6% the study women. Moreover 15.1% of women had excessive body weight, whereas 8.1% of women had decreased body weight. The study group also comprised 7.8% of women who had other extragenital pathology.
The biomedical and clinical characteristics of the study women.

BMI: body mass index; DBP: diastolic blood pressure ΔDBP: change of diastolic blood pressure; ΔMAP: change of mean arterial pressure; ΔSBP: change of systolic blood pressure; MAP: mean arterial pressure; Me: median; PBP: pulse blood pressure; Q25–Q75: interquartile range; SBP: systolic blood pressure.
The observed ACE genotype frequencies in the study participants were in Hardy-Weinberg equilibrium. The frequency of allele D in the entire group (n=591) was 0.533. Frequency of genotypes II, ID, and DD were 19.97% (n=118), 53.47% (n =316), and 26.56% (n =157), respectively, which is consistent with data reported in other European populations. 21 No statistically significant differences in the distribution of the ACE genotypes prior to pregnancy were observed between the three study groups (Table 2).
Associations of the angiotensin-converting enzyme (ACE) insertion-deletion (I/D) polymorphism with the blood pressure parameters in the study women.

ANOVA: analysis of variance; DBP: diastolic blood pressure; MAP: mean arterial pressure; p: value for the Mann-Whitney test; pcor : p: value for the Mann-Whitney test with Bonferroni correction; PBP: pulse blood pressure; SBP: systolic blood pressure. The values of blood pressure level are expressed as median (Me) and interquartile range (Q25–Q75).
Friedman′s ANOVA test allowed us to reveal that the BP parameters increased significantly by the end of pregnancy in comparison with those prior to pregnancy, with most increased BP level in carriers of genotype DD. However, as can be seen from Table 2, the values of the systolic and mean BP during pregnancy were the lowest in women with the II genotype and the highest in women with the DD genotype. At 37–40 weeks of gestation, women with genotypes DD and ID had greater values of SBP, DBP and average BP as compared to those with genotype II. Furthermore, the frequency of allele D was the highest in the group of women with hypertension at the end of pregnancy (56.6%) followed by the subjects with normotension (50.7%) and hypotension (35.0%) (the data are shown in Figure 2). Accordingly, the largest number of individuals with genotype DD and the lowest one with genotype II were observed in the hypertensive women (29.5% and 16.4%, p=0.01, pcor=0.03), while the opposite pattern of the genotype distribution was seen in the hypotensive group (6.7% and 36.6%, p=0.02, pcor=0.06) (Figure 3). None of the study groups (normotensive, hypotensive or hypertensive women) showed statistically significant differences in the parameters of BP between the carriers of the ACE genotypes among women before and during a pregnancy (Table 3).

Distribution of the alleles of the angiotensin-converting enzyme (ACE) insertion-deletion (I/D) polymorphism in the groups of pregnant (37–40 weeks term) women with different blood pressure status.

Distribution of the genotypes of the angiotensin-converting enzyme (ACE) insertion-deletion (I/D) polymorphism in the groups of pregnant (37–40 weeks term) women with different blood pressure status.
Association analysis of the angiotensin-converting enzyme (ACE) insertion-deletion (I/D) polymorphism with blood pressure parameters in hypotensive, normotensive and hypertensive groups of women.

SBP: systolic blood pressure; DBP: diastolic blood pressure; p: value for the Mann-Whitney test; PBP: pulse blood pressure; MAP: mean arterial pressure. The value of blood pressure level is expressed as median (Me) interquartile range (Q25–Q75).
Linear regression analysis observed the impact of current age (t=2.9, p=0.004), weight (t=8.2, p<0.0001) and the ACE polymorphism (t=−3.8, p=0.0002) on SBP at the end of pregnancy (R2=15.33%). In addition, the DBP depended (R2=10.9%) on the same factors such as current age (t=2.3, p=0.02), weight (t=6.7, p<0.0001) and the ACE genotypes (t=−3.5, p=0.0006). The impact of the same factors was seen with respect to the pulse pressure of pregnant women.
Discussion
The results of the present study suggest that the I/D polymorphism of the ACE gene is associated with the level of arterial BP at the later stage of pregnancy (37–40 weeks) in women. Allele D confers higher BP, whereas allele I is associated with lower BP. The observed association between the I/D polymorphism of the ACE gene and level of BP in women at the end of pregnancy is supported by the data about the physiological role of this enzyme. It has been recently reported that healthy individuals possessing the D allele of the ACE gene had significantly higher levels of the circulating enzyme in blood than those possessing the homozygous II genotype, while the heterozygotes had the intermediate levels.11–13 The ACE enzyme participates in the synthesis of angiotensin II, which has a strong vasoconstrictor effect. 22 Therefore, individuals with the highly expressed DD genotype have a higher vascular tone and BP level. 23 Furthermore, under normal conditions, concentration of the ACE in plasma of pregnant women constantly increases until the third trimester. Notably, women with genotype DD ACE have the maximum concentration of the enzyme as compared to those with genotypes ID and II,11,12 and in turn, this results in higher BP at the end of pregnancy.
Ample evidence exists about association of the I/D ACE polymorphism with various cardiovascular disorders such as essential hypertension,24,25 coronary artery disease,26,27 myocardial infarction, 28 and myocardial hypertrophy. 29 It should be noted that the renin-angiotensin-aldosterone system may be involved in the development of both insulin resistance and gestational diabetes mellitus. 30 The increased levels of ACE in plasma accounted for by the DD genotype 11 may be responsible for the increasing levels of aldosterone and thereby lead to insulin resistance and gestational diabetes.
The literature data on association between the I/D polymorphism of the ACE gene and hypertension during pregnancy are contradictory. In Table 4, we summarize several genetic studies which investigated the association of I/D polymorphism of the ACE gene and BP level during pregnancy. In particular, a higher frequency of allele D and genotype DD was reported among patients with pregnancy-induced hypertension (PIH) in the Chinese population.31,32 One of the studies 32 has found the association of genotype DD with higher concentrations of plasma angiotensin II in pregnant women with hypertension, as compared to healthy women. Similar results were obtained in the Indian sample consisting of 50 pregnant women with PIH and 50 pregnant women with normotension. 33 The authors reported the association of genotype DD with PIH, although they did not find any association of the I/D polymorphism with either plasma ACE levels or hypertension. 33
A summary of studies investigated the association of insertion-deletion (I/D) polymorphism of the angiotensin-converting enzyme (ACE) gene and blood pressure level during pregnancy.
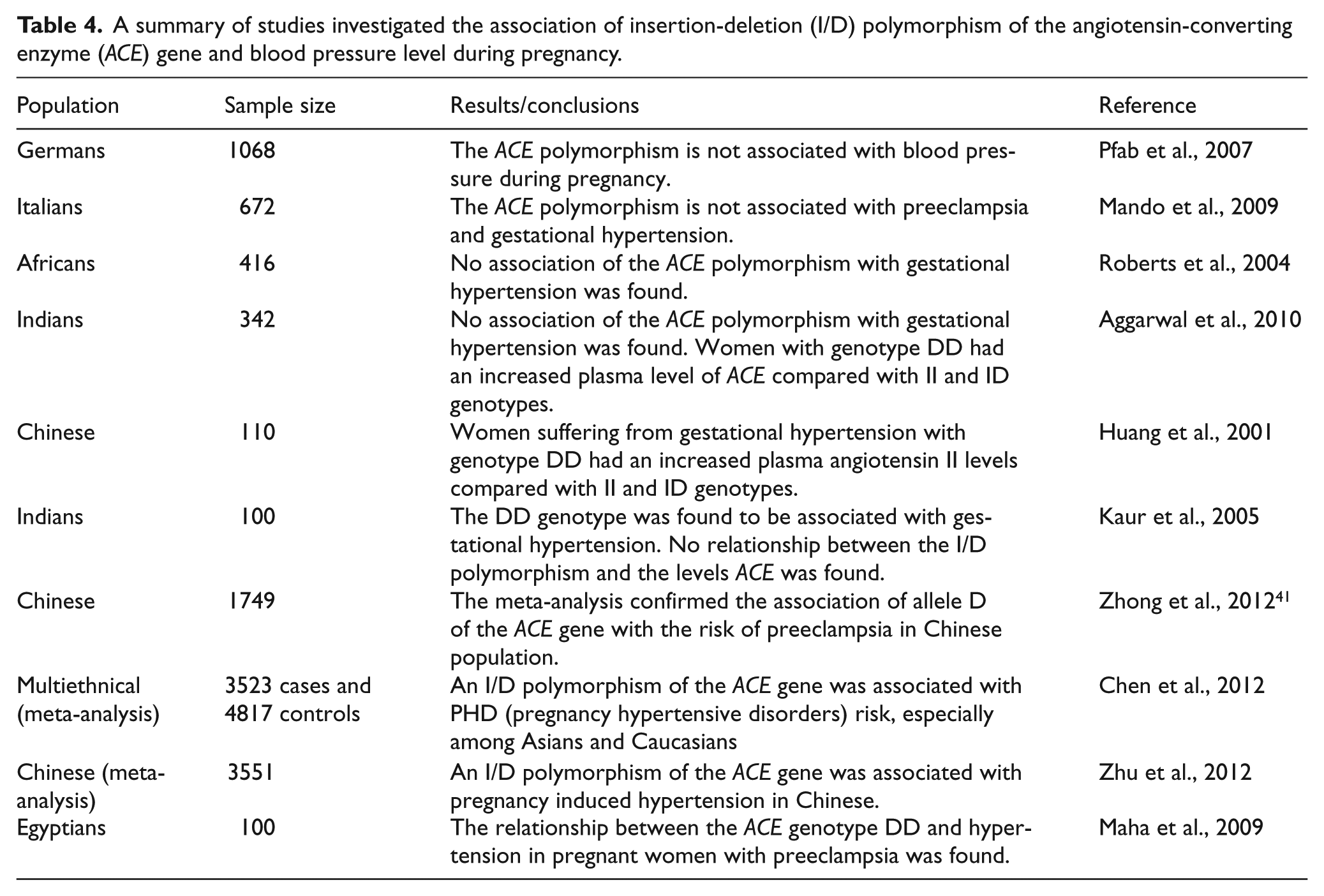
The study conducted on the Arabian population has found a relationship between the genotype DD and hypertension in pregnant women with preeclampsia. 34 However, contradictory results have been obtained in a number of studies conducted in Chinese, Indian, African and Italian populations.35–38 In particular, in the sample of 104 pregnant women from Northern India, no association of either allele D or genotype DD with PIH was observed despite the higher blood ACE levels in the carriers of DD genotype as compared to the carriers of the ID and II genotypes. 36 Similar results were reported for the Chinese, Africans and Italians.35,37–39 A large study (more than 1000 Caucasian women) conducted by Pfab with coworkers did not reveal the association of I/D polymorphism of the ACE gene with BP level during a pregnancy. 40 Meantime, a meta-analysis of more than 50 studies showed a significant association of the I/D polymorphism with PIH and preeclampsia in Chinese,41,42 and in Asians and Caucasians. 43 The observed inconsistency in the above results may be explained by inter-population and interethnic differences in the distribution of the I/D polymorphism: allele D is predominant in Caucasians from Europe, Australia and the USA, whereas allele I is more prevalent among Chinese and Indians.44–47 Therefore, this feature may explain the different clinical importance of the polymorphism for PIH in populations of the world. The existing inconsistency in the genetic studies warrants further research into the role of the ACE gene in the regulation of BP and the development of PIH.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.