
Abstract
Introduction:
Blockade of the renin-angiotensin system (RAS) is a critical approach to the management of hypertension, especially in proteinuric patients. It is well proven that the direct renin inhibitor aliskiren shows comparable clinical efficacy to the angiotensin II receptor blocker valsartan on blood pressure control and albuminuria. However, there is only limited data on the hand-to-hand effectiveness of these two RAS blockers in improving arterial stiffness. We tested whether aliskiren or valsartan would improve arterial stiffness in hypertensive patients with albuminuria who are already on antihypertensive therapy.
Material and methods:
Thirty-four patients with hypertension and albuminuria < 1 g, after a wash-out period of three weeks, were randomized to aliskiren or valsartan in a 24-week randomized parallel-group study.
Results:
A nonsignificant difference in blood pressure was seen between the two treatment groups. Albuminuria was significantly reduced in both groups (56% for the aliskiren group, p < 0.05, and 38% for the valsartan group, p < 0.05). Only valsartan but not aliskiren significantly reduced carotid-femoral pulse wave velocity (–1.1 ± 0.8 m/s (p = 0.02) for valsartan and +0.1 ± 0.7 m/s (ns) for aliskiren).
Conclusion:
The results of our study showed that valsartan improves arterial stiffness to a significantly greater extent than aliskiren, despite a similar antihypertensive and antiproteinuric effect.
Introduction
Hypertension is a prevalent risk factor for cardiovascular (CV) disease, affecting up to 30% of the adult population in the Western world. 1 On the other hand, microalbuminuria is an early marker of endothelial dysfunction and a strong prognostic predictor of mortality and CV disease. 2 In recent years, great emphasis has been placed on the role of arterial stiffness in the development of CV diseases and it is used in the assessment of patients with hypertension. Moreover, it has a better predictive value than classical CV risk factors entering various types of risk score.
The renin-angiotensin system (RAS) has emerged as a key target for the management of hypertension. In the presence of albuminuria, it is suggested that RAS blockade with angiotensin-converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARBs) should be the first line of antihypertensive treatment. 2 Aliskiren is the first and sole drug in the new class of direct renin inhibitors approved for the treatment of hypertension that blocks the RAS at its point of activation.
The aim of our study was to assess whether aliskiren compared to valsartan would improve arterial stiffness and albuminuria in hypertensive patients.
Material and methods
Patients
Eligible patients were aged 18 years or older, diagnosed with mild to moderate hypertension (stage 1 or 2) with a spot urine albumin-to-creatinine ratio (u-ACR) more than 17 mg/g in men, 25 mg/g in women and less than 1 g/g. Key exclusion criteria were hyperkalemia, secondary hypertension based on clinical and laboratory findings, atrial fibrillation or other cardiac rhythm disorders and pregnancy.
Study design
This was a 24-week single-center, randomized, open-label, parallel-group, prospective study. In patients receiving anti-hypertensive treatment, blood pressure (BP) medications were discontinued for a wash-out period of three weeks during which all patients received clonidine 300–600 mcg/day according to medical needs. At the end of the run-in period, patients were randomized to receive either aliskiren 150 mg or valsartan 160 mg once daily (od) and administration of clonidine was interrupted. After two weeks, aliskiren and valsartan were titrated to 300 mg and 320 mg, respectively, if BP was not well controlled (sitting BP ≥ 140/90 mmHg). In patients who remained out of target after four weeks, diltiazem 300 mg or nebivolol 5 mg od was added according to medical indications. The third anti-hypertensive agent that patients received if required (BP ≥ 140/90 mmHg) was hydrochlorothiazide 12.5 mg od. No other antihypertensive agent was permitted during the trial to prevent interference with study evaluations and interpretation of results. However, if sitting systolic BP (SBP) and/or diastolic BP (DBP) exceeded the safety parameters of ≥ 180 mmHg and ≥ 110 mmHg, respectively, at any point during the study, patients were withdrawn from the study and were treated accordingly. Similarly, if SBP < 100 mmHg and DBP < 60 mmHg, patients were discontinued for safety reasons. Each patient’s assessment with office BP measurements was performed at screening and at the third week in the clonidine run-in phase as well as every four weeks thereafter, while 24-hour ambulatory BP monitoring (ABPM), arterial stiffness and laboratory measurements were performed at baseline (run-in phase) and at week 24.
All patients were recruited from the outpatient renal clinic of our hospital. The hospital’s Ethics Committee approved this study protocol, and informed consent was obtained from all subjects.
Laboratory measurements
All laboratory measurements were performed at the laboratory of biochemistry of our hospital using standardized methods and an Olympus AU 600 clinical chemistry analyzer (Olympus Diagnostica, Hamburg, Germany). Blood samples were obtained following a 12-hour overnight fast.
Glomerular filtration rate (eGFR) was estimated using the Cockcroft-Gault formula: eGFR = ((140–age) × body weight)/(72 × serum creatinine), where body weight is in kg, age is in years and serum creatinine is in mg/dl. For women the results were multiplied by a factor of 0.85 to compensate for the lower average muscle mass. The concentration of total cholesterol (TChol) and triglycerides (Trg) was determined enzymatically. High-density lipoprotein cholesterol (HDL) was determined in the supernatant after precipitation of the ApoB-containing lipoproteins with dextran sulfate-Mg2+ (Sigma Diagnostics, St Louis, MO, USA). Low-density lipoprotein cholesterol (LDL) was calculated using the Friedewald formula provided fasting Trg levels were less than 400 mg/dl. In patients with serum Trg values greater than 400 mg/dl, LDL concentrations were not determined. On-the-spot urine sample, urine albumin and creatinine concentration were measured within eight hours of specimen collection. Solid-phase fluorescence immunoassay was used to measure urinary albumin. All assessments were performed to a standard protocol that conformed to the international standards for definitions and measurements.
Hemodynamic measurements
BP determinations were taken after a 5-minute rest in a sitting position at each visit. Brachial BP was measured three times at 2-minute intervals by an automated sphygmomanometer (Omron Digital Blood Pressure Monitor 705-IT, Kyoto, Japan) The mean values of the last two readings for both brachial SBP and DBP were used for calculation. Brachial pulse pressure (PP) was calculated as SBP–DBP.
Following the last measurement, three successive recordings, each over 10 seconds, of the radial artery pressure wave forms were sampled by applanation tonometry (Millar tonometer, Millar Instruments, Houston, TX, USA) using the Sphygmocor system (Atcor, Sydney, Australia). Data that met the automatic quality controls specified by the Sphygmocor software were used to derive central aortic pressure waveforms by a previously validated generalized transfer function, 3 from which central aortic SBP, DBP and PP values were obtained. Brachial arterial BP was used to calibrate the radial pressure pulse. Aortic pressure waveforms were subjected to further analysis by the Sphygmocor software to calculate the aortic augmentation index (AIx). AIx is defined as the increment in pressure from the first systolic shoulder (inflection point) to the peak pressure of the aortic pressure waveform expressed as a percentage (of peak pressure) and provides a quantitative measure of augmentation of central BP. 3 AIx data were corrected for a heart rate of 75 beats per minute.
Carotid-femoral pulse wave velocity (PWV) was determined from carotid and femoral pressure waveforms obtained non-invasively by applanation tonometry (Millar tonometer, Millar Instruments) using the Sphygmocor system (Atcor). Waveforms were referenced to a concurrently recorded electrocardiogram, and carotid to femoral transit time (ΔT) was computed from the foot-to-foot time difference between carotid and femoral waveforms. The distance between the surface markings of the sternal notch and the carotid (dc) and femoral artery (df) were used to estimate the path length between the carotid and femoral arteries (L = df–dc) and carotid-femoral PWV computed as L/ΔT. The within-subject standard deviation of carotid-femoral PWV assessed using this method in our laboratory is 0.5 m/s and the intraobserver and interobserver coefficient of variation are 3.0% and 3.5%, respectively.
Twenty-four-hour ABPM was performed noninvasively on the non-dominant arm using a SpaceLabs model 90207 device and spacing the readings at 15-minute intervals. 2 Patients were instructed to continue with their usual activities, return the following morning for device removal and keep their arm extended and immobile at the time of the cuff’s inflation. For this study, ABPM was regarded as valid only if ≥ 80% of BP measurements during the daytime and nighttime periods (from subject diaries) were satisfactory. All of the valid recordings were analyzed to obtain average 24-hour, daytime and nighttime SBP and DBP. The mean BP of the above measurements was used for analyses in this study.
Statistical analysis
Treatment-related changes in parameters were analyzed using a t test. Moreover, the more conservative non-parametric Wilcoxon test was performed. We analyzed the relationship between the change in arterial stiffness and changes in other parameters using Spearman’s correlation test. Continuous values are expressed as means ± standard deviation (SD). A p value of less than 0.05 was considered statistically significant. Statistical analysis was performed using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Thirty-four patients were randomized in the study. A total of 29 patients completed the full study protocol and were eligible for analysis. Five patients discontinued the study treatment because of: noncompliance (one patient), uncontrolled hypertension (one patient) and loss to follow-up (three patients). Fifteen patients (10 males) were randomized in the aliskiren group and 14 (10 males) in the valsartan group. The two groups were matched for anthropometric and somatometric parameters (Table 1). There were no significant differences in basic biochemical parameters between the studied groups (Table 2).
Baseline demographic characteristics of the two therapeutic groups.

M: male; F: female; CVD: history of cardiovascular disease; BMI: body mass index; ns: nonsignificant.
Biochemical parameters at baseline.
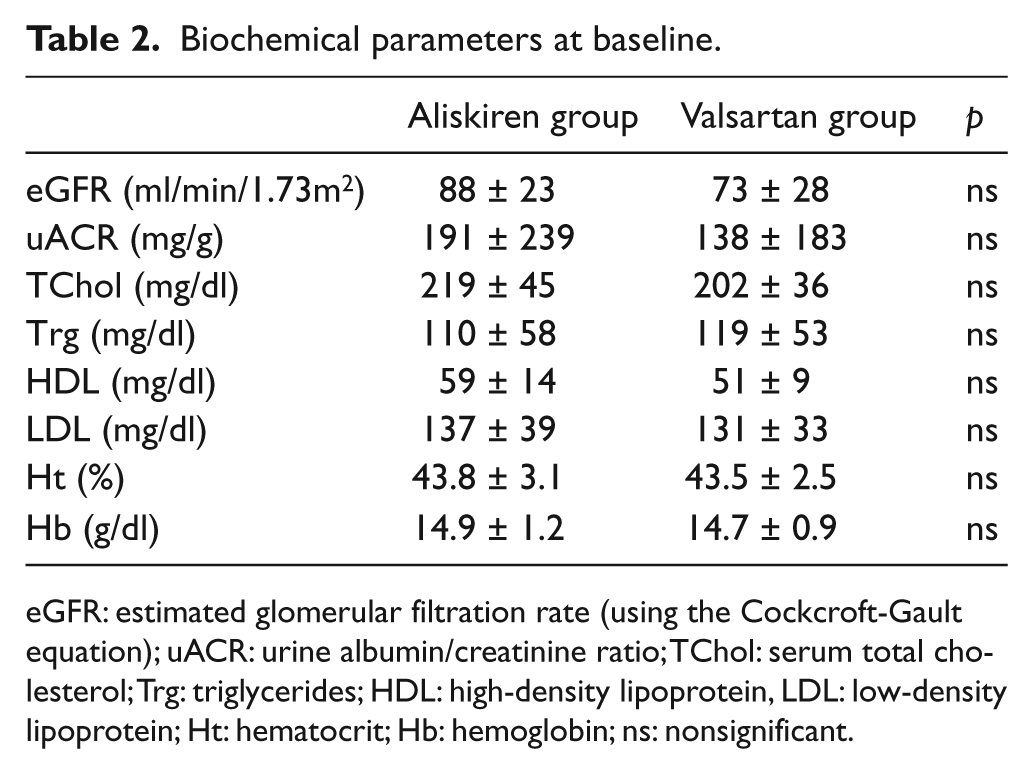
eGFR: estimated glomerular filtration rate (using the Cockcroft-Gault equation); uACR: urine albumin/creatinine ratio; TChol: serum total cholesterol; Trg: triglycerides; HDL: high-density lipoprotein, LDL: low-density lipoprotein; Ht: hematocrit; Hb: hemoglobin; ns: nonsignificant.
In seven patients, additional antihypertensive agents were administered for the control of BP in each group of the study. The mean number of medications used per patient was 1.6 in the aliskiren group (diltiazem in six patients, diuretic in two patients, nebivolol in one patient) and 1.56 in the valsartan group (diltiazem in five patients, diuretic in three patients).
Mean office SBP and DBP were similar at baseline in both groups (Table 3). After the 24-week treatment period, a nonsignificant reduction in office SBP and DBP measurements was found in both therapeutic arms (Table 4). In particular, a decrease of 5.1/1.1 and 2.9/3.7 mmHg was noticed in SBP and DBP in the aliskiren group and in the valsartan group, respectively (Table 5). Between the studied groups, no significant statistical difference in SBP and DBP reduction was noticed (Table 5).
Baseline hemodynamic assessment.
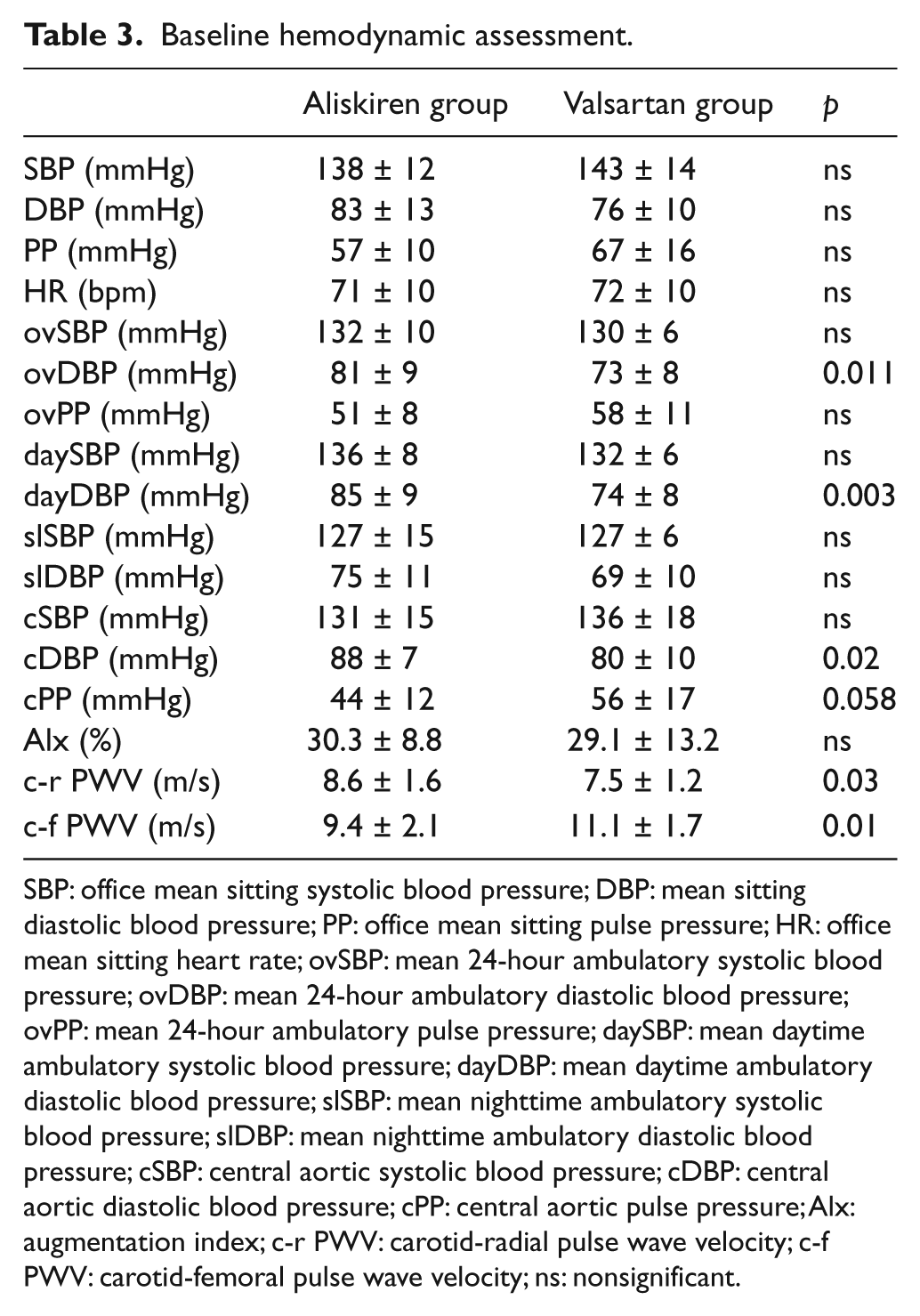
SBP: office mean sitting systolic blood pressure; DBP: mean sitting diastolic blood pressure; PP: office mean sitting pulse pressure; HR: office mean sitting heart rate; ovSBP: mean 24-hour ambulatory systolic blood pressure; ovDBP: mean 24-hour ambulatory diastolic blood pressure; ovPP: mean 24-hour ambulatory pulse pressure; daySBP: mean daytime ambulatory systolic blood pressure; dayDBP: mean daytime ambulatory diastolic blood pressure; slSBP: mean nighttime ambulatory systolic blood pressure; slDBP: mean nighttime ambulatory diastolic blood pressure; cSBP: central aortic systolic blood pressure; cDBP: central aortic diastolic blood pressure; cPP: central aortic pulse pressure; Alx: augmentation index; c-r PWV: carotid-radial pulse wave velocity; c-f PWV: carotid-femoral pulse wave velocity; ns: nonsignificant.
Effects of studied agents after the 24-week treatment period.

SBP: office mean sitting systolic blood pressure; DBP: mean sitting diastolic blood pressure; PP: office mean sitting pulse pressure; HR: office mean sitting heart rate; ovSBP: mean 24-hour ambulatory systolic blood pressure; ovDBP: mean 24-hour ambulatory diastolic blood pressure; ovPP: mean 24-hour ambulatory pulse pressure; daySBP: mean daytime ambulatory systolic blood pressure; dayDBP: mean daytime ambulatory diastolic blood pressure; slSBP: mean nighttime ambulatory systolic blood pressure; slDBP: mean nighttime ambulatory diastolic blood pressure; cSBP: central aortic systolic blood pressure; cDBP: central aortic diastolic blood pressure; cPP: central aortic pulse pressure; Alx: augmentation index; c-r PWV: carotid-radial pulse wave velocity; c-f PWV: carotid-femoral pulse wave velocity; uACR: urine albumin/creatinine ratio; ns: nonsignificant.
Response after the 24-week treatment period.

SBP: office mean sitting systolic blood pressure; DBP: mean sitting diastolic blood pressure; PP: office mean sitting pulse pressure; HR: office mean sitting heart rate; ovSBP: mean 24-hour ambulatory systolic blood pressure; ovDBP: mean 24-hour ambulatory diastolic blood pressure; ovPP: mean 24-hour ambulatory pulse pressure; daySBP: mean daytime ambulatory systolic blood pressure; dayDBP: mean daytime ambulatory diastolic blood pressure; slSBP: mean nighttime ambulatory systolic blood pressure; slDBP: mean nighttime ambulatory diastolic blood pressure; cSBP: central aortic systolic blood pressure; cDBP: central aortic diastolic blood pressure; cPP: central aortic pulse pressure; Alx: augmentation index adjusted for heart rate 75 beats/minute; c-r PWV: carotid-radial pulse wave velocity; c-f PWV: carotid-femoral pulse wave velocity; uACR: urine albumin/creatinine ratio; ns: nonsignificant.
After the 24-week treatment period, a significant reduction of central SBP was found in the valsartan group (Table 4). Wave reflections, expressed with Alx, had a nonsignificant reduction in both arms and between both arms after the 24-week treatment period (Table 4). Carotid-femoral PWV had no significant changes in the aliskiren group, while a statistically significant reduction was found in the valsartan group at the latest follow-up (Table 4). Between groups no significant differences were found in arterial stiffness indices after the 24-week treatment period (Table 5).
Additionally, the number of patients with carotid-femoral PVW < 10 m/s increased in the aliskiren group by one versus four in the valsartan group after the six-month treatment period (Table 6).
Tertiles according to pulse wave velocity measurements.

c-f PWV: carotid-femoral pulse wave velocity.
After the 24-week treatment period, albuminuria expressed with u-ACR was decreased significantly in both therapeutic groups. In particular, u-ACR was decreased by 56% (107 mg/g) in the aliskiren arm and by 38% (54 mg/g) in the valsartan arm. Additionally, there was no significant difference in u-ACR reduction between the groups (Table 4).
Discussion
Blockage of the RAS is a critical approach to the management of patients with arterial hypertension and micro- or macro-albuminuria. 4 However, the cardio-renal protection afforded by inhibitors of the RAS may be mediated, at least in part, by drug-specific effects on arterial stiffness and albuminuria.
In our study, the antihypertensive agents aliskiren and valsartan showed similar antihypertensive effects in office BP measurements and in 24-hour ABPM measurements. However, it must be noted that the baseline BP was well controlled in the study, which allowed for only a lower rate of BP decline. Both agents reduced BP levels in both groups of patients. Additionally, there was no significant difference between them in BP reduction.
Our results are in accordance with two recent trials that showed similar reductions in BP comparing aliskiren and valsartan monotherapy5,6 in patients with hypertension.
Increased arterial stiffness is a powerful and independent risk factor for early mortality and provides prognostic information above and beyond traditional CV risk factors such as blood pressure itself, age, gender, diabetes, smoking and cholesterol.7,8 Carotid-femoral PWV is considered the “gold-standard” measurement of arterial stiffness, 9 and a large amount of evidence indicates that PWV is an intermediate endpoint for CV events, either fatal or non-fatal,10–12 and able to predict outcome in subjects with diabetes mellitus. 13 Guidelines for the Management of Arterial Hypertension not only recommend measurements of arterial stiffness in patients with arterial hypertension, but also a threshold of carotid-femoral PWV greater than 12 m/s has been suggested as an estimate of subclinical organ damage. 2
The results of our study showed that carotid-femoral PWV was significantly reduced only in the valsartan group after the treatment period compared to baseline levels, and aliskiren has no effect in PWV when office BP is stable. However, we should note that the mean baseline carotid-femoral PWV was significantly smaller in the aliskiren group, which may affect the PWV reduction in this group.
On the other hand, to our knowledge there is only a small pilot study 14 evaluating arterial stiffness changes with the administration of aliskiren. In that study, using a typical therapeutic dose in type 1 diabetes mellitus patients, PWV was reduced 12.8% during hyperglycemia state. These outcomes were the opposite of those in our study, where aliskiren did not show any change in arterial stiffness after six months of therapy. In the above study, patients enrolled were non-hypertensive, without microalbuminuria with a significant reduction of BP with one month’s administration of aliskiren.
In our study one could also argue that the number of patients with carotid-femoral PVW < 10 m/s increased in the aliskiren group by one versus four in the valsartan group after the six-month treatment period, which means that valsartan may have better effectiveness in PWV reduction.
Changes in PWV are believed to be influenced by long-term pressure-dependent structural changes that may be slowed but not reversed by pharmacotherapy. 15 Our group of patients had BP well controlled from the beginning, were treated for a short period of time (24 weeks) and, even so, PWV was significantly reduced in the valsartan group.
There are no previous reports in patients with hypertension and albuminuria regarding the effects of aliskiren compared to valsartan on arterial stiffness. Our results suggest that valsartan reduces arterial stiffness beyond what would be expected from the antihypertensive effects and support the view that in this patient group arterial wall properties are ameliorated to a greater extent and more durably by valsartan than aliskiren.
In our study a significant reduction in central SBP was found in the valsartan group while Alx had a non-significant reduction in both arms. Central aortic pressures and AIx measurements do not necessarily reflect the same arterial wall properties as measured by PWV, which reflect changes in pressure wave reflections from distal sites. The reflective properties of the vasculature can be modulated independently of arterial stiffening.16,17 In a recent study, lower central aortic pressures despite similar brachial BP lowering effects resulted in fewer CV and renal events. 18 In our study the valsartan group performed more favorably compared to aliskiren.
In a recent report comparing aliskiren and ramipril, PWV was significantly reduced by both drugs and aliskiren induced a significantly greater AIx reduction than ramipril. 19 These findings were found in hypertensive patients when BP was significantly reduced. On the other hand, valsatran reduced PWV when administered in hypertensive patients with albuminuria. There are reports that valsartan reduced brachial ankle PWV (Ba-PWV) compared with a calcium channel blocker despite similar brachial BP control in patients with essential hypertension. 20 In that study, however, no significant reduction in Ba-PWV from baseline was seen with calcium channel blockade; furthermore carotid-femoral PWV, as a measure of arterial stiffness, was not evaluated. In another study treatment with valsartan/hydrochlorothiazide reduced carotid-femoral PWV by 0.9 m/s more than amlodipine in patients with diabetes, systolic hypertension and albuminuria despite similar attained brachial and central aortic PP in both groups at the end of the study. 21
In our study u-ACR was decreased significantly in both therapeutic groups. RAS blockade agents have been shown to confer significant renal protection in terms of the reduction of albuminuria and the retardation of renal failure when administered to patients with albuminuria.
The reduction in albuminuria achieved with RAS blockade may be a critical step toward achieving renoprotection. The magnitude of albuminuria reduction during the first months of therapy with an RAS blocker in patients with diabetic and non-diabetic disease was linearly associated with the degree of eGFR loss decline during long-term follow-up.22–24
Valsartan is a well-established antihypertensive agent used successfully for more than 15 years,25,26 while ARBs have shown that they reduce albuminuria by approximately 35%. 27
Aliskiren, on the other hand, since the first publication describing it as a BP-lowering drug, 28 appeared promising in the management of hypertension and as an alternate antihypertensive agent because it blocks renin at the first and rate-limiting step of the RAS pathway and thus provides strong potential for more comprehensive RAS inhibition. The two drug classes have divergent effects on angiotensin II concentrations and receptor occupancy. Preclinical studies have shown that aliskiren also has kidney-protective effects in diabetic as well as non-diabetic models of kidney disease.29,30 The hypothesis has been tested in the past by Parving et al., 31 who showed that treatment with aliskiren and losartan was superior to losartan and placebo, as evidenced by a 20% reduction in albuminuria compared with placebo, with a reduction of 50% or more in 24.7% of the patients. It was suggested that the renoprotective effect of aliskiren was independent of BP. Another smaller study 32 using irbesartan instead of losartan in patients with type 2 diabetes, hypertension and albuminuria > 100 mg/day confirmed the results of the previous trial in that the combined treatment with irbesartan and aliskiren reduced albuminuria by 71%, versus 48% and 58% with aliskiren and irbesartan as monotherapy. Recently, Aliskiren Trial in Type 2 Diabetes Using Cardio-Renal Endpoints (ALTITUTE)’s data safety monitoring board advised against continuing the study because “the active treatment group experienced an increased incidence of non-fatal stroke, renal complications, hyperkalemia, and hypotension over 18 to 24 months of follow-up.” The committee concluded that patients were unlikely to benefit from aliskiren on top of standard antihypertensive treatment, and aliskiren-based combination therapy in hypertensive patients with concomitant high-risk type 2 diabetes or GFR < 60 ml/min/1.72m2 is not recommended (http://www.novartis.com/newsroom/media-releases/en/2011/1572562.shtml).
Conclusions
The present study shows that aliskiren and valsartan have similar antihypertensive and antiproteinuric effects and reduced BP levels in a cohort of patients with hypertension and albuminuria without significant difference in BP reduction between them. Regarding arterial stiffness parameters, a significant reduction was noticed in central SBP and carotid-femoral PWV in the valsartan group only. However, this was an open-label design and of a relatively small sample size, which limits the extent to which results should be generalized.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.