
Abstract
This article examines the World Bank’s role as a ‘problem broker’ in national policymaking, specifically its influence on healthcare financing policy, using the case of Albania’s healthcare financing reforms (1995–2013). While the Bank is widely acknowledged as a ‘Knowledge Bank’, its role in problematising national issues remains underexplored. Employing qualitative methods, including content and frame analysis of Technical Assistance reports, the study explores how the Bank’s problem-brokering activities and its framing of reform issues shaped national policy actors’ perceptions. The analysis highlights the Bank’s influence in guiding national policy agendas through problematisation, extending its influence beyond the traditional role of a ‘proposal actor’. This study enriches our understanding of the Bank’s ideational, non-coercive influence in national policy arenas, complementing existing literature on its conditional and coercive power.
Introduction
The World Bank (referred to as the Bank), a prominent International Organisation (IO) often acknowledged as the Knowledge Bank, exerts significant influence over national policymaking processes (Bazbauers, 2018; Béland and Orenstein, 2009). Nonetheless, most scholarly work has concentrated on the Bank’s role as a proposal actor, advancing specific policy solutions (Orenstein, 2008) while overlooking its equally significant role in problematising policy issues. This article addresses this gap by arguing that the problematisation of national policy issues represents another crucial dimension of the Bank’s ideational influence. Specifically, the article casts the Bank in the role of a problem broker, an actor capable of ‘fram[ing] conditions as public problems and work[ing] to make [national] policymakers accept these frames’ (Knaggård, 2015: 451).
To understand how the Bank engages in the role of a problem broker and what specific activities and strategies it employs to influence national policymaking processes, the analysis draws on Albanian healthcare financing (HCF) reforms, focusing on the period from 1995, the year of the Social Health Insurance (SHI) introduction in the country, to 2013, when as detailed in section ‘Background: Albania and its healthcare financing reforms’, the Bank’s ideas on HCF policy issues began to capture the attention of national actors and resonate with the Albanian policymaking arena. 1
The Bank’s involvement in health has drawn considerable scholarly attention (e.g. Clinton and Sridhar, 2017; Sridhar et al, 2017; Kaasch, 2015; Ruger, 2005; Tichenor and Sridhar, 2017), along with numerous empirical studies (e.g. Malinar and de Carvalho, 2025; Noy, 2017; Weyland, 2007), due to the policy specificities. Healthcare reform is inherently complex and politically charged, with various competing interests and values at play. Healthcare systems are ‘complicated and multifaceted’, encompassing not just medical aspects but also ‘financial, managerial, informational, and promotional’ dimensions (Weyland, 2007: 182). This complexity sets healthcare apart from other social policies, like pensions, where the Bank’s influence is more straightforward and well documented (Orenstein, 2008; Weyland, 2007). Unlike reforms of ‘income-maintenance programs, like unemployment insurance or retirement schemes’, healthcare reform intersects with fundamental normative issues such as the right to health and relies on technical expertise to navigate the intricacies of healthcare system design (Béland, 2010: 630). Moreover, the organisation of healthcare systems often hinges on the relationship between expert knowledge and state authority, which makes healthcare policy a particularly sensitive political terrain (Carpenter, 2012: 287). The contention around healthcare reforms is also amplified by a lack of consensus among IOs (Kaasch, 2013: 55).
Healthcare financing reform, in particular, underscores these challenges. More than determining the allocation of financial resources, HCF policy requires balancing competing values such as equity, access, efficiency, and sustainability within healthcare systems. Different IOs prioritise these values differently in their approaches to HCF reforms in low- and middle-income countries (LMICs) (see Kaasch, 2013). It is worth noting that since the start of the new millennium, a growing convergence between the World Health Organization (WHO) and the Bank, referred to as ‘two global ministries of health’ (Noy, 2017: 1), has placed equitable access to healthcare at the forefront, with Universal Health Coverage (UHC) emerging as the ideal goal for balancing equity and sustainability in healthcare systems (see WB, 2018, 2023; WHO, 2014). However, this alignment is rooted more in shared norms (equity) and metrics (financial hardship in accessing healthcare services) rather than clear ‘prescriptions’ (solutions) for LMICs to achieve UHC. These considerations make examining the Bank’s role as a problem broker in HCF reforms particularly relevant.
The case of Albania is instrumental in illustrating this role, particularly in understanding how the Bank exercises non-coercive influence in contexts of vulnerability and financial dependency. As a post-communist Central and Eastern European (CEE) transition country and a low- and later middle-income country, 2 Albania presents a setting where a coercive, conditional approach by the Bank would typically be expected (see Deacon and Hulse, 1997; Paloni and Zanardi, 2006). However, Albania’s case diverges from this theoretical expectation, revealing that the Bank’s influence was driven by knowledge and expertise rather than imposed conditions. Examining this case highlights how ideational influence, through technical assistance, shapes national policymaking even in financially dependent contexts. As such, insights from Albania’s case contribute to a broader understanding of how transnational policy actors (TNAs) shape HCF reforms in other similarly vulnerable national contexts.
The theoretical framework builds on International Relations (IR) studies, integrating concepts from ideational scholarship and policy process studies. First, and aligned with many IR studies (e.g. Barnett and Finnemore, 1999; Cormier and Manger, 2022; Weaver, 2008), the Bank is conceptualised as an international bureaucracy that maintains a certain level of coherence in its actions and activities, despite its complex and decentralised structure as an IO. 3 Second, the framework incorporates the scholarship on the Bank as a knowledge transfer agent, disseminating ideas to national arenas (Bazbauers, 2018; Stone, 2004). Third, the framework integrates ideational concepts from policy process studies, especially around problem definition. Mehta (2011: 27) describes problem definitions as ‘a particular way of understanding a complex reality’, emphasising how policy discourse shapes which definitions dominate and which are excluded (pp. 35–38). Similarly, frames are linked to problem definitions (Campbell, 2002) and reflect how actors use discourse to draw attention to policy issues through deliberative processes (Baumgartner and Jones, 1993).
Two qualitative methods are employed in the analysis. First, a case study examines the Bank’s problem-brokering activities and instruments through a content analysis of its Technical Assistance (TA) reports (see section ‘Background: Albania and its healthcare financing reforms’). Second, a frame analysis of excerpts from these reports identifies how the Bank constructed and presented SHI problems within its discourse. 4 Eleven documents (totalling 1359 pages) were examined using both methods.
The rest of the article is structured as follows: The next section examines the Bank’s approach(es) to HCF policy and explores existing research on how the Bank’s influential roles in national reforms have been studied. The theoretical section presents key concepts and the analytical framework guiding the methodology. Background information on Albania is then provided. The empirical section is divided into two parts: the first examines the Bank’s problem-driven approach and activities, while the second analyses the Bank’s framing of SHI reform issues. The discussion section explores the implications of these findings, and the final remarks highlight the study’s broader contributions to the field.
The Bank in health: evolution, influence and theoretical perspectives
This section revises what we know about the Bank’s approach to health and HCF reforms in LMICs, highlighting both the shifts in its approaches and its varied roles in national policymaking arenas, with a particular focus on the understudied role of problem broker. The objective is to broaden our understanding of the Bank’s roles in these contexts, an aim that is further developed in the subsequent theoretical section.
The evolution of the Bank’s approach to health and healthcare financing policy
The Bank’s focus on population health has evolved considerably since its involvement began in 1968, initially addressing disease-specific issues, nutrition, and family planning. However, the Bank’s view on health (care) and social policy has closely mirrored its evolving stance on development, which has been characterised by a continuous redefinition of economic and development policies. As Vetterlein (2007) argues, this shifting approach to development has had a profound impact on the Bank’s interpretation of social policy. Consequently, the Bank’s understanding of health (care) policy issues has transformed, leading to varying problem definitions and, in turn, diverse policy prescriptions.
In the late 1970s, social policies were central to the Bank’s development perspective, but they lost prominence in the 1980s with the rise of structural adjustment lending. In the 1990s, the focus shifted to economic growth as the primary driver for poverty alleviation, positioning social policies, particularly education and health, as investments towards this broader goal. By the 2000s, the Bank had adopted a more comprehensive social development approach, highlighting the interconnectedness of social and economic development. This shift aligned the Bank’s efforts with the Millenium Development Goals and Sustainable Development Goals, focusing on global poverty alleviation and sustainable development.
The Bank’s approach to HCF policy mirrors these broader shifts in economic and political thought, particularly regarding the role of government versus the market. In the 1970s and early 1980s, recognising market failures in healthcare, such as information asymmetry and externalities, the Bank justified a strong government role in financing health services to ensure equity, advocating for increased public spending to address market shortcomings (WB, 1980). However, the 1986 policy study marked a turning point, advocating for reduced government involvement, user charges, health insurance, and private sector participation (WB, 1986). The 1993 World Development Report further solidified this market-oriented approach, promoting competition and market forces in healthcare financing (WB, 1993). Many studies argue that these policies exacerbated health inequities in low-income countries (Laurell and Arellano, 1996; Nuruzzaman, 2007).
By the late 1990s, the Bank moderated its position, acknowledging that neither the government nor the market alone could effectively manage healthcare. The 1997 report introduced the concept of ‘rebalancing the public-private interface’, advocating for quasi-market mechanisms and strengthening government regulation (WB, 1997). This approach was again criticised for shifting the accountability for failures onto governments, attributing shortcomings to the implementation or capacity of governments rather than recognising inherent flaws in the Bank’s approach (Harman, 2009: 4). Despite continuing to promote market-oriented policies, the 2007 Healthy Development policy document explicitly adopted the language and goals of strengthening health systems towards achieving UHC and re-emphasising the connection between the Bank’s overarching goal of poverty reduction and the financial constraints and risks that illness imposes on poor people (Tichenor and Sridhar, 2017: 2–3; WB, 2007).
Theoretical perspectives on the Bank’s influence in national policymaking: insights and Limitations
Research on the Bank’s influence on national policy arenas often draws on two scholarly traditions: transnational policy actors (TNAs) studies and sociological analyses of global norm-making. Both offer valuable insights for this study; however, as discussed below, each has its own limitations.
TNA studies explore how external actors, like the Bank, influence national policymaking by shaping the values, preferences, and capacities of national actors. Scholars in this tradition have empirically illustrated the Bank’s roles as an agenda setter, policy advisor, and policy proposal actor (e.g. Noy, 2017; Orenstein, 2008; Weyland, 2007). They argue that the Bank’s influence is wielded by providing technical expertise and proposing policy solutions, thereby shaping the policy choices of national actors, especially when these actors lack the capacity or knowledge to develop their own informed policy positions in complex policy areas like health. They explain that, by stepping into this knowledge gap, the Bank not only offers technical guidance but also steers national policy agendas, pushing governments towards specific reform paths. However, while empirically rich on the Bank’s role as a policy proposal actor, TNA studies overlook how the Bank defines the underlying problems these (policy) proposals address.
On the other hand, sociological studies highlight the influence of IOs’ norms in national policymaking. A norm, by definition, is a shared understanding within an IO that guides the ‘fram[ing] of a reform issue’ by ‘diagnos[ing] of problems followed by a set of prescriptions’, ‘codified in the forms of a script’ (Halliday et al., 2010: 84; Kentikelenis and Seabrooke, 2017: 1067). Global norm-making processes are marked by ‘iterative’ and ‘recursive’ cycles, where international and national actors engage in ongoing ‘interactions’ and ‘negotiations’, shaping and refining dominant norms (Halliday and Carruthers, 2007: 1135; Kentikelenis and Seabrooke, 2017: 1067). The norm amendment processes within national arenas, commonly reflected in law reforms, enable IOs to exert influence over national policies. Halliday and Carruthers (2007) argue that these processes are particularly influential in national agenda setting, as they involve diagnostic struggles where policy actors compete to define problems, and those who control the problem definition often gain the authority to prescribe solutions. In this context, the Bank’s resources, particularly its technical expertise, empower it significantly to shape these processes. However, while most empirical studies have focused on the Bank’s role in economic policy (e.g. bankruptcy law, Halliday and Carruthers, 2007), its influence on healthcare policy, the latter priorities include equity, access, and public welfare, introduces unique dynamics that require further exploration, as these have been largely overlooked in existing studies.
In conclusion, while TNA studies provide valuable insights into the Bank’s role in proposing policy solutions, sociological studies on global norm-making theorise its diagnostic activities but lack empirical grounding in healthcare policy. This article addresses these gaps by integrating ideational scholarship and policy process concepts into the TNAs influence framework (Orenstein, 2008), as outlined below.
Analytical framework: the Bank as a problem broker in national policymaking arenas
Before conceptualising the Bank as a problem broker in national policy arenas, this section first outlines key theoretical concepts from ideational scholarship, which are crucial for understanding the Bank’s influence. Two forms of ideas, ideas as policy problems and ideas as frames, are relevant to the analytical framework of this study (Béland, 2016; Campbell, 2002). Both concepts play a critical role in the agenda-setting stage of policy processes. Dominant policy problems often shape the policy agenda, while framing a problem can significantly influence the desirability of policy solutions (Mehta, 2011: 27, 33). Frames, as a specific form of ideas, embody discursive elements central to agenda setting and policy implementation (Agartan and Béland, 2024: 84, 86). They involve deliberative processes through which policy actors define problems to attract attention and shift them onto the policy agenda (Baumgartner and Jones, 1993). In policy implementation, frames help shape public perceptions and influence the trajectory of policies (Béland and Ridde, 2016: 10; Kangas et al., 2014).
In transnational studies, TNAs are typically identified as ‘proposal actors’, presenting ready-made policy solutions to national policymakers (Orenstein, 2008). This role underscores TNAs’ ability to engage ‘sympathetic interlocutors’ (Bazbauers, 2019) who help introduce these ideas into national venues. However, by shifting the focus to how TNAs define policy problems, I introduce the concept of the problem broker, emphasising their influence not only in proposing solutions but also in shaping the understanding and prioritisation of policy issues in national policymaking arenas.
Conceptualising the problem broker role
In policy process studies, the problem broker is an actor who assumes a strategic role in policymaking processes by framing how certain conditions are portrayed as public problems (Knaggård, 2015). The goal is to persuade policymakers to view these conditions as significant concerns that warrant attention and action (Knaggård, 2015: 452). To achieve this, problem brokers employ ‘problem frames’ to delineate various aspects of the issue. These frames encompass defining the essence of the problem (what it pertains to), determining its attribution (whether it is a public concern or someone else’s responsibility and who bears responsibility) and providing a rationale for addressing it (clarifying why action is necessary) (Schön and Rein, 1994).
Framing represents an ongoing and dynamic process in policymaking (Baumgartner and Jones, 1993). Through framing, the definition of an issue becomes part of the power dynamics because when a particular perspective successfully prevails, it effectively shapes the collective understanding of the issue (see Gusfield, 1981: 15). This process, called the ownership of the framing (Mehta, 2011: 37), underscores the close connection between the struggle to establish a dominant problem definition and its profound influence on how policymakers perceive the problem and, consequently, their decisions.
The role of knowledge in framing is undeniable (Schön and Rein, 1994). Constructing a problem frame necessitates a deep understanding of the issue, with scholarly knowledge often being one of the most authoritative sources. Problem brokers frequently harness the credibility of academic research to bolster the validity of their frames (Pielke, 2007). The Bank, recognised as a ‘knowledge empire’ and a powerhouse of information, is particularly well suited for this role. Numerous studies identify the Bank as a knowledge broker (Smith, 2008; St Clair, 2006), an actor that facilitates ‘knowledge transfer across a variety of settings’ (MacKillop et al., 2020: 335). Knowledge brokerage involves an iterative process encompassing information-related, communication-related and relationship-related activities. Knowledge brokers play a crucial role in acquiring and assessing high-quality research for its policy relevance, translating complex findings into accessible language for policymakers, and building and maintaining essential relationships to ensure the integration of research into policy decisions (Weber and Yanovitzky, 2021). They are especially influential in situations marked by complexity and uncertainty (Litfin, 1994), which are common in healthcare policy.
However, constructing a persuasive problem frame involves more than just knowledge; it necessitates underlying values that elucidate why an issue should matter and who should take action (Rochefort and Cobb, 1994). Values, which encompass a spectrum ranging from more universally accepted to ideologically driven, underscore the significance of a problem and attribute responsibility for addressing it. This is particularly evident in health (care) politics, which is deeply entangled with moral values and human identity (Carpenter, 2012). For instance, policy debates over UHC, which rests on the concepts of equity and fairness (WB, 2023; WHO, 2014), are not just about policy effectiveness but also reflect fundamental beliefs about human dignity and social responsibility.
Building on this understanding, equity emerges as a key objective of healthcare financing policy and its functions: revenue generation, pooling and purchasing. As a guiding principle, equity ensures that all individuals receive affordable, high-quality health services according to need. However, healthcare financing policy decisions might conflict with the equity objective or be made without thoroughly considering the consequences on equity, leading to persistent or even widening inequities (Rodney and Hill, 2014). Therefore, adopting a problem-driven approach is crucial in dealing with HCF problems because inequity is a core issue to address. While numerous potential solutions exist, focusing on the underlying problem ensures that future policies are designed to target and resolve the root causes of inequities.
In conclusion, this subsection examined the role of problem brokers as traditionally understood in public policy research – they are national policy actors and their role is predominantly defined by framing strategies (Knaggård, 2015). For TNAs such as the Bank, which are external to national policy processes, framing strategies are equal in importance to their problem-brokering activities within a country. The next section will provide a detailed theoretical exposition of these activities and explore framing as a discursive strategy.
The Bank’s problem-brokering activities at the country level
The Bank’s Technical Assistance (TA) activities exemplify its role as a knowledge broker, while Survey Missions (SMs), the most prominent TA activities in a country, represent its role as a problem broker. SMs are central to the Bank’s information, communication and relationship-building efforts in a country (Weber and Yanovitzky, 2021). They draw on extensive, country-specific data and are considered high-quality research outputs, with their credibility stemming from the Bank’s reputation for technical expertise (IEG, 2008: 49–57). For example, the Country Economic Memoranda provide comprehensive country data, serving as ‘a leading source of development statistics’ (Bazbauers, 2018: 182). SMs also play a crucial role ‘in formal dialogues between the Bank and the country’, contributing to the ‘discourse surrounding development and how it (is) both to be understood and pursued’ (Bazbauers, 2018: 185).
Primarily designed to measure and assess a country’s development status, SMs are often identified by the reports they produce, such as Country Economic Memoranda, Country Assistance Strategies, Economic and Sector Work, and Country Partnership Frameworks (Bazbauers, 2018: 175–176). These missions are inherently diagnostic in nature; for instance, Economic and Sector Work reports aim to ‘identify, analyse, and understand development issues within specific contexts, sectors, or countries . . . (by) generating original analytical content rather than simply disseminating or applying existing knowledge’ (WB, 2005: 14 in Bazbauers, 2018: 160). These reports feed into the Bank’s Country Assistance Strategies and Country Partnership Frameworks, which are two core diagnostic reports compiled by the Bank on individual countries, prepared every four years and tailored to national conditions like election cycles. Economic and Sector Work also contributes to specialised analytical reports on topics such as Health Sector Notes, Health Policy Reviews and poverty reduction strategies.
In summary, due to their diagnostic and probing nature, SMs essentially embody the Bank’s problem-brokering activities in a country. I examined the reports they produced, as they illustrate how the Bank articulated healthcare financing policy problems, which is essential in understanding the frames through which these issues were perceived and addressed.
Frames, framing and problem definition
The final element of the analytical framework involves the frame as a type of idea (Campbell, 2002) and framing as a strategic approach actors employ in defining problems (Mehta, 2011; Schön and Rein, 1994).
Frames are cognitive filters – ideas or mental constructs – that individuals, groups or institutions employ to make sense of the world around them (Campbell, 2002). Frames influence how these entities perceive and interpret situations, events or phenomena. For example, let us consider the concept of ‘social health insurance’ (SHI). One prominent frame views SHI as an economic tool, emphasising its capacity to pool resources and efficiently distribute the financial costs of services. On the other hand, a social solidarity lens frames SHI as a means to foster fairness and equity, highlighting the shared responsibility to ensure healthcare access regardless of socio-economic status. A market-based frame sees SHI as an avenue for introducing competition and consumer choice into healthcare. In contrast, a political frame reveals how SHI can serve as a political instrument for securing support and votes or advancing ideological agendas. Each of these frames holds a degree of validity and emphasising different aspects leads to distinct policy implications.
Framing is a discursive strategy political actors employ to influence how issues are perceived and understood (Mehta, 2011). This strategy involves presenting and organising information to highlight certain aspects of a problem while downplaying others, thus influencing the debate around an issue (Entman, 1993). While closely related, ‘problem definition’ and ‘framing’ differ, with ‘framing’ better representing the process of portraying policy problems. Defining a problem is considered a specific instance of framing (Knaggård, 2015: 453). In addition to insights from political science research and social policy debate studies (Schön and Rein, 1994), social movement scholars (Lindekilde, 2014; Snow and Benford, 1988) have shown that framing precedes action, as actors intentionally use specific patterns and interpretations to gain support for their political objectives and influence the decisions of others.
In this article, however, the focus remains exclusively on the Bank’s activities without extending the inquiry to the actions of national policy actors. This focus is maintained for two reasons. First, to provide a rigorous analysis of the Bank’s role as a problem broker, an area that remains unexplored in the existing literature to the best of my knowledge. Second, the existing scholarship already offers substantial evidence on the implications of framing in policy processes. 5
Research design
I employed a dual qualitative methodology: a case study method to chronologically outline the Bank’s approach and activities to problematising Albanian healthcare financing policy issues and its employed instruments, alongside a frame analysis utilising qualitative data from the Bank’s reports. The latter was employed to dissect and interpret layers of meaning within texts, revealing how ideas were constructed and communicated across time (Entman, 1993). Operationalisation followed Chong and Druckman’s (2007) method ‘for identifying frames in communication’ (p. 103).
The corpus for analysis consisted of eleven documents from the Bank’s Survey Mission activities in Albania, such as Economic and Sector Work (ESW), Country Assistance Strategies (CASs) and other pertinent problem-brokering TA activities, all sourced from the WB open repository website (Table 1).
Analysed documents – Survey Mission reports (1995–2013).
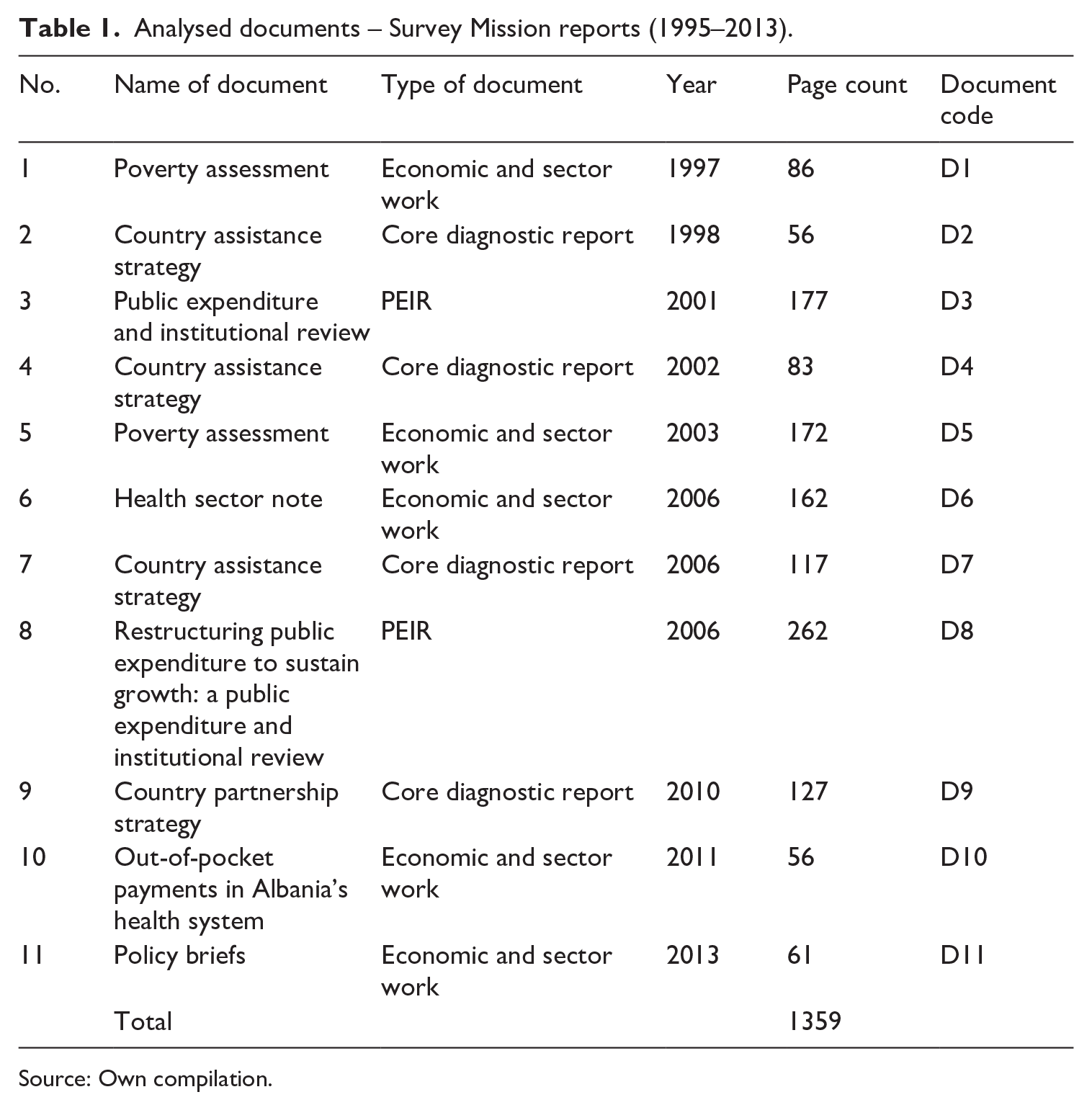
Source: Own compilation.
Inclusion criteria for document selection were established as follows: (1) documents must be authored by the Bank and/or its affiliated experts; (2) they must not contain disclaimers stating that the document does not necessarily represent the opinions of the Bank; (3) they must specifically address healthcare financing policy topics; and (4) they must have been published within the observation period from 1995 to 2013.
I began the analysis by familiarising myself with the texts. Using MAXQDA software (version 24), keyword searches of ‘health’, ‘healthcare’, ‘health financing’, ‘coverage’, ‘access’, ‘health insurance’ and ‘social health insurance’ identified text segments. Initially, qualitative content analysis of these segments outlined the Bank’s problem-brokering activities and the various instruments and tools the Bank utilised in presenting, illustrating and substantiating policy problems. The frame analysis followed. This entailed coding excerpts followed by a combined approach of a deductive and an inductive strategy. As informed by the literature (section ‘The Bank in health: evolution, influence and theoretical perspectives’), I relied on the normative frame of the Bank’s health discourse. In the context of healthcare financing reforms, it pertains to principles of ensuring service equity and granting financial protection to the entire population. The functional frame, which emerged inductively from the text, involves the practical, operational aspects and challenges of implementing SHI. The text was coded by marking instances of each frame and assessing how they relate to each other and how they collectively contribute to the overall argument presented in the texts.
Background: Albania and its healthcare financing reforms
The development of Albania’s healthcare system during communism shared many characteristics with other Central and Eastern European (CEE) countries. 6 Under the communist government, influenced by the Soviet Semashko model, Albania nationalised all private clinics, hospitals, and diagnostic centres, placing the healthcare system under the centralised control of the Ministry of Health. Services were funded entirely through state revenues, with all medical staff employed by the government. The system relied on a labour-intensive network of facilities, with a distinct separation between primary, ambulatory, and hospital care. This model suffered from low funding, limited technological advancements, and a complete ban on private medical practice (Druga, 2021; Nuri, 2002). Despite these constraints, however, Albania managed to maintain relatively universal healthcare access (Nuri, 2002).
Following the transition to political pluralism and a market economy in 1991, the country faced intensified fiscal pressures, which exacerbated existing challenges. The extensive healthcare infrastructure, once a point of national pride, became unsustainable due to limited resources (Nuri, 2002). In response, the government introduced a series of reforms, beginning with the decentralisation and privatisation of healthcare services (Nuri, 2002: 15). A key milestone in this transformation occurred in 1994 when the SHI law adoption marked a fundamental shift in HCF policy. Under this law, entitlements changed from a universal model to a contribution-based system, restricting healthcare access to those paying contributions, primarily formal sector employees (Kaminska et al., 2021).
The Bank’s involvement in Albania began in 1991, with preparations for the country’s admission to the World Bank Group that was realised in October 1991. Despite the Bank’s early engagement in healthcare reforms, its influence on healthcare financing policy change and SHI introduction remained limited. Between 1992 and 1993, the Bank strongly opposed the introduction of a SHI model, citing Albania’s lack of essential prerequisites for its successful implementation, such as a formal labour market, administrative capacity, sound financial management, accurate cost estimations, and effective reimbursement mechanisms. In addition, the Bank raised concerns that the SHI law conflicted with Albania’s broader social sector reforms, particularly pension reform, which the Bank had already endorsed. In light of these challenges, the Bank recommended maintaining a state-funded healthcare system until Albania’s economic and institutional conditions improved. Despite these warnings, national actors disregarded the Bank’s recommendations to keep the old financing system (Druga, 2022).
Implementation began with the establishment of the Health Insurance Institute in 1995. However, public health expenditures continued to rely heavily on government funds rather than social health contributions (Kaminska et al., 2021). By the early 2010s, the latter accounted for less than one-quarter of public health expenditure, with out-of-pocket payments (OOPs) becoming the dominant source of total health expenditure, up to 58% and 59% of them (Figure 1).
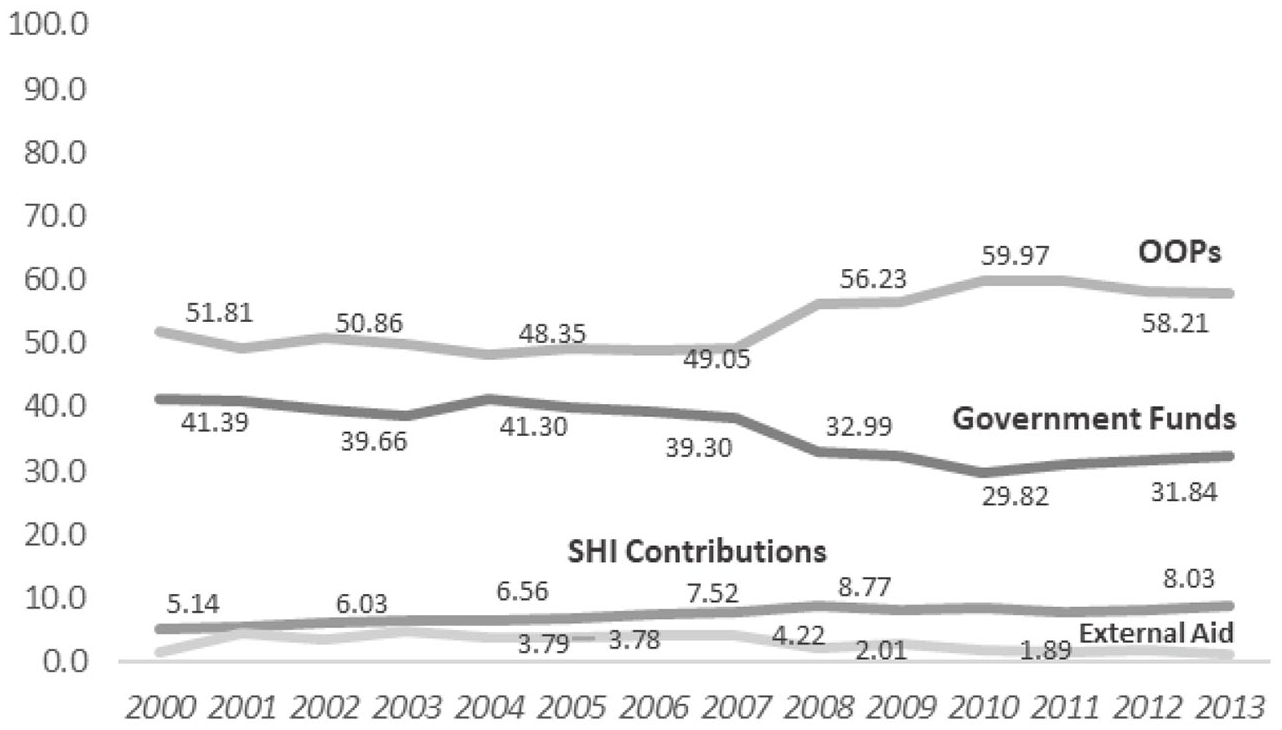
Health expenditures in Albania (2000–2013). 7
Although the Bank’s influence on the introduction of SHI was limited, it remained actively engaged in HCF reforms through three lending projects, 8 all of which were notably implemented without any conditionality (Druga, 2024). As illustrated in the next sections, this non-coercive approach, grounded in advisory support and technical assistance, enabled the Bank to maintain a close relationship with the government, which allowed it to continue critiquing policy decisions while providing expert guidance. By maintaining this ongoing involvement, the Bank ensured its presence in the reform processes, positioning itself as an actor capable of shaping how problems were understood and, therewith, the direction of future reforms. Over time, this advisory role gained traction as resistance to the Bank’s ideas began to wane. By the early 2010s, some national actors started to adopt the Bank’s framing of policy issues, leveraging the Bank’s problematisation of HCF to garner political support and further their own agendas. This shift in perspective became particularly evident during the 2013 parliamentary election campaign when healthcare issues took centre stage. Politicians from the Socialist Party of Albania echoed the Bank’s concerns about the SHI law, arguing it was unsuitable for Albania due to the informality of the labour market and high unemployment rates (Beqja, 2013). They emphasised the need to address inequities in access to healthcare, calling for ‘a radical reform of the healthcare system, ensuring no citizen is excluded’ (Spahiu, 2013). This alignment with the Bank’s concerns marked a critical moment, highlighting the Bank’s growing influence in shaping national policy discourse and its role in framing HCF issues as critical for the country’s future.
The Bank as a problem broker in Albanian healthcare financing reforms
This section first delineates the Bank’s approach to problematising issues in Albanian health financing policy from 1995 to 2013 by shedding light on the activities it engaged in and the instruments it employed. Following this identification, I illustrate the Bank’s framing of policy issues. A more comprehensive discussion of the Bank’s role as a problem broker in this context is presented in the final section.
The Bank’s diagnostic activities in Albanian healthcare financing reforms
From 1995 to 2013, the Bank gained a comprehensive understanding of the problems in Albanian healthcare financing reforms. The Bank employed a variety of statistical tools and analytical instruments that evolved with time, providing a detailed understanding of the Albanian socio-economic landscape and the financial and institutional challenges in the country’s healthcare system.
In the 1990s, as Albania struggled with widespread poverty and economic instability, the Bank’s approach to healthcare financing was intricately linked to broader poverty reduction goals, economic growth and human development. This phase was marked by the use of statistical tools designed to gather detailed data and construct poverty indicators, which were crucial for understanding the socio-economic context of the healthcare financing reform.
One of the primary statistical tools was the Household Budget Survey (HBS). Initiated in 1993–1994 and conducted by the newly established statistical agency with training and support from the Bank, the HBS collected detailed information on household income, expenditure and consumption patterns. In the context of healthcare financing reforms, the HBS served as a critical diagnostic tool, providing insights into healthcare expenditure. This data was instrumental in identifying the financial barriers faced by households and helped the Bank understand the economic burden of healthcare costs on different segments of the population. A further statistical tool was the Living Standards Measurement Study (LSMS). Initiated in 1996, the LSMS was a comprehensive research programme organised by the Bank to collect high-quality data on household living standards, including income, expenditure and socio-economic characteristics. The data from LSMS supported several analyses on poverty and economic development, enriching the Bank’s understanding of the multifaceted dimensions of poverty in Albania and their implications for healthcare financing policy.
Based on these two statistical tools, the Bank produced the Poverty Assessment Report (PAR) (initiated in the late 1990s and presented in 2003), which offered an in-depth evaluation of the Albanian population’s economic conditions and living standards. This report shed light on income distribution, access to basic services such as healthcare and other socio-economic indicators, providing a holistic understanding of poverty dynamics in the country (D5: 6). The findings from this report were crucial not only in highlighting systemic issues within Albania’s healthcare financing system, but also in informing the Bank’s subsequent activities (D6, D7, D10).
By the 2000s, the Bank’s approach had shifted from focusing solely on poverty reduction to enhancing governance and addressing institutional weaknesses by highlighting the importance of establishing transparent, efficient and accountable public institutions. The Country Assistance Strategy, a core diagnostic instrument published by the Bank in 2002, underlined the critical need for regular household surveys and robust monitoring and evaluation systems, emphasising data-driven policymaking as essential for achieving sustained progress in healthcare financing reforms (D4: 11).
A noteworthy evolution in the Bank’s problem-driven approach was the incorporation of analytical instruments alongside statistical tools. The Public Expenditure and Institutional Review (PEIR) was introduced in 2001 to evaluate the budgetary planning process and institutional frameworks for managing public expenditure. This instrument aimed to enhance the efficiency and accountability of public health spending and lay the groundwork for better budgetary planning and medium-term expenditure frameworks (D3: 9, 80).
By the late 2000s and early 2010s, the Bank’s view on the SHI reform issues was substantiated by robust evidence gained from statistical tools and analytical instruments. The LSMSs (in 2002 and 2005) and the PEIRs (in 2001 and 2006) further enriched the Bank’s understanding of income and non-income dimensions of poverty. They identified key shortcomings in Albania’s health finance system, such as high out-of-pocket spending, inequitable resource allocation and inefficiencies in provider payment systems (D8). Other analytical instruments dedicated to healthcare reforms, such as the Health Sector Note (D6) and the Policy Brief (D11), provided detailed insights into problems in revenue collection, pooling and purchasing policies.
To summarise, examining the Bank’s activities from 1995 to 2013 revealed the problem-driven approach to healthcare financing policy. The Bank relied on statistical tools, such as the HBS and LSMS, as well as analytical instruments, including PEIR, the Health Sector Note and Policy Briefs to understand and address healthcare financing problems. Furthermore, as explored in the following subsection, these tools and instruments have been crucial in shaping the Bank’s discourse, underpinning it with a well-evidenced framing of the policy problems.
How did the Bank frame the Albanian healthcare financing policy problems?
Frame analysis of the Bank reports identified two central frames: a normative and a functional frame. The normative frame underscored health equity and financial protection principles – health equity denotes the absence of unjust differences in healthcare access among diverse population groups (Braveman et al., 2018), and financial protection in health ensures that healthcare costs do not cause financial burdens for individuals or households (WHO, 2000). The functional frame underlined the practical intricacies of implementing healthcare financing reforms.
The framing of health financing policy problems began to take shape in the late 1990s with a clear normative stance – it involved underlying values about what is fair, just and desirable in the healthcare system. In the early 2000s, alongside the normative frame, the functional frame emerged. The normative frame, however, dominated the Bank’s discourse, appearing in over 62% of the text segments (Table 2). By the mid-2000s, a notable aspect of the Bank’s discourse was the amplifying of the normative frame with the functional frame’s influence upon it.
The composition of frames in the WB analysed texts.
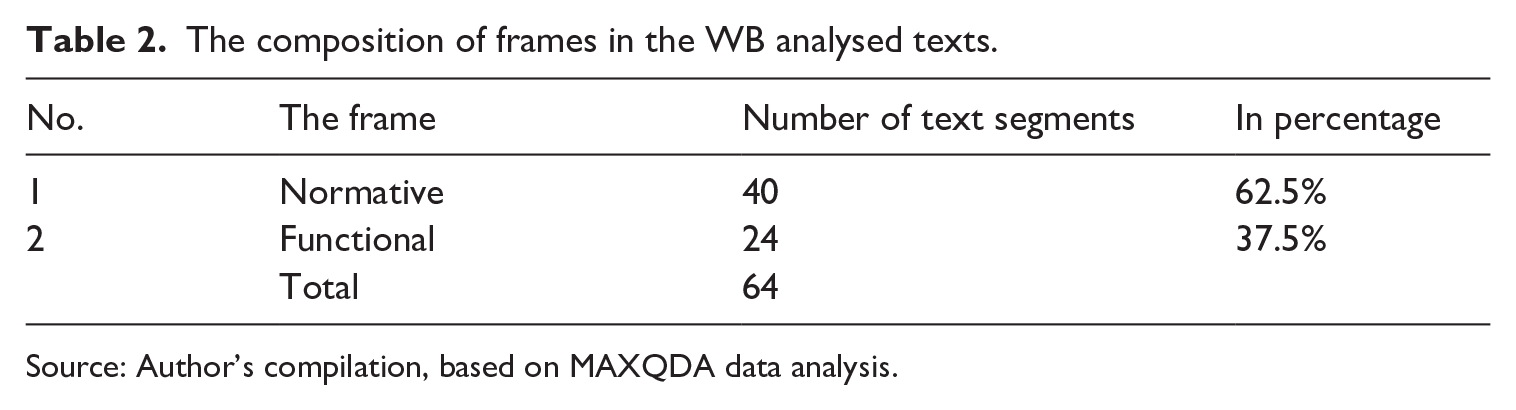
Source: Author’s compilation, based on MAXQDA data analysis.
By the late 1990s, the Bank’s discourse began incorporating normative elements. For instance, the Poverty Assessment Report 1997 indicated, ‘Prior to 1995, access to health services was not limited by ability-to-pay barriers as the healthcare delivery system was fully financed from the state budget’ (D1: 19). This statement, while factual, implicitly values a healthcare system where access is not constrained by financial means. By highlighting the absence of ‘ability-to-pay barriers’, the report suggests a normative preference for an accessible healthcare system, regardless of economic status. Furthermore, the report emphasised that ‘inability to pay was preventing some sick people from receiving healthcare’ (D1: 19). Identifying financial barriers implies that they are undesirable and that this problem should be addressed. Including poignant quotes in the report, such as the remark from a woman in Lezha who stated, ‘they do not get help; the poor are left to die’ (D1: 19), is a powerful ethical appeal. This quote humanises the statistics, appealing to one’s sense of justice and morality. The emotional weight of such personal testimonies amplifies the normative critique of the existing policy model. Moreover, the historical context provided by the report, contrasting the pre-1995 system with the post-1995 situation, carries significant normative weight. By documenting the negative impacts of financial barriers introduced with the SHI reform, the report implicitly critiques these reforms and suggests a preference for the earlier state-funded model. This comparison indicates that the shift towards a system with financial barriers is a step backwards, reinforcing the normative position that healthcare services should be universally accessible.
The normative frame remains prominent in the Bank’s discourse as its diagnostic activities increasingly contribute to uncovering problems in healthcare financing policy. The first problem is the inadequacy of coverage. For instance, the Poverty Assessment Report 2003 (D5: 106-7) reveals that ‘only about 39% of the total population reports having health insurance’, highlighting a normative issue by implicitly questioning the equity of the SHI model. By underlining that nearly two-thirds of the population lacked coverage, the Bank suggests that the existing healthcare financing model was insufficient in ensuring widespread access to healthcare benefits. Second, the frame emphasises geographical disparities and unequal access to healthcare services within the Albanian population by illustrating that ‘People in urban areas, especially Tirana (the capital), are much more likely to have a (health insurance) license than people living in rural areas’ (D5: 106-7). Third, the additional statistics that ‘only 40% of children were issued a health insurance license’ (D5: 106-7) despite existing state funding for all children highlights a concerning issue regarding children’s access to healthcare services. It underscores the inequitable distribution of health insurance benefits, especially among vulnerable groups like children, who ideally should have comprehensive coverage. Thus, the normative concern extends to a principled dimension, emphasising the need for reforms in expanding coverage to include all population segments and mitigate financial risks associated with healthcare costs.
In addition, the Bank’s normative framing in the 2000s reveals a significant ethical concern regarding the reliance on out-of-pocket payments (OOPs) for healthcare services. The Country Assistance Strategy Report of 2002 notes that OOPs constituted one-third of total healthcare expenditure, highlighting systemic inequity (D4: x). This reliance on OOPs was recognised not only as a substantial financial burden but also as a factor pushing individuals ‘to fall into poverty or deeper into it’, as stated in the Poverty Assessment Report (D5: 80-6). By spotlighting the economic hardship caused by high OOPs, the Bank shifts the discourse from merely identifying economic inefficiencies in the healthcare financing model to addressing the ethical implications on human well-being – the Bank frames healthcare financing policy problems as a moral concern rather than just a technical one. This normative framing demonstrates how problem brokering involves diagnosing issues while embedding ethical considerations into the discourse.
In parallel with this normative discourse, a functional perspective emerged in the early 2000s, highlighting the complex challenges associated with implementing the SHI model, particularly regarding collecting health insurance contributions. The Bank’s framing focuses on pragmatic issues of policy implementation. It underscores the operational difficulties encountered in enforcing contributions, especially among individuals working in agriculture and informal sectors (D5: 107). The Bank’s analysis reveals that the predominance of informal employment complicates efforts to ensure the steady payment of health insurance contributions.
By the mid- and late 2000s, this functional perspective expanded to address a broader range of policy implementation problems. It identified issues such as ‘the absence of a robust formal labour market’, inadequate administrative capacity for collecting contributions, and insufficient regulatory and oversight structures – all of which impeded the effective collection of contributions necessary for sustaining the healthcare system (D5: 121). The functional frame offered a detailed examination of the systemic inefficiencies undermining SHI implementation. It noted that in ‘low and middle-income countries where a large share of the labour force is either in the informal sector or unsalaried, payroll tax-based contribution systems create incentives for non-participation’ (D5: 122). This misalignment with Albania’s labour market realities was starkly evident, as only ‘7% of public spending (is) derived from payroll tax contributions to the Health Insurance Institute’ (D5: 120). Consequently, these discrepancies resulted in substantial gaps in health insurance coverage, undermining the healthcare system’s financial stability and its ability to provide comprehensive services. Through this functional frame, problem brokering is illustrated by focusing on the practical barriers and operational challenges in healthcare financing policy, thereby guiding policy adjustments to better align with local labour market conditions and improve system effectiveness.
The normative frame has remained dominant over time, particularly regarding financial protection. This persistence is evident in the Bank’s ongoing discourse, which continues to highlight extensive OOPs and corruption in healthcare delivery (D6; D9; D10; D11). For example, the Bank reports that ‘Healthcare remains a critical area in which individual households are affected by corruption, with close to a third of survey respondents reporting that they have paid a bribe to receive medical attention’ (D9: 12). The emphasis on OOPs and corruption underscores a crucial normative concern: the moral imperative to protect individuals, particularly the poor, from catastrophic health expenditure that can deepen poverty. This ethical dimension is highlighted by data showing that ‘nearly 60 percent of healthcare funding’ comes from OOPs, resulting in significant disparities in access to services (D9: 12).
In addition to this persistent normative focus, the mid-2000s saw the Bank’s discourse increasingly emphasise the interplay between the normative and functional frames. This interplay underscores how operational problems inherent in the Albanian SHI model have exacerbated disparities in healthcare access and undermined population financial protection. This dynamic is illustrated by the Bank’s remark that when faced with an informal labour market, the SHI model exacerbates inequalities, leading to a ‘better’ system for the formally employed and an inadequate one for others (D11: 28); hence, revealing how operational problems not only affect the effectiveness of health financing but also deepen the ethical issues related to equity and access.
In conclusion, this empirical section illustrated the Bank’s role as a problem broker in Albanian HCF reforms from 1995 to 2013 by exemplifying the knowledge power of a TNA through targeted diagnostic activities and discursive strategies in addressing complex national healthcare policy problems. The Bank first engaged in diagnostic activities, employing statistical tools such as HBS and LSMS and analytical instruments including PAR, PEIR, Health Sector Notes and Policy Briefs, which were pivotal in identifying and exposing policy problems. In addition, the Bank utilised discursive strategies and framed these problems through normative and functional lenses, highlighting ethical concerns related to equity and access alongside policy implementation challenges. This framing strategy aimed to bring these problems to the forefront of national policy debates and pave the way for future policy change.
Discussions and final remarks
The article theorises a novel ideational role for the Bank as a TNA influencing national policy processes, as illustrated by its involvement in Albanian HCF reforms. It portrays the Bank as a transnational problem broker, a concept traditionally associated with national policy actors, which involves the framing of policy problems to increase attention and prompt future action (Knaggård, 2015). While the Bank, as an external actor, lacks institutional power within national arenas (Orenstein, 2008), its lending and TA activities facilitate access to and close relationships with the government and national policy actors. As illustrated above, TA activities like Survey Missions enabled the Bank to identify and understand national policy issues. Thus, a transnational problem broker, unlike a traditional national problem broker, is defined not only by framing strategies but also by engaging in diagnostic activities, recognised in the literature as knowledge-making and knowledge-sharing processes (Stone, 2000), but with a probing nature.
Building on this concept, the analysis revealed both the frames and the framing strategy employed by the Bank in Albania. Specifically, two frames were identified: the normative frame, which views health as a fundamental right, and the functional frame, which assesses efficiency as an economic parameter. These findings align with previous research on the Bank’s role in social and healthcare policy (Noy, 2017; Weyland, 2007), with Noy (2017) noting the significant, ‘more . . . than expected’ emphasis on the normative frame (p. 108). The analysis further illustrated how the Bank leveraged both frames to highlight operational challenges and equity principles. While the functional frame gained prominence over time due to evolving understandings of reform issues during implementation, the normative frame remained dominant. The Bank’s discourse evolved to emphasise a causal link between functional and normative issues, showing how growing functional concerns exacerbated normative problems. This approach underscores the Bank’s strategy of constructing a persuasive discourse to shape policymakers’ perceptions and engagement with reform challenges.
These findings deepen our understanding of the influential role of the Bank’s ideas and knowledge in national policy processes (Noy, 2017; Orenstein, 2008; Weyland, 2007), extending beyond the previously identified proposal actor role in TNA studies (Orenstein, 2008). These roles represent distinct but complementary pathways for TNA influence: one redefines policy problems to shape national policy actors’ perceptions and priorities, thereby influencing policy agendas and future policy directions, while the other proposes specific policy solutions to broaden the range of choices available for policy decisions. The actions of a problem broker, however, extend far beyond agenda setting. A problem broker has the ability to influence the entire policy process by determining which issues are prioritised, how they are interpreted, and the context in which solutions are proposed and implemented. This capacity to shape the policy agenda, which is also highlighted by sociological scholars in global norm-making processes (Halliday and Carruthers, 2007), can carry significant long-term implications for the trajectory of policy development. The study revealed that the Bank’s diagnostic activities and problem-framing strategies in Albania took place during policy development (the implementation of reforms). This is particularly significant for a TNA like the Bank, which engages in many TA activities and commits both material and financial resources to policy implementation, as evidenced by its health lending in Albania (Druga, 2024). This level of engagement is relatively uncommon with other TNAs.
The article focuses exclusively on the Bank’s activities without examining its interaction with national policy actors and limits the investigation period to 2013, both of which open avenues for future research. Future research may also explore the portability 9 of ‘the problem broker’ role to other policy areas for the Bank and potentially to other TNAs. Notably, this study underscores the importance of Survey Missions as a subtle yet pervasive component of the Bank’s TA activities, a finding that resonates with Bazbauers’ (2018) assertion that SMs, while less visible, are integral to the Bank’s broader influence (p. 175). In this context, in line with Smith (2008: 239), the analysis highlights how the Bank mobilises knowledge ‘as an instrument to achieve similar outcomes’ as its lending conditionalities.
Footnotes
Acknowledgements
I sincerely thank Hilde van Meegdenburg for her guidance and support throughout this research. Any remaining errors are entirely my own.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Proofreading of this article was financially supported by Socium–Research Center on Inequality and Social Policy at the University of Bremen, Germany.