
Abstract
Disability-targeted cash transfers are increasingly used by governments in low- and middle-income countries as a tool to address poverty and exclusion among people with disabilities. However, in many settings, accurate estimates of coverage and an understanding of factors affecting uptake are needed for effective delivery. This study explores coverage of the Disability Allowance in the Maldives, an unconditional, non-means tested cash transfer (2000 MVR or US$130 per month) and factors affecting uptake. It uses mixed methods, combining data from a nationally representative population-based survey with qualitative research among people with disabilities who are and are not receiving the Disability Allowance. This research found that 25.6% of people with disabilities across the Maldives are receiving the Disability Allowance. Coverage was lowest for women, older adults, people living in the capital (Malé), wealthier households and people with sensory impairments. Factors affecting uptake included lack of information about the programme, perceptions of disability and eligibility criteria, geographical and financial factors, and stigma.
Introduction
There is increasing recognition that social protection is an important tool for alleviating poverty. Social protection is referenced directly or indirectly in at least four of the seven Sustainable Development Goals (SDGs) and is considered instrumental to achieving others, particularly SDG 1 ‘ending poverty in all its forms’ (United Nations, 2015). The term ‘social protection’ encompasses contributory schemes (social insurance) and social assistance schemes, which are being increasingly implemented by governments, in low- and middle-income countries (LMICs) in particular. These schemes are non-contributory transfers of cash or kind to groups that are vulnerable or in poverty (Barrientos, 2011).
People with disabilities make up over 15% of the global population and have a higher need for social protection because they are significantly more likely to be experiencing poverty and social exclusion (Banks et al., 2017; United Nations, 2019). In addition to need, their right to inclusion in social protection programmes is reflected in international treaties such as Article 28 of the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) as well as the Articles 22 and 25 of the Universal Declaration of Human Rights (United Nations, 2006; United Nations General Assembly, 1948). These treaties confirm that in order to fulfil the rights to inclusion in social protection, states must ensure that people with disabilities have equitable access to mainstream social protection programmes where disability is not an explicit condition of inclusion, such as social security and health insurance (Devandas Aguilar, 2017). In addition, states may introduce disability-targeted programmes to improve access to or offset the cost of additional disability-related goods and services such as accessible transport, personal assistance, specialist healthcare and assistive devices (Devandas Aguilar, 2017; International Labour Organization, 2017; Mitra et al., 2017).
The International Labour Organization (ILO) reports that 170 countries provide periodic cash transfers to people with disabilities (International Labour Organization, 2017). However, information is lacking on the reach of these programmes (Banks et al., 2016). Modelled estimates suggest that only 27.8% of people with severe disabilities globally receive a disability-targeted transfer, with significant regional differences (9.4% in Asia & the Pacific, 97.9% in Eastern Europe; no data from Africa). However, these estimates are modelled based on the 15% global estimate of disability from the 2002–2003 World Health Surveys, rather than through direct survey. Thus, accurate estimates of social protection coverage among people with disabilities are needed to inform planning at national levels. Furthermore, it is important to understand individual and system-level factors that affect access to programmes, which can influence both programme coverage and the effectiveness and longevity of programmes (Devereux et al., 2017; Kidd, 2017).
Consequently, this study uses mixed methods, including a nationally representative population-based survey and in-depth interviews, to assess national coverage of the Disability Allowance among people with disabilities in the Maldives and to explore factors affecting uptake. The Maldives is a compelling setting to explore access to a disability-targeted cash transfer, as it is one of the largest cash transfers in an LMIC setting (Walsham et al., 2018). Furthermore, it is a universal scheme that is open to all citizens with an eligible disability, and does not include other criteria such as inability to work or living in poverty. These additional criteria have commonly excluded many people with disabilities from social assistance, who may still require a cash transfer to cover disability-related extra costs even if they are working or do not meet a national definition of poverty, which is typically based on the consumption needs of people without disabilities (Banks et al., 2016; Mont and Cote, 2020). This research is thus relevant to other countries as they seek to design and implement new – or adapt existing – disability-targeted social assistance programmes.
Disability-targeted social protection in the Maldives
The Maldives has an estimated population of 540,542 people dispersed across 185 islands (World Bank, 2020). A third of the population live in the capital, Malé, where central government and tertiary health facilities are based (National Bureau of Statistics, 2014). The Maldives is categorised as an upper middle-income country, although challenges remain in equitable service provision and economic diversification (National Bureau of Statistics, 2014).
A national population-based survey found 6.8% of the Maldivian population have a disability using the Washington Group Short Set Enhanced (Banks et al., 2020). People with disabilities and their households were more likely to be living in poverty and faced participation restrictions in areas such as school, work and social life compared with people without disabilities (Banks et al., 2020).
The right to social protection for persons with disabilities is specified in Articles 17 and 35 of the Maldivian Constitution (Government of Maldives, 2008). The Maldives ratified the UNCRPD in 2010, and in the same year, enacted the Protection of the Rights of Persons with Disabilities and Provisions for Financial Assistance Act (or Disability Act) (Government of Maldives, 2010). A central provision of the Disability Act was the creation of the Disability Allowance.
The Disability Allowance is non-contributory, non-means tested, unconditional cash transfer of 2000 Maldivian Rufiyaa per month (US$130). Eligibility is restricted to Maldivians with disabilities, defined as ‘all persons with long term physical, psychological, sensory or mental illness facing difficulty in participating in community activities to the same level as others shall be considered as persons with disabilities’ (Government of Maldives, 2010) . The definition of disability is therefore largely in-line with the UNCRPD. The National Social Protection Agency (NSPA) is the implementing body for all social protection programmes, including the Disability Allowance. Applications are accepted on a rolling basis and can be sent to either Island Councils or NSPA’s office in Malé. Application is by self-selection, and applicants must submit medical documentation of an impairment from a relevant specialist. In some cases, NSPA staff may also perform a ‘functional assessment’ based on the Disability Certification and Assessment Guideline, on an ad hoc basis if they deem further information is needed (National Social Protection Agency, 2010).
In addition to the Disability Allowance, people with disabilities may receive other cash transfers. For example, the Old Age Pension (US$320, equivalent to 5000 Maldivian Rufiyaa) is available for all people aged 65 years and older, while the Single Parent Allowance and the Foster Parent Allowance are available for people who are currently unmarried and caring for children aged under 18 years who are living with them (US$65 per child per month). NSPA also runs the Medical Welfare programme, a non-targeted programme for medical services and products not covered under Aasandha, the national healthcare financing scheme. Importantly, people with disabilities – with a certification of impairment – can apply for assistive devices and medication not already covered by Aasandha. The Disability Allowance can be received concurrently with any of these other schemes.
A process evaluation of the Disability Allowance conducted in 2016/17 highlighted issues linked to implementer’s delivery and intervention design that could affect the programme’s reach (Hameed et al., 2022). These included limited actions being taken to drive recruitment, to communicate eligibility criteria, and to manage inconsistent practice among central and island-level actors during and after applications. This article first details the methods used in the present study, then presents results showing coverage of the Disability Allowance and factors affecting uptake from beneficiaries’ perspectives. The article concludes with a discussion of the findings in relation to other similar works, and implications for design and implementation of social protection programmes both within and outside of the Maldives.
Methods
This study used a mixed-methods approach. A nationally representative population-based survey estimated the coverage and predictors of enrolment, while a survey and in-depth interviews of Disability Allowance recipients and non-recipients explored factors affecting uptake. All data were collected in July–December 2017.
Data collection
Population-based survey
A nationally representative, population-based survey was conducted to estimate the prevalence of disability and coverage of the Disability Allowance in the Maldives.
A target sample size was set at 6500 people aged 2 years and older, based on an expected prevalence of disability of 7%, response rate of 75%, confidence level of 95%, design effect of 1.5 and precision of 15%. A two-stage sampling strategy was used, in line with methods of similar studies (Kuper et al., 2006; Marella et al., 2016). In the first stage, probability proportionate to size sampling was used to identify 52 clusters (defined as an island enumeration area) using the 2014 Maldivian Census as the sampling frame (National Bureau of Statistics, 2014). In the second stage, modified compact segment sampling was used to enumerate 125 Maldivian citizens aged 2 + years (including non-responders) in each cluster. When the selected segment did not include 125 eligible people, another segment from that enumeration area was chosen at random and recruitment continued until the cluster threshold was reached.
Household details (e.g. housing characteristics, indicators of socioeconomic status, household membership) were collected from each participating household. Furthermore, each household member (2 + years) was screened for disability and asked about their participation in different social protection schemes, including the Disability Allowance.
Data were collected using ODK-based questionnaires on computer tablets. All questionnaires were translated into Dhivehi (Maldivian language) and pilot tested.
Overall, 5472 people were included in the population-based survey (response rate: 82%). Overall, 402 people met this study’s definition of disability (n = 368, 91.5% by the Washington Group – Extended Question Set [WG-ES] and anxiety/depression criteria; n = 34, 8.5% by additional question on health conditions).
Survey of Disability Allowance recipients
An additional 161 newly enrolled recipients of the Disability Allowance were also recruited from NSPA registers. Recipients who were newly enrolled each month between July and December 2017 were contacted by phone or in-person and invited to participate. Both new recipients from the NSPA registers and existing recipients identified in the population-based survey were asked about their experience applying for the Disability Allowance, including details on medical and functional assessments and on out-of-pocket spending for costs associated with applying. Median costs and interquartile ranges (IQR) were derived from total expenditures across categories (e.g. for medical/functional assessment, travel, gathering documents).
Qualitative data
Qualitative research was also undertaken to complement the quantitative data, and to further explore the experience of people with disabilities in accessing the Disability Allowance.
Participants were purposively sampled using data from the population-based survey, ensuring that the sample included people with disabilities who were and were not receiving the Allowance, males and females, children and adults, and people with a range of impairment types.
Interviews were semi-structured with extensive probing, and questions included need for social protection, knowledge of the Disability Allowance, eligibility, facilitators and barriers to inclusion. For Allowance recipients, views on the programme, experience of application process, and level of satisfaction were explored.
All interviews were conducted in Dhivehi by SH, who is a female Maldivian researcher and has extensive experience in qualitative methods and disability research. Interviews were audio-recorded after obtaining informed consent, and transcribed.
A total of 23 people with disabilities were selected for in-depth interviews – 18 were direct interviews and 5 were proxy interviews with caregivers (in the presence of the person with disability). Of these, 11 were female and 12 were male; 9 were based in Malé, and 14 from other islands; and comprised the following impairment types: physical (n = 5) sensory (n = 11), intellectual/cognitive (n = 4), psychosocial (n = 8), multiple (n = 3). 10 were Disability Allowance recipients and 13 were non-recipients.
Measuring disability
To assess coverage of the Disability Allowance, this study employed tools to measure disability that most closely matched the eligibility criteria for the programme as outlined in the Disability Assessment and Certification Guideline (National Social Protection Agency, 2010). Disability was only assessed in people aged 2 + given the shortage of validated survey tools for younger ages (Mactaggart et al., 2016).
The main tool for measuring disability was the Washington Group question sets, which are internationally validated and recommended tools for measuring disability (Washington Group on Disability Statistics, 2009). All enumerated individuals were screened for disability using the Washington Group Short Set Enhanced for adults (aged 18 +) and the United Nations International Children’s Emergency Fund (UNICEF)-Washington Group Child Functioning for children (age-specific modules for children aged 2–4 and 5–17) (Washington Group on Disability Statistics, 2011; Washington Group on Disability Statistics and UNICEF, 2016). The question sets include 9–11 questions depending on the age of the participant. Questions ask about the level of difficulty (none, some, a lot, cannot do) that the individual faces in performing everyday activities (e.g. seeing, hearing walking). In addition, adults (18 +) were asked about the frequency and intensity of symptoms for anxiety and depression, while children (5–17) were asked about frequency only. These questions are also in line with eligibility criteria for the Disability Allowance in the Maldives. For example, the Disability Allowance assessment and certification guidelines cover vision, hearing, speech, physical, intellectual and psychosocial impairments of at least a moderate severity, which is similar to the domains covered in the Washington Group question sets and the cut-offs used. In addition, assessments of eligibility take into account functioning with available assistive and corrective devices, as does the Washington Group questions.
The study definition of disability differed from the Washington Group definition of disability in two ways to better align with Disability Allowance eligibility criteria. First, additional questions were added for people reporting anxiety and depression. Participants screening positive for depression/anxiety through the Washington Group questions were asked additional questions on if their symptoms had an impact of on school, work (in and out of the home) and social relationships. Second, all participants were asked an additional question after the Washington Group screening on if they had a physical or mental impairment that had a substantial and long-term negative effect on their ability to do typical daily activities. Respondents answering affirmatively were asked to specify their health condition, which was then reviewed by the study team to ensure the inclusion of conditions that may not be captured by the Washington Group questions but would be eligible for the Disability Allowance. 1
In summary, individuals were defined as having a disability if they fulfilled at least one of the following criteria:
Experiencing ‘a lot of difficulty’ or ‘cannot do’ for at least one activity in the WG-ES or UNICEF Child Functioning module.
Experiencing symptoms of anxiety or depression daily with an intensity of symptoms described as ‘a lot’ (adults 18 +) or experiencing symptoms daily (children 5–17 years). Depression/anxiety also had to have an impact on school, work (in and out of the home) or social relationships.
Diagnosis of a health condition that meets Disability Allowance eligibility criteria (e.g. autism, psychosocial impairment).
Participants self-reported on their level of functioning, although proxies were used for children 10 years and younger, people with impairments that severely affected their ability to understand/communicate and household members that were not reachable after a minimum of three revisits.
Data analysis
Quantitative data were analysed using STATA 16.
Coverage of the Disability Allowance was estimated by the dividing the number of people enrolled in the Disability Allowance by the total number of people meeting the study definition of disability. Enrolment in other programmes was determined by dividing the number of recipients by the number of people eligible (e.g. people over 65 years for the Old Age Pension) or by the total population (Single Parent Allowance, Foster Parent Allowance), disaggregated by disability status.
Comparisons of Disability Allowance coverage by subgroup was undertaken using multivariate regression. Regression analyses included variables for the individual’s age and gender and the household’s location (Malé vs atolls outside Malé). Impairment types were grouped as physical (functional limitation in mobility, upper body), cognitive (functional limitation in communicating, cognition), sensory (functional limitation in seeing, hearing) and psychosocial (anxiety, depression, autism and other write-in mental health conditions). Income quartiles were derived from household per capita income from all sources (including social assistance) among all households in the population-based survey.
Qualitative data were analysed thematically using NVivo 11. Transcripts were grouped and analysed according to selection criteria (e.g. location, gender, impairment type, receipt of Disability Allowance). Transcripts were read and re-read to allow familiarisation with the data. Codes were generated, expanded, refined and grouped into themes in an iterative process. Data analysis was conducted in Dhivehi to prevent loss in translation. Specific quotes were identified and translated to illustrate key points.
Themes were shared with participants through two feedback workshops (one in Malé and one outside of Malé).
Ethical considerations
Ethical approval was obtained from the London School of Hygiene & Tropical Medicine, the Maldives National Bureau of Statistics and the National Health Research Committee at the Maldives Ministry of Health.
Informed consent (written or recorded) was obtained from all participants before the start of data collection. Carers provided consent for children below the age of consent (18 years) and for people with impairments that severely limited their ability to communicate/understand with available supports (e.g. sign language interpretation, simplified interview schedules). In these instances, the child/person with a disability provided assent and their input was sought whenever possible and appropriate. Participants who reported that they had unmet health needs were referred to local services.
Findings
Coverage of the Disability Allowance
Overall, 103 people out of the 402 people identified as having a disability were receiving the Disability Allowance, giving an overall programme coverage of 25.6%. There was no evidence of inclusion errors, as all Disability Allowance recipients had a disability according to the study definition (n = 76, 73.9% by Washington Group criteria; n = 27, 26.2% by other eligible health conditions).
Coverage of the Disability Allowance differed among people disabilities (Table 1). Women were less likely to receive the Disability Allowance compared with men (18.7% vs 34.5%, aOR = 0.4, 95% CI: 0.2, 0.6). Coverage also varied by age, with coverage highest in children (34.4%) and younger adults (48.5%), and lowest for older adults (8.0%). By location, the capital Malé had lower coverage among people with disabilities compared with other areas (18.6% vs 30.6%, aOR = 2.1, 95% CI: 1.2, 3.7). By income level, coverage was highest for people in the two poorest quartiles both pre- and post-inclusion of the Disability Allowance allotment amount. Finally, coverage differed by impairment type, with coverage lowest for people with sensory impairments (14.9%) and highest for people with intellectual impairments (35.0%).
Coverage of the Disability Allowance, by participant characteristics (n = 402).
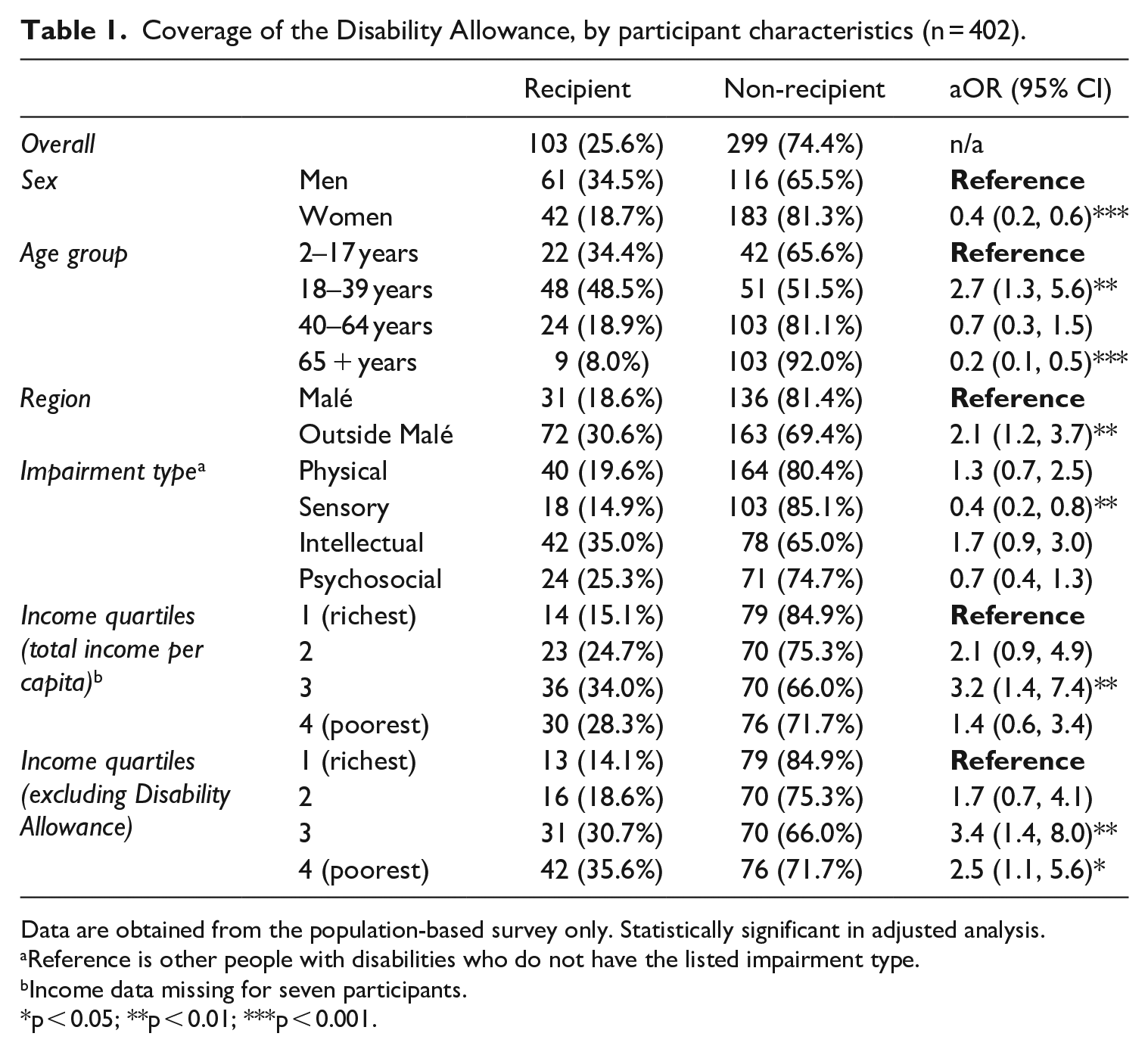
Data are obtained from the population-based survey only. Statistically significant in adjusted analysis.
Reference is other people with disabilities who do not have the listed impairment type.
Income data missing for seven participants.
p < 0.05; **p < 0.01; ***p < 0.001.
People with disabilities may also be eligible for other social protection programmes, which they can receive concurrently to the Disability Allowance. Notably, 97 people with disabilities received the Old Age Pension (coverage among people with disabilities over 65 years: 86.6%), which was similar to eligible adults without disabilities (84.1%, aOR = 1.6, 95% CI: 0.8, 3.3) (Table 2). Only 9.3% of older adults eligible for both the Disability Allowance and the Old Age Pension received both. Overall, 198 people with disabilities (49.4%) received at least one form of social assistance. Enrolment in social assistance was much higher compared with people without disabilities (4.1%), as people with disabilities were more likely to be eligible for the two largest programmes (Disability Allowance, Old Age Pension). Enrolment in other programmes (Single Parent and Foster Parent Allowances) was low for both groups.
Enrolment in other social assistance programmes, people with and without disabilities.
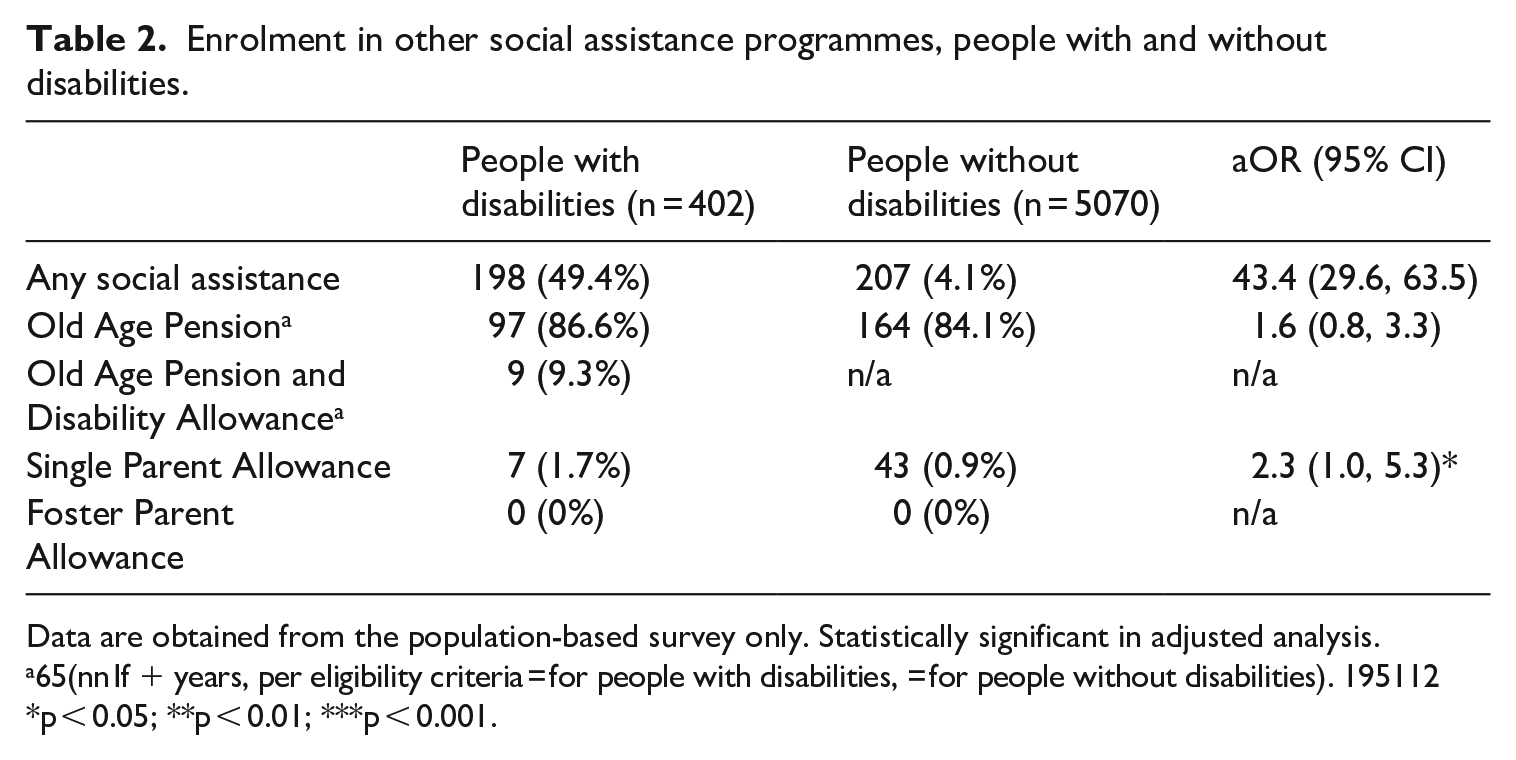
Data are obtained from the population-based survey only. Statistically significant in adjusted analysis.
65(nn If + years, per eligibility criteria = for people with disabilities, = for people without disabilities). 195112
p < 0.05; **p < 0.01; ***p < 0.001.
Factors influencing access to the Disability Allowance
The most common reasons for not receiving the Disability Allowance were lack of awareness (36.2%) and uncertainty over eligibility (46.6%) (Table 3). Other reasons for not applying were difficulties with the application process (9.7%) and feeling that the benefits were not helpful (1.1%). Others had applied for the Allowance but were either waiting for a decision or had been denied (4.7%).
Reasons for not being enrolled in the Disability Allowance (n = 279).
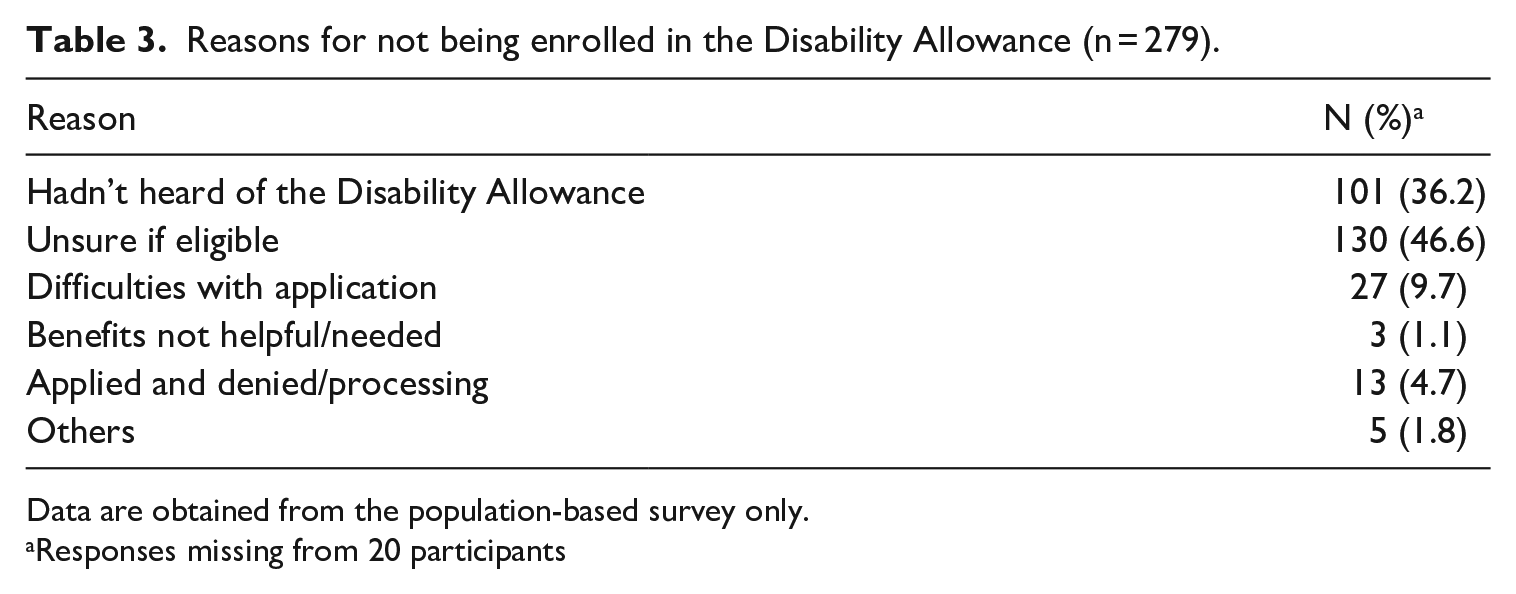
Data are obtained from the population-based survey only.
Responses missing from 20 participants
Furthermore, Disability Allowance recipients from the population-based survey and the survey of new Disability Allowance recipients were asked about their experience applying for the programme (Table 4). Most participants (80.7%) reported having undergone a medical assessment as part of their application. Recipients living in Malé mostly had their assessments in Malé, although 21.2% had travelled abroad. Almost all recipients living outside of Malé had to travel for their medical assessments, with only 18% having assessments on their home island and a further 13% having assessments in atoll/regional hospitals. More than half (59.6%) had to travel to Malé. Overall, two-thirds of Disability Allowance recipients travelled outside their home island for one component of the application. Out-of-pocket costs associated with applying varied widely, with a median of US$51.78 (IQR: US$366.00). Costs were much higher for participants living outside of Malé, who reported a median cost of US$87.38 (IQR: US$394.82), compared with participants living in Malé (median cost: US$15.28; IQR: US$166.34). Medical welfare was used to cover at least some of the costs for 8.4% of recipients.
Application experience of Disability Allowance recipients (n = 264).
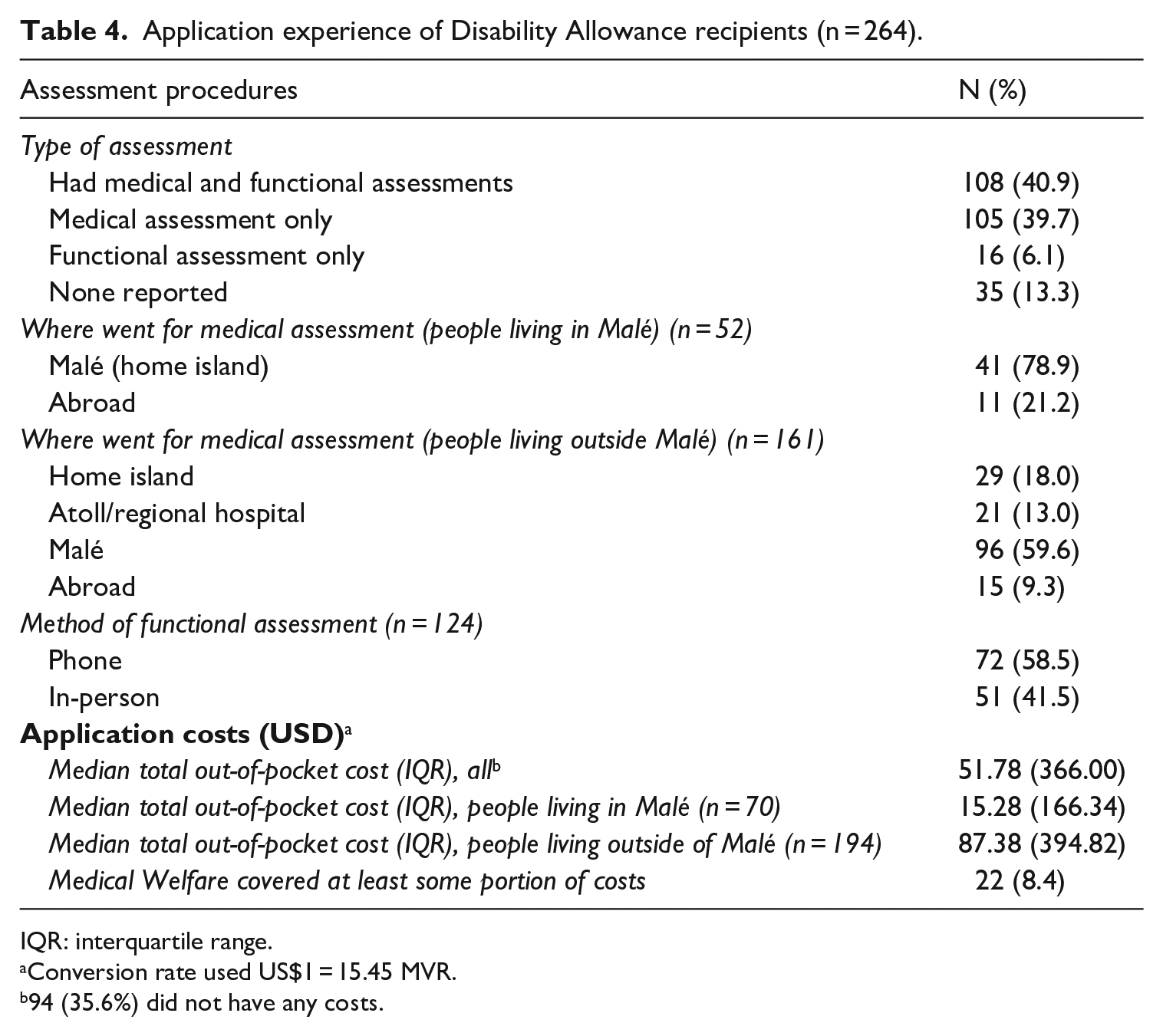
IQR: interquartile range.
Conversion rate used US$1 = 15.45 MVR.
94 (35.6%) did not have any costs.
The qualitative interviews provided more nuanced insight into factors affecting uptake, indicating several intersecting factors that shape people’s access to the Disability Allowance. Many respondents who expressed a desire to enrol in the programme faced informational, financial and/or geographical barriers in doing so. Others decided not to enrol due to stigma and perceived benefit weighed against the time and resources required for application.
Information and perceived eligibility
Similar to the survey responses (Table 3), many qualitative respondents lacked basic information about the programme, such as what it constituted (e.g. that it is a monthly transfer), how or where to apply. According to a linked process evaluation (Hameed et al., 2022), information about the programme and its application process is communicated mostly through registration drives, such as to commemorate notable days. This may partly explain the higher coverage in islands than in Malé (Table 1), where such events are common.
A key challenge was confusion over eligibility criteria, which had not been made publicly available by NSPA at the time of data collection. Nearly half the non-recipients from the survey reported being unsure if they were eligible (Table 2). This was echoed by some qualitative respondents who felt they would not be considered as having an eligible disability, and thus did not apply for the Disability Allowance. Most common perceptions were that an eligible disability would be something you were born with, and that limitations needed to be extreme, for example, being bedridden or nonverbal. Media attention around autism and some mental health conditions has raised awareness and acceptance that these are ‘valid’ disabilities. In contrast, some respondents felt that ‘invisible disabilities’ such as pain, would not be recognised by the programme staff, even though they restricted participation in everyday life.
Do you think you would be eligible?
I don’t think so. But if people who can’t walk can get it, then I will too. Do they give it if people can’t walk?
[. . .] So do you think what you have is a disability?
Hmm?
Do you think that?
Yes well, not being able to walk is a disability, isn’t that right?
(Male, over 65 years, physical impairment)
Furthermore, some participants did not perceive themselves as having a disability, even if they had pronounced functional limitations. In particular, older people with disabilities often identified themselves as ‘just being old, not disabled’, and opted to not apply for the Disability Allowance. Some had incorrectly assumed that they could not receive both the Disability Allowance and Old Age Pensions concurrently: they thus chose the Old Age Pension which was more straightforward to apply for and provides more than twice the amount given by Disability Allowance. These factors may explain why coverage among adults aged over 65 years is the lowest (8%) among all age groups (Table 1).
Father, well, he can do things like walking but ‘disabled’? THAT’s why we didn’t apply for him, to be honest [. . .] Father can [walk] slowly because [he is] ill, we do believe he is ill. But even if he is ill he is mobile. We didn’t apply because he is mobile. Well Father does get [Old Age Pension], because he is over 65 years, he gets 5000 Rufiyaa as benefit from the government.
(Caregiver of male, over 65, physical impairment)
In addition to disability eligibility, there were misconceptions that the Disability Allowance was tied to inability to work or poverty. For example, some participants, particularly men, who were receiving the Allowance tied their eligibility to their ability to work.
Geographical factors
The geographical dispersion of the Maldivian islands creates barriers to applying. In particular, many respondents reported needing to travel to obtain the necessary medical certification required for the application, as a result of scarcity of specialist services. Although there are six regional facilities offering various specialist services throughout the country, respondents noted difficulties finding specialists specific to their disability. This necessitates travel to Malé where the tertiary health facilities are located, bringing costs for travel and accommodations for both the applicant and anyone accompanying them, as well as for specialist services which are not always covered by Aasandha. Nearly 60% of survey participants based outside Malé reported travelling to Malé for the medical assessment (Table 4). The quote below is from an island-based caregiver who struggled to identify relevant specialists for her child’s impairment.
I was so relieved to finally show her [to a specialist]. They told us to come again. [. . .] They told us to come to Malé, I said I can only come during holidays, they said come to show her. But my financial situation . . . I couldn’t, but they said its VERY . . . they said even then, we can use their document to get that assistance . . .
(Caregiver of child, female, intellectual disability)
Furthermore, some participants reported travelling to Malé to submit their applications, although this can be done at the more local Island Council Offices.
Financial factors and perceived need
There is evidence that poverty can act as a barrier to entry, particularly for people requiring complex assessments. For example, the caregiver of a boy with intellectual and physical impairments explained that they have been unable to gather needed medical documents to support their application, as they must travel abroad for the specialists required for the medical assessment. Their application for the one-off Medical Welfare assistance (sometimes granted to cover application costs) was also rejected.
I have to ask my family for money and also work for over a year before I can take him abroad, every time. I’m not able to cover [the cost] by working one year. It takes me about two years to arrange one trip. But I do want to [take him], when we went to Bangalore for the first time, they told us to bring him after a year. But I know I can’t.
(Caregiver of a child, male, cognitive impairment and physical difficulties)
Data from the survey indicated that people in the 2nd poorest quartile were most likely to be enrolled in the Disability Allowance (Table 3), which matches data from the qualitative research. Living in poverty was a major driver of wanting to enrol in the Disability Allowance, but people with the lowest incomes often could not afford the upfront costs. Among wealthier participants, there was less of a desire to enrol in the programme. For example, some participants did not apply because they felt their financial situation was sufficient to meet their current costs, or that the additional income received through the Disability Allowance would not make much of a difference to their standard of living. The quote below is from an older man whose severe visual impairment required regular monthly trips to Malé, often staying there for two weeks.
[I haven’t applied] because of my [financial] situation today. If I get to a different situation, then my children will have to [apply]. Isn’t that what will happen?
Do you yourself think that ‘I am someone eligible to receive this assistance’?
There are people who are in worse [financial] situations than I am
I understand that, but when you think about yourself, do you think that you are someone who is eligible?
I don’t [think that] at all. That is because of my situation now.
(Male, over 65, severe visual impairment)
Mistrust
Some respondents mentioned the need for an influential ‘insider’ within the government would push for their application to be approved. Here, caregivers of a child talk about repeated attempts at applying but being unsuccessful with their applications. They also know someone else who has been successful, for whom they helped prepare the application documents.
He said, ‘I have a connection with someone there’, so that’s corruption right there, isn’t it?
Was [the allowance] settled for him?
It was settled for him. So, he went off then, he was very good at it
What sort of difficulty did he have?
He was close to some people, politically
No, I mean what kind of disability
His child?
The child had, how do I say, he has some issues like hyperactivity [. . .] and later I submitted the forms he said, like he said. It didn’t go anywhere
(Caregivers of a child, male, cognitive impairment, and physical difficulties)
This perception that having a disability alone does not qualify one for Disability Allowance, and that Disability Allowance recipients are not always people with disabilities, creates mistrust in the programme. This, in turn, contributes to self-exclusion among some eligible people, and reduces the access to the programme.
Stigma
Another factor that limits access to the programme is stigma. Respondents who want to apply for the Disability Allowance reported concerns about facing criticism from others in the community, particularly if others do not perceive them to have a disability. For example, people may not accept a worsening condition that prevents them from working when they had before, or they may be compared with another person in ‘worse’ situation. Concerns about such sentiments seem to be a powerful deterrent to respondents living in small island communities where most people know each other and their families. This is amplified in situations where applications for the programme sent through the Island Council Office are not kept confidential.
[Doctors] told me even then that I should apply and get this cash assistance. [. . .] People in this island criticise all the time ((Interviewer interjects: why?)). That is, people in this island always, even now, towards kids who are like that [disabled], kids who take [the cash allowance], always criticises them. [. . .] On the island we have the Council Office, right. We apply and things at the office. Then people there tell others about it, tell many different people [. . .] and we hear a lot of their stories all the time, that’s why my husband does not agree [to apply], to not listen to things like that [. . .] ‘that is what you people are doing just to eat up the money, you shouldn’t use that up’ we hear words like that [from others in the community]. That’s why my husband doesn’t want it. He said we will do what we can, and I said doing THAT doesn’t get her the therapy she needs, in reality . . . I don’t want her to not know anything.
(Caregiver of child, female, intellectual impairment)
Discussion
Overall, this research found that one in four (25.6%) people with disabilities in the Maldives are receiving the Disability Allowance. Coverage was lowest for women, older adults, people living in Malé, wealthier households and people with sensory impairments. All recipients met the study definition of disability, and thus there were no inclusion errors. Qualitative data identified barriers to enrolling in the Disability Allowance, which included information, financial and geographical challenges. Moreover, stigma and lack of clarity in eligibility criteria often led people to self-exclude from the Disability Allowance programme.
Few other studies have directly measured national coverage of disability-targeted schemes using direct survey methods. Access to disability-targeted cash transfers among working-age adults (18–59 years) was found to be 36% in South Africa and 11% in India, although these schemes include other eligibility criteria (e.g. capacity to work, poverty) (Kidd et al., 2018; Wapling et al., 2021). In South Africa, the Disability Grant was found to have high inclusion and exclusion errors (34% and 42%, respectively), although exclusion errors were more serious as eligible people with disabilities not receiving the Disability Grant were more likely to be living in poverty and facing food insecurity (Mitra, 2010). All age coverage in universal disability-targeted grants similar to the Maldives was 13.4% in Tanahun, Nepal, and 36.8% in Cam Le, Vietnam, although these are regional rather than national estimates (Banks et al., 2019a, 2019b). Enrolment in mainstream social protection programmes such as health insurance and non-disability targeted cash transfers, and generally have found similar levels of enrolment between people with and without disabilities, even though people with disabilities tend to have a higher need for programmes (e.g. poorer heath, higher levels of poverty) (Banks et al., 2016; Bernabe-Ortiz et al., 2016; Kidd et al., 2019; Kuper et al., 2016).
Lower coverage of the Disability Allowance among older adults in the Maldives matches trends found in other studies (Banks et al., 2019a, 2019b). Part of this trend may reflect preferences for Old Age Pensions, which are easier to apply for as they only require a certification of age, rather than the often costly, time-consuming and unclear assessment of disability (Kelly, 2016; Kidd, 2017). Furthermore, applying for an Old Age Pension may be less stigmatising than for a Disability Allowance, as it is less subjective to identify an older adult compared with a person with a disability. The qualitative research highlighted in this and other studies (Loeb et al., 2008; Mont, 2007) indicates that many older adults may not consider themselves as having a disability. Consequently, older adults with disabilities may choose an Old Age Pension instead of a Disability Allowance, in settings where they can only choose one. In the Maldives, where concurrent enrolment is allowed, only 9% of eligible older adults were enrolled in both programmes. These findings have important learning for contexts beyond the Maldives on the complex decision-making processes around application decisions, that include reflecting on stigma linked to receiving certain benefits, and on identifying as a person with a disability.
Coverage of the Disability Allowance was lowest in Malé, even though many barriers to access are reduced (e.g. travel to application points and health services for the medical assessment, stigma in small communities) and costs associated with the application were much lower (median of US$15 compared with US$87 for people living outside Malé). Although this issue requires further study, this finding most likely reflects the low value of the cash transfer in comparison to the cost of living in Malé, as the average monthly household income in Malé is MVR 37,035 (US$2400) compared with MVR 18,358 (US$1200) for other regions (National Bureau of Statistics, 2016). The Disability Allowance therefore is a less meaningful contribution to household resources in Malé, representing just 5.4% of average household income compared with 10.9% in the atolls. Similarly, people with disabilities living in poorer households were more likely to apply for the Disability Allowance. Even though the addition of the Disability Allowance was insufficient to push most households out of poverty – which mirrors other research from South Africa (Hanass-Hancock and McKenzie, 2017) – it is still an important source of income for people living in poverty. This finding reinforces the importance of benefit relevancy (Devandas Aguilar, 2017), which has implications not only for impact of the benefit, but also for decisions regarding enrolment.
Some of the barriers to applying for the Disability Allowance have been identified in other studies. In particular, the medical certification of disability is a major barrier due to both the centralisation of services required for assessments and subjective or inconsistently applied eligibility criteria (Devandas Aguilar, 2017; Gooding and Marriot, 2009; Kidd, 2017). Undergoing medical assessments also brings high direct costs and opportunity costs particularly if applicants must travel far distances as found in the Maldives where travel costs were often higher than the cost of the services. Other studies have found using community-based registration drives or having assessments conducted at more decentralised administrative offices could lead to improved enrolment (Banks et al., 2018, 2019a), which could be used as a policy tool in the Maldives and other settings to improve coverage.
Informational barriers, such as lack of clarity in eligibility and application processes contributed to low coverage of the programme, as in other settings (Devandas Aguilar, 2017; Graham et al., 2013; Kelly, 2016; Kidd et al., 2019; Macgregor, 2006). In the case of Maldives, the eligibility criteria used by implementers had not been made publicly available. As a result, self-exclusion is common among eligible people with disabilities, sometimes due to fears that their disability will not be recognised, or misconception that eligibility is linked to unemployment or poverty. Misconceptions about capacity to work may explain the relatively higher proportions of men among beneficiaries, as the loss of income or non-participation in income-generating work may be more significant to men than women. It is also important to note, that participants with disabilities in this study who were not enrolled in the Disability Allowance were provided with information about the programme, including how to apply. However, on a follow-up study 18 months later (Hameed et al., 2022), only 10 individuals (2.6%) had enrolled, underscoring the importance of the qualitative research in highlighting more nuanced and multifaceted barriers to enrolment.
Misconceptions about eligibility and social attitudes about who ‘deserves’ a cash transfer can be what Devereux et al (2017) consider social and psychological costs of applying for and receiving social assistance. In this study, these costs were particularly high for people with disabilities living in small island communities or whose circumstances did not align with social norms on who should receive of a cash transfer (e.g. were not poor or could work, had ‘hidden’ or non-socially recognised forms disabilities). Consequently, people in this study did not want to apply either because they did not want to self-identify as having a disability or face the psychological and social costs of applying. Factors not captured in this qualitative component include those stemming from the perspective of implementers, as this study only sampled people with disabilities. However, the process evaluation linked to this study did highlight how difficulties with the disability assessment contribute to uptake of the Disability Allowance programme.
Still, this research has highlighted strengths of the Maldives’ Disability Allowance. At 25.6% coverage is much higher than the 9.4% estimate for Asia and the Pacific (International Labour Organization, 2017). Furthermore, the ability to enrol concurrently in other schemes such as the Old Age Pension takes into account intersecting vulnerabilities (e.g. loss of income due to ageing, need to cover additional costs of having a disability) (Drucza, 2016; World Health Organization and World Bank, 2011). The grant is also universal to all citizens with disabilities and does not include other criteria linked to poverty or capacity to work – which have been found to exclude people with disabilities who require cash transfers to meet both basic needs and disability-related costs (Banks et al., 2016; Mont and Cote, 2020) – although increased awareness-raising is needed to improve understanding of the eligibility criteria for both potential applicants and community members.
There are several limitations that should be considered when interpreting the results of this study. Our sample was restricted to people ages 2 + as the Washington Group questions were the primary tool used for measuring disability and so this study is unable to comment on access to the Disability Allowance among children under 2 years. In addition, the Washington Group questions do not capture all forms of disability. We added additional questions to include impairments that would meet programme eligibility criteria (e.g. autism, psychosocial impairments); however, these additional questions have not been validated and rely on self-report of conditions, and therefore, may not capture all eligible individuals. Furthermore, although the definition of disability used in this study closely matches the eligibility criteria of the Disability Allowance, the latter is determined through clinical assessment rather than self-reported functioning, and so there may be some discrepancies in determinations of who would have an eligible disability per the Allowance guidelines.
Key strengths of this study included the use of mixed methods, which allows for a more comprehensive exploration of access to the Disability Allowance and the triangulation of findings. In addition, this study uses a large-scale, nationally representative, population-based data and so findings can be generalisable to the situation across the Maldives, which is important for national planning and policies.
Overall, this research carries several implications for improving the delivery of social protection within the Maldives. Furthermore, although the Maldives is a small and upper-middle income country, and offers a relatively high value allowance compared with other LMICs, several findings from this research may be applicable to other countries as they design or adapt their social protection systems. Importantly, this research found that many people with disabilities had not enrolled in the Disability Allowance, even though it is a universal scheme and can be received concurrently with other cash transfers. This is in contrast to other universal schemes such as Old Age Pensions, in both the Maldives and in other settings (Banks et al., 2019b) which have significantly higher coverage compared with Disability Allowances. Mixed-methods research revealed several complex challenges that may affect coverage for the Disability Allowance in the Maldives, some of which have been found in other settings. For example, raising awareness about the existence of social protection schemes and how to apply is important, but it may be insufficient to improve coverage without efforts to widen knowledge of eligibility criteria and address stigma of receiving such benefits. Furthermore, high monetary and opportunity costs linked to the medical assessment may be key barriers to entry to the programme, while social and psychological costs (e.g. stigma and tension in the community) can also contribute through self-exclusion. Finally, benefits may not be perceived as sufficiently valuable to offset costs of applying and the stigma encountered, particularly in urban areas where cost of living is high.
These findings provide key insights that could contribute towards strategies used by governments and non-state actors (e.g. Organisations of Persons with Disabilities [OPDs], international NGOs [iNGOs] such as the International Labour Organization, World Bank and UN agencies) for improving uptake of social protection among people with disabilities in the Maldives and other settings. For example, OPDs and iNGOs could work with governments to standardise eligibility criteria and assessments to align better with the UNCRPD, and consult on the combination of cash and in-kind benefits that would be most useful to meet the needs of people with disabilities. Similarly, complementary programmes to reduce stigma of disability and offset costs of applying could improve access.
Further research is needed to explore access of people with disabilities to different types of social protection programmes in different settings. In addition, research is needed to assess the impact of social assistance and other forms of social protection, both in the Maldives and globally. The evidence also suggests that consultations are needed with people with disabilities and their representative groups to develop strategies to address these barriers and further improve access to Disability Allowance among people with disabilities in the Maldives.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from 3ie (the International Initiative for Impact Evaluation), grant number PW3.11.MDV.IE.