
Abstract
This article mobilises Heather Love’s writings on description to provide a novel analysis of recovery from drugs and alcohol. It discusses thin descriptions deriving from the presence of the researcher in the recovery space, and the service-users’ thick descriptions of their recovery experiences, produced through one-to-one interviews and photovoice. Thin and thick descriptions of recovery are brought together with the Deleuzo-Guattarian assemblage, for the provision of an insight into the practice of recovery that focuses on its daily crafting through small practices of care. Observing and describing how phone calls and text messages, assessment forms, doorways and art materials inform the generation of caring practices, recovery is reconfigured as an amalgam of small gestures that gradually expand life possibilities. This epistemological and methodological shift has the potential to unsettle the way we understand and do policy, and to re-think it as a practice emerging organically inside the recovery assemblage.
Keywords
Introduction
In her paper ‘Small Change: Realism, Immanence, and the Politics of the Micro’, Love (2016) challenges the constitution of small-scale observations of everyday life as conservative, and she argues instead for the political utility of description at the micro scale. The question that traverses Love’s analysis is whether description and small-scale observation can change things, or if, as Goffman argues, the role of the sociologist is not to awaken people from their deep sleep, but to sneak in and watch the way they snore (1974: 13–14, cited in Love, 2016: 428). In this paper, I argue that the observation of small-scale practices of care can shift how we understand and do recovery from drugs and alcohol. Paying attention to service-users’ descriptions of the connections emerging in assemblages of recovery from drugs and alcohol, my aim is to draw attention to, and open up understandings of, the spatialities, temporalities and practices of care (Latimer, 2018: 380), that enhance the life possibilities of people in recovery.
Critical analyses have often situated recovery within a neoliberal system of thought, exposing a long-standing systemic disinterest in the needs of drug-using bodies (Fraser and valentine, 2008; Nettleton et al., 2013). However, they have also led to the production of a grand narrative, an interpretation of recovery that neglects its site-specific, daily crafting through small-scale, material practices of care. The analysis of recovery through a neoliberal framework reflects the focus of policy-making practices on the outcome of recovery, the production of recovered subjects in neoliberal worlds, rather than on the present of recovery and the life possibilities that it creates. Love’s analysis of description as a sociological method observing operations and interactions, rather than producing interpretations (2010; 2013), offers us the tools to think of and describe recovery otherwise; as a process where policy is produced in practice. Thinking with the politics of the micro (Love, 2016) and focusing on the description of small-scale practices of care (Puig de la Bellacasa, 2012) has the potential to shift the way we do and think about policy, as a practice that is not imposed upon subjects, but emerges through the daily crafting of recovery.
According to Love, good descriptions do not add anything ‘extra’; ‘they account for the real variety that is already there’ (Love, 2010: 377). Describing how material components of the recovery assemblage enhance practices of care reflects the commitment to account for the real variety present in spaces of recovery. In so doing, the aim is to challenge the interpretation of recovery as the reinforcement of a neoliberal way of being. I am interested instead in how the daily practice of recovery resists these systems of thought; how the description of the present of recovery matters, and how staying with the trouble of recovery (Haraway, 1988) in empirical research, extends beyond the recovery space and provides care-full ways of thinking about the connections we produce, and how these enhance life possibilities.
Engaging with recovery requires an acknowledgement that the object of our research is slippery. It encompasses infinite connections, difficult and neglected. The description of practices produced around objects encountered in assemblages of recovery and beyond, and the caring practices and connections that they enable, has the potential to unfold the complex thread of recovery. Observing and describing how phone calls and text messages, assessment forms, doorways and art materials inform the generation of caring practices, I challenge the dominant narrative of recovery as the process of disassociation of a body from a substance. By following the materiality and spaces of care (Latimer, 2018: 381), by observing objects, how they mediate relationships between service-users and workers, and enhance caring practices, I pay attention to the service-user’s descriptions of these objects and the new possibilities that they open.
Through the deployment of the Deleuzo-Guattarian assemblage (Deleuze and Guattari, 2004), a description of how this complex world of recovery is ‘really like’ (Love, 2013: 430) is set up. Assemblages are omnipresent and never fixed. They are mobile, being transformed as the connections that hold them together shift. They multiply in every direction; they are fluid, impermanent and complex (Delanda, 2016). Their applications are infinite and choosing to apply the assemblage theory on spaces of recovery entails the commitment to understand the recovery process as a transformative one, that does not simply produce drug-free subjects but suggests another way of being in the world. By focusing on practices of care as assemblages in which persons, social processes and things interact, we ‘can also reveal how “neglected things” are as important occasions for care as any of the more heroic aspects of healthcare’ (Latimer, 2018: 385). Latimer’s call for a shift from heroic to small-scale aspects of healthcare is enacted in this paper through an empirical and methodological shift from an interest in the recovered subject (Fomiatti et al., 2019), to care for the recovering subject and the description of the recovery process as an assemblage that expands life possibilities.
Setting up a description field
Bringing together Love’s (2010; 2013) practices and politics of description with the Deleuzo-Guattarian assemblage (Delanda, 2016; Deleuze and Guattari 2004; Duff, 2014) and feminist approaches to materialities of care (Latimer 2018; Martin et al., 2015; Puig de la Bellacasa, 2012), a description field is set up; one that grasps the ever-changing formations of the recovery process, without diminishing its complexity through interpretations. In what follows, the description of the recovery assemblage is structured around the generation of care through small, every-day practices. The aim of this approach is twofold: (a) to challenge the constitution of recovery as a neoliberal practice and (b) to explore how empirical social methods do not just account for, but transform worlds. I specifically describe how certain objects and their mobilisation by service-users and workers produce practices of care. I do so by (a) providing a thin description of the recovery assemblage based on my presence in the field and (b) paying attention to the service-users’ thick descriptions of the meaning of these objects, through one-to-one interviews and visual methods.
In August 2018, I started volunteering at Genie in the Gutter, 1 a Liverpool-based daily recovery centre. Becoming a volunteer at the drug recovery services I was collaborating with was an essential part of the fieldwork process. While one-to-one interviews and photovoice had been set as the primary research methods, it was a requirement of both the researcher and the collaborating services that trust relationships with participants would be built through my engagement with the service’s daily activities. Genie’s activities run from Monday to Friday, starting at 10 am and finishing at 5 pm. These activities involved one recovery group per day and various other creative (art, drama, music) and well-being (meditation, yoga, walks) activities. As part of my duties, I was spending time at the reception of the service, talking to service-users, answering the phone, taking part in creative and well-being activities and facilitating recovery groups.
Through my presence in the recovery space and participation in the recovery activities, a field for a thin description of the practices of care emerging in the recovery assemblage was set up. Being present, as well as part of the field site through volunteering, my intention was to observe the emergence of practices of care, to describe them but not interpret them. Love (2010: 377) argues that good descriptions ‘are close, but they are not deep; rather than adding anything extra to the description, they account for the real variety that is already there’. Becoming part of the daily practice of recovery offered me the opportunity to refrain from ‘generating’ data, and to experience instead what is already there, to observe how caring practices unfold in the present of the recovery practice and affect the lives of people. ‘Thin description means, in effect, taking up the position of the device; by turning oneself into a camera, one could – at least ideally – pay equal attention to every aspect of a scene that is available to the senses and record it faithfully’ (Love, 2013: 407). Applying Love’s call to turn oneself into a camera in spaces of recovery, I paid attention to every aspect of the daily crafting of recovery, faithfully recording the recovery practices available to the senses. Holding this position gave me the opportunity to challenge the perception of recovery as a practice that focuses on the separation between a person and a substance, and to produce knowledge that goes beyond dominant perceptions on the lives of the people we do research with. Love’s thin description revealed recovery as a practice that does not force disconnections but enables meaningful connections that expand life possibilities.
While the description deriving from the researcher’s presence in the recovery assemblage is thin, the service-users’ descriptions coming together through oral and visual methods are thick, in the sense that they offer a rich account of significance and individual intention (Love, 2010: 380). In this paper, I bring together a thin description of the present of the recovery assemblage, and the participants’ thick descriptions of the significance of the caring practices emerging in spaces of recovery and extending to other social assemblages. Following how objects and practices matter inside and beyond spaces of recovery reveals opportunities for intervention and care that enhance well-being.
Interviews with participants were focused on their lived experiences of recovery and care. My role as interviewer was to create a framework for the narration of these stories, rather than to focus on the human and non-human components that I had become attentive to during my presence in spaces of recovery. The participants’ descriptions of the objects, connections and practices discussed in this paper do not constitute responses to direct questions about their position in the recovery assemblage, but emerged within broader discussions about the experience of recovery.
Through the deployment of photography, we addressed the issue of re-engagement with assemblages that extend beyond the recovery assemblage. Photovoice gives the camera and the analytic voice to participants. ‘Photovoice has emerged from the fields of health and community assessment studies as a photo elicitation technique that facilitates participant involvement at all stages of the research process’ (Given et al., 2012). According to Harper (2002: 13), ‘photo elicitation is based on the simple idea of inserting a photograph into a research interview’. What photovoice adds to this idea is the requirement that the images used in the interviews should be participant generated. My deployment of photovoice reflects McLeod’s (2017) use of photography with people with depression. In her empirical research, McLeod mobilises photography as a way to make materials central and active, and to direct her attention to non-human action. Her participants planned, took and edited their photos in their own time, and then delivered ‘a rehearsed narrative about each photo’ (McLeod, 2017: 31), through one-to-one encounters, where ‘the photos were the key communicative device. . .The position [that McLeod] moved to in these encounters was simply to be present and witness the affective force or sensation of the photos’ (McLeod, 2017: 33). In turn, my encounters with service-users were driven by the photographs and the photographers’ narratives. My role was to observe rather than to ask questions, to follow how service-users chose to photograph and talk about certain objects and places and not others. By choosing to capture and describe certain objects, the participants follow the affect of caring practices produced in spaces of recovery, as this extends to other personal and shared spaces they inhabit. Furthermore, their description of the photographs is accompanied by the feelings emerging through the contemplation of the objects and spaces captured.
Overall, participants’ observation together with oral and visual methods produced an assemblage of objects and practices that most matter to service-users. These empirical accounts drive the unpacking of the human and non-human encounters that constitute the recovery assemblage in all its complexity. Bringing together thin and thick descriptions of recovery, my aim has been to explore the ‘possibility of an alternative ethics, one grounded in documentation and description rather than empathy and witness’ (Love, 2010: 375). Approaching recovery through alternative ethics gave me the opportunity to reclaim it from neoliberal systems of thought and to re-constitute it as a practice of resistance to the production of neoliberal subjectivities. The focus is on how experiences of illbeing and well-being are brought together in the recovery assemblage through the narratives of service-users, and on how these experiences are re-embodied and re-negotiated through caring practices and the enablement of affective relations.
By ‘relying on description rather than interpretation’ (Love, 2010: 375), an account concerned with ‘what the real world [of recovery] is really like’ (Love, 2013: 430) is produced. It is in this desire to capture the ‘real world’, or the ‘real experience’ (Duff, 2014) of recovery that Love’s descriptive turn meets the Deleuzo-Guattarian assemblage. Unpacking recovery as an assemblage provides us with the structure and the frame of thought needed in order to stay with its complexity. According to Deleuze and Guattari, the assemblage is tetravalent, comprised of a horizontal and a vertical axis, where both these axes comprise two segments. Horizontally, we encounter ‘the machinic assemblage of bodies, of actions and passions, an intermingling of bodies reacting to one another’ (Deleuze and Guattari, 2004: 97–98, emphasis in original). This is the content, the pragmatic system of the assemblage. On the other side of the horizontal axis, we encounter ‘a collective assemblage of enunciation, of acts and statements, of incorporeal transformations attributed to bodies (Deleuze and Guattari, 2004: 98, emphasis in original); the expression or semiotic system of the assemblage. The assemblage allows for a new relation to emerge between content and expression. Following this outline of the horizontal axis of the assemblage, the content, or pragmatic system of the recovery assemblage is comprised of the bodies that inhabit it: the service-users and members of staff. On the other side of the horizontal axis, we encounter the daily practices of the assemblage, the collective assemblage of enunciation where its expression comes into being. The new relations that emerge between the content (service-users and workers) and the expression (practices) in the recovery assemblage are described in the forthcoming analysis.
Attempting to describe rather than interpret does not imply that the positions we hold as researchers are neutral. The positionality of the researcher in the field affects the form that care takes and shapes the knowledge and the descriptions produced. Description is not an all-encompassing method that pays equal attention to all human and non-human components that constitute a ‘field’. As researchers, we become attentive to certain practices, instead of others. I understand description as an expression of care, and care as a selective mode of attention and knowledge-making practice (Martin et al., 2015). The attention is on practices that emerge through the encounter between human and non-human components, and on how these practices unfold recovery as an act of resistance to neoliberal systems of thought. Attentiveness to these practices derives from the desire to take seriously all actors involved in the recovery process, to care for the daily crafting of recovery. Holding this position does not render the researcher neutral, but aware of the implications of the knowledge produced (Gomart, 2004). The analysis that follows is a description of a recovery assemblage as this emerged through my presence in and care for the practice of recovery, and the visual and oral accounts of service-users. Its aim is to ‘. . .create the conditions of possibility through which practitioners and patients alike are participants in world making, and through which care becomes an emergent property of their alignment not their division’ (Latimer, 2018: 389).
Describing spaces of recovery
Assessment forms
The first step towards building a connection with a recovery service is to make an appointment and turn up for an assessment. The practical aim of this first assessment is to gain an insight to the background of the service-user, collect information on their substance use and their living conditions. In turn, the assessment form is used for the production of a risk assessment, identifying both potential risks for the service-user, as well as how they might pose risks to others. Finally, once the service-user has been accepted, all this information is used for the production of a needs assessment, where a support plan is designed. The efficiency and implications of such assessment forms and other treatment tools have been the subject of criticism of empirical researchers (Savic and Fomiatti, 2016). The workers of Genie stressed the importance of being flexible when completing these forms, carefully collecting essential information and in turn skipping sections that might tire new service-users with unnecessary questions. Service-workers also provided a distinction between the completion of forms as a process of ‘ticking boxes’ and as a caring practice that leads to action towards addressing the service-users’ needs. In the quote that follows, the manager of Genie talks about assessment forms as meaningful components of the recovery practice, only when they contribute to the establishment of affective connections:
‘[It’s not about] getting someone in and filling out the form, well I’ve filled out that form so you go home, have a good weekend. It’s about making sure it’s a reality, you know. Is that form, is that going to help this person to get through the weekend? Are they going to walk out of here and they’ve got somewhere to go, you know?’
Assessment forms can become useful tools for the identification of a service-user’s needs as well as devices that enable the first encounter between a user and service. Making an assessment appointment is not just a practicality, but most importantly a symbolic gesture, a commitment from both sides that on a chosen day they will make time for each other. This commitment becomes the first point of negotiation between the potential service-user and the service, and it requires patience and work from all actors involved. It is the agreement to ‘share time’ with each other that initiates the production of a connection. Drug use time though is a non-linear, complicated experience that clashes with normative understandings of time, including the ability to keep appointments (Fraser and valentine, 2008; Knight, 2015). In my experience from Genie, assessment appointments would often not show up, in most cases without cancelling in advance. It then becomes the responsibility of the worker to contact the person that missed their appointment and invite them to book another one. This admission process can be lengthy and time-consuming, occasionally successful, occasionally not – but in any case, a first attempt to establish a committed and caring relationship.
Neoliberal systems of thought present the drug user as a ‘free’ subject that can make informed, ‘healthy’ choices and respectively take responsibility for those choices and actions. The reality however of the initial encounter between the service and the user, as accounted for by people in recovery, reveals the process of ‘asking for help’ as a complex one, where the practices of care are not known in advance. The commitment to ‘turn up’ for an assessment appointment is an expression of the desire to connect with the recovery assemblage, even when the help that one is asking for cannot yet be translated into specific demands. Through this connection, recovery shifts from an abstract formation into a specific practice taking place at a space where one has to physically go, in order to see what kind of help can be given. Therefore, the assessment form stands symbolically as a threshold (Latimer, 2018: 380) that potential service-users must pass, accompanied by service-workers, in order to become part of the recovery assemblage. Passing this threshold is an active affirmation of the service-user’s desire for care, and a service-worker’s commitment to provide this care.
Exploring the practices of ‘asking for help’ in all their complexity and heterogeneity serves to challenge the neoliberal production of subjectivity through which responsibility is placed on the individual and its ability to make informed, ‘healthy’ choices. Mol (2008) argues that a ‘logic of choice’ dominates health care, and she proposes instead a ‘logic of care’ where the needs of each subject are navigated collectively by the user, the worker and the service. The provision of care becomes thus a shared responsibility that requires all actors involved to shift their practices in order to engage with each other in ways that enhance life possibilities.
Texting and calling
An example of an approach to care that challenges the ‘logic of choice’ is Genie’s daily practice of ‘checking-in’ with service-users by calling them. One of the daily tasks of workers at Genie is to send a text (SMS) to all service-users that details Genie’s activities for the day. The workers then call as many service-users as possible, first thing in the morning, to ask how they are doing and encourage them to ‘come in’ for the day. This is a task that requires attention to and knowledge of each service-user’s schedule. For example, during my fieldwork at Genie, being there on Mondays and Tuesdays, it was my responsibility to call the regular service-users of those days, and those that had not shown up for a while and check-in with them. This practice extends beyond the physical territory of the recovery assemblage, reaching out to other assemblages that service-users operate within. By caring for them, whether they are physically present at the recovery space or not, the recovery process extends beyond a specific territoriality. This small gesture was very often commented upon by service-users as important for them, as a practice of care that increased their engagement with the service:
‘yeah, with Genie, they’re very, they do care about the clients and they do keep an eye on you, they send you texts and they phone you up’ ‘I did come along and after a while I stopped coming along, I thought I didn’t need to and I was drinking for quite a while. . .and [member of staff] she called me one day and asked me to come back and I did and I’ve been coming back since.’
The service-users value Genie’s practice of ‘checking-in’ as a consistent attempt to establish a connection between the service-user and the service. The fact that the workers ‘keep an eye on you’ is experienced as a caring practice, potentially leading to the re-connection with the service in cases when the engagement has been interrupted (‘I stopped coming along. . . she called me one day and. . .I’ve been coming back since’). Within a logic of choice, this practice could be evaluated as time-consuming, unnecessary and even harmful in that it could undermine the service-users’ agency. Considering that the service-user has already been given information regarding the schedule of the service, the practice of calling non-attenders could be seen as undermining their choice to not show up. Furthermore, side-lining the specifics of their daily lives, it could be framed as non-compliance with the service’s requirements and lack of desire to establish meaningful connections. However, service-users’ narratives tell a different story that enacts the practice of ‘checking-in’ as care and in turn complicates the question of agency and emphasises the ambivalences that inform their daily decisions:
‘they’re very nice people here and you know quite friendly bunch and non-judgemental and supportive and, they give you a kick up the arse if you need the motivation, and they can tell if you, you’re down and they try to bring you up again and get you moved back up and I, I realise that this time they meant it! They were actually trying to help and they are nice people and they are doing it for the right reasons, whereas before I kind of got the impression that they were just trying to tick boxes and say, and show willing, you know. . .So usually, because I’m quite intelligent, perceptive, so I can tell the difference between people who mean it and people who don’t mean it. So I think I, you know I suppose I felt sort of welcomed here more genuinely than I did like say when I went on the CBT course because that was more a case of just someone whose job it is to do this for a couple of weeks with this patient, you know to, you know show that the NHS is doing something, to show that, I don’t know some politician set that up at some point, did something, whatever!’
In the account above, making choices is talked about as a process that requires ‘a kick up the arse if you need the motivation’, as well as the occasional phone call from a worker that asks the service-user to come back and re-engage with the service. This narrative challenges the constitution of service-users as autonomous individuals that make personal choices, disassociated from their encounters with others. ‘Making choices’ is talked about as a situated and relational process where the encounters with others matter, and the affective relations in place have the power to change the course of this process. In other words, ‘making choices’ in recovery is not about making the ‘right’ choice following a linear path that leads to abstinence, but about experiencing caring practices that expand life possibilities.
Birthday cards
‘Turning up’ for an assessment appointment is a collective effort that takes into consideration the everyday realities of service-users. ‘Filling out forms’ matters when it works towards the establishment of the connections and support required, when it leads to the provision of this support in practice rather than in paper, ‘making sure it’s a reality’. Staying with this commitment, ‘checking in’ through calling and texting, stabilises this relationship of care. One more practice of Genie, deployed to enhance the connection between the service and its users – whether their presence is consistent or not – is the posting of birthday cards:
‘A lot of people come and they, you know, they get a birthday card from us, it’s not rocket science, but a lot of them don’t have anyone. And that makes someone come back we’ve not seen in months, you saw [name of service-user] before, we haven’t seen him about a year, but he would have got a birthday card from us’
Through this practice, the presence of the service remains consistent even when the presence of the service-user in the recovery service is not. Through the birthday card, the recovery assemblage as well as the care that it provides, extends beyond a specific territoriality and reaches out to the service-users’ personal spaces. The fact that none of the service-users ever gets crossed off the birthday list, no matter for how long they had not ‘turned up’ at the service, constitutes a resistance to recovery models that follow a logic of choice that ‘punishes’ the service-users’ occasional inconsistency by interrupting their connection with the service.
Observing and describing these material practices as they unfold within the recovery assemblage leads to an understanding of practices of care that goes beyond their measurability and translatability into policy documents. The ‘success’ of mental health interventions like CBT courses is usually measured through feedback forms that enable the quantification of participants’ responses (Kim et al., 2012; Pickering et al., 2017). However, non-quantifiable elements, like the connection between these practices and the daily realities of service-users, are systematically side-lined by short-term treatment approaches. What the empirical testimonies of service-users emphasise is the importance of gestures that establish the service and its users as co-authors of the recovery process; practices that create a shared responsibility by generating the feeling that ‘[the workers of a service] do care about [them], that ‘[they] keep an eye on [them]’, and ‘can tell if you’re down’. These accounts indicate how care matters, and more specifically how unmeasurable practices of care matter.
Describing the connections that objects like assessment forms enhance in the recovery assemblage, as well as following the descriptions of service-users on how practices like texting and sending birthday cards matter, opens the way for a different ‘reading’ of the practice of recovery. ‘By foregrounding observation and description. . .we can better account for all the things that texts are – the way they appear, how they behave, what they communicate’ (Love, 2013: 412). Going back to the example of the assessment form, it can be argued that it operates as a tool for the quantification and categorisation of service-users. However, following Love and the form’s deployment by Genie, it can be described otherwise – as a text that does not communicate quantifiable data, but a promise of care.
Through the method of description, the service-users’ agency is seen under a new prism: the focus of attention shifts from the provision of information that will render them to make ‘healthy’, informed decisions, to the deployment of caring practices that create a shared commitment between the user and the service. Through their accounts it becomes apparent that not only can service-users ‘tell the difference between people who mean it and people who don’t mean it’, but also that they care about whether they mean it or not, they can tell when the provision of ‘care’ reflects an attempt to ‘tick boxes’. Through these narratives, a desire for care (Biehl and Locke, 2010) is articulated, a desire for affective relationships that come into being through unmeasurable caring practices.
Describing recovery beyond the recovery space
Up until now, I have focused on the enactment of care through the connections and practices enabled by objects encountered inside the recovery assemblage. Assessment forms, birthday cards, phone calls and texts have been described as devices that render care desirable and possible. Following service-users’ descriptions of their experience of assemblages that extend beyond the recovery territory, I argue that the caring practices that become possible in the recovery assemblage are not site- or time-specific, but able to enhance life possibilities overall. This process is accounted for through the Deleuzo-Guattarian concept of deterritorialisation, meaning the extension of the small shifts and transitions that become possible in the recovery assemblage to other assemblages, eventually leading to life-changing transitions.
According to Deleuze and Guattari (1977: 379), art causes ‘increasingly decoded and deterritorialised flows to circulate in the socius, flows that are perceptible to everyone, which force the social axiomatic to grow ever more complicated, to become more saturated’. Thinking with the descriptions of the visual material produced by Genie’s service-users’ with Duff’s (2011) concept of enabling places, and the Deleuzo-Guattarian concept of deterritorialisation can enhance our understanding of the relationship between social inclusion and recovery from primary health problems. Duff (2011: 155) argues:
Places are rarely settled, and their coordinates are never fixed. They are forever mobilised, transformed and reproduced in the dynamic force of inhabiting place. To conceive of an ecology of enabling places is to emphasise this material and relational production of place. . .enabling places are made rather than merely discovered.
The visual material produced by Genie’s service-users and the descriptions that accompany them reveal the array of connections made possible through creative practices taking place within and beyond the recovery assemblage. Through these encounters, enabling places are made, deterritorialising the life possibilities produced inside the recovery assemblage.
Doorways and buzzers
‘I took a picture of the art gallery because we’d just been there and it’s just an example of some of the stuff I’d done at Genie that I wouldn’t normally do like before I came to Genie, I wouldn’t have gone to art galleries or museums really to look at exhibitions and stuff like that. If you’re just wandering around, some sort of pointless drunk and then you only get to see the outside of buildings. I do actually appreciate the architecture and that but you always feel like you’re barred and you’re not allowed in or something, like you go past a nice pub but you can’t go in there (laughs) or a nice building or a nice hotel, you know, you’re not going to stay there, or a nice, a sort of like upmarket shop or something, you know you’re not going to go in there to buy stuff and that. So there’s that sense of exclusion. So it’s like the doorways are a metaphor, like you can go in like you know, I think because a lot of it’s just your own mindset isn’t it? You’ve convinced yourself you don’t belong, so you stay outside of everything! And so, but it’s nice to have people to like encourage you to sort of take part I suppose on the indoor culture side of things! Because when I first came here, you know it was, it was nice to go to other places where other things are happening. . .or when we were going to the cathedral to play the drums outside and stuff like that, to go somewhere and get inside and get involved.’
The above (See Figure 1) is a description of the making of an enabling place, the connections and deterritorialisations that render its production possible and the new encounters that derive from it. The service-user describes the visit to the gallery as a new experience that became possible through his engagement with Genie, providing an example of how the recovery assemblage extends to other territorialities and generates affective encounters that enable participation in ‘the indoor culture side of things’. Being ‘outside’ is symbolically talked about as a space of exclusion. The gallery space becomes an enabling place due to the way that it is experienced; a space that becomes accessible with others, with people that ‘encourage you to take part’. The gallery doors are described as a metaphor for the exclusions that one experiences when they are still using, and the inclusions that become possible through the engagement with recovery. Another aspect of this description is the photographer’s embodiment of self-blame for his past exclusion from institutions like art galleries. As a ‘pointless drunk wandering around. . .you always feel like you’re barred and you’re not allowed in or something’. Instead of criticising the institution for the exclusions that it reproduces, the responsibility shifts to the excluded: ‘I think because a lot of it’s just your own mindset isn’t it? You’ve convinced yourself you don’t belong, so you stay outside of everything!’ As discussed above, the doorways of the buildings work as a metaphor, separating those who ‘belong’ from those who convince themselves they ‘don’t belong’. The recovery assemblage, extending to other institutions and social spaces renders the ‘inside’ possible, as well as desired (it was nice to go to other places where other things are happening). The internalisation though of the exclusions that using bodies suffer persists. The transition from a using to a recovering body, from the ‘outside’ to the ‘inside’, is ongoing and under negotiation, when permission to gain access is asked:
‘Well I have to press the button and say who I am, but they let me in though, when I’ve said who I am, which is like, still come to terms with that, it’s me (laughs) can I come in, are you sure, I just said it’s me, like, are you absolutely sure?! (laughs) But yeah. . .Well I suppose it’s a symbol of the fact I’m connected at least.’
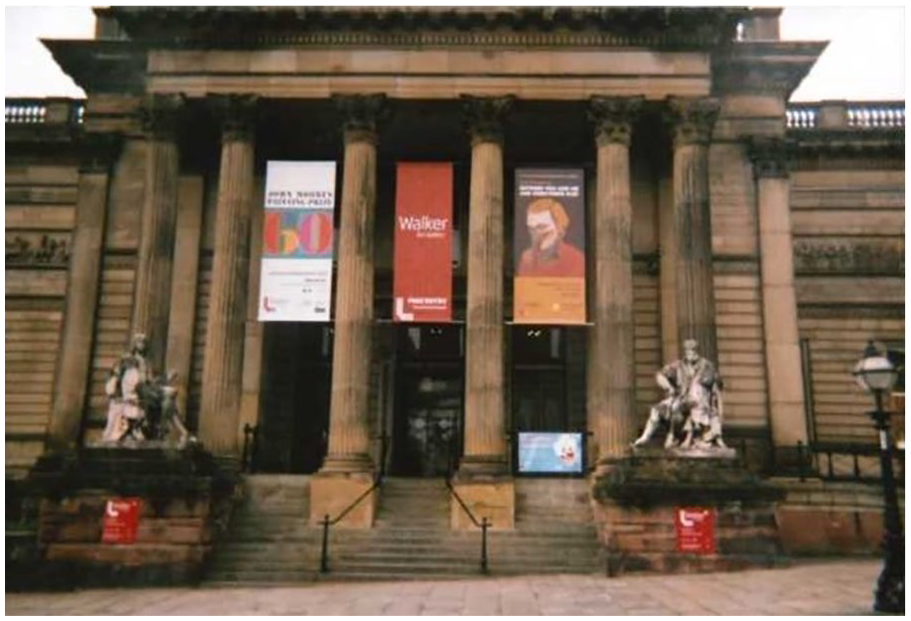
The Walker Art Gallery, Liverpool.
The doorways of the previous picture are now replaced by the buzzer of a creative service the service-user is engaged with, standing in-between the ‘inside’ and the ‘outside’ (See Figure 2). The narrator still tries to ‘come to terms with’ the fact that it is by stating who he is that access is granted. In his words, the door that opens when he says his name is ‘a symbol of the fact I’m connected’. This ‘surprise’ that comes with one’s inclusion is described by one of Genie’s workers as a ‘challenge’ for those used to being excluded:
I think he [one of Genie’s service-users] can’t believe that he’s still accessing us and hasn’t been excluded, because he gets excluded everywhere he goes. I think that for him has been his biggest challenge in accepting that, that regardless of his behaviour, we’ll still work with it!

Entrance of a creative recovery service, Liverpool.
In these visual and oral narratives, the opening doors are symbols of connections, and the ones that remain shut are symbols of disconnection and isolation. When mediated by recovery, connections with other social spaces become possible, while the drug using, individual body remains ‘outside’, embodying systems of thought that render it accountable for its isolation. These accounts emphasise the significance of the connections produced inside the recovery assemblage. At the same time, they problematise longstanding questions of inclusion and exclusion that the recovering body experiences in its attempt to extend to other assemblages.
The oil painting
Apart from the recovery and other assemblages service-users are included and excluded from, private spaces are also transformed through the deterritorialisations enabled during the recovery process. The description of how the oil painting came into being is indicative of how practices of care emerging in the recovery assemblage extend beyond the disassociation of a body from a substance and expand life possibilities (See Figure 3).
‘That’s an oil painting I did because I felt inspired, because I was doing the art classes here [Genie] and. . .I’d found a canvas and I’d found a bag full of different paints and art materials and stuff, and some of it was oil paints and thought it would be interesting to do an oil painting because I’d never done an oil painting, I’d done all sorts of other types of art but I hadn’t done an oil painting. So one day when I just felt like it, I just sat down and did it, because I had the canvas and I had the oil paints so I thought why not, so I did it! I was pretty pleased with the results!’
Oil painting produced by one of the participants.
The oil painting depicted in the picture is the outcome of an encounter between the ‘inside’ and the ‘outside’. The ‘inspiration’ comes from the creative practices taking place within the recovery space, while the materials are found and collected ‘outside’. This encounter produces an oil painting in the private space of the service-user. Following the route of these encounters opens up the way for a wider understanding of ‘enabling places’, as places that are not only produced on sites where the encounters take place, but extend beyond them and include social as well as private places. In the description of the creation of the oil painting, the private place becomes an enabling one when the desire to do art extends beyond the recovery assemblage. The art classes at Genie generate a desire deterritorialised to other assemblages, like the street, where the materials for the production of the oil painting are found, and eventually to the private space, where the painting is produced. While under different circumstances these found water colours might not have been regarded as an opportunity for creative practice, the narrator allows himself to be affected by this random encounter, extending it to his private space where the art work is produced.
Conclusion: can description change policy?
The fundamental question is whether describing care as it is felt through small gestures can shift the way we do policy. Recent science and technology studies address the complex relationship between policy and care, and how these can be reconfigured together (Gill et al., 2017: 8). My response in this paper is that policy, care and empirical research can be reconfigured together through a close exploration of recovery practices and the small-scale gestures that render recovery possible. Current policy narratives focus on the outcome of the recovery process, rather than on its present, as it is crafted daily in the recovery assemblage. In so doing, they neglect materialities of care, and how these matter for people in recovery. Following the service-users’ descriptions of neglected objects and practices, I have attempted to render visible how ordinary practices can shift the world (Latimer, 2018: 385).
As discussed at the introduction of this paper, Love’s deployment of description goes beyond the observation of the worlds we do research with. Accounting for and describing the interactions that are already there, rather than attempting interpretations, can shift things. Focusing on practices of care, and describing how small gestures expand life possibilities, opens the way not only for the observation, but most importantly for the transformation of the ways we think about and do recovery. Thinking recovery with the Deleuzo-Guattarian assemblage renders visible the connections emerging through the recovery process, transforming the service-users’ lives in positive ways. As I have argued elsewhere (Theodoropoulou, 2020), this frame of thought challenges the segregation between harm reduction and recovery based on the presence or absence of substances, and provides us with epistemological tools that enable a shift towards the understanding of drug treatment as a practice of care that enhances a body’s capacity to act. Accordingly, the in-situ materialities of care described in this paper are mobile and adaptable, able to transform normative understandings and practices of health and recovery. Focusing on the emergence of care through daily human and non-human encounters constitutes a call for attention to the small gestures that nurture novel connections and render well-being possible.
The commitment towards the description of how these connections come into being constitutes policy in practice. Following this line of practice, I argue that by deploying description we can unsettle policy; we can challenge its constitution as a force emerging outside spaces of recovery and reconfigure it instead as practice (Gill et al., 2017). Following the transformative power of materialities like assessment forms, phones and art material, as these mobilise assemblages of care inside and beyond spaces of recovery, constitutes an example of how policy can emerge through small gestures rather than normative narratives. As explained by the manager of Genie, the problem starts when policy decisions are made elsewhere and do not emerge from, or attempt to develop any connections with the recovery space:
‘I think the government is not looking at what’s happening on the ground. I think in funding they look at dotting I’s and crossing T’s, what looks good on paper, but they’re not out there and seeing how it affects people on a day to day basis. I think they’re out of touch on how they fund.’
This is a description of policy as an external force that side-lines small recovery gestures that generate care. Through the unwillingness of policy-makers to engage with ‘what’s happening on the ground. . .on a day to day basis’, it becomes apparent that the current focus of policy is not on the recovery process, as it is crafted in the recovery space but on the ‘recovered’ subject. This is further emphasised by policy approaches that regard the recovery process as ‘successful’, based on the ‘recovered’ subject’s return to employment (HM Government Drug Strategy 2010 and 2017). Recovery is therefore framed as a space expected to produce functional individuals, able to ‘return’ to society. This way of thinking produces the substance and its consumption as a problem to be ‘solved’, and neglects all other connections, built and broken, that rendered the consumption of the substance necessary.
The reconfiguration of policy as practice demands the shift of our attention from the outside, or the ‘after’ of recovery, to the present of recovery, and the connections emerging inside the recovery assemblage. The ‘minimalist but painstaking work of description’ (Love, 2010: 387) can contribute to the close examination of the caring practices that render recovery possible, and to the reconfiguration of policy as a practice emerging organically inside spaces of recovery. By closely paying attention to, and describing recovery practices, we can produce policies that respond to the needs and desires of the drug using population, rather than to the expectations attributed to them through neoliberal systems of thought.
Objects encountered inside and beyond the recovery assemblage have been mobilised for the description of recovery as a practice not primarily concerned with the interruption of a body’s relationship with a substance, but with the enhancement of connections that expand life possibilities. This way of thinking constitutes an ethical approach, not only applicable to spaces of recovery but to all assemblages where notions of well-being and illbeing are produced. Describing how encounters between objects and people matter, challenges the production of well-being as a stable state and reconfigures it as a process being slowly and carefully weaved through small gestures. The aim of this approach is not to suggest better policy interventions but to disrupt the logic of policy overall – to shift the attention from policy as intervention to policy as practice. This shift requires attention to small gestures, practices, and materialities that slowly render well-being possible. The description of materialities of care and small gestures paves the way not only for the researcher’s capacity to observe people as they sleep; it extends beyond observation and holds the power to awaken people and change worlds.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through a 3+1 scholarship awarded by the Economic and Social Research Council.