
Abstract
Background:
Compared to patients with similar levels of hypertension, patients with primary aldosteronism have a greater left ventricular hypertrophy (LVH). The presence of LVH should be detected as early as possible to prevent cardiovascular complications associated with the condition. We evaluated comparative diagnostic value of electrocardiographic (ECG) indexes for LVH in patients with primary aldosteronism.
Methods:
ECG and echocardiographic data were obtained in 88 patients with primary aldosteronism. We analyzed the four most commonly used ECG indexes, including Sokolow-Lyon index, Cornell voltage index, Cornell product index, and Gubner index.
Results:
Echocardiographic LVH was found in 35 patients (40%). Sensitivity ranged from 0% for Gubner index to 49% for Cornell product index. Specificity ranged from 81% for Sokolow-Lyon index to 100% for Gubner index. Sokolow-Lyon index (r=0.43, p<0.001), Cornell voltage index (r=0.55, p<0.001) and Cornell product index (r=0.52, p<0.001) correlated significantly with left ventricular mass (LVM) index. No significant correlation was found between Gubner index and LVM index.
Conclusions:
ECG indexes had a reasonably high specificity, but a low sensitivity for LVH in patients with primary aldosteronism. Cornell voltage index and Cornell product index had a better diagnostic value of LVH, and had a better correlation with LVM index in these patients.
Introduction
Primary aldosteronism is characterized by hypertension, hypokalemia, suppressed plasma renin activity (PRA) and autonomous aldosterone production.1–3 The excess aldosterone could be associated with a pressure-independent remodeling of the left ventricle. Compared to patients with similar levels of hypertension, patients with primary aldosteronism have greater left ventricular hypertrophy (LVH) and increased rate of cardiovascular complications.4,5 The presence of LVH should be detected as early as possible to prevent cardiovascular complications associated with the condition. The 12-lead electrocardiography (ECG) is recommended as the routine test for detection of LVH in patients with arterial hypertension because of its established clinical value, broad availability, and low cost. Sokolow-Lyon index, 6 Cornell voltage index, 7 Cornell product index, 8 and Gubner index 9 have been most commonly used to rule out LVH in patients with arterial hypertension. In this study, we evaluated their comparative diagnostic value for LVH in patients with primary aldosteronism.
Methods
Study population
From January 2005 to December 2011, a total of 93 patients with primary aldosteronism were referred to our hospital. Primary aldosteronism was confirmed with captopril challenge test, furosemide plus upright test and/or salt loading test. One patient with ventricular pacing and four patients with bundle branch block were excluded from analysis because electrocardiographic LVH could not be assessed in these patients. Thus, this study consisted of 88 patients with primary aldosteronism. Informed consent was obtained from each patient.
Laboratory examinations
PRA and plasma aldosterone concentration (PAC) were measured by radioimmunoassay. Blood was collected from an antecubital vein, and serum potassium concentrations were measured using a standard ion electrode method. Hypokalemia was defined as serum potassium less than 3.6 mEq/l. 10
Electrocardiogram
A 12-lead ECG was recorded on admission at a paper speed of 25 mm/sec and an amplification of 10 mm/mV. We analyzed in detail the four most commonly used ECG indexes, including Sokolow-Lyon index, Cornell voltage index, Cornell product index, and Gubner index. These indexes were measured in each ECG as follows:

Electrocardiographic LVH was defined as Sokolow-Lyon index > 3.5 mV, Cornell voltage index > 2.8 mV in men and > 2.0 mV in women, Cornell product index ≥ 2440 mm•ms in men and > 2440 mm•ms in women, and Gubner index ≥ 2.5 mV.
Echocardiography
Transthoracic echocardiographic data were obtained on admission using a commercial ultrasound machine. Two-dimensional guided M-mode measurements of left ventricular end-diastolic diameter (LVDD), interventricular septum thickness (IVS), and posterior wall thickness (PW) were measured. Left ventricular mass (LVM) was calculated using the formula of Deverreux and Reichek11,12: left ventricular mass (g) =1.04[(LVDD+IVS+PW)3−(LVDD)3]−13.6. LVM index was calculated by dividing LVM by body surface area. Echocardiographic LVH was defined as LVM index > 131 g/m2 in men and > 100 g/m2 in women. 13
Statistical analysis
Statistical analysis was performed with chi-square and Student’s t-tests. Relations between variables were determined by linear regression analysis. All data are expressed as mean±SD. Differences were considered significant if the p value was <0.05.
Results
Patient characteristics
Patient characteristics are shown in Table 1. There were 44 male and 44 female patients with a mean age of 56.2 ± 12.1 years. Systolic blood pressure was 145.5 ± 20.0 mmHg. PRA and PAC were 0.51 ± 0.38 ng/ml/h and 27.4 ± 21.8 pg/ml, respectively. Serum potassium was 3.68 ± 0.61 mEq/l.
Patient characteristics.

Incidence of electrocardiographic and echocardiographic LVH
Heart rate was 70.6±12.4 bpm. QRS duration was 93.2±11.1 ms. Sokolow-Lyon index, Cornell voltage index and Gubner index were 3.07±0.87 mV, 1.72±0.81 mV, and 0.90±0.50 mV, respectively. Electrocardiographic LVH was found in 25 patients (28%) on Sokolow-Lyon index, in 12 patients (14%) on Cornell voltage index, and in 25 patients (28%) on Cornell product index. No patient had electrocardiographic LVH on Gubner index. LVM index was 116.2±32.2 g/m2. Echocardiographic LVH was found in 35 patients (40%).
Accuracy of ECG indexes for diagnosis of echocardiographic LVH
Table 2 shows the accuracy of the four ECG indexes for diagnosis of echocardiographic LVH. Sensitivity ranged from 0% for Gubner index to 49% for Cornell product index. Specificity ranged from 81% for Sokolow-Lyon index to 100% for Gubner index. Correct diagnosis was obtained in 66% with Sokolow-Lyon index, in 69% with Cornell voltage index, in 70% with Cornell product index, and in 60% with Gubner index.
Accuracy of electrocardiographic indexes for diagnosis of echocardiographic left ventricular hypertrophy.

LVH=left ventricular hypertrophy; NM=not measured.
Figure 1 shows the correlations between the four ECG indexes and LVM index. Sokolow-Lyon index (r=0.43, p<0.001), Cornell voltage index (r=0.55, p<0.001) and Cornell product index (r=0.52, p<0.001) correlated significantly with LVM index. On the other hand, no significant correlation was found between Gubner index and LVM index.
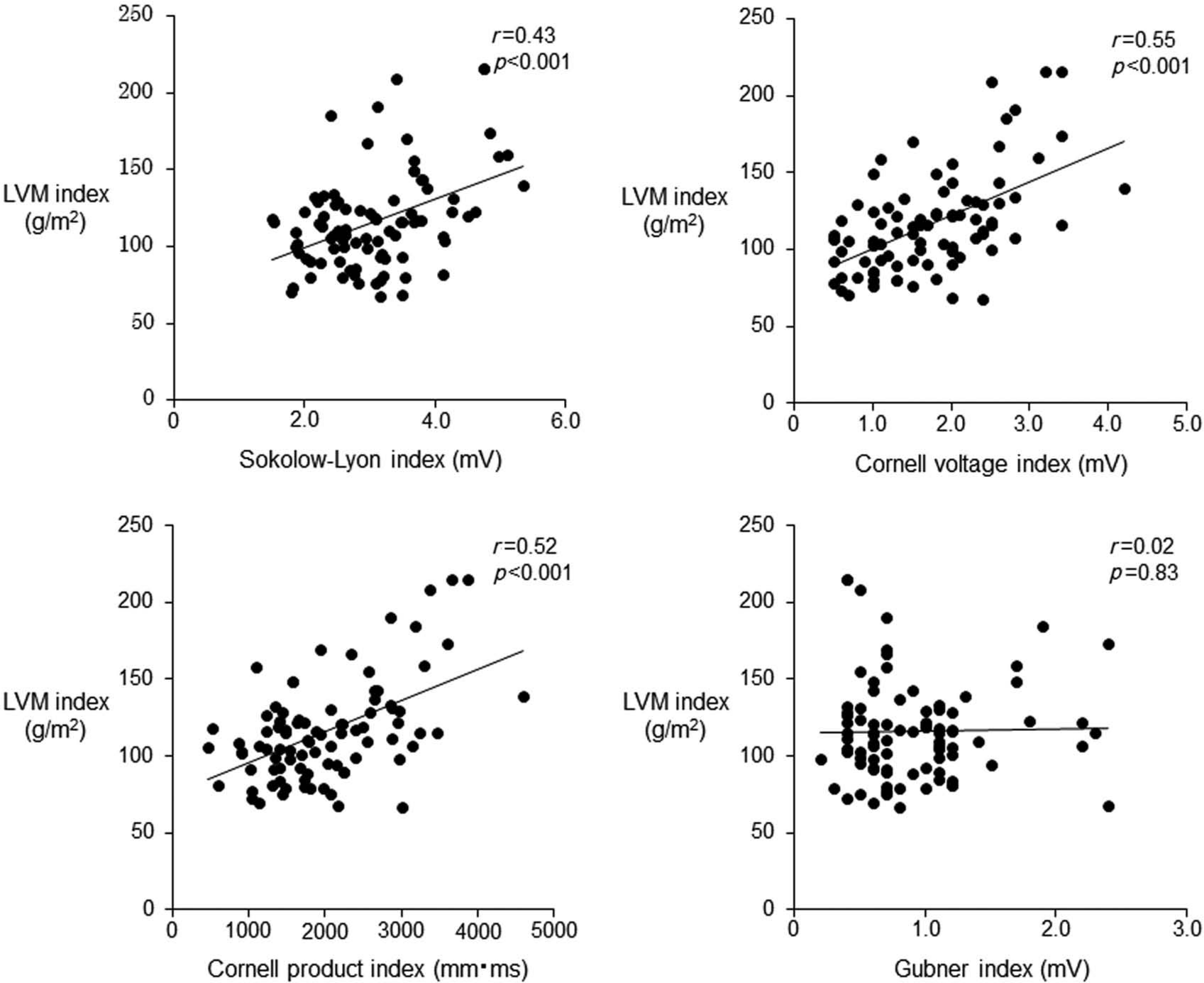
Correlations between the four electrocardiographic indexes and left ventricular mass (LVM) index.
Effect of hypokalemia on QRS voltage of ECG indexes
There were 28 patients with hypokalemia and 60 patients with normokalemia (Table 3). Serum potassium levels were 2.98 ± 0.47 mEq/l and 4.00 ± 0.31 mEq/l, respectively. Sokolow-Lyon index and Cornell voltage index as well as LVM index were significantly higher in hypokalemic patients than normokalemic patients. However, these ECG indexes divided by LVM index were similar between the two groups. There was no significant difference in Gubner index between the two groups.
Comparison of QRS voltage between hypokalemic and normokalemic patients.

LVM: left ventricular mass.
Discussion
The current study demonstrated the following: 1) commonly used ECG indexes had a reasonably high specificity, but the power to rule in LVH was unsatisfactory because of low sensitivity in patients with primary aldosteronism; and 2) Cornell voltage index and Cornell product index had a better diagnostic value for LVH, and had a better correlation with LVM index.
Arterial hypertension is a major cause of coronary artery disease, stroke, LVH, and heart failure. Several studies have shown that LVH is an important risk factor in patients with hypertension, leading to a 5- to 10-fold increase in cardiovascular risk.14–16 ECG is a routine test to rule out LVH in patients with hypertension. Although more than 30 indexes for detection of LVH have been described, only several ECG indexes such as Sokolow-Lyon index, Cornell voltage index, Cornell product index, and Gubner index remain to be used in the clinical setting.
Previous clinical studies showed that patients with primary aldosteronism had greater LVH and worse diastolic function compared to patients with similar levels of hypertension. 4 The renin–angiotensin–aldosterone system is thought to play an important role in the pathogenesis of LVH independent of increased blood pressure. 17 Experimental studies have shown that aldosterone induces cardiomyocyte hypertrophy, profound changes in the extracellular matrix, leading to collagen deposition and subsequently to myocardial fibrosis.18–20 Although primary aldosteronism is often accompanied by LVH, there has been no report evaluating comparative diagnostic value of ECG indexes for LVH in these patients. In the current study, we demonstrated that commonly used ECG indexes had a reasonably high specificity, but a low sensitivity for LVH in patients with primary aldosteronism. Our results in primary aldosteronism were similar to those previously shown in arterial hypertension. 21 Among the four indexes, Cornell voltage index and Cornell product index had a better diagnostic value for LVH, and had a better correlation with LVM index in patients with primary aldosteronism. Both adrenalectomy and aldosterone antagonists are known to be effective in reducing LVM index in patients with primary aldosteronism.22,23 Our results suggested that Cornell voltage or Cornell product index might be suitable for evaluating the degree of LVH or monitoring reduced LVH after these interventions.
The ECG was insensitive for detection of LVH in the current study. However, previous studies have shown that electrocardiographic LVH and echocardiographic LVH predict mortality independently of each other, 24 and that combined these findings improve risk stratification. 25 These imply that electrocardiographic LVH and echocardiographic LVH in part carry different prognostic information. Therefore, both ECG and echocardiography should be performed to assess the considerable risk associated with these conditions in patients with primary aldosteronism.
Previous studies reported that a significant reduction of QRS voltage was observed after short-term potassium supplementation, suggesting hypokalemia might be at least partly relevant to the high QRS voltage in patients with primary aldosteronism. 26 In the current study, Sokolow-Lyon index and Cornell voltage index as well as LVM index were significantly higher in hypokalemic patients than normokalemic patients. However, these ECG indexes divided by LVM index were similar between the two groups, suggesting that QRS voltage reflected LVM index well in spite of serum potassium level. It appeared that hypokalemia did not affect QRS voltage as much as LVM index. In the current study, PAC was significantly higher in hypokalemic patients than normokalemic patients. Therefore, we speculated that hypokalemia reflected more severe hyperaldosteronism that could cause greater LVH.
There are several limitations in the current study. First, we did not assess other ECG indexes. Romhilt-Estes score has been also used to rule out LVH in patients with arterial hypertension. However, this scoring system is not easy in the clinical setting, and includes ST-T segment pattern with high points that is often associated with hypokalemia.27,28 Because there was a possibility that Romhilt-Estes score might overestimate LVH especially in hypokalemic patients, we did not include Romhilt-Estes score in the current study. Second, we obtained ECG and echocardiographic data routinely only before potassium supplement in hypokalemic patients. Therefore, we could not assess the change in these data before and after potassium supplement. There was a possibility that, in hypokalemic patients, ECG indexes after potassium supplementation might have a better diagnostic value for LVH, and had a better correlation with LVM index in patients with primary aldosteronism.
In conclusion, ECG indexes had a reasonably high specificity, but a low sensitivity for LVH in patients with primary aldosteronism. Cornell voltage index and Cornell product index had a better diagnostic value of LVH, and had a better correlation with LVM index in these patients.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.