
Abstract
Our comparative study uses practice-based understandings of behaviour to expose the hidden ‘inequalities of ease’ which underlie healthy eating behaviours in different socioeconomic circumstances. This adds depth to the well-established direct impacts of socioeconomic factors through illuminating the more subtle contextual factors which enhance these effects and reduce the ease of healthy eating in contexts of deprivation. Drawing on in-depth multi-method research with 25 mothers living in two contrasting areas of Bristol and a subsequent survey with 310 respondents, we illustrate how the materials, competences and meanings which shape our eating practices are socioeconomically patterned. What is the impact of socioeconomic differences in mundane materials such as dining tables? Or in the risks involved in developing skills related to unprocessed food preparation? Or in the prioritisation of ‘health’ among the many meanings of good food? In all of these examples we show that the materials, competences and meanings which are more likely to be associated with the practices of those who live in deprived areas serve to systematically skew easy unthinking eating habits away from the minimally-processed fruits and vegetables which were universally understood to be key to healthy eating. Applying a practice lens to inequalities in healthy eating in this way provides novel insights into how deeply structural inequalities are embedded in the microcosms of everyday life and how they affect the ease of eating healthily through shaping what we do unthinkingly on ‘autopilot’. Education and awareness-raising interventions which ignore the systematic skewing of easy unthinking eating practices cannot close the healthy eating gap, instead serving to justify blaming those who are already most disadvantaged for the inequalities in preventable ill-health which tax their wellbeing and take years off their lives.
Introduction
This paper aims to illuminate the hidden ways in which inequalities in healthy eating reflect disparities in the ease of eating healthily more than a lack of effort or knowledge. We will argue that such socioeconomically striated differences in healthy eating reflect not so much a difference in voluntary effort put into eating by individuals, as differences in the extent to which our limited conscious capacities for controlling our actions are supported by the non-conscious factors which determine the bulk of what we do. Those living in socioeconomic deprivation are only too aware of the gap between basic ideas of what healthy eating is (which they mainly share) and their ability to live up to them, while the inequalities of ease they face in eating healthily remain hidden. This situation is deeply problematic. So long as these contextual injustices are obscured in favour of addressing presumed discrepancies in knowledge or individual motivation, inequalities in healthy eating will be seen as the product of individual failures rather than systematic biases making healthy eating harder for those living in deprivation.
We argue that understanding the systematic skewing of (un)healthy eating requires detailed attention to the role of effort in conditioning action and the ways in which the effort required to carry out the same eating behaviours varies. Although moment-to-moment, task-to-task effort varies, as recent psychological studies demonstrate, in general people tend to follow the path of least effort – the path of ease. Effortful action is clearly possible, but it is not the norm (Kahneman, 2011). This is certainly true of eating, where our behaviour has been found to be largely habitual. We typically consume in ways that don’t require much effort or conscious thought: we eat what is easy for us to eat (van’t Riet et al., 2011; Naughton et al., 2015; Sobal and Wansink, 2007; Wansink, 2006; Wansink, 2010). A body of empirical research indicates that in many instances eating can be characterised as an ‘automatic’ behaviour “over which the environment has more control than do individuals” (Cohen and Farley, 2008, 1; Moldovan and David, 2012; Rothman et al., 2009; Neal et al., 2011). If effort is universally limited regarding eating (as these studies demonstrate) and knowledge as fairly equally distributed regarding the healthiness of fruit and vegetables and the unhealthiness of ultraprocessed foods (as several studies and our own data confirm – see 3.4), then the size of the gap between everyday default eating habits and common understandings of healthy eating could be seen as indicative of the size of inequalities in the amount of effort which would be required of individuals to bridge this gap between norms and ideals and feed themselves well.
The direct effects of socioeconomic factors increasing the struggle to eat healthily in deprivation, such as relatively high prices for healthier foods (Darmon and Drewnowski, 2015; Jones et al., 2014) and differences in the relative availability of ‘junk foods’ (e.g. Maguire et al., 2015), have already been well established. Where practice-based theoretical approaches are well placed to add value is in illuminating the more subtle contextual factors which enhance these obvious differences in the ease of various eating behaviours. Since the turn of the century they have gained traction as an alternative theory of action (Schatzki, 2001; Lizardo, 2009; 714), viewing eating as a habitual social ‘practice’ made up of largely non-cognitive materials, meanings and competences and diminishing the role of rationality and intention in explaining what we do (Shove et al., 2012; Warde, 2013). This understanding of action has huge potential when it comes to understanding how contextual disparities affect the ease of eating unprocessed or ultra-processed foods. In providing a conceptual lens through which to understand the way that non-cognitive and habitual aspects of our lives facilitate and constrain our eating behaviours, practice-based approaches are uniquely well placed to illuminate the ways in which lab-based insights about limited cognitive control of eating might play out in complex real-world contexts of socioeconomic inequality.
However, there have so far been no studies which have used a practice approach to enhance our understanding of how socioeconomic inequalities play out in habituating (un)healthy eating – indeed, using practice approaches to understand or address socioeconomic inequalities has been noted as a lack in the literature (Walker, 2013). A large body of research demonstrates the importance of habit in eating (see van’t Riet et al., 2011), as well as the socioeconomic distribution of many of the non-cognitive elements supporting (un)healthy eating patterns (e.g. inequalities in meanings around healthy eating (Parsons, 2016), inequality of access to healthy foods (Cooksey-Stowers et al., 2017), inequalities in risk aversion around food waste and ultra-processed foods (Daniel, 2016), etc). However the potential for using practice theory’s joined up understanding of the non-cognitive determinants of habitual action in conjunction to improve our understanding of the socioeconomic distribution of effort and social justice has yet to be realised.
This paper will address this research gap by using a practice-based approach to better understand how socioeconomic inequalities affect the ease of eating minimally processed or ultra-processed foods, and how this underpins population-level inequalities in healthy eating. Based on in-depth multi-method research with 25 mothers living in two contrasting areas of Bristol and 310 mothers from the city who responded to a subsequent survey, we illustrate how the materials, competences and meanings which shape our eating practices tend to align more with the consumption of ultra-processed foods and make eating unprocessed foods harder for those living in deprived areas. After outlining our sequential mixed-methods research design we present and discuss our results in four parts: 1) reframing food preparation as a practice made of mostly non-cognitive elements, 2) focusing on differences in overlooked materials such as dining tables, 3) looking at differences in risk involved in developing competences for unprocessed food preparation, and 4) considering differences in meaning of ultra-processed foods in terms of their importance in providing comfort and care. Through these examples we demonstrate how the materials, competences and meanings which are more likely to be part of the practices of people living in deprived areas serve to systematically skew easy unthinking eating habits away from unprocessed and toward ultra-processed foods – increasing the relative ease of ultra-processed eating and exacerbating more apparent socio-material inequities.
Our study has important implications for public health policy around inequalities in healthy eating. The thrust of the majority of interventions is to teach people what to eat or how to cook, presuming that this will empower individuals to ‘take responsibility’ of their health and address unhealthy eating inequalities by consciously re-orienting or increasing their effort toward this end (Department of Health, 2014; 22; Brambila-Macias et al., 2011). However, if eating is habitual and predominantly determined by the social distribution of non-cognitive contextual elements rather than effort, then this reliance on individual capacities for control fuels a deep injustice – blaming those who are already most disadvantaged for the inequalities in effort and resulting preventable ill-health which taxes their wellbeing and takes years from their lives.
There is no evidence to suggest that more deprived socioeconomic groups think that ultra-processed foods are healthy or put less effort into eating fruit and vegetables - in fact here we present evidence suggesting the opposite is more likely to be true. The contention built up in this paper is that engaging with the underlying non-conscious tapestry determining which foods are the default easy to eat options should be the focus of anyone serious about improving healthy eating and addressing grave inequalities in this area. While limited capacities for voluntary control could hold the balance if the non-cognitive elements and practices you ‘carry’ make a range of actions almost equally easy, it is these non-cognitive factors which hold the real power over our behaviour. The space for agency is created through largely unthinking practices, which determine what is easy or hard, possible or not. If the elements constituting our eating practices are not allied with healthy consumption even the best intentions will ultimately flounder.
Methodology
The underpinning of a practice approach is that if we are to stand a chance of understanding and changing behaviours effectively, we must pay attention to the non-cognitive, embodied and material elements which are often overlooked. As Nicolini writes, “practice always… needs to be made visible, articulated, and turned into an epistemic object in order to enter discourse” (2009; 200). Practices of eating are complex, multifaceted and substantially habituated into invisibility - no one actor or method has an adequate vantage point from which all of the elements involved in practices become visible.
Overview of key features, purpose and support for research tools used.
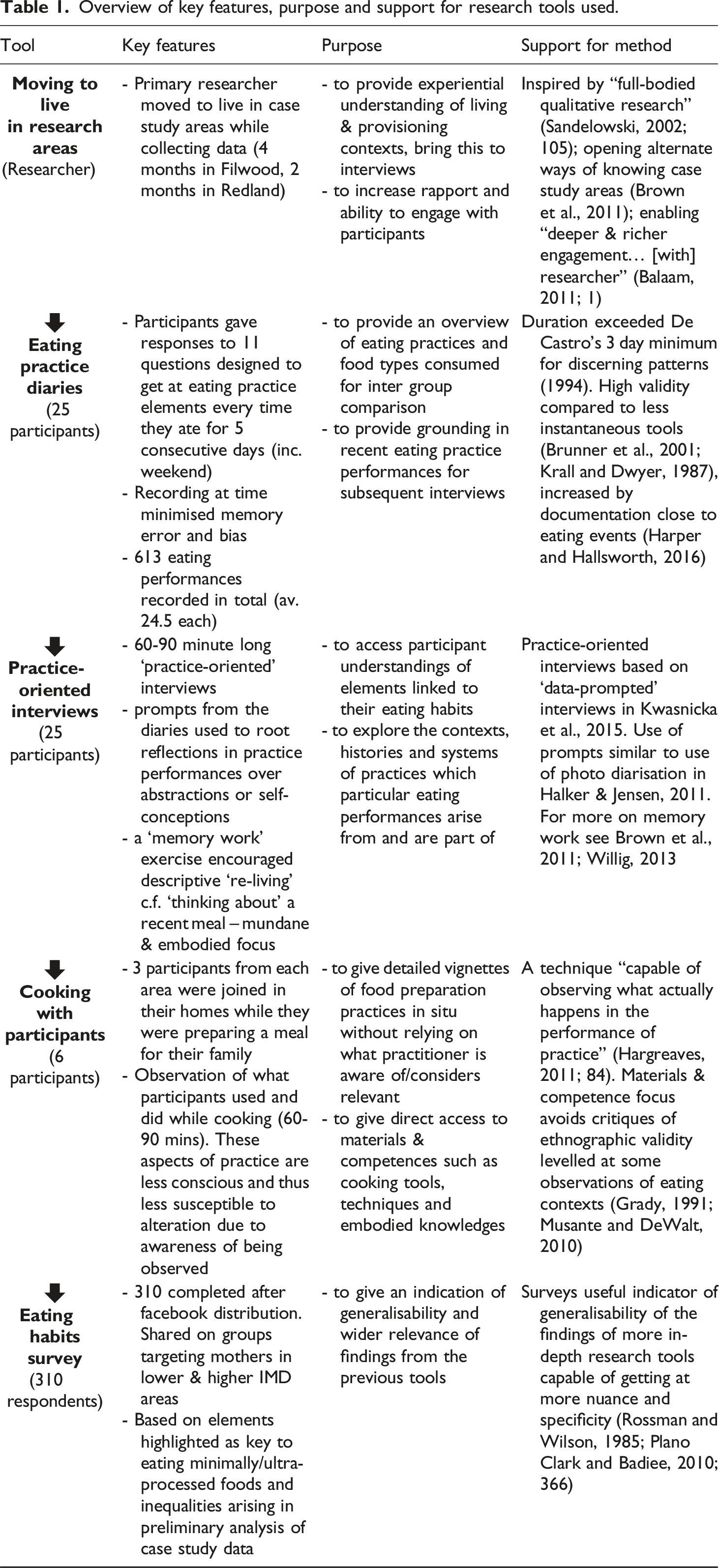
While interviews were still a major part of the research design, they were grounded as closely as possible in actual practice performances through the use of prompts from data collected from preceding tools (eating diaries, grocery receipts and living in the area) and using ‘memory work’ techniques which encourage participants to descriptively re-live an instance of eating rather than explaining it (Brown et al., 2011). All participants were provided £40 compensation to value their time and contributions, and those who participated in the cooking observations were provided an additional £15. Survey participants were paid £5 each in Amazon vouchers or Paypal credit as an incentive.
As eating inequalities were a key focus of the research, we used a comparative design to provide insights into eating habits at both ends of the socioeconomic spectrum. The majority of the research involved 25 mothers of young children living in Bristol, from the electoral wards of Filwood (n = 10) or Redland (n = 15). Mothers were chosen as parenthood is an important time of eating habit change and reproduction (Laroche et al., 2012; Reczek et al., 2014; Schäfer et al., 2010) and mothers still tend to be more central to household eating than fathers, shaping not just their own practices but also those of the next generation (Carrigan and Szmigin, 2006; Davison et al., 2020; Draxten et al., 2014; Elfhag et al., 2008). Focusing on just mothers (rather than also including fathers) also simplified the comparison between the different areas under consideration. Participants were drawn from two areas of Bristol representing very different levels of deprivation according to the Index of Multiple Deprivation (IMD), with local council data also demonstrating stark differences between these areas in a host of other wellbeing-related indicators (Bristol City Council, 2017a, 2017b). For instance, despite less healthy alcohol drinking habits, women in Redland lived 5 years longer than those in Filwood and residents reported a lot less health problems: almost three times fewer were living with a long-term health problem, half as many died before 75 from cancer and 25% less from cardio-vascular diseases (Bristol City Council, 2017a, 2017b) - conditions which have strong links to diet (Anand et al., 2008; BMA, 2016).
In keeping with their approximately 90% white ward profiles, only two of the 25 participating mothers were non-white (Bristol City Council, 2017a; 2017b). Apart from one single mother and one who had a non-resident partner, all of the participants were living with long term partners and all had 1, 2 or 3 children under 8 years old, with over 80% having at least one child under 5. The mothers ranged in age from 24 to 47, being slightly older in Redland than Filwood (means of 37 and 34 respectively). Redland participants were much more highly educated (87% degree or above c.f. 30% Filwood), more likely to own their own homes (80% c.f. 50%), more likely to be employed (73% c.f. 40%) and were all in (or previously in) ‘white collar’ professions.
The survey data came from 310 mothers living across the whole of Bristol, recruited through postcode-specific Facebook groups. Responses were skewed toward those from areas of the city with higher average income and education levels (200 c.f. 110) as responses from more deprived areas were harder to achieve and came in much more slowly (in keeping with the findings of Bonevski et al., 2014). Despite this bias, the numbers of respondents from the underrepresented lower income and education respondents was still high enough to achieve statistically significant differences between many of the variables measured.
Throughout the paper, the categorisation of ultra-processed foods as ‘unhealthy’ and minimally processed foods as ‘healthy’ is used, following the work of Carlos Monteiro (Monteiro et al., 2010). In this categorisation, ‘ultra-processed’ foods are those mass produced through industrial processes, and tend to be characterised by being high in fats, salts and sugars and low in fibre, micronutrients and phytochemicals (Ministry of Health of Brazil, 2014; Monteiro et al., 2010; Moubarac et al., 2013, 2014). This contrasts with ‘minimally processed’ foods “obtained directly from plants or animals… (e.g. fruits, vegetables, milk, eggs)” and ‘processed’ ingredients and foods (such as oil, sugar, cheeses, cured meats or simple bread) – which are all grouped together under the term ‘minimally processed’ in this paper from here on (Monteiro et al., 2015; 2313). Foods in the ultra-processed category have been linked to increased risk of diet-related non-communicable diseases (Rauber et al., 2018) as well as weight gain and obesity (Canella et al., 2014; Juul and Hemmingsson, 2015; Mendonca et al., 2016; Poti et al., 2015) with the nutritional content and ‘convenience and rapidity’ associated with consumption of these types of foods favouring consumption patterns which impede ‘mechanisms that regulate energy balance’ (Monteiro et al., 2010; 2047). Being around a third of the price per calorie of less processed foods (Jones et al., 2014; Wiggins et al., 2015) ultra-processed foods have been steadily replacing minimally processed foods over the last four decades (Monteiro et al., 2010). They dominate supermarket shelves in high income countries (Monteiro et al., 2018) accounting for the majority of price promotions and over half of the calories sold in the UK (Which, 2016; Health Select Committee, 2017; Monteiro et al., 2010). Although this is a somewhat crude and simple categorisation we believe it maps well enough onto nutritional content definitions of health to serve as a ‘healthy eating’ rule of thumb for this paper (Poti et al., 2015).
Results & discussion: Inequalities in the ease of eating un/ultra-processed foods
Analysis of data from the eating practice diaries showed a large discrepancy between the two case study areas in terms of the percentage of eating occasions which were predominantly minimally processed foods and those which were dominated by ultra-processed foods. In both groups, snacks were much more likely than meals to consist of largely ultra-processed foods (85% Filwood c.f. 64 % Redland) and Filwood mothers ate marginally more snacks than Redland (2 c.f. 1.7 per person per day), but the inequality persisted even when these were excluded from the analysis, with Filwood recording eating minimally processed foods substantially less (12% c.f. 26% of their meals) and ultra-processed foods more frequently (68% c.f. 49% of their meals) over the 5 day period (see Figure 1). Minimally and/or ultra-processed dominated meals by area.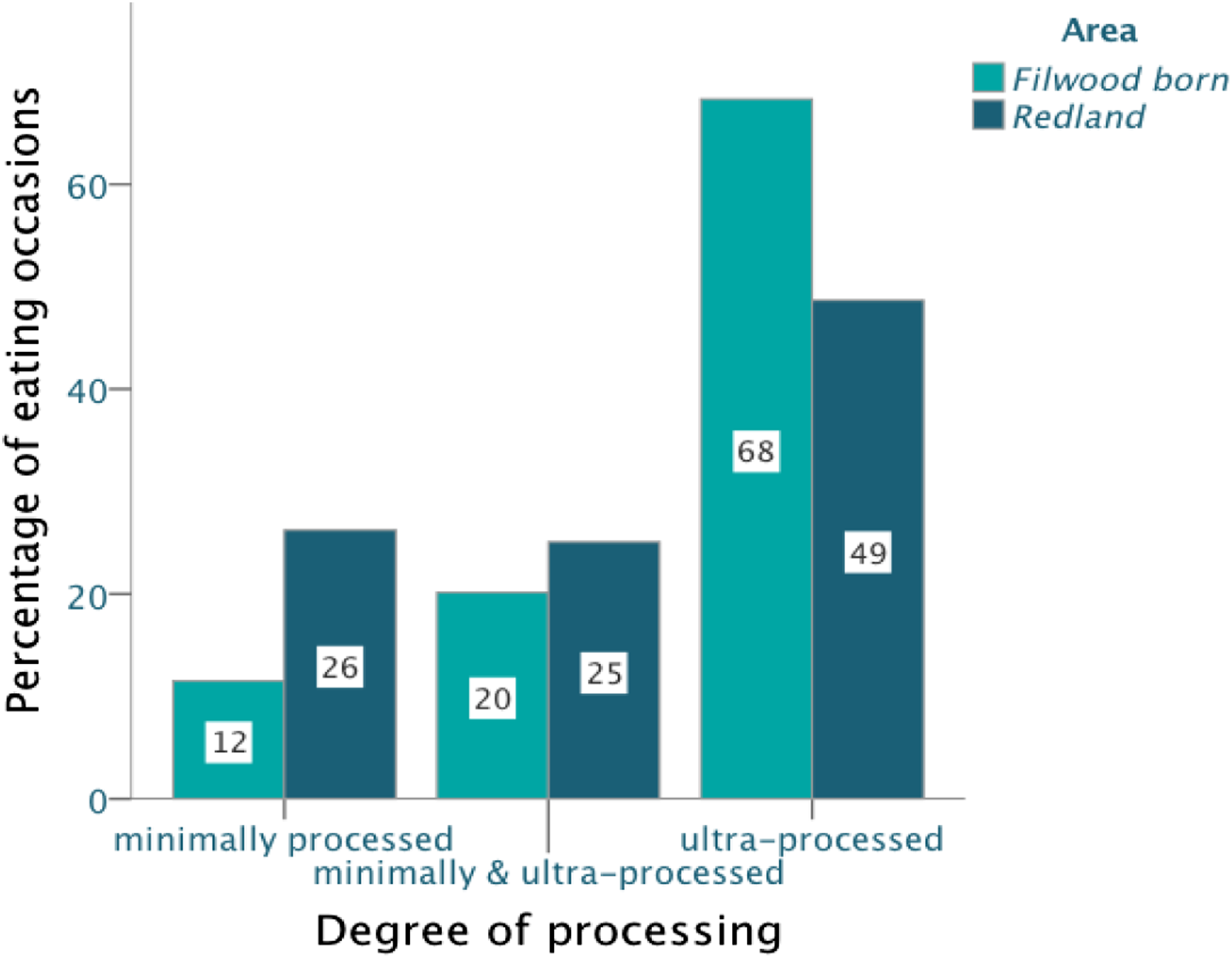
What might explain this divergence? Through combined analysis of the cooking observations, interviews and findings from the wider survey, the rest of this paper will illustrate how food consumption practices are made up of many elements beyond individual intentionality and how different socioeconomic distribution of these elements (i.e. meanings, competences and materials) affects the ease of minimally processed food preparation.
From voluntary to involuntary: The materials, competences and meanings underlying ease
Several times during the interviews and meal preparation observations, participants mentioned ‘reading recipes’ as the way they had learnt to cook dishes they made – but this understanding is in itself a perfect demonstration of how much our awareness is limited to the rational and intentional determinants of action over the vast web of involuntary elements which underly them. For instance, Maria was baffled at how hard her husband found it to make a simple pasta sauce from instruction: If he wanted to cook spaghetti Bolognese and I bought him a tin of tomatoes, tomato puree, onions, mushrooms, oregano, garlic – he would get all confused and be like ‘I don’t understand how to make the sauce’ – even if I tell him like 100 times!
Whereas, in contrast, she talked about being able to cook something she had never made before by just looking up a recipe – as when she needed Yorkshire puddings to go with her Sunday roast but had run out of the ready-made ones she normally used. However, her detailed description of that cooking occasion reveals how small a part of this process the recipe was: I just didn't know how to make Yorkshires… [but] remembered that the other weekend I'd seen my mum make Yorkshires, so I... just looked in these cookery books that my mum bought me…I had the tiniest bit of flour, and I almost added it to the last thing I made… so just read the recipe and I made my first ever Yorkshires from scratch – I was like ‘oh my god, this is so easy, I’m going to do this all the time’… but while we were stirring it I was like, [makes effortful noise] cos we don’t have a whisk so we were doing it by hand and I know that things take way longer and I didn’t know what it was meant to look like and it looked too runny and I was like ‘I remember my mum saying the oil has to be hot’ and I looked in the recipe and it said ‘make sure the oil’s hot’ so I said ‘I think there’s something really important about the oil being really hot’ so I did it, and I was pouring this really runny mixture that I thought should look way thicker and as soon as I pour it in the really hot oil it just goes [makes erupting/exploding noise] and I was like ‘yeeah!!’ But I didn’t realise that if you cook Yorkshires from scratch they take like 15-20 minutes, not like from a pack when they take a few minutes to heat up cos they’ve actually already been cooked, so I put them in at the last minute – everything else is ready and we’re like that: ‘come on Yorkshires!’
From this account it is clear that making her first ever Yorkshires involved a whole host of elements beyond reading the recipe - having a practice exemplar in her mother who showed her it was possible, gave her recipe books and told her about the importance of hot oil, having the ingredients around because she cooks other things from scratch, fitting the recipe instructions into existing knowledge about thickness of batter and hotness of oil, knowledge that the thickness of the batter matters, having a hand whisk, having a family who accept dinner taking longer, feeling excited about the end result, etc. Expressed in terms of materials, meanings and competences, the required elements included materials like having various ingredients around ‘because of the last thing I made’ or a hand whisk, competences like knowing their erupting was a good thing, or that she could substitute a hand whisk for an electronic one and that this would affect timings and meanings such as the understanding that Sunday dinner requires Yorkshires or believing she is a competent cook (so confident to go for it even if it doesn’t look right).
Thus, bringing the Yorkshires to the table was made possible by a wide range of involuntary materials, competences and meanings - the distribution of which are shaped by contexts of deprivation rather than willpower. These will be considered in turn in the following sections.
Materials: The alliance of suitable tables and unprocessed eating
Materials of eating are perhaps the elements of eating in which inequalities with socioeconomic deprivation are the least surprising. Differential abilities to acquire material elements of healthy eating are often directly tied to the economic contexts of life. Much has been written about the much higher relative expense of unprocessed foods per calorie (Darmon and Drewnowski, 2015; Jones et al., 2014) and the much higher relative availability of ultra-processed foods in poor areas (Cooksey-Stowers et al., 2017; Maguire et al., 2015; PHE, 2018a). The areas in our study were no exception to these patterns, with a much higher relative density of fast-food relative to full-service restaurants in Filwood (9:0 c.f. 19: 28 in Redland) and a much higher proportion of food retailers in the ward being convenience stores selling few minimally processed foods (41.3% c.f. 10% in Redland) (FEAT, 2017). However, as these have been well documented, we want to focus this section on the micro-scale materials in our homes which play a potentially large role in determining which food types are easier or harder to eat (Wansink, 2011, 2016; Wansink and Van Kleef, 2014). For instance, having access to specialised equipment like a bread-maker took on some of the effort of unprocessed food preparation for Katherine, and having a dishwasher she “couldn’t live without” and a tumble dryer enabled her to “just chuck [dishes/clothes] straight in,” thus freeing up time and energy for more involved food preparation practices. On the other hand, in Filwood, Katie not being able to afford to change her old electric hob which is hard to adjust and makes cooking slower hinders her frequent performance of involved cooking practices.
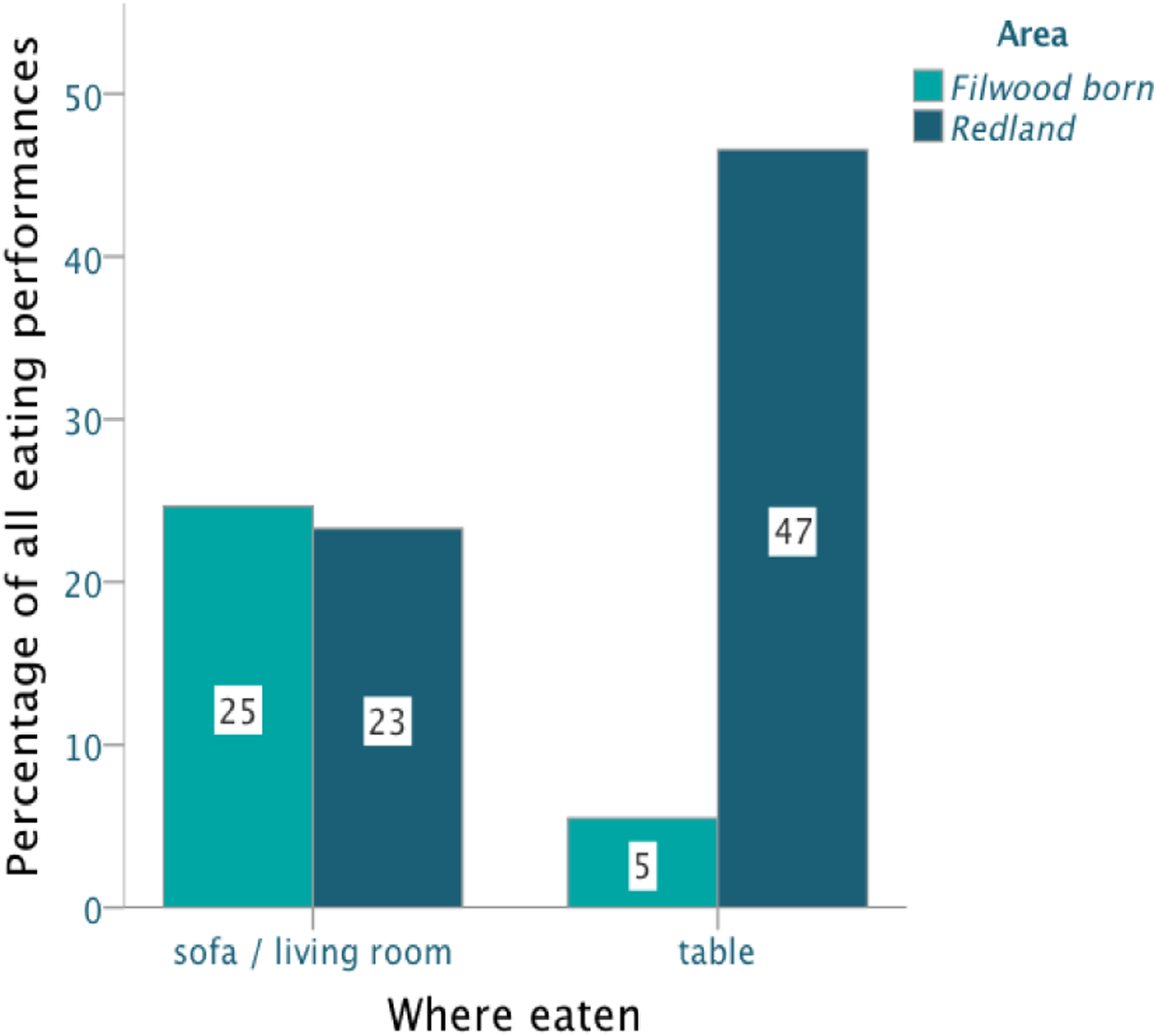
One material element which the eating diaries found was particularly strongly linked to whether participants ate minimally processed or ultra-processed foods is whether they ate at a dining table compared to on a sofa or in the living room (see Figure 2) and this corresponded with a large difference in the number of meals eaten around a table between the two areas (Figure 3). Where participants ate different types of foods. Eating occasions on sofa or at table by area.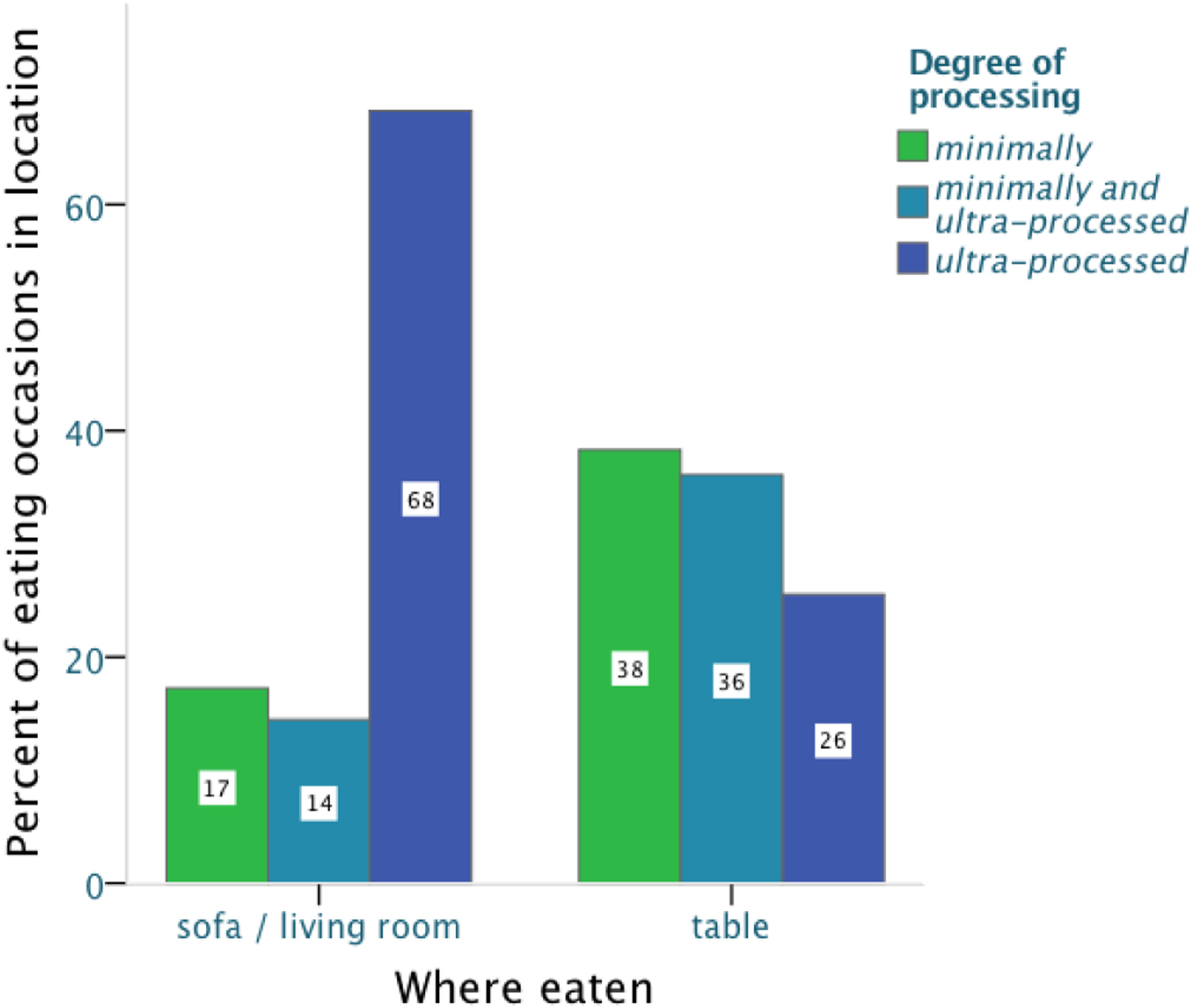
While it was commonly held that shared meals and eating around the table with family are good things, so too was the perception that it can be demanding trying to establish and uphold standards of proper table eating while children “run a train track across the table… or shout things at each other, or pour their drinks into their food” (Rosie, Redland). The strength of the norm or sense of importance of eating around a table given these challenges might vary by area, but “social practices are… always embedded in material arrangements” (Shove et al., 2015; 274) and the impacts of mundane material differences in making it more effort for some to organise around a table than others should not be overlooked.
One of these differences was the suitability of the available tables for eating on. The Redland mothers all had at least one table which was the right shape and size for dining at, with enough dining chairs around it. Rachel (Redland) noticed from writing her diary that “we always seem to eat at the table. It just happens naturally… I was really pleased about that.” But this ‘natural’ ease was facilitated by having three table options for different occasions. Ruth (Redland) has a dedicated 8-seater dining table which the kids don’t also have to play at so they can eat there at any time, and Katherine’s house (Redland) has a whole room for eating in, with a large table dedicated to this purpose and enough chairs for the whole family, making it easy to eat family meals at it.
This is something many of the Filwood mothers lacked. Emily likes hosting, but otherwise her table stays folded up under a shelf in her kitchen “cos we’ve not got much space and we want room for kids to play” (Filwood). Katie’s one living space in Filwood has only a tiny pack-away kids table with two tiny kids chairs, increasing the relative appeal of convenience meals she can eat with her hands and “put by me on the sofa” over eating more elaborate cooked “meals like this [which mean] we’ve got to sit at the table cos of the mess.” As the sole table in her house it has to be used for everything and was necessarily messy each time dinner came around: her children drew on it with glitter glue and crayons as Katie cooked above them “I’ll put [the garlic bread] on the table if you clear your glue away!” Although far too small for an adult to sit at, it still felt like “it takes up a lot of space” and had to be moved into a different position before eating, and she “obviously… [didn’t] usually sit down to eat.” This socioeconomic difference in the availability and suitability of tables to eat on also came out very strongly in the survey. When asked about four table characteristics conducive to easy family eating 1 70% of the low income and education participants said their table had either only one or none of these traits – compared with the same amount of high income and education participants saying their tables had 3 or 4 of them. Almost a third the low income and education respondents answered ‘none’ as they ‘did not eat at a table’ compared to less than 10% of their high income/education counterparts.
Correlation of dining table suitability with effort of eating around the table with children, being too tired to eat at the table and reported enjoyment of unprocessed foods.
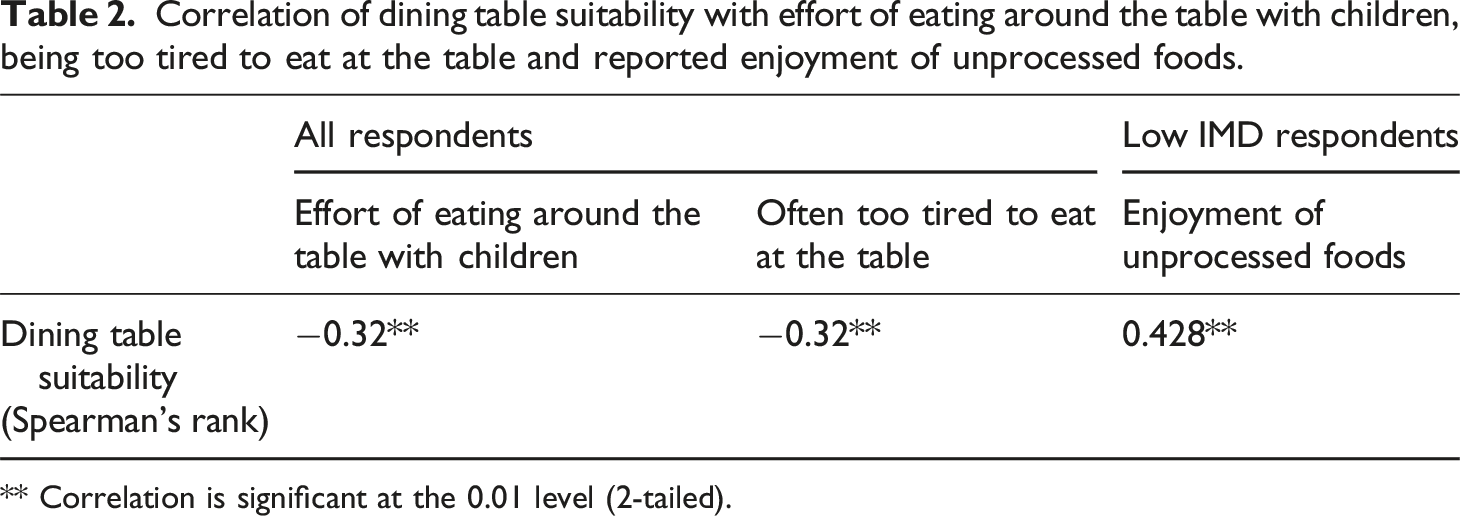
** Correlation is significant at the 0.01 level (2-tailed).
Although small, each seemingly mundane material inequity places a tax on every unprocessed meal occasion, making them that little bit harder. Eating at a table was experienced as an effort by most of the mothers, but the effort of such practices is unequal, as differences in the quality of mundane materials like tables illustrates.
Competences: minimally processed cooking fluency and relative risk
Correlation of cooking fluency with consumption and enjoyment of un- and ultra-processed foods.
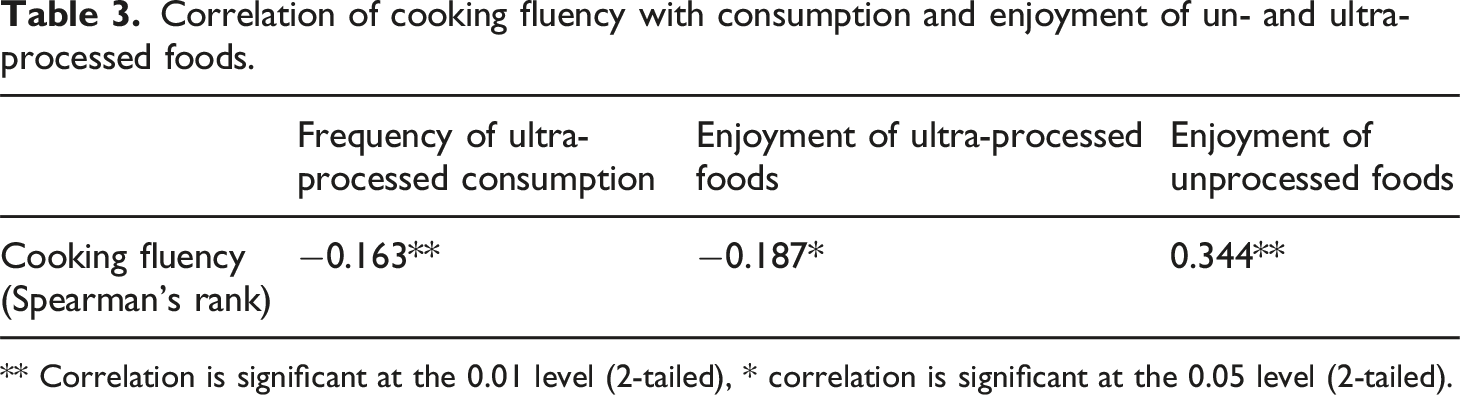
** Correlation is significant at the 0.01 level (2-tailed), * correlation is significant at the 0.05 level (2-tailed).
In interviews, mothers from both areas talked about specific techniques they had developed to make eating vegetables more palatable for themselves and their families: chopping the veg in bolognaise really small so her son would eat it (Ruth, Redland), grating otherwise unacceptably raw and crunchy carrots so their texture was more like cheese (Emily, Filwood), overcooking vegetables (Lucinda, Filwood), avoiding cooking vegetables (Rachel, Redland) or making sure vegetables aren’t mixed together (Maria, Filwood) - specific competences of unprocessed food preparation developed for particular circumstances over histories of experimentation. However, this process of ‘adaptation, improvisation and experimentation’ (Warde, 2005; 141) necessarily carries with it the risk of meals which fail, when, as Ruth (Redland) put it, “we all decide that they're disgusting and it goes in the bin.” Mothers recalled first attempts at cooking with tofu “I can’t eat that” (Liz, Redland) and trying new recipes which don’t “work out… [or] taste of anything I imagined” and have to be got rid of (Mariana, Filwood). But those who were able to persist found dishes which worked: discovering a curry with coconut milk in which they really liked tofu (Liz, Redland) or finding through “having a go” at several things that the sweet potatoes they disliked were much nicer mashed in combination with normal potatoes (Rachel, Redland). Such histories of experimentation with different vegetable preparations, ingredients and recipes lie behind the evolution of successful minimally processed practices which are a good fit for particular bodies, contexts and practice ecosystems and the unique combinations of these in each family.
Yet the repeated risks inherent in this experimental evolution, of meals which ‘fail’ or are rejected by members of your family, are obviously much more serious if your resources are already thinly stretched and you might struggle to replace meals if innovations on what you know fail to pass muster. Daniel (2016) found that sticking to feeding children foods they knew they would eat allowed low-income participants to minimise the risk of food waste, whereas higher-income respondents who were more able to bear the cost were less concerned with this and more likely to repeatedly try out new foods on their children. In our data, Katie from Filwood and Kathrine from Redland illustrate this difference well. In the context of Katie’s worry that her kids are “still hungry – it’s not enough,” cooking was more about being able to meet an essential need, a need which untested cooking practices could jeopardise given the very tight budget she was working within and which a whole host of her other living practices were competing to use. Katherine’s cooking experiments aren’t circumscribed by such stressful limitations – although her son can be ‘fussy’ about the foods she presents, it “doesn’t matter” as she can always provide something else for him to eat if he refuses it. With monetary constraints less of an issue, she sees cooking as something she can be creative with, enjoying going beyond feeding her family to making elderflower cordial and novel preserves for all 20 preschool staff. While both mothers believe in not wasting, in a context of risk Katie avoids waste by constraining what she buys and cooks to avoid waste where Katherine, without a strict budget, will freely accumulate and store surpluses, cooking excess to use it up and creating plenty to give away to friends and school teachers as “it’s nice to have an offering” - as with the excess of grown and bought rhubarb she was making into jam as part of our cooking observation.
These examples illustrate how scarce resources can be seen to structure a reluctance to experiment beyond ‘safe’ established practices and devote resources to developing competences through unproven cooking performances. Whether the investment in increasing the ease of unprocessed food preparation for potential long-term health improvements is worth the potentially costly risks of failed experiments will be strongly influenced by socioeconomic deprivation.
Meanings: the ease of prioritising ‘health’ in eating practices
It might be tempting to account for differences in eating minimally/ultra-processed foods in terms of differences in understandings of healthy eating, however this is counter to the findings of our data. When asked to think of healthy foods, virtually all in-depth participants shared sentiments like “fruit and vegetables… are my first thing” (Ruth, Filwood) and every one of the survey respondents gave minimally-processed foods as examples of their ‘go-to’ healthy meals. Further, none of the survey respondents disagreed that fruit and salad were healthy, and none agreed that the ultra-processed food examples were healthy. These findings and their lack of socioeconomic differentiation align with a host of other studies (e.g. Ares et al., 2015; Dressler and Smith, 2013; Paquette, 2005; Van der Horst et al., 2011).
Rather than a divergence in healthy eating ideas, what we found was a divergence in the ease of prioritising ideas of health over other meanings of food. For instance, although typically low in nutrient density, ultra-processed foods carry strong meanings of self-care or care for loved ones you feed (Meah and Jackson, 2017). Across all mothers the survey found that ultra-processed foods were most enjoyed when respondents might need practices of self-care: when their mood or energy was low, or they needed a treat. 83% of the respondents from both high and low IMD groups gave ultra-processed foods in answer when asked ‘What is your favourite food to eat as a treat?’ Similarly, when asked about when they enjoyed eating particular examples of ultra-processed foods, ‘as a treat’ was the most common answer, followed by ‘when I’m tired or down.’ While ultra-processed foods were associated with treating yourself and those you love across socioeconomic categories, conveying love and care through cheap and tasty ultra-processed eating practices is more necessary when resources for showing this in other ways are scarce (Vanderbroek, 2016).
When asked if there were other things that could play the comforting role of sugary treats when she’s had a hard day, Lucinda (Filwood) said “I’d probably just sit and veg out in front of the TV or something… and not do a lot. But if I had some biscuits out I’d just…” she mimed eating them all as a contented look spread across her face. Where after a hard week or a ‘bad’ day Emily (Filwood) “will just want to eat junk food,” Redland mothers are able to substitute a much broader range of more costly but less processed foods for their treat practices. Rosie (Redland) buys “lovely, but expensive… treat food” like ‘really nice olives’ or ‘truffle brie’ from the local deli, and Ruth (Redland) finds that “smoked salmon… makes me feel good because it's a treat… having little luxuries like that, that feel like a treat, then I don't necessarily think, “I need some cake.” Alternatively, they could also indulge in non-food treats - as one of the Redland mothers told me “I’m going to spend this [participation incentive] on a pair of new shoes… a treat for me” (Carrie, Redland). Ultra-processed foods can also serve as an inexpensive way to show love and care for children, and give them pleasures when scarcity limits other gifts, outings and experiences (Chen, 2016; Hendy and Williams, 2012; Pescud and Pettigrew, 2014). For instance, creating celebrations by giving the kids a McDonalds (Emily, Filwood), or making small joys in otherwise hard situations, as when Katie (Filwood) broke off telling me about how “I got robbed at knife point” to feed her kids smarties, chocolates and jellies.
When abstracted from everything else about eating, conceptions of health were simple: fruit and vegetables were first on everyone’s mind. However, in daily life nutritional health is just one among numerous other important meanings competing to constitute eating practices. Among this web of meanings deprivation tends to increase the role of ultra-processed foods in conveying comfort and care, making it harder to translate shared abstract healthy eating ideas into enacted practices.
Ingrained inequalities of ease: path dependence and the effort of deprivation
Far from those in poverty trying less hard to eat healthily, consideration of the underlying elements enabling different patterns of eating indicates that it is more likely to be the other way around. If your only table is two foot high and covered in crayons, it will be more effort to eat a home-cooked meal requiring a knife, fork and plate than an ultra-processed option needing only your hands and the sofa. The same is true for preparing a meal with unprocessed ingredients if the risk involved impedes the repeated experimentation needed to develop the related competences, or if you can’t draw from lived examples of what eating ‘5 fruit and veg’ really means in practice. These are some of the ways in which deprivation can be seen to systematically skew easy and unthinking default eating habits away from unprocessed foods, making it more of an effort to match abstract understandings of healthy eating with everyday consumption. As Sarah from Filwood describes, her experience of eating healthily is a constant effortful struggle of consciously trying hard, yet still often failing: ‘be good, be good, be good!’ … keep on the focus… I prayed a lot about my weight, about Slimming world – that God would give me the grace and the strength to stick at it… when I was pregnant, I didn’t care! I just ate whatever I wanted… That was a glorious 9 months!… that was the only time ever that I didn’t think about it, didn’t worry about it. Is that weird?
These inequalities in healthy eating effort multiply over time. Practices evolve “through the association of various combinations of elements and repeated performances over time” (Maller, 2015; 53), and over long life histories of cooking performance underlying inequalities in conscious effort involved in eating healthily are likely to multiply. The elements enacted in present practices participate in the formation of the elements available for future practices, multiplying inequalities and creating path dependence.
This inclination of practices toward path-dependence is further enhanced by the conditions of poverty which make it harder to deviate from established habits (Haushofer and Fehr, 2014; Mani et al., 2013; Sheehy-Skeffington and Rea, 2017). Resource scarcity and instability tax the cognitive system, with persistent juggling of insufficient resources and related stressors affecting the amount of attention and ‘cognitive-bandwidth’ available for practice innovation (Shafir, 2017; Zhao and Tomm, 2017). For instance, Katie in Filwood buys her Christmas presents in the previous year’s January sales, has her daughter’s birthday presents sorted 4 months in advance and pays for her party in weekly increments over months, juggling her expenditures under the ominous threat that “otherwise it’ll get there and I’ll have no money to pay.” Such unequal economic conditions unevenly consume people’s cognitive capacity at the most basic level (Arnsten, 2009; Evans and Schamberg, 2009; Middlemiss, 2003) increasing the effort of deviating from established practices among those in poverty for whom the elements of eating practices are more likely to be initially allied with ultra-processed foods.
Conclusion
This paper aimed to demonstrate that linking inequalities in healthy eating to differences in voluntary effort is unsubstantiated. Such differences are better explained by the varying extents to which our limited conscious capacities for controlling our actions are supported by the non-conscious factors which determine the bulk of what we do. Those living in socioeconomic deprivation only too aware of the gap between ideas of healthy eating (which they share) and their ability to live up to them, while the inequalities of ease they face in eating healthily remain hidden. So long as these unacceptable contextual injustices are obscured, inequalities in healthy eating can be passed off as justifiable inequalities of outcome caused by differences in willpower or healthy eating effort.
Understanding the social determinants of health through a lens of Practice shows how inequalities go beyond typical socioeconomic indicators to become part of the materials, competences and meanings of every action, shaping the unthinking default eating behaviours which constitute most of our eating performances. In this paper we have shown how deeply structural inequalities are embedded in the microcosms of everyday life by focusing on seemingly small inequalities affecting the ease of repeating ‘(un)healthy’ eating practices. For instance, our findings identify free experimentation with unprocessed food preparation, the integration of ultra-processed foods into care practices, possessing stores of relevant ingredients and having suitable dining tables as unequally influencing the health of eating at the level of reproduction of routines.
In so doing, we add an integrated understanding of effort and ease in the minutiae of everyday practices to the wide range of material and psychological factors affected by deprivation which have been shown to impact the health of what people are likely to eat (e.g. access to healthy foods (Cooksey-Stowers et al., 2017), healthy eating meanings (Parsons, 2016), risk aversion and food waste (Daniel, 2016), etc). This paper also goes beyond studies which have demonstrated the importance of habit to eating (e.g. van’t Riet, 2011) in considering how these habits are constructed and reproduced over long histories of situated performance where each repetition has been affected by subtle, socioeconomically striated, ease incentives and taxes. In doing so it uncovers a diversity of hidden non-conscious ways in which socioeconomic deprivation makes eating to protect your health harder, representing an unacceptable injustice to the most vulnerable in society. Rather than attempting to make individuals take high effort actions, the focus of interventions should be on making healthy eating easy and unthinking for all by increasing and equalising access to the elements of eating practices which are allied with minimally-processed foods.
Taking social, systemic practices as the site of intervention instead of individuated performances of practices erodes individual blame and makes it clear that healthy eating inequalities are socially created and probably inextricable from wider inequalities in life chances and circumstances. Although giving preference to such ‘upstream’ interventions is already widely supported by reviews of health policy effectiveness (Lorenc et al., 2013; McGill et al., 2015), this practice-based research can bring to bear a much-needed understanding of the power of automatic behaviours (Sheeran et al., 2013) and how they evolve in a gradual and ineluctable interaction with apparently minor and mundane-seeming aspects of social stratification. In so doing it suggests some new examples of what interventions could focus on at the level of practice. These could include addressing the micro-scale material inequities in dining table suitability, taking on some of the risks of repeated failures in cooking competence development (e.g. by reducing the money/energy costs of experimentation through free provision of unprocessed foods and the tools for processing them easily), or replacing abstract one-way healthy eating information provision with two-way support which engages with the specificities of what healthy eating coexists and competes with in complex lives.
This perspective challenges a deeply ingrained ideology and strong vested interests which depend on the illusion that actions are a product of rational choices and thus living healthily is an individual responsibility (Egger and Swinburn, 2010; Navarro, 2009). As Baum and Fisher point out “political actors with a strong commitment to neoliberalism individualism are very likely to be to drawn to behavioural solutions… Evidence is not likely to change the ideology of these actors [emphasis added]” (2014; 220). For instance, despite the power of the social determinants of health having been established for decades (WHO, 1978) there is still a tendency for health policy to ‘drift downstream’ toward the individual (Popay et al., 2010) and a review of European healthy eating interventions found two thirds aimed to support individuals in making ‘more informed choices’ rather than the changing the conditions underlying their actions (Capacci et al., 2012). This can be clearly seen in UK healthy eating interventions which focus on addressing unhealthy eating through ‘empowering’ “consumers… with better information about healthier choices… [to] stimulate demand for healthier foods” (Defra, 2022; 23) - placing the burden of responsibility squarely on individual ‘choices.’ With a few notable exceptions (such as the sugary drinks levy (HM Revenue and Customs, 2016) and some local authority initiatives using planning policies to restrict the proliferation of fast food restaurants (GLA, 2018)), the thrust of the majority of interventions has been to educate and motivate rationally choosing actors to change their eating habits with the strength of their own conscious willpower – despite limited evidence of the efficacy of such approaches (Brambila-Macias et al., 2011; Hyseni et al., 2015).
Changing eating behaviours by instruction in this way dangerously ignores the iceberg of non-conscious elements which determine the bulk of action, setting up those living in deprived areas for failure and blame in the face of largely unacknowledged discrepancies in conscious effort. Despite an increase in recognition of the ‘5 a day’ message (Herbert et al., 2010) the consumption of fruit and vegetables is well below the recommendations and still deeply unequal (PHE, 2021), the upward trend of purchasing ultra-processed foods continues (Monteiro et al., 2018) and obesity (linked to high ultra-processed consumption - Poti et al., 2015) is increasing across the globe (Jaacks et al., 2019). Diet-related ill-health has become the leading cause of preventable death and the gap in healthy eating between the richest and poorest people in the UK shows no signs of decreasing (Maguire and Monsivais, 2015; PHE, 2017a). We cannot carry on endorsing outdated educational interventions providing tips to make the ‘right choice’ and making increasingly irrelevant appeals to individual ‘willpower’, while allowing the prevailing social elements of practice to draw us, and especially the most vulnerable among us, towards overconsumption of the ultra-processed foods which are taking untold healthy years away from our lives.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.