
Abstract
Aims:
Carrying the D-allele of the angiotensin-converting enzyme (ACE) I/D polymorphism and high ACE activity are prognostic factors in diabetic nephropathy, which predicts mortality in type 1 diabetes. We studied the association between the ACE D-allele and ACE phenotype and long-term all-cause mortality in three single-institution outpatient cohorts.
Methods:
Genotype-based analyses were performed in 269 patients from Hillerød Hospital (HIH) (follow-up: 12 years) and in 439 patients with diabetic nephropathy and 437 patients with persistent normoalbuminuria from the Steno Diabetes Center (SDC) (follow-up: 9.5 years). Patients not on renin-angiotensin system (RAS)-blocking treatment were included in analyses of serum ACE activity (HIH: n = 208) and plasma ACE concentration (SDC: n=269).
Results:
In the HIH cohort, carrying a D-allele was associated with excess mortality (hazard ratio (HR) = 4.0 (95% confidence interval (CI) 1.0–16)), but not in the SDC cohorts. At HIH, serum ACE activity was associated with excess mortality (HR=1.04 (95% CI 1.0–1.1 per unit increase)), but in the SDC cohort plasma ACE concentration was not.
Conclusion:
In unselected patients with type 1 diabetes, carrying the ACE D-allele and high spontaneous serum ACE activity were associated with 12-year excess mortality. These findings could not be reproduced in two other cohorts with persistent normoalbuminuria or diabetic nephropathy.
Introduction
The angiotensin-converting enzyme (ACE) I/D polymorphism is a common and functionally highly significant gene variation explaining almost half of the interindividual variation in circulating and tissue ACE activity. 1 Subjects carrying the DD genotype have almost two-fold higher ACE activity compared to subjects homozygous for the I-allele. 1 The polymorphism is implicated as a prognostic factor in several conditions in which the renin-angiotensin system (RAS) is believed to play a pathophysiologic role including cardiovascular disease (CVD), hypertension, nephropathy,2,3 as well as several other conditions.4–6 In type 1 diabetes, D-allele carriage is associated with CVD and faster progression of diabetic nephropathy.7–11 In accordance, pharmacologic inhibition of the RAS delays progression of diabetic nephropathy in type 1 diabetes. 12 Presence of diabetic nephropathy is a powerful predictor of mortality in type 1 diabetes.13,14 Therefore, we tested the hypothesis that presence of the ACE D-allele and a correspondingly high spontaneous ACE activity are associated with excess long-term all-cause mortality in type 1 diabetes. We studied an index cohort of unselected patients with type 1 diabetes and—because of the result of this analysis—sought to replicate and validate these findings in two other independent cohorts of patients with type 1 diabetes.
Subjects and methods
Design
We conducted a prospective, observational follow-up study in three single-institution outpatient cohorts: an index cohort from Hillerød University Hospital (HIH) and two cohorts from the Steno Diabetes Center (SDC). Written informed consent was obtained from all participants before entering the studies and the studies were approved by the regional ethics committee on Biomedical Research Ethics. Data from medical records and the Danish Cause of Death register were collected without knowledge of the results of the genetic and biochemical analyses.
Patient cohorts
Hillerød Hospital
Cohort one (HIH-total) comprised consecutive patients with type 1 diabetes recruited from the outpatient clinic at Hillerød Hospital in 1998–2001 15 and was followed for 12 years. A subpopulation of this cohort was not treated with any RAS blocking agents (HIH-nonRAS). Inclusion criteria in HIH-total were age ≥ 18 years, duration of diabetes for longer than two years, no end-stage renal disease or significant comorbidities. Thus, HIH-total consists of patients in generally good health. The patients were characterized according to ACE genotype and serum ACE activity as well as history of use of any RAS-blocking agents. At baseline, data about diabetes history and complications were extracted from patient records. The patients were followed for a median of 12 years. Four patients stopped control in the outpatient clinic and were therefore followed only until their last contact. Nephropathy was classified as either normoalbuminuria (urinary albumin excretion rate <30 mg per 24 hours), microalbuminuria (urinary albumin excretion rate 30–300 mg per 24 hours) or macroalbuminuria (urinary albumin excretion rate >300 mg per 24 hours). Presence of macrovascular complications (i.e. stroke, myocardial infarction (MI) or claudication) were classified at baseline as either none or any macrovascular complication.
Steno Diabetes Center
The second cohort (SDC-DN) comprised patients with diabetic nephropathy (urinary albumin excretion rate >300 mg per 24 hours) enrolled in a study at the Steno Diabetes Center in 1993–2006 7 who were followed for a median of 9.5 years.16,17 Cohort three (SDC-NA) consisted of patients with persistent normoalbuminuria despite 15 years with type 1 diabetes.16,17 Plasma ACE concentration was measured at baseline in a subpopulation (n=231) of SDC-DN and SDC-NA. These patients not treated with any RAS-blocking agents were included in a subpopulation study (SDC-ACE) on the effect of plasma ACE concentration on mortality. The SDC-ACE cohort included patients with persistent normoalbuminuria (56%) as well as patients with diabetic nephropathy (44%). Baseline data about diabetes history and measures of HbA1c, blood pressure and the ACE I/D polymorphism were obtained. 7 Macrovascular complications were classified at baseline as either none or any macrovascular complications (i.e. MI, stroke or amputations due to vascular disease).
Endpoint registration
Information regarding mortality was obtained through the Central Office of Civil registration. Cause of death was extracted from medical records and cross-checked with the Danish Cause of Death Register. Cause of death was classified as CVD if classified as acute MI, death from heart failure, cardiac arrhythmic death, cardiovascular procedure-related death or other cardiovascular death according to the death certificate and World Health Organization (WHO) ICD10 code. In the cohorts from the Steno Diabetes Center, cause of death was classified as cardiovascular deaths unless an unequivocal noncardiovascular cause was established. 18 Cause of death was classified as non-CVD if owing to malignant disease, suicide, violence or accident, infection, renal failure, hypoglycemia, respiratory insufficiency or other non-CVD. If no cause could be obtained, the cause of death was labeled as unknown.
Laboratory analysis
ACE genotype was determined by polymerase chain reaction (PCR) on total genomic DNA extracted from frozen whole blood, including a check for misclassification of DD patients by means of an insertion-specific primer. In the HIH cohort, serum ACE activity was determined kinetically at 340 nm utilizing the tripeptide N-(3-(2-furyl)acroloyl)-L-phenylalanylglycylglycine (FAPGG) as the substrate (Sigma Diagnostics, St. Louis, MO, USA). The within-assay and between-assay variability were 13% and 11%. 15 In the SDC-ACE cohort, plasma concentration of ACE was measured by an enzyme-linked immunosorbent (ELISA) assay method using a sandwich combination of monoclonal and poly clonal antibodies. 19 HbA1c was measured as reported elsewhere.16,20
Statistical analysis
We used an age-truncated Cox proportional hazard model using SAS 9.3 when analyzing the unadjusted and adjusted hazard ratios (HR) for mortality. This model takes into account the wide age range in the cohorts as well as the strong association with age, duration of diabetes and mortality. Use of age-truncation instead of follow-up time as in a regular Cox regression allows correction for duration of diabetes without the collinear relationship with age. It also adjusts for the fact that patients have the same genotype throughout their lives. The ACE ID polymorphism is associated with nephropathy and cardiovascular complications in type 1 diabetes. 7 Therefore we analyzed for multicollinearity using the variance inflation factor (VIF) in SPSS software package 19. All VIFs were below 1.2, indicating no risk of multicollinearity between the variables included in our model. 21 In the model we allowed six to eight events per degree of freedom, which allowed us to include six variables (gender, diabetes duration, HbA1c, CVD, nephropathy, and D-allele carrier status) in the adjusted model on the HIH-total (Table 1) and two variables (CVD and serum ACE activity) in the adjusted model on the HIH-nonRAS cohort (Table 2). In the SDC-DN and SDC-NA cohorts, we used all the same variables but nephropathy in the adjusted model (Table 1) as in the HIH-total study to compare the study findings. In SDC-ACE analysis we included data about nephropathy, HbA1c, and plasma ACE concentration (Table 2). Before including any parameters in the multivariate analysis, we analyzed each variable for linear proportionality to be true to the assumption of linear proportionality in the model. In the HIH-total cohort linear proportionality was present for all variables except macrovascular complications, which were then included in the multivariate analysis as strata. The assumption of linear proportionality was true for the variables included in the HIH-nonRAS, SDC-DN, SDC-NA and SDC-ACE cohorts. Finally, a backward age-truncated Cox proportional hazard analysis was performed to identify the importance of each significant variable.
Result of the unadjusted and adjusted age-truncated Cox proportional hazard analysis for the ACE ID polymorphism.
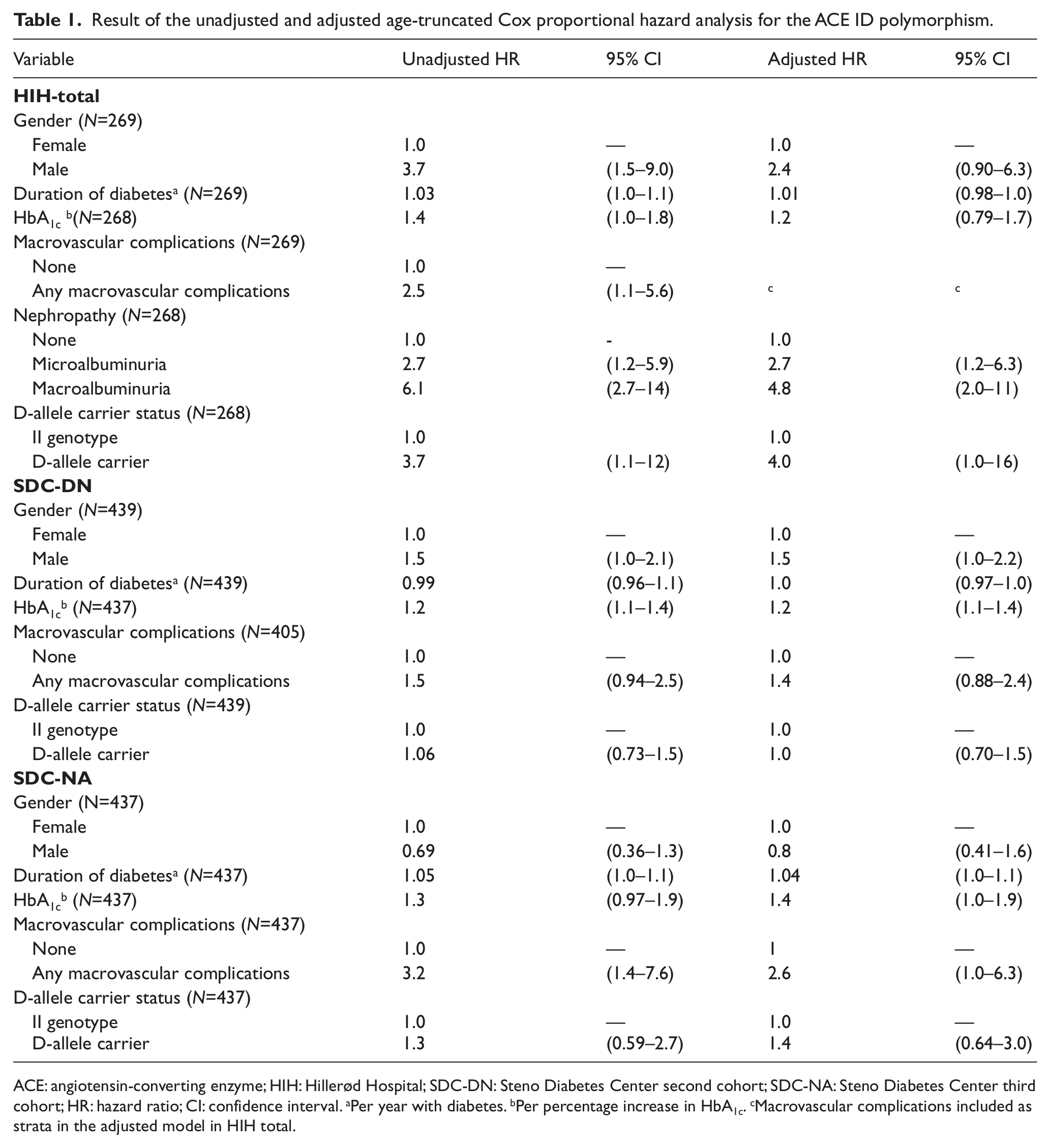
ACE: angiotensin-converting enzyme; HIH: Hillerød Hospital; SDC-DN: Steno Diabetes Center second cohort; SDC-NA: Steno Diabetes Center third cohort; HR: hazard ratio; CI: confidence interval. aPer year with diabetes. bPer percentage increase in HbA1c. cMacrovascular complications included as strata in the adjusted model in HIH total.
Result of the unadjusted and adjusted age-truncated Cox proportional hazard analysis for serum ACE activity (HIH-nonRAS) and plasma ACE concentration (SDC-ACE).

ACE: angiotensin-converting enzyme; HIH: Hillerød Hospital; RAS: renin-angiotensin system; SDC-DN: Steno Diabetes Center second cohort; SDC-NA: Steno Diabetes Center third cohort; HR: hazard ratio; CI: confidence interval. aPer 1 U/l or µg/l increase in serum ACE activity or plasma ACE concentration, respectively. bPer percentage increase in HbA1c. cIn the unadjusted model we tested gender, diabetes duration, HbA1c, macrovascular complications, nephropathy and D-allele carrier.
Results
Patient characteristics
At baseline 269 patients (60% males) were included in the HIH-total. Eight percent had CVD at baseline, 9% had nephropathy (Table 3), and 20% were treated with ACE inhibitors (Table 4). After a median follow-up of 12 years, 39 patients (15%) had died; 33% of the deceased patients died of CVD, 61% of non-CVD and 6% of unknown causes. In the SDC-DN cohort, 439 patients (62% males) with diabetic nephropathy were included at baseline. Ten percent had CVD (Table 3) and 61% were treated with ACE inhibitors (Table 4). After a median follow-up of 9.5 years, 140 patients (32%) had died; 50% died from CVD, 33% from non-CVD and 17% from other causes. Finally, in SDC-NA, 437 patients (53% males) with long-standing normoalbuminuria were included at baseline. Four percent had CVD and 9% were treated with ACE inhibitors (Table 4). After a median follow-up of 9.5 years, 36 patients (8%) had died; 31% died of CVD, 46% of non-CVD and 23% of other causes.
Baseline characteristics of the patients included in the cohorts investigating the effects of the ACE ID polymorphism.

Values are median (SD) or n (%) as indicated. ACE: angiotensin-converting enzyme; HIH: Hillerød Hospital; SDC-DN: Steno Diabetes Center second cohort; SDC-NA: Steno Diabetes Center third cohort. aDifference between HIH-total and SDC-DN. bDifference between HIH-total and SDC-NA. cDifference between SDC-DN and SDC-NA.
Characteristics of the RAS in the different cohorts investigating the effects of the ACE ID polymorphism.
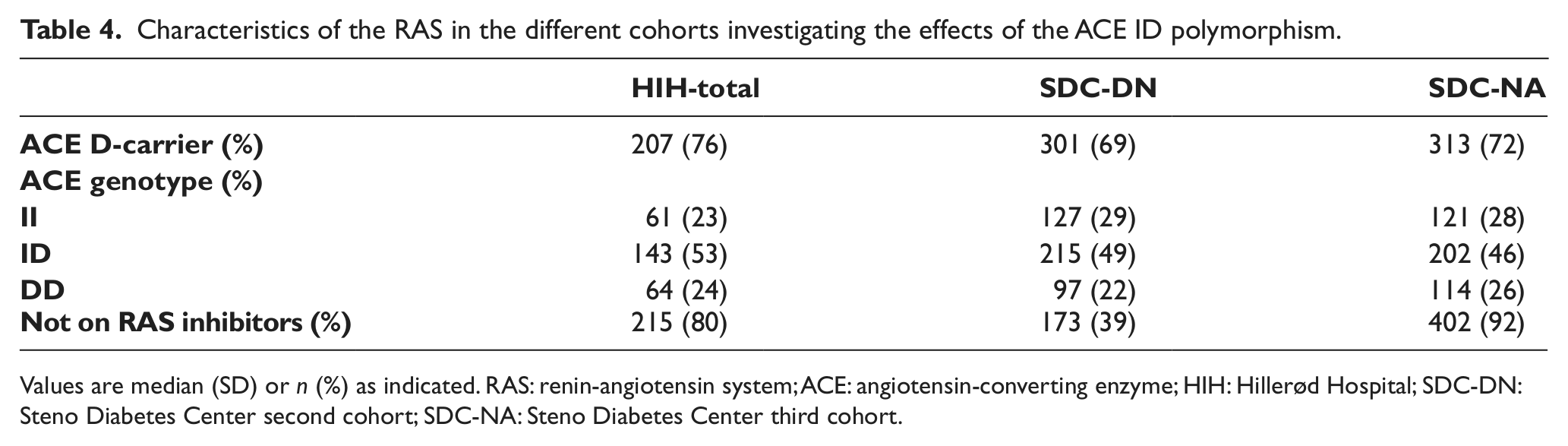
Values are median (SD) or n (%) as indicated. RAS: renin-angiotensin system; ACE: angiotensin-converting enzyme; HIH: Hillerød Hospital; SDC-DN: Steno Diabetes Center second cohort; SDC-NA: Steno Diabetes Center third cohort.
Duration of diabetes was longer in SDC-DN and SDC-NA than in HIH-total (p < 0.0001) and slightly longer in SDC-DN than in SDC-NA (p < 0.005) (Table 3). At baseline, macrovascular complications were more frequent in HIH-total (p < 0.05) and SDC-DN (p < 0.0005) than in SDC-NA. Diabetic retinopathy was more frequent in SDC-DN than in SDC-NA (p < 0.0001) and more frequent in SDC-NA than in HIH-total (p < 0.01). Death from CVD was more prevalent in SDC-DN than in HIH-total and SDC-NA (p < 0.01), while causes of death did not differ between HIH-total and SDC-NA.
HIH-nonRAS consisted of 208 patients. Four percent had macrovascular complications and 1% had nephropathy (Table 5). During follow-up, 16 (8%) died; 12.5% died of CVD, 68.5% of non-CVD and 19% of other causes. SDC-ACE consisted of 231 patients (59% males). Two percent had CVD and 29% had nephropathy (Table 5). During follow-up, 60 (26%) died; 47% of CVD, 38% of non-CVD and 15% of other causes. Microvascular complications (retinopathy and nephropathy) were more frequent in SDC-ACE than in HIH-nonRAS (p < 0.0001) (Table 5). Death from CVD was more prevalent in SDC-ACE than in HIH-nonRAS (p < 0.05).
Baseline characteristics of the patients included in the cohorts investigating the effect of either serum ACE activity or plasma ACE concentration.

ACE: angiotensin-converting enzyme; HIH: Hillerød Hospital; RAS: renin-angiotensin system; SDC-DN: Steno Diabetes Center second cohort; SDC-NA: Steno Diabetes Center third cohort. Values are median (SD) or n (%) as indicated. aDifference between HIH-nonRAS and SDC-ACE.
Associations between mortality and ACE genotype and phenotype
In HIH-total, one or two D-alleles of the ACE ID polymorphism were present in 90% of the dead patients and in 75% of the survivors (p < 0.05). ACE D-allele carriage was associated with excess mortality (HR 3.7 (95% confidence interval (CI) 1.1–12.3), p < 0.05) in the unadjusted age-truncated Cox proportional hazard analysis, and also when adjusting for gender, duration of diabetes, HbA1c, presence of macrovascular complications and presence of nephropathy (HR 4.0 (1.0–17), p<0.05) (Table 1). The backwards analysis revealed that ACE D-allele carriage ((HR 3.8 (1.0–14), p<0.05) and signs of kidney disease (microalbuminuria: HR 2.7 (1.2–6.3), (p < 0.02)) and (macroalbuminuria: HR 4.8 (2.0–11) (p < 0.001)) were independently associated with mortality (Table 1).
In SDN-DN and SDN-NA, there were no differences in the distribution of the ACE ID polymorphism in the dead and alive patients. In SDC-DN, HbA1c (HR 1.2 (1.1–1.4), p < 0.001) was significant in the unadjusted Cox model but ACE D-allele carrier status was not (HR 1.1 (0.7–1.5), p = 0.76). A similar result was found in the adjusted model (Table 1). At backwards analysis HbA1c (HR 1.2 (1.1–1.4), p < 0.0005) and male gender (HR 1.5 (1.0–2.1), p < 0.05) were independently associated with mortality (Table 1). In SDC-NA, duration of diabetes (HR 1.1 (1.0–1.1), p<0.05) and CVD (HR 3.2 (1.4–7.6), p < 0.01) were significant in the unadjusted model. In the adjusted model, both HbA1c (HR 1.4 (1.0–1.9), p < 0.05) and CVD (HR 2.6 (1.0–6.3), p < 0.05) were significantly associated with mortality. At backwards analysis only CVD remained significant (HR 2.6 (1.0–6.3), p<0.05) (Table 1).
In HIH-nonRAS, the median serum ACE activity was 44 U/l (Table 6) and higher in patients who died during follow-up as compared to those who remained alive (52±15 vs 43±17 U/l; p < 0.05). CVD (HR 5.2 (1.3–22), p < 0.05) and serum ACE activity (HR 1.0 (1.0–1.1), p < 0.05) were associated with excess mortality in this cohort. In the adjusted model, serum ACE activity was independently associated with excess mortality (HR 1.0 (1.0–1.1), p < 0.05), corresponding to an HR of 1.5 (1.1–2.0) per 10 U/l increase in serum ACE activity (Table 2). In SDC-ACE the median plasma ACE concentration was 449 µg/l and higher in the patients with diabetic nephropathy than in the normoalbuminuric patients (512±180 vs 424±298 µg/l; p < 0.005) (Table 6). Presence of nephropathy (HR 3.1 (1.5–6.2), p<0.005) and HbA1c (HR 1.4 (1.1–1.8), p < 0.01) were associated with excess mortality in SDC-ACE but plasma ACE concentration was not (p = 0.5). In the adjusted model only nephropathy (HR 2.6 (1.2–5.6), p < 0.05) remained significantly associated with mortality (Table 2).
Characteristics of the RAS in the different cohorts investigating the effect of either serum ACE activity or plasma ACE concentration.

ACE: angiotensin-converting enzyme; HIH: Hillerød Hospital; RAS: renin-angiotensin system; SDC-DN: Steno Diabetes Center second cohort; SDC-NA: Steno Diabetes Center third cohort. Values are median (SD) or n (%) as indicated.
Discussion
In this study, we assessed the impact of the ACE ID polymorphism and ACE phenotype as determined by a random measurement of serum ACE activity or concentration on mortality in three different cohorts of patients with type 1 diabetes. In the relatively healthy but otherwise unselected index cohort (HIH-total) that ACE genotype (being a D-allele carrier) and phenotype (high serum ACE activity) were associated with excess mortality, as well as in analyses adjusted for gender, diabetes duration, macrovascular complications and nephropathy. Because of consistent statistically significant findings of associations between both ACE genotype and ACE phenotype with excess mortality and since the cohort was relatively small, we sought to validate the findings in two other independent cohorts of patients with type 1 diabetes. In these two cohorts—one apparently resistant to diabetic complications (SDC-NA) and one prone to diabetic nephropathy (SDC-DN)—we were unable to demonstrate associations between ACE genotype and phenotype and mortality.
Although we cannot rule out that our findings in the index cohort are false positive because of low statistical power, the effect of the ACE genotype on mortality in the HIH-total may be a true association. The reason for the lack of consistency with the SDC-DN could be that most patients in this cohort were treated with RAS-blocking drugs. The treatment effectively blunts the difference in ACE activity between the genotypes, reducing the effect of ACE genotype on RAS activity. In SDC-NA the event rate might be too low to permit replication. Similarly, if the association between serum ACE activity and mortality in the index cohort is valid, the inconsistency with the results in SDC-ACE could be explained by the fact that the patients in the latter cohort had more advanced diabetes with longer duration of diabetes and higher frequency of late diabetic complications and thus they were not comparable. Furthermore, plasma ACE concentration and not serum ACE activity was measured in SDC-ACE. While ACE activity is effectively blocked by ACE inhibitors, ACE concentration may be paradoxically increased by these agents (unpublished data from the Steno cohorts). The results in the SDC-DN and SDC-NA cohorts may potentially indicate that the effects of the ACE I/D polymorphism and serum ACE activity are important only in unselected patient cohorts, but not in cohorts presenting the extremes in terms of mortality risk, in whom other factors may be more important.
The RAS is present in almost all tissues and involved in various pathological conditions. 22 In type 1 diabetes the D-allele is associated with faster development and progression of diabetic nephropathy9–11 independent of glycemic control. 23 In patients with type 1 diabetes and diabetic nephropathy, the II genotype acts as a protective factor for coronary heart disease. 7 Furthermore the D-allele confers an increased risk of MI24–26 independently of other risk factors. RAS is implicated in prolonged QTc interval during hypoglycemia, 27 a condition that predisposes to ventricular arrhythmia. 28 Thus several studies do support the relevance of our hypothesis that presence of the ACE D-allele and a correspondingly high spontaneous ACE activity are associated with excess long-term all-cause mortality in type 1 diabetes as also found in the HIH-total cohort. However, the reasons for our divergent findings are unclear and further research is needed to prove or disprove our findings.
In conclusion, we found an association between the ACE ID polymorphism and the correspondingly high serum ACE activity with all-cause mortality in a largely unselected cohort of patients with type 1 diabetes. The finding could not, however, be reproduced in two larger cohorts representing two extremes of mortality risk in type 1 diabetes. To further investigate the role of the ACE ID polymorphism in mortality in type 1 diabetes, studies are warranted in larger unselected cohorts of patients.
Footnotes
Acknowledgements
We thank research nurses P. Banck and T. Larsen, Hillerød Hospital, for handling patients and data, and Børge Nordestgaard, MD, DMSc, Herlev Hospital, Denmark, for analyzing serum ACE activity.
Novelty statement
Add knowledge to established effects of the renin-angiotensin system (RAS). In a cohort of unselected patients with type 1 diabetes, high RAS activity is associated with excess mortality. In two cohorts of patients with type 1 diabetes without albuminuria or with diabetic nephropathy, this finding could not be reproduced.
Contribution statement
Ulrik Pedersen-Bjergaard collected data in the HIH cohorts and Lise Tarnow did so for the SDC cohorts. The SDC cohort database was updated by Maria Lajer. Data about mortality in the HIH-total were collected and updated in the database by Anne-Sophie Sejling. Louise Færch is the main author of the manuscript and has performed all the statistical analysis in the manuscript. All authors have participated in the writing process and approved the final manuscript.
Funding
This study was funded by grants from The EFSD/JDRF/Novo Nordisk Programme for Research in Type 1 Diabetes, The Foundation of Harald Jensen and Wife, Region 3 Foundation, The Foundation of Tvergaard, The Foundation of Frederiksborg County, and a research grant from Hillerød Hospital.
Conflict of interest
None declared.