
Abstract
While qualitative researchers on sensitive topics spend significant and important time assessing and mitigating risks for their research participants, there is much less focus on risks to researchers doing this work. Sensitive qualitative research requires researchers to empathise with participants talking about some of life's most challenging moments, and exposure to this can be deeply emotional and even traumatic for researchers. Researchers need a range of strategies to care for themselves throughout the research process. Currently, verbal and written strategies in line with researcher critical reflection and reflexivity are often advocated as key ways of mitigating the emotional impact of research. There is increasing evidence that arts-based approaches facilitate different kinds of reflections on emotional and embodied experiences. This paper describes how the arts-based method, body mapping, can be used by researchers to support researcher reflection on qualitative research. The process of creating, describing and reflecting on the embodied experience of doing the research through body mapping facilitated not only an engagement with the emotions elicited during the project but also illuminated absences and future actions. The paper provides clear guidelines for other researchers wishing to try the approach and also points to the need for institutional and structural responsibility for researcher health.
Background
In qualitative research, the focus is usually on risks to research participants (Pillow, 2003), with formal ethics processes in place to ensure their physical and emotional safety, and that research approaches uphold participant rights (Dickinson-Swift et al., 2007). This is necessary and appropriate. However, there is also an underexplored need to support the safety of researchers themselves (Dickinson-Swift et al., 2007).
Qualitative research is embodied – ‘an activity saturated with sensory, corporal experiences’ (Oreton, 2004, 305) – and requires empathy to understand, connect to and portray the stories of others (Jafari et al., 2013). As such, it can place researchers in positions of emotional vulnerability and distress (Dickson-Swift et al., 2007; Fenge et al., 2019; Jafari et al., 2013). This is particularly the case for research on sensitive topics such as grief, death and dying, sexual abuse, abortion, violence and marginalisation (Dickson-Swift et al., 2007; Fenge et al., 2019; Jafari et al., 2013), where it is not uncommon for researchers to feel guilt, sadness, powerlessness, frustration, anxiety and hopelessness (Woodby et al., 2011).
These researcher experiences can cause vicarious trauma (Taylor et al., 2016), particularly if the topic touches on things the researcher themselves has experienced (Michell, 2020). A term usually used in care-related professions, vicarious trauma refers to ‘profound psychological effects that can be disruptive and painful … and can persist for months and years’ (McCann and Pearlman, 1990: 133) and can result in re-experiencing the (research participant) survivor's trauma, avoiding or numbness to the trauma and persistent arousal (Nikischer, 2019). Researchers doing qualitative research on sensitive areas are at high risk of secondary traumatic stress (Whitt-Woosley and Sprang, 2018).
Despite the risks of engaging in sensitive research, qualitative researchers receive little training to address the emotional aspects of their work (Nikischer, 2019). Woodby and colleagues (2011) argue that this is largely because academic work is seen as a strategic enterprise, rather than a therapeutic one – with a clear goal to gather and report on data. There are some practical strategies for researcher self-care in qualitative research (spacing interviews out, maintaining boundaries with participants), with most strategies for managing researcher health and wellbeing couched in terms of researcher reflection and reflexivity (Cridland et al., 2016). Researcher reflexivity is a part of critical reflection that incorporates the researcher's positionality and is action-oriented (Adjepong, 2019; Anwar and Viqar, 2017; Berger, 2015; Kennedy and Gardner, 2021; Watts, 2019). Taylor (2019) identifies researcher reflexivity as one way a researcher can flag their experiences of vicarious trauma and provide an impetus to seek support.
Commonly cited methods for researcher critical reflection and reflexivity include: reflective journaling (Fook, 1999; Kennedy and Gardner, 2021; Sharma and Rickly, 2018), which may be written down or audio-recorded (as in Nilson, 2017); supervision (Kennedy and Gardner, 2021); and taking part in reflexivity groups (Fook, 1999; Leggatt-Cook, Sheridan, 2011) or participating in peer consultation (Berger, 2015). Despite the usefulness of arts-based approaches in therapeutic contexts, they are not often discussed as a form of research reflection or reflexivity.
Art-making can be an effective way for people to communicate aspects of their experiences that are difficult to describe verbally or in writing (Boekhoven et al., 2012; Van Lith, 2014). According to Boekhoven et al. (2012: 166), art-making allows people to ‘express themselves, unblock emotions … and circumvent the need for verbal representations’. Art-making for reflection also supports people to question perceptions and articulate intangible things that are important to them (Potash et al., 2015; Van Lith, 2014).
In this paper, I will describe the arts-based method of body mapping and how I used it to help me reflect on my experience doing qualitative research with people with late-stage dementia living in a dementia unit of a care home. I explain how body mapping not only supported me to understand the emotional impacts of my research but also offered opportunities for reflexivity potentially impossible with verbal or text based methods.
Body mapping as a tool for self-care and reflection
Originally used in art therapy, body mapping has been applied to research – particularly around the exploration and embodiment of sensitive topics (Boydell, 2020). Usually body mapping involves the participant lying on a large piece of paper in a position that represents how they feel about the significant event or series of events they are mapping. They are traced and then use colours, symbols, magazine cut outs, drawings and other art supplies to ‘map’ the event/s onto the inside, surface and outside the body. Facilitators usually guide the body mapper by inviting them to think about what was in their heart, head, stomach and so forth during the event being mapped (De Jager et al., 2016; Dew et al., 2018).
When I have used body mapping as a research method, participants often talk about how they have never told the story that way before and how it prompts different kinds of self-reflection, particularly around experiences of trauma (Smith and Senior, 2020; Collings and Smith, 2020). My participants have found body mapping integrating – allowing them to see how different aspects of their experience overlap and is contextualised (Smith and Dowse, 2019). Most importantly, they have loved seeing all of their experience on the one page, often inviting other people into the research space to ‘see’ them (Smith and Senior, 2020). In these exchanges I have noticed the power of body mapping to expose the ways in which the body keeps score (Van De Kolk, 2014) of complex and contradictory emotions and situations in our lives.
This paper reports on my experience using body mapping to support my reflections on a sensitive research project a year after its conclusion. The research project involved people with dementia and complex support needs who lived in a secure (locked) dementia unit in residential aged care facility in Australia. The project included a focussed ethnography about engagement of people with dementia living in the dementia unit, as well as the co-development of personalised scarfs and blankets that supported their engagement and connection, particularly during moments of change (Smith and Phillipson, 2021, 2022; Smith et al., 2023).
Doing body mapping for researcher health and reflection
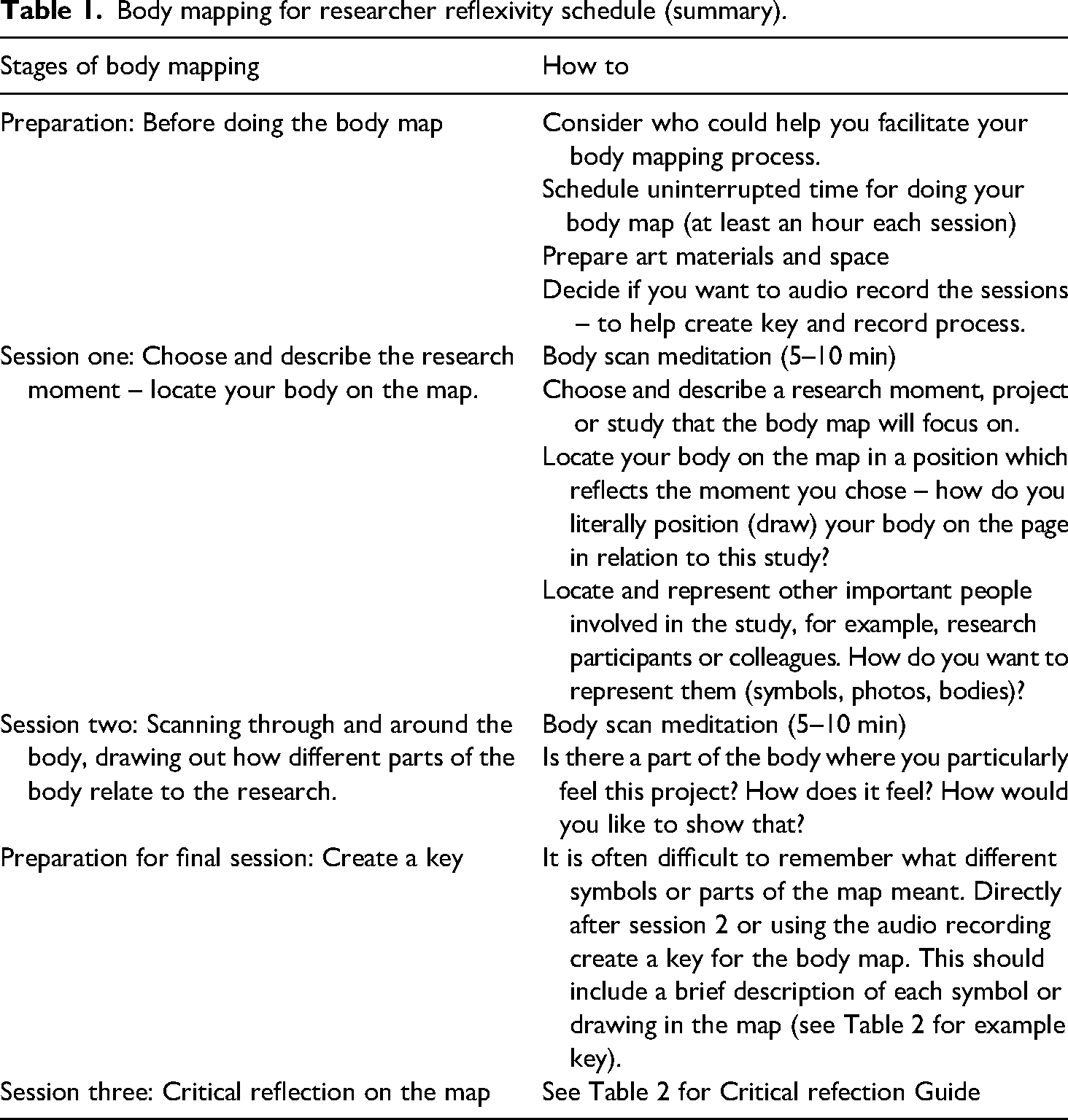
To conduct this body map, I developed a Body Mapping for Researcher Reflection schedule (the summary of which can be found in Table 1, contact me for more details). Creating and reflecting on the body map took three, 1 hour sessions, with some preparation time both prior to the first and last session. The first two sessions were for making the body map and the last session was for reflecting on it. My research assistant, Isabelle, who had been involved in body mapping before, acted as a facilitator for the three sessions. I audio recorded our conversation to support my reflection after completing the map. Due to COVID-19 lockdown restrictions, I converted the life-sized body map I created in my first session into an A3 one that could be used in my home office (see Figure 1).
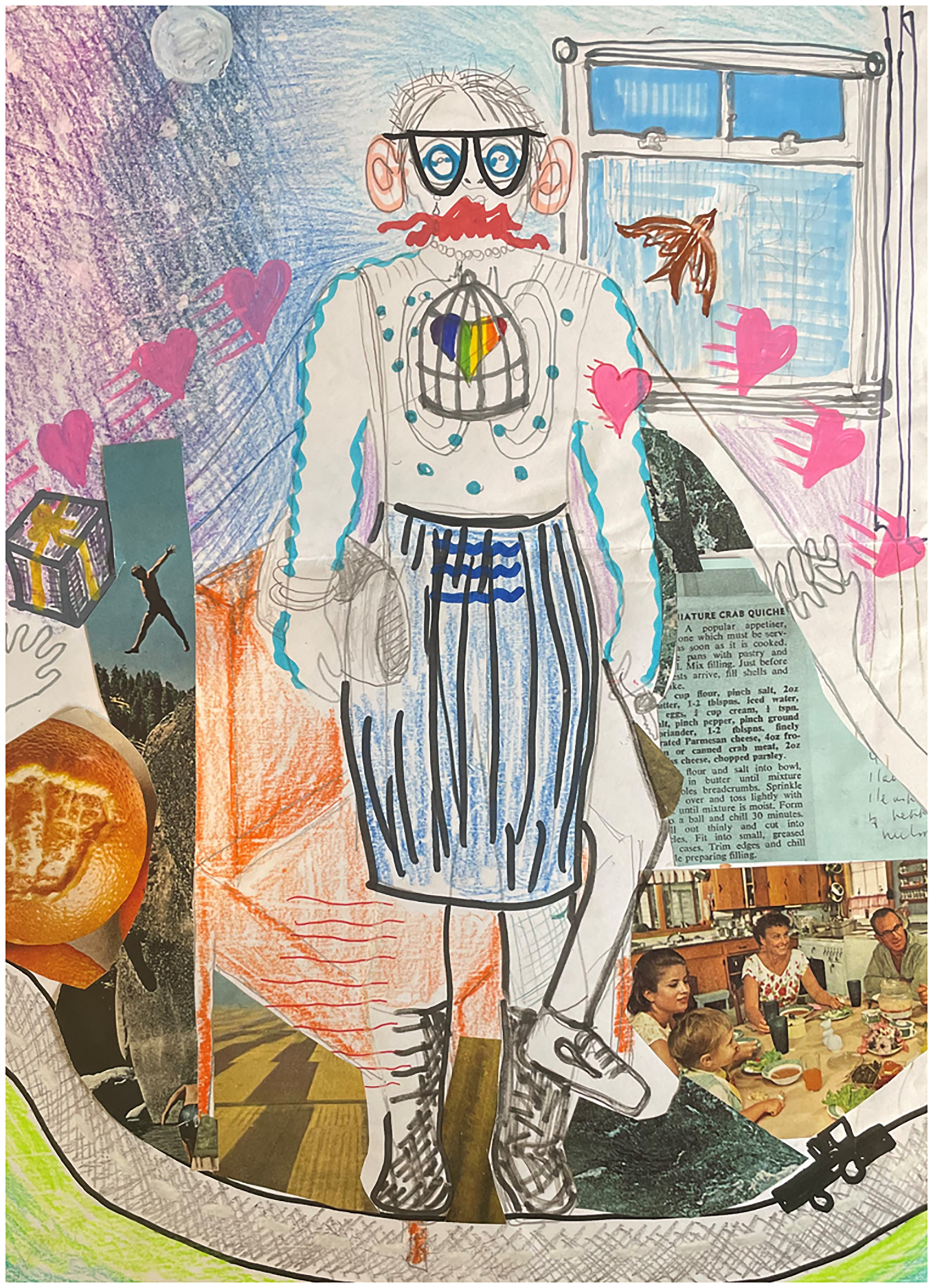
Completed body map.
Body mapping for researcher reflexivity schedule (summary).
In the following sections, I will explain my experience body mapping this research project and some of the issues that arose as I did so. The aim is both to illustrate the processes of body mapping and the issues that you can confront as you do it.
Session 1: locate your body on the map: choose and describe the research moment
As discussed above, I chose to body map my experience as lead researcher in a study with people living with dementia and complex support needs who lived in a dementia unit within a care home. This project was confronting and difficult emotionally, particularly because people living with dementia in this setting were not always supported to live good or meaningful lives. I chose to body map this project because it was one that was difficult for me to maintain my boundaries around. I felt deeply for the participants and their situation, and, as many of them did not use speech to communicate, we developed research methods that involved interactions usually associated with emotional intimacy – such as touch, singing, sitting together and making things together. In addition, due to COVID-19 restrictions, the project ended abruptly; it felt unfinished. I still thought about the participants often and wondered about whether they were still alive and if they were being treated with care. In Session 1, Isabelle said, ‘You’ve done some thinking about this already’ and I replied, ‘I haven’t gotten inside it…it's still sitting in me.’ Getting ‘it’ – the project, the feelings – outside of me was one of my main motivations for doing the body map.
I couldn’t settle on a way to position my body in the body map. I wanted to show myself reaching out – making an offer to the participants living with dementia. But I also wanted to show how much time I spent sitting on horrible vinyl chairs – sticky and disconcertingly wipeable. In the end, I drew my body doing both these things, and as the body mapping session went on, I added arms and changed the shape of my legs to show other things that were important: what I was holding on to (my keys, my hand bag, people's hands); what I was offering (a gift); what I was taking (a gift); and what I was trying to avoid (feeling trapped). I knew before Isabelle traced my body that I didn’t want the outline of my body to be complete – half my leg outline is absent. I wanted to show that my body felt leaky, and what leaked was not just my emotions (my love and my grief) but also myself. I will come back to this.
I then added the research participants to my map – the people living with dementia. I represented them as hearts with streaks behind them, the hearts to emphasise the importance of deep connection for so many of them and the streaks to show their long histories. I immediately drew my own heart on my sleeve, to show how I felt like we connected with real intimacy, dropping lots of pretexts usually found in meeting new people and instead joining together quickly by holding hands, dancing, singing songs and crying.
Already, in Session 1, doing the map with Isabelle's facilitation was helpful. She practically collaborated with me on making the large map: doing the outline of my body and asking if I wanted help colouring bits in. She also checked in on me. Knowing I had a meeting following the session she asked, ‘Do you feel like you want to dive into things before your meeting?’ This is deep and sensitive work – it helps to have a witness and a guide.
Session 2: scanning the body and around it
In the interests of space, I will not describe everything on my body map here. I will, however, give you a few glimpses of the process and how it unfolded, including the prompts that Isabelle, as facilitator, helpfully provided.
For me the mapping began on my face, with the big eyes, glasses and ears which all represented me trying to be an ethnographic sponge. I felt this tremendous responsibility to bear witness to what was happening: to witness the pain of others. I drew my eyes like the arrows of the refresh sign on a computer, this attempt to constantly stay fresh, awake and processing. The squiggly lines on my skin and in my stomach showed my nervousness at capturing it all, at being able to do the participants justice.
My clothes were really important throughout my fieldwork in this project. I drew a pencil skirt and a polka dot silk top which I bought specially for the field work. As the project progressed I wore more and more 1940s and 1950s style fashion. This is not my usual style but the participants loved it. Some of the women asked to try on my clothes and jewellery, one of the men said my ‘dress was an accomplishment, especially in these times of war’. The participants’ enjoyment of my clothing fed directly into my eventual choice of material research methods for the PAR project (Smith and Phillipson, 2022; Smith et al., 2023).
But while becoming central to my methodology, my dress was also moving further and further away from how I recognised and usually represented my queer self (no leather jackets or short hair here). This led me to draw a rainbow heart trapped in a bird cage inside my body. This dementia unit was not a place to be a queer woman. I couldn’t come out, people asked about my husband and I nodded and stayed silent (as my not-wife ran around at home after our kids). Dressing this way, while pivotal and playful also felt like a kind of betrayal, not just to me but to everyone else – including to any of the people living with dementia who were gender and/or sexuality diverse and couldn’t risk being seen in the locked dementia ward either.
Outside my body what I drew contrasted to the oppressive and intimate images that were on and in it. I drew large wide skies, for stars and birds to fly in. Open windows and roads. Trucks or U-Hauls to carry everything, even you, away in. I collaged the rich histories of my participants behind me, because I felt as if their histories were somehow mine too. Because I was the one listening, I became their custodian.
Session 3: making sense of the map and pushing it forward
To critically reflect on the map, I developed a series of questions based on standard structure for critical reflection (Fooks and Gardner, 2007; Watts, 2019). These questions are represented in Table 2.
Guide for critically reflecting on body map for researcher reflexivity.
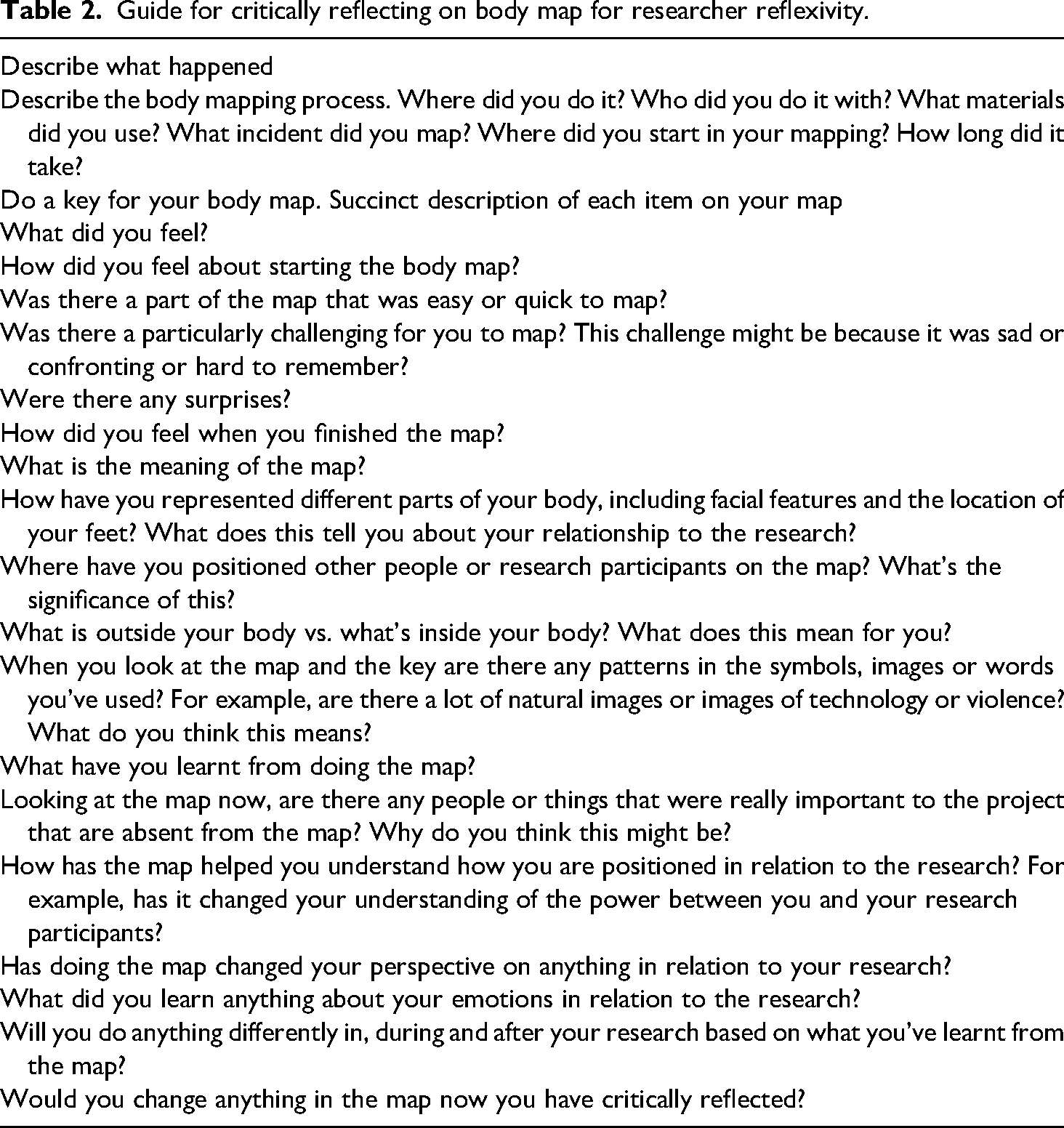
Throughout the body mapping process, I began addressing these questions in my discussions with Isabelle, however, working systematically through them a week after I completed the body map was useful. To do the critical reflection, I not only looked at the body map, I also went back and listened to sections of the audio recording from the body mapping sessions. I will discuss more about what I discovered through this process in the next section, but it is important to note that this process was particularly helpful for me to locate the absences in the initial map and in my reflexive processes to date.
For example, when I listened to the audio recording about the body mapping session, all I could hear was rage. I was raging at the injustice of the ways in which we ‘care’ for people at the end of their lives. Raging about the unmet needs of people living with dementia in dementia units. Unmet needs sounds too clinical. I was raging that older people remain literally unmet, alone, isolated and unknown, while often yearning to connect. As I listened to myself, I felt the rage as a red intensity in my throat, but it was absent from my map. As I added red lines onto my map, I considered ways in which I had spoken to this rage in my research project, but also ways in which I’d sidelined the rage for academically and personally acceptable outputs. That's why I didn’t include it on the map. But following that rage seems like a useful way forward, and I’ll discuss how I’ve begun to do this below.
In addition to locating this rage, critical reflection also made me uncomfortable about other absences. In particular, the ways in which my whiteness did not come up explicitly in my mapping process. Even with the literal centrality of my white body on the page, I did not mention it until the critical reflection. This is despite the ongoing impacts of colonisation in Australia, Australia's cultural diversity and the migrant workforce which dominates aged care. Not drawing this out in the body map highlights the ways in which while the body map helped me explore certain forms of corporeal discomfort, silence or absence that immediately related to aspects of my identity – particularly if I felt them threatened (my sexuality, my freedom) – it did not help me identify or literally draw out the discomfort, silence and absence around the identities of others who may have been in the space.
What did I learn from this process of researcher body mapping
As discussed in the introduction, I had engaged in reflexive processes throughout this study. I’d kept a research journal, had debriefing sessions with my colleagues and followed Braun and Clarke's (2019, 2021a, 2021b) processes for Reflexive Thematic Analysis. This was useful for helping me question my assumptions about the research data (Braun and Clarke, 2019) and improve the accountability and trustworthiness of the research – a core aim of reflexivity (Finlay, 2002; Lazard and McAvoy, 2020). Body mapping and the critical reflection about it, helped me push my reflexive practice further. Literally centering my body did two things. Firstly, it allowed me to engage with my own emotional and embodied experience of the project and put that on a page. But secondly, by seeing myself drawn there surrounded by my depiction of the research, I could ‘step back and take a long view’ (A Prayer of Oscar Romero). I could not only see my position but recognise how my location in the research obscured parts of myself (my queerness, my whiteness) and, in the process, obscured other people too.
Just like many of the research participants who I’ve used body mapping with, I found it very useful to see my experience represented in one place. It helped highlight the emotional and embodied tensions that I experienced as a researcher; the deeply material and sensory nature of the research (Oreton, 2004) and its intimacies (holding hands, secrets and gifts), as well as big uncomfortable and distancing feelings like guilt (at not having done enough, at wanting to leave), responsibility (to see it all, to do something about what I see) and rage (that this is happening at all). These things, they all happen at once, and seeing them overlapping as they did on the map was ameliorating. Moreover, the way these tensions came to rest on the page of the body map and in my reflections that followed solidified and motivated research plans and actions that otherwise may have remained ghosts.
One example of this was in the power of finding my rage, and tracing that rage through my body, back through the project and then forward into new research possibilities. When I started the project, my rage at the everyday harms in the locked dementia ward were so intense that I could barely speak about them. I remember crying in a very small office with two senior colleagues who had pulled me aside to check on me. But once I started to implement my action research, my anger was transformed into the urgency of getting something done, of addressing injustice. Doing the body map not only made me relocate my rage, it also helped me recognise how it intersected with my own embodiment, in particular around old rage about expressing my sexuality. Hiding my sexuality in residential aged care was uncomfortably familiar. It prompted me to consider the lives of LGBT+ older people living with dementia, who have experienced lifetimes of discrimination and found themselves in a place where no one was affirming their identity. Someone in my study might have been LGBT+, I’ll never know.
The reignition of my rage through body mapping motivated me to take up a new program of research around supporting LGBT+ people living with dementia. In addition, the critical reflection process on the body map also allowed me to see that only tracing my rage through my embodiment failed to recognise other kinds of marginalisation – such as the experiences of Aboriginal and Torres Strait Islander older people or those from migrant or refugee backgrounds. This is not a separate project, and I’m thinking deeply now in my research plans around how to incorporate this understanding from the outset. Ironically, while this reflexive process involved me putting myself in the centre of the page, it has actually pushed me out by allowing me to know my limits and seek collaborations to address them.
I think it is worth noting that despite seeming straight forward and simple, this paper has been difficult for me to write. Core to this difficulty was centring my body and my experience, when a driving aim of my research is to amplify voices not often heard and in so doing promote change. It feels self-indulgent. I have persisted because when I started out as a qualitative researcher doing research on young people with disability, I was immobilised by the data collection, transcription and analysis. In retrospect, I experienced vicarious trauma, but I had no awareness around this and nor did those I was working with.
My struggle in writing this paper is in many ways also indicative of the institutional and structural failure to recognise a responsibility to the needs of qualitative researchers. Engaging in processes like the one described in this paper should not be a reactive personal attempt to regain equilibrium and wellbeing, it should instead be built into researcher training, formal ethics processes and human resource approaches with qualitative researchers.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received funding from the Dementia Australia Research Foundation and the Medical Research Futures Fund.
Author biography
Louisa Smith's research explores the intersection between disability, dementia and complex support needs. Louisa has a particular interest in research that actively develops supports for those who are most socially isolated, including people with disabilities and/or dementia who experience gender and sexuality diversity, live in large residential accommodation or are from refugee backgrounds. Louisa's research works across the disciplines of sociology, disability and dementia studies and policy studies, with a particular focus on inclusive and participatory methodologies. Louisa's current program of research focusses on Participatory Action Research approaches to co-develop and co-design resources to support people with disabilities and dementia and complex support needs. An example of such work with people with dementia is documented in this short video: https://www.youtube.com/watch?v = LI721G6ORN8&feature = emb_title