
Abstract
Summary
Deinstitutionalization a globally recognized child protection reform, seeks to transition children from residential institutions to family and community-based care models that align with the UN Convention on the Rights of the Child. Despite its noble intent, implementing deinstitutionalization in Zimbabwe remains in its formative stages, with significant gaps in policy and practice. Guided by the 7Cs Protocol Framework, this study explores the challenges and ambiguities hindering the process.
Findings
Semi-structured interviews were conducted with 13 practitioners, including social workers and evaluators from the Department of Social Development and private voluntary organizations. Data were analyzed using MAXQDA and 7Cs framework, revealing five significant themes: unstructured and inconsistent transition processes, skill deficiencies among Child Protection Officers, resistance from institutional staff, reluctance to explore alternative care strategies, and insufficient prereintegration preparation and support. The findings indicate that a lack of standardized reintegration guidelines, limited training, and systemic resistance undermines the effectiveness of deinstitutionalization efforts. Institutional caregivers often resist reforms due to fears of job loss and funding reductions, while social workers hesitate to explore alternative care strategies due to high workloads and resource constraints. Prereintegration preparation remains inadequate, leaving children and families vulnerable during transitions.
Application
Recommendations bar for a strengthening-gatekeeping mechanisms, aligning resource allocation with caseload demands, implementing awareness campaigns to shift societal attitudes, fostering partnerships for family support, and developing child-centered care plans. These measures, supported by interdisciplinary collaboration, are critical for refining Zimbabwe's deinstitutionalization efforts and ensuring sustainable reform.
Keywords
Introduction
Globally, an estimated 5‒6 million children reside in residential care institutions (Neville et al., 2024), a reality that contrasts sharply with the United Nations Convention on the Rights of the Child (UNCRC), which upholds every child's right to grow up in a family environment. In response, the UN General Assembly has repeatedly called for the progressive replacement of institutional care with high-quality alternatives, including family reunification, kinship care, foster care, and adoption. This shift is underpinned by extensive evidence showing the harmful impacts of institutionalization. Despite Henderson’s (2023) call for new reflection on the real impact of deinstitutionalization, some studies (e.g., Bos et al., 2011; Gozho et al., 2024a; Neville et al., 2024) consistently demonstrate that children in institutions experience developmental delays across mental-cognitive, physical, social, and socio-emotional domains. Institutions often lack the capacity to provide personalized, nurturing care, leading to poor outcomes, particularly after children exit care. However, emerging scholarship cautions against treating institutional care as uniformly detrimental, noting that outcomes vary significantly across contexts and that well-regulated residential settings can, in some cases, offer stability that poorly supported family-based placements cannot.
Deinstitutionalization has thus emerged as a transformative child protection reform, aiming to transition children from institutional settings to family-based care. Deinstitutionalization refers to the deliberate, systemic replacement of institutional care with permanent family- or community-based alternatives, distinct from routine reunification, which seeks to eliminate reliance on institutions altogether rather than using them as temporary placements (Harlow, 2022; Murthi & Jayasooriya, 2020). This approach promotes holistic well-being by prioritizing stable relationships, emotional security, and community integration (Murthi & Jayasooriya, 2020). While institutional care may be necessary as a last resort, it often fails to meet children's psychological and emotional needs. Many countries have embraced this reform as a benevolent yet challenging shift toward family-based alternatives. Although Zimbabwe-specific studies remain limited, global research (Chege & Ucembe, 2020; Harlow, 2022; Murthi & Jayasooriya, 2020) reveals significant implementation gaps, including unsafe placements, inadequate caregiver preparation, and weak follow-up support (Milligan, 2016; Murthi & Jayasooriya, 2020), highlighting the need for more strategic efforts. Therefore, while the vision of deinstitutionalization is noble, its execution demands comprehensive studies to assess programmatic readiness, often in countries at the formative stage, with the process guiding implementation that can exacerbate child protection risks. This study adopts the position that the debate is not about choosing between ‘good’ family-based care and “bad” institutional care, but about understanding the practical, contextual, and systemic conditions under which each care option succeeds or fails. With Zimbabwe at the formative stage of deinstitutionalization, this study critically examines the gaps in the status of the strategy, focusing on the perspectives of child protection practitioners. Identifying gaps in policy and practice seeks to improve Zimbabwe's readiness for reform and contribute valuable lessons for global societies navigating similar transitions.
Common Barriers to Deinstitutionalization
Despite widespread policy endorsement, deinstitutionalization efforts across diverse contexts continue to be undermined by structural and cultural barriers. In Romania, reforms initiated in the 1990s, driven by international pressure and EU support, led to reductions in institutionalized children through foster care and reunification. Yet, inconsistent training of foster carers and inadequate monitoring mechanisms left reintegrated children vulnerable to neglect, while overburdened social workers struggled to provide meaningful support (Dragu, 2019). A similar pattern is evident in Bulgaria, where over half the institutions were closed between 2010 and 2020, but the shift to family-based care stalled due to cultural resistance to nonkin caregiving, fragmented services, and insufficient social work capacity (Bilson & Larkins, 2013; Hadjiev, 2018). Comparable constraints are found in India, where the Integrated Child Protection Scheme (ICPS) promotes family-based alternatives, yet deep-rooted stigma around nonbiological caregiving and under-resourced child protection systems continue to limit effectiveness. Social workers lack the tools and supervision to monitor reintegration outcomes, leading to protection gaps (Ramaswamy & Seshadri, 2020). In Brazil, despite the progressive Statute of the Child and Adolescent (ECA), regional inequities in funding and professional capacity result in uneven implementation. Poor follow-up systems expose children to neglect and increase the risk of re-abandonment (de Almeida McCann, 2016). In Nepal, efforts to promote family reintegration are similarly constrained by poverty, political instability, and public attitudes that continue to favor institutional care (Dahal et al., 2024; Forber-Pratt et al., 2020).
In Zimbabwe, policy frameworks such as the National Orphan Care Policy have long emphasized family- and community-based care, reflecting traditional values and statutory commitments. However, economic decline, HIV/AIDS, and the breakdown of extended family systems have eroded the viability of kinship care. The increase in institutional placements over the past decade underscores a growing reliance on institutional care as a default rather than as a last resort (Gozho et al., 2024b; Muzingili & Gunha, 2017). Limited investment in foster care, weak reintegration programs, and fragmented service delivery further compound the problem. These trends echo barriers seen in other low-resource settings and raise critical questions about the feasibility of deinstitutionalization when foundational systems remain fragile.
Importantly, the assumption that institutional care is inherently harmful has been increasingly challenged, with several scholars arguing that the global deinstitutionalization agenda sometimes oversimplifies the complex realities of care (Ainsworth & Huefner, 2025). Evidence from Latvia shows that some children prefer residential settings over unstable family placements, citing predictability and relational continuity (Kessler et al., 2025). Likewise, in Germany and Denmark, where over 30% of children in care remain in residential settings, positive outcomes are associated with professionalized services and robust regulation. These findings, also evident in Sweden, where residential care continues to serve 22% of children, challenge the binary framing of institutional versus family-based care and suggest a need for contextual assessment rather than ideological commitment (Tøssebro, 2016; Ulybina, 2024). Taken together, these perspectives do not negate the value of deinstitutionalization but highlight that its success depends less on the placement type and more on the quality, stability, and cultural fit of the care environment.
A major fault line in the position of NGOs is the assumption that residential and foster care are mutually exclusive; in practice, many children enter residential care after disrupted foster placements, especially in the Global North. Foster care does not always provide the stability it is imagined to offer. Critics of deinstitutionalization, such as Ainsworth and Huefner (2025), argue that global advocacy has often turned deinstitutionalization into a prescriptive model, applied indiscriminately without regard for local realities. Their critique goes further, describing deinstitutionalization as a “fraudulent concept” that may cause harm when applied without careful adaptation to context. This critique is particularly salient in Zimbabwe, where donor-driven agendas have sometimes taken precedence over investment in sustainable, culturally embedded alternatives. The emphasis must shift from care type to care quality, with careful evaluation of what works in specific contexts. Islam and Fulcher (2022) and Nadesan (2021) similarly argue that deinstitutionalization is often culturally inappropriate and practically unfeasible across much of the Global South. Thus, the framing of deinstitutionalization must move beyond ideological binaries and engage with the lived realities of children, especially those with complex needs or older age, for whom family-based options may not always be viable. The recent work of Sen (2022) and Henderson (2023) also calls for more critical reflection on whether deinstitutionalization is achievable or desirable in contexts where foundational systems are weak.
Enabling Conditions for Deinstitutionalization
Where deinstitutionalization has progressed more successfully, it has done so not through ideological adherence but through strategic alignment of policy, resources, and professional capacity. In Norway, Sweden, and Denmark, deinstitutionalization has been buttressed by long-standing welfare systems, strong political commitment, and substantial public investment. In these contexts, institutional care is used sparingly and strategically, while family- and community-based alternatives are supported by well-trained social workers and integrated service delivery systems (Tøssebro, 2016; Ulybina, 2024). Residential care, where it exists, is well-regulated and staffed by professionals, contributing to positive outcomes and demonstrating that institutional settings, when properly resourced, can remain a legitimate part of the care mix. It is important to note, however, that Norway is an outlier even within Europe, due to its oil wealth and unusually high public investment capacity. In Germany and the UK, similar patterns emerge. The UK's Children Act (1989) prioritizes family-based care through adoption and foster care, with institutional care as a last resort. However, challenges persist in serving older children and those with complex needs, often due to insufficient foster parent training and weak postplacement support (Khetawat, 2020). Germany, while maintaining a significant proportion of children in residential settings, invests heavily in professionalization and oversight to ensure quality standards are upheld.
Australia's National Framework for Protecting Australia's Children (2009–2020) demonstrates another model of coordinated reform, replacing large-scale institutions with foster care and small group homes while focusing on early intervention and family reunification. Nevertheless, the overrepresentation of Indigenous children in care highlights the systemic inequities that deinstitutionalization must address through culturally responsive policies (Golding et al., 2021; Musgrove, 2023). However, in the Asia-Pacific, progress has been more uneven. Cambodia's “Family Care First” initiative, led by UNICEF, has promoted family reintegration and community-based care. Yet weak regulatory oversight and unregistered orphanages continue to undermine reforms (Nhep, 2024). The Cambodian experience underscores the need for robust governance and enforcement mechanisms—elements that are also underdeveloped in Zimbabwe. From the African context, Rwanda offers a more regionally relevant example. Its “Tubarerere Mu Muryango” program has been praised for closing most orphanages and reintegrating children into family and community settings. The program's success rests on a combination of government leadership, donor support, and community mobilization (Murthi & Jayasooriya, 2020). However, capacity gaps and cultural discomfort with nonkin care remain, revealing the complexity of sustaining such reform.
In Zimbabwe, enabling conditions for deinstitutionalization must similarly extend beyond policy declarations. Recognizing the contested nature of deinstitutionalization allows Zimbabwe to avoid uncritically adopting global models and instead to focus on the structural and cultural foundations that determine whether deinstitutionalization can be implemented safely and sustainably. Investment in a professionalized social service workforce, the development of culturally aligned kinship and foster care systems, and sustained public engagement are essential. Without addressing these structural foundations, deinstitutionalization efforts risk becoming symbolic rather than substantive. This highlights that successful deinstitutionalization models tend to embed child protection reforms within broader social protection strategies that address poverty, education, and health—areas that require greater integration in Zimbabwe's context. van IJzendoorn et al. (2020) and Goldman et al. (2020) provide vital frameworks for aligning policy and practice with child development outcomes in these contexts.
Lessons from Countries at Formative Stages
Countries at early or transitional stages of deinstitutionalization reform provide instructive lessons for Zimbabwe, revealing both the potential and the pitfalls of system transformation. In Kenya, government efforts to expand kinship and foster care through partnerships with NGOs have been hampered by weak regulatory frameworks, insufficient social worker training, and poor inter-agency coordination. As a result, many children remain in unregulated institutions despite policy shifts (Chege & Ucembe, 2020). Similarly, in Uganda, fragmented service delivery, limited funding, and public preference for institutional care have undermined reform efforts, even as deinstitutionalization gains rhetorical traction (Milligan, 2016). India's experience with the ICPS further reveals the importance of addressing cultural norms and practitioner capacity. While legal frameworks encourage family-based care, societal discomfort with fostering and resource limitations continue to drive institutional placements. As in Zimbabwe, public education, community dialogue, and targeted investment in social work are critical to shifting perceptions and establishing viable alternatives (Ramaswamy & Seshadri, 2020).
In Brazil, the emphasis on reunification without adequate postplacement support has led to high rates of re-entry into care. Regional disparities in service provision and poor monitoring systems have left reintegrated children vulnerable, especially in under-resourced areas (de Almeida McCann, 2016). These outcomes highlight the importance of aftercare services and sustained case management—elements that are not yet fully institutionalized in Zimbabwe's care system. Cambodia, despite its progressive deinstitutionalization agenda, also illustrates the limits of reform when enforcement mechanisms are weak. Poorly regulated orphanages and limited state capacity undermine reintegration efforts, exposing children to secondary harm (Nhep, 2024). Nepal, too, has faced difficulties maintaining placements due to poverty and instability, with public preference for institutional care further complicating the challenge (Dahal et al., 2024; Forber-Pratt et al., 2020). For Zimbabwe, rather than viewing deinstitutionalization as an unavoidable or universally better reform, this study highlights the practical obstacles to its viability in low-resource settings. It involves navigating complex cultural, social, and economic realities. Institutional closure without the parallel development of robust alternative systems—professionalized foster and kinship care, aftercare support, and culturally responsive practices—will not lead to sustainable outcomes. The literature indicates that such a strategy must be iterative and learning-focused—adaptable to community feedback and responsive to the evolving needs of children, rather than rigidly aligned with international templates (Harlow, 2022; Sen, 2022; Tøssebro, 2016).
Theoretical Framework
This study uses the 7Cs Protocol Framework to examine Zimbabwe's efforts to deinstitutionalize child protection. The framework assesses essential aspects—content, context, commitment, capacity, clients and coalitions, communication, and coordination—that influence whether policy implementation succeeds or fails. This framework also enables the study to move beyond normative debates about whether deinstitutionalization is “good” or “bad” and instead interrogate the operational realities that determine its success.
Content pertains to the substance of policies and programs, including their goals, strategies, and operational procedures (Molobela, 2019). Zimbabwe's National Orphan Care Policy introduces a six-level system that emphasizes family-based care, with institutional care as a last option. Although this framework provides a good foundation, operational ambiguities limit its effectiveness. For example, the absence of detailed guidelines for monitoring reintegrated children increases the risk of neglect or re-abandonment. In contrast, Romania's deinstitutionalization reforms show how gaps in foster care regulations and a lack of foster parent training can leave children vulnerable (Tøssebro, 2016). Fixing these ambiguities in Zimbabwe's child protection efforts requires clearer implementation plans, caregiver training modules, and robust monitoring systems to track children's well-being after reintegration (Muzingili et al., 2025; Muchinako et al., 2018). The content should also reflect the second C, context, encompassing the social, cultural, economic, and political environments in which deinstitutionalization policies are enacted (Molobela, 2019). Zimbabwe's historical reliance on extended family systems for child protection has been undermined by socioeconomic challenges, poverty, and the HIV/AIDS epidemic, leaving many children without traditional safety nets (Muchinako et al., 2018; Muzingili & Ghuna, 2017). As a result, there is increased reliance on institutional care, despite professional views that still regard orphanages as “safe” options. Similarly, in India and Cambodia, cultural resistance to nonbiological caregiving has slowed the development of foster and kinship care systems (Nhep, 2024). In Zimbabwe, overcoming these contextual barriers will require targeted public awareness campaigns, like Rwanda's “Tubarerere Mu Muryango” initiative, to promote family-based care and foster trust in alternatives to institutions.
Following the appreciation of context, capacity plays a crucial role in policy implementation. Capacity refers to the resources, infrastructure, and human capital available to carry out deinstitutionalization programs (Colborne, 2021). Zimbabwe faces significant capacity constraints, particularly in its social work sector. Social workers are overwhelmed with high caseloads, insufficient training, and resource shortages, which hinder their ability to support reintegration effectively (Mavuka et al., 2024; Muzingili & Tembo, 2025). This situation is similar to challenges in Romania, India, and Kenya, where underfunded social workers struggle to monitor placements and deliver personalized care. Improving capacity in Zimbabwe involves investing in professional development, recruiting more social workers, and providing adequate tools and resources to ensure effective service delivery. Achieving sustainable capacity can be supported by the fourth C: commitment. Commitment reflects political will and stakeholder dedication to implementing deinstitutionalization policies (Colborne, 2021). Zimbabwe has shown commitment through its legal frameworks, such as the Children's Act and the National Orphan Care Policy (Muchacha et al., 2016). However, inconsistent funding and competing priorities hinder sustained progress (Gozho et al., 2024b). For instance, although deinstitutionalization is cost-effective compared to institutional care, limited budgets slow down its implementation. Countries such as Sweden and Norway demonstrate how sustained political support and financial investment can lead to long-term success (Tøssebro, 2016). In Zimbabwe, increasing commitment requires stronger advocacy efforts to secure dedicated funding for deinstitutionalization and to align stakeholders’ priorities with child welfare goals.
As indicated in the literature, the success of deinstitutionalization depends on strong stakeholder and partnership involvement, reflecting the 5th C of Clients and Coalitions. This aspect emphasizes the participation of key stakeholders (Molobela, 2019); in the case of deinstitutionalization, this includes children, families, communities, and coalitions of organizations (Bilson & Larkins, 2013; Dragu, 2019; Hadjiev, 2018). In Zimbabwe, NGOs and international organizations play a vital role in supporting deinstitutionalization, but weak collaboration with government agencies often leads to fragmented efforts. Likewise, poor coordination among stakeholders has slowed progress in Kenya (Chege & Ucembe, 2020) and Uganda (Milligan, 2016). Engaging clients, children, and families is equally important to ensure interventions respond effectively to their needs and realities. For example, Rwanda's success in deinstitutionalization has been credited to strong coalitions between the government, UNICEF, and communities, combined with participatory approaches (Murthi & Jayasooriya, 2020). Zimbabwe needs to strengthen coalitions and improve community engagement to successfully implement family-based care systems. Sustainable stakeholder success in policy implementation requires the 6th C, communication. Communication involves sharing information with stakeholders and the public to raise awareness and foster alignment. The limited public understanding of family-based care sustains cultural resistance to alternatives like foster care, kinship care, and adoption. Examples from around the world, such as Rwanda's public awareness campaigns, show how targeted communication can change societal perceptions and support acceptance of noninstitutional care (Murthi & Jayasooriya, 2020). Zimbabwe should prioritize communication strategies that highlight the developmental and emotional benefits of family-based care, utilizing media and grassroots outreach to dispel misconceptions about institutional care.
Finally, effective policy implementation depends on strong coordination. Coordination involves aligning stakeholders’ efforts to ensure efficient and effective execution (Molobela, 2019). In Zimbabwe, fragmented coordination among government agencies, NGOs, and international partners leads to inefficiencies and overlaps. Similar issues in Kenya (Chege & Ucembe, 2020) and Uganda (Milligan, 2016) emphasize the need for unified approaches to reintegration, monitoring, and support systems. Improving coordination requires defining clear roles and responsibilities for stakeholders, supported by accountability mechanisms and regular collaboration. Creating a centralized database to track reintegration outcomes and interventions could further improve coordination and close service gaps (Colborne, 2021).
Materials and Methods
Participants
The study's participants were carefully selected to ensure a comprehensive understanding of Zimbabwe's deinstitutionalization landscape. Thirteen individuals were included, representing varied professional backgrounds and organizations directly involved in the deinstitutionalization program in Mashonaland Central. Criterion-based purposive sampling was employed to ensure that participants met specific inclusion criteria, including direct involvement in the deinstitutionalization process, knowledge of policy implementation, and experience with child welfare programs. These participants were drawn from the Department of Social Development, Zimbabwe's primary custodian of child protection, and two Private Voluntary Organisations (PVOs). One PVO was actively implementing the deinstitutionalization program, while the other had conducted a preliminary evaluation of the program's outcomes. This sample was purposively selected to capture insights from government social workers, program evaluators, and other practitioners with direct experience in child protection activities. The final sample size was based on the availability of eligible participants during the data collection period. Previous qualitative studies on child welfare reforms have similarly employed small samples, highlighting the value of in-depth engagement with key stakeholders (Bilson & Larkins, 2013; Dragu, 2019). This approach was considered appropriate for the study context, where access to practitioners with direct, hands-on experience was both purposeful and time-bound.
Research Instrument
The study utilized a semi-structured interview guide as the primary data collection instrument. Semi-structured interviews were chosen for their flexibility, allowing the researcher to explore predefined themes while accommodating emerging insights from participants. The guide was developed with input from two child protection experts to ensure its relevance to deinstitutionalization policies and practices. It included seven major questions rooted in the 7Cs Protocol Framework, each addressing specific gaps identified in the literature. Open-ended sub-questions were incorporated to probe deeper into participants’ experiences and perspectives. The seven significant questions were designed to align with the dimensions of the 7Cs framework—content, context, capacity, commitment, clients and coalitions, communication, and coordination—while being contextualized to the deinstitutionalization process in Zimbabwe. Each question was informed by gaps and deficiencies highlighted in the literature, ensuring that the research addressed critical areas in policy and practice. The seven significant questions in the semi-structured interview guide are indicated in Table 1.
Research Questions.
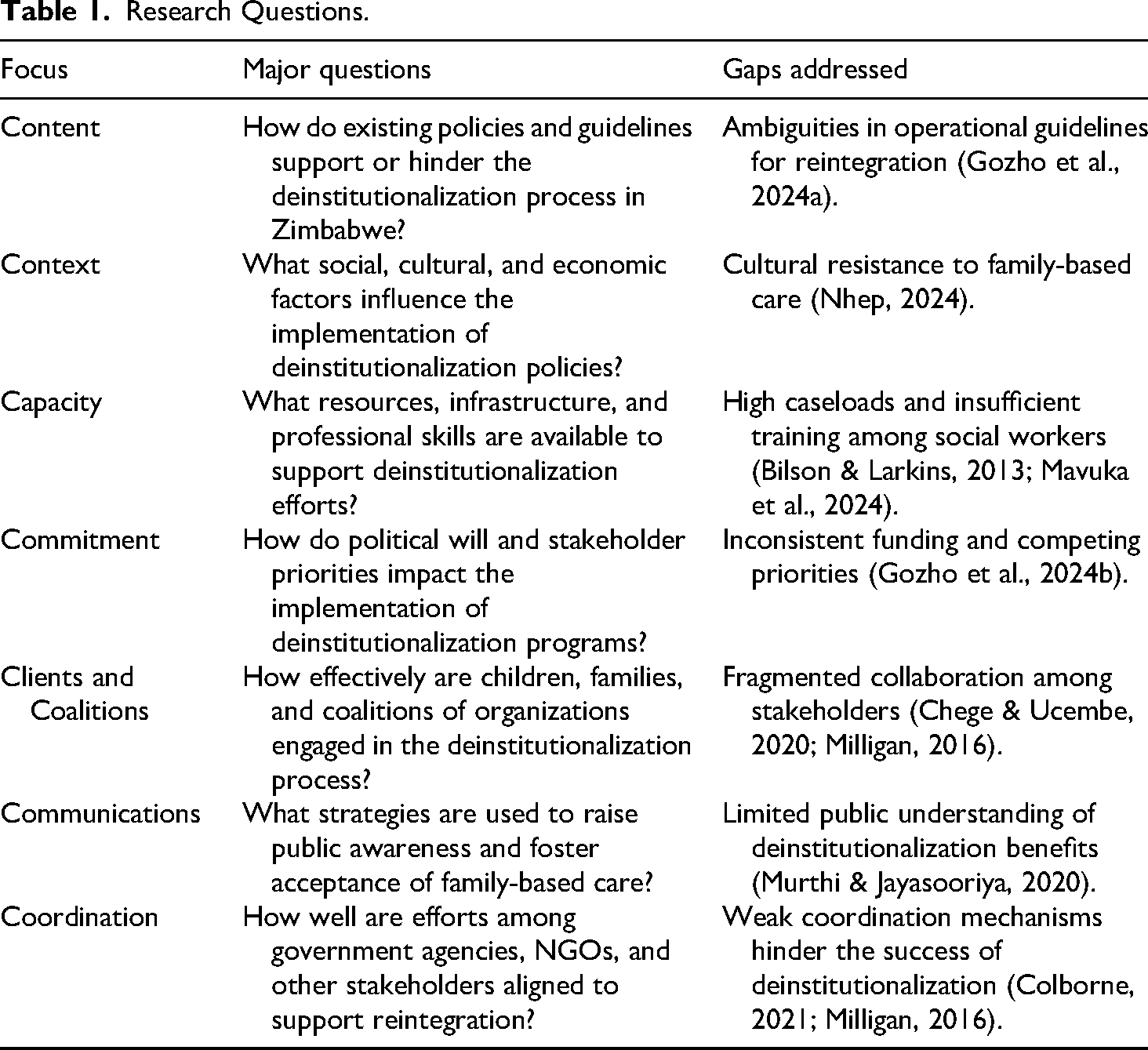
Each question was designed to elicit detailed responses that addressed the identified gaps while capturing participants’ lived experiences. The semi-structured interview guide was pretested between 3 and 7 October 2024 with a small group of five practitioners to refine its clarity and relevance. Adjustments were made based on their feedback to ensure the questions were accessible and elicited meaningful insights. The guide also included prompts and follow-up questions to explore participants’ responses in greater depth, thereby maximizing the richness of the collected data. By grounding the research instrument in theoretical frameworks and empirical evidence, the study ensured its findings would be robust and actionable.
Data collection Procedure
Data collection for this qualitative study was conducted from 23 October to 7 November 2024, using semi-structured interviews as the primary method. The interviews were conducted in participants’ workplaces, with scheduling based on availability and flexibility. This approach ensured minimal disruption to participants’ day-to-day responsibilities while fostering a comfortable environment for open and candid discussions. Of the four researchers involved in the study, two conducted the interviews, while the remaining two—due to their affiliations with the government and PVOs under study—were excluded from the data collection phase to minimize social desirability bias. This deliberate selection reflected the researchers’ commitment to reflexivity, ensuring the interview process remained impartial and free from undue influence.
All interviews were audio-recorded upon obtaining participants’ informed consent, with session durations ranging from 43 to 69 min. While the interview guide included predetermined open-ended questions, the researchers allowed for flexible discussion to accommodate participants’ narratives, ensuring they remained within the scope of the study. This flexibility and careful probing ensured that data collection was rich and contextualized while minimizing procedural bias. The interviews were conducted primarily in English, with clarifications made in Shona where necessary to ensure participants’ comfort and understanding. Procedures were designed to avoid time constraints during interviews, reflecting the researchers’ priority of depth over brevity. The decision to conclude the data collection process on 7 November 2024 was determined once all 13 participants had been interviewed, rather than based on data saturation.
Data Analysis
The data analysis was conducted using MAXQDA software and facilitated by a senior qualitative research advisor with expertise in thematic analysis
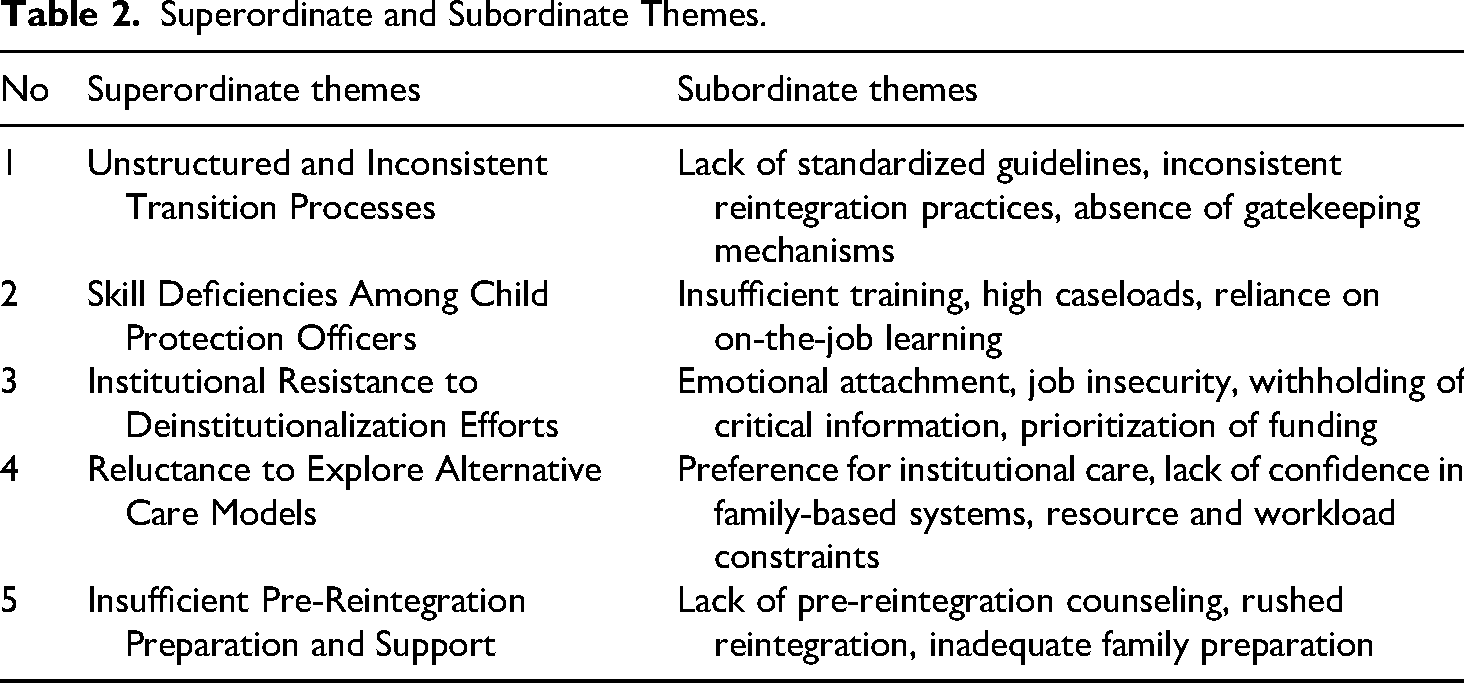
To enhance reliability, a second coder independently reviewed a subset of transcripts, with discrepancies resolved through discussion to ensure coding consistency. Using MAXQDA's “IF” computation function, codes were grouped based on semantic and conceptual overlap. For example, codes related to “emotional attachment,” “job insecurity,” and “institutional funding concerns” were consolidated under the broader theme of “Institutional Resistance to Deinstitutionalisation Efforts.” This process culminated in the identification of five superordinate themes, as shown in Table 2.
Superordinate and Subordinate Themes.
To enhance credibility, expert debriefing sessions were held with four professionals familiar with the deinstitutionalization context. While these experts were not affiliated with participating institutions, they did not participate in data collection or interviews. Their role was to provide analytical insight rather than to validate findings. A member-checking session with 11 of the 13 participants was conducted online on December 14, 2024. Participants were invited to critically review and provide feedback on the themes, rather than merely confirm them. Confidentiality was assured, and participants were informed they could speak freely without risk, given the sensitive nature of the topic.
Findings
Unstructured and Inconsistent Transition Processes
The findings indicate that the process of reintegrating children from institutional care into family or community settings in Zimbabwe is marked by a lack of consistency and structure. Participants commonly described fragmented practices in which decisions were made on an individual basis rather than according to standardized procedures. This led to significant variability in how children were prepared for reintegration, how transitions were managed, and whether any follow-up support was provided. Several participants reported that the absence of clear reintegration frameworks and gatekeeping protocols left Child Protection Officers to rely on personal judgment. This often resulted in rushed placements and inadequate preparation of both children and caregivers. In some cases, reintegration occurred without prior introductions or assessments of family readiness. The lack of systematic monitoring further compounded these issues, with officers acknowledging difficulty in tracking outcomes postplacement.
The pattern suggests that reintegration is often treated as a procedural requirement rather than a developmental process. This perspective may contribute to the marginalization of emotional and relational factors that are critical to successful transitions. Moreover, the absence of institutional guidelines leaves room for wide interpretation of policy, which can lead to uneven standards of practice across different districts or institutions. Two excerpts illustrate this broader pattern: …I have been in the department for a while now, and it seems every officer has their way of reintegrating children into the community. …Despite legislation, there is no step-by-step manual to help us in the process. (Participant 3, Social Worker) …we were just informed that Tinashe [pseudonym] was supposed to be released to the care of his relatives without him having met them before. It was a huge call, and up to now, we haven’t been able to follow up on how he has settled. (Participant 9, Child Protection Officer)
Taken together, these accounts suggest that procedural clarity is lacking, contributing to inconsistent reintegration outcomes and exposing children to heightened social and emotional risks.
Training and Skills Gaps
Participants consistently reported that many Child Protection Officers (CPOs) lacked the experience and training required to manage complex reintegration cases. Several indicated that officers were unfamiliar with assessment protocols, reintegration planning, and child-centered approaches. This gap was particularly evident among those recently appointed to the department, many of whom were said to be navigating their roles without formal induction or ongoing professional development. Rather than following structured reintegration plans, CPOs were described as relying heavily on peer consultation or improvisation. Officers often concluded their involvement once a child left the institution, without conducting proper follow-up. One participant reflected on this challenge by saying: …most of the team at my workstation has been there for less than five years, and we are learning as we go. …there hasn’t been any structured training, at least not since I joined. We just do what we think is best, but we’re not always sure if it's the right approach. (Participant 6, Child Protection Officer)
Beyond procedural issues, participants noted limitations in analytical skills, particularly in evaluating the suitability of family placements. Some officers reportedly placed children in foster care despite the availability of biological relatives who had not been assessed. Participants viewed this as both a technical and an ethical oversight issue. As one evaluator noted: …most children in foster care should have been staying with their biological relatives…but those options are not explored in depth. It's like we skip the full assessment part because there's not enough time or capacity. (Participant 2, NGO Evaluator)
These accounts suggested that the implementation of reintegration strategies was shaped not only by external resource constraints but also by internal professional limitations. Training opportunities were described as irregular and reliant on donor availability. Officers worked under high caseloads, with limited tools and supervision. Ultimately, reliance on informal learning and the absence of a structured training framework weakened CPOs’ ability to make sound reintegration decisions, thereby compromising the effectiveness of Zimbabwe's deinstitutionalization efforts.
Institutional Resistance to Deinstitutionalization Efforts
Participants widely acknowledged that resistance from residential care staff posed a persistent barrier to the implementation of deinstitutionalization. Staff members were described as reluctant to participate in reintegration efforts, often withholding information or delaying processes. This resistance was attributed to a combination of job insecurity, emotional attachment to children, and fear of institutional irrelevance or funding loss. Several participants observed that caregivers who had developed long-term bonds with children found it difficult to support their children's departure. These emotional ties, while human and understandable, were seen to conflict with the strategic goals of family reunification. One Child Protection Officer shared: …caregivers play a crucial role in deinstitutionalisation, having spent significantly more time with the children than we have. …they know the children's routines, personalities, and fears. But some of them withhold key information because they feel the children are better off staying in the institution, or maybe they’re afraid of losing them. (Participant 5, Social Worker)
Others described how institutional priorities sometimes overtook child-centered goals. In some cases, participants reported that residential facilities were reluctant to release children because the number of children in care was directly tied to donor support and operational sustainability. A program evaluator explained: For some institutions, more children translate to more resources. So, when [ child is reintegrated, it's not just about the child leaving, [… ]it's about the loss of funding. That pressure is real. I’ve seen institutions delay decisions or question reintegration plans, even when they know it's in the child's best interest. (Participant 11, NGO Evaluator)
These accounts illustrated how institutional resistance was not merely attitudinal but structurally embedded. The findings showed that caregivers’ emotional bonds and financial dependencies on child headcounts contributed to subtle forms of obstruction. While not always overt, these acts of resistance had a tangible impact on the pace, quality, and sustainability of reintegration. Deinstitutionalization, as experienced by practitioners, was thus shaped not only by resource limitations but by competing interests within the care system itself.
Reluctance to Explore Alternative Care Approaches
Participants widely acknowledged that resistance from residential care staff posed a persistent barrier to the implementation of deinstitutionalization. Staff members were described as reluctant to participate in reintegration efforts, often withholding information or delaying processes. This resistance was attributed to a combination of job insecurity, emotional attachment to children, and fear of institutional irrelevance or funding loss. Several participants observed that caregivers who had developed long-term bonds with children found it difficult to support their children's departure. These emotional ties, while human and understandable, were seen to conflict with the strategic goals of family reunification. A program evaluator explained: Reliance on institutionalisation continues because alternatives are treated as ‘choices’ rather than resourced pathways. If the pathway is not funded, it won’t be used. (Participant 11, NGO Evaluator)
These accounts illustrated how institutional resistance was not merely attitudinal but structurally embedded. The findings showed that caregivers’ emotional bonds and financial dependencies on child headcounts contributed to subtle forms of obstruction. While not always overt, these acts of resistance had a tangible impact on the pace, quality, and sustainability of reintegration. Deinstitutionalization, as experienced by practitioners, was thus shaped not only by resource limitations but by competing interests within the care system itself.
Insufficient Pre-Reintegration Preparation and Support
Participants described a prevailing reluctance among government social workers to discharge children from residential institutions, even when viable family or community-based alternatives were available. This hesitation was linked to a lack of confidence in the capacity of extended families and communities to provide safe and stable care, especially in the context of widespread poverty and weak aftercare systems. Social workers were said to favor institutional placements because they perceived them as more predictable and administratively manageable. This institutional preference was often reinforced by the socio-economic environment in which practitioners operated. Officers were reported to be overwhelmed by high caseloads, limited time, and inadequate resources, leaving them little opportunity to assess or support alternative care options. One participant explained: With the socio-economic challenges bedeviling Zimbabwe, government Child Protection Social Workers are reluctant to explore other forms of care in residential care institutions. With heavy workloads, they don’t have enough time to explore alternatives. So, they just leave the child in the institution where everything is already set up. (Participant 4, Department Officer)
In addition to systemic constraints, some participants pointed to a cultural mindset that viewed institutions as safer or more “complete” environments for children, especially when compared to fragile or unfamiliar family arrangements. Even when children had known relatives, social workers were hesitant to initiate reunifications, citing doubts about the relatives’ reliability or economic readiness. As one officer noted: …we have communicated with our Department of Social Development Officer regarding the children who are known relatives. However, they seem reluctant to move the children to the community. […]there is a general feeling that they are okay in the institution, and that's where they should stay until they are older. (Participant 10, NGO Practitioner)
These findings showed that reluctance to explore alternative care was shaped by a complex interplay of workload pressures, cultural perceptions, and systemic underinvestment in family-based support. Institutional care became the default not necessarily by design, but by omission—where alternative pathways required more time, trust, and infrastructure than the current system allowed. As a result, institutionalization persisted not as a last resort, but as a convenient and habitual response to broader structural constraints.
Discussion
While global debates on deinstitutionalization often polarize around its benefits or risks, this study's findings show that the main challenge in Zimbabwe is not whether deinstitutionalization is desirable as a concept, but whether the system is ready to implement it safely. The practical barriers identified—capacity constraints, weak coordination, cultural resistance, and inconsistent reintegration processes—suggest that the outcomes rely less on the care model itself and more on the structural conditions that support or hinder it. The discussion of these findings is also framed within the 7Cs Framework.
The absence of standardized procedures in Zimbabwe's deinstitutionalization process mirrors global challenges, particularly those observed in Romania and Brazil. In Romania, inconsistent foster care regulations and inadequate monitoring of reintegrated children left many vulnerable (Dragu, 2019), while Brazil's poor follow-up mechanisms exposed children to neglect and re-abandonment. Similarly, participants in Zimbabwe reported that Child Protection Officers lacked clear operational guidelines and were left to improvise reintegration processes, often resulting in rushed, poorly planned placements. This lack of structure increased the risks for children, as officers failed to prepare families or monitor postreintegration outcomes adequately. However, Zimbabwe's context adds unique challenges to this issue. The erosion of traditional caregiving systems—historically reliant on extended families—due to poverty and the HIV/AIDS epidemic has heightened the country's dependence on institutional care (Muzingili & Gunha, 2017). Unlike countries like Sweden and Norway, which rely on well-established foster care systems (Tøssebro, 2016), Zimbabwe lacks the infrastructure to support family-based alternatives effectively. This dependence on institutions and the absence of precise gatekeeping mechanisms highlight the need for locally adapted guidelines that integrate traditional care practices into modern deinstitutionalization frameworks. Addressing these gaps aligns with the “content” and “context” dimensions of the 7Cs Framework, emphasizing the importance of culturally sensitive policies and operational clarity for sustainable reform.
Skill gaps among Child Protection Officers in Zimbabwe reflect a global challenge, with similar issues reported in Kenya, India, and Romania (Chege & Ucembe, 2020; Ramaswamy & Seshadri, 2020). Participants in Zimbabwe noted that many officers were new to their roles, lacked training in child assessment and reintegration planning, and relied heavily on on-the-job learning. This led to rushed transitions, with officers concluding their involvement as soon as children exited institutions. Similarly, undertrained social workers in India and Romania have struggled to monitor reintegrated children effectively, leaving them vulnerable to neglect or re-entry into care (Dragu, 2019; Ramaswamy & Seshadri, 2020). What sets Zimbabwe apart is the scale of its resource constraints and their impact on social work capacity. Many officers manage high caseloads with minimal tools and support, limiting their ability to provide individualized care (Muzingili, 2025). Unlike Scandinavian countries, where sustained investments in professional development have strengthened social work systems (Tøssebro, 2016), Zimbabwe lacks the financial and institutional capacity to train and retain skilled officers. Addressing this gap requires targeted investment in professional development, recruitment, and capacity-building initiatives tailored to Zimbabwe's socio-economic realities. Additionally, integrating community-based knowledge and traditional caregiving practices into training programs could enhance the cultural relevance of reintegration efforts, reflecting the “capacity” and “context” dimensions of the 7Cs Framework.
Resistance from caregivers and staff within Zimbabwe's residential care institutions mirrors similar challenges observed in Bulgaria and Romania, where institutional staff feared job losses and financial instability (Dragu, 2019; Hadjiev, 2018). Participants in Zimbabwe reported that caregivers withheld vital information, delayed reintegration, and prioritized institutional funding over children's best interests. Emotional attachments further complicated efforts, with some caregivers reluctant to let go of children they had cared for over extended periods. Zimbabwe's unique socio-economic context amplifies this resistance. Institutions in Zimbabwe often act as safety nets for vulnerable families, with their operational funding tied to the number of children in care. This creates a conflict of interest, where deinstitutionalization threatens staff livelihoods and the perceived stability of care systems. Unlike Rwanda, where public awareness campaigns have successfully shifted societal perceptions toward family-based care (Murthi & Jayasooriya, 2020), Zimbabwe has yet to implement similar strategies. Addressing resistance requires a two-pronged approach: diversifying institutional funding sources to reduce financial dependence on child numbers and engaging stakeholders through targeted communication campaigns to build trust in family- and community-based care. The “clients and coalitions” and “communication” dimensions of the 7Cs Framework are particularly relevant here, as they emphasize the importance of stakeholder collaboration and public awareness in overcoming resistance.
The findings indicate that Zimbabwean social workers are hesitant to discharge children from institutions, reflecting a lack of confidence in community-based care systems. This reluctance is consistent with challenges reported in Cambodia and India, where cultural stigma surrounding nonbiological caregiving and resource constraints have hindered the adoption of alternative care strategies (Nhep, 2024; Ramaswamy & Seshadri, 2020). Participants in Zimbabwe highlighted that social workers often defaulted to institutional care due to concerns about inadequate community support systems and the complexities of reintegration. Zimbabwe's reliance on institutional care is deeply rooted in its socio-economic context, where poverty and the erosion of traditional care structures limit the viability of family-based alternatives. Unlike countries such as Sweden, where foster care systems are well-funded and guided by strong child welfare policies (Tøssebro, 2016), Zimbabwe's foster care and kinship care systems remain underdeveloped. The “context” and “commitment” dimensions of the 7Cs Framework underscore the need for political will and culturally sensitive approaches to build trust in alternative care systems. Strengthening these systems requires structural reforms—such as reducing social worker caseloads and increasing funding for community-based programs—and cultural interventions, such as public awareness campaigns to counter stigma and promote family-based care.
The lack of pre-reintegration preparation in Zimbabwe is consistent with global challenges, particularly those observed in Brazil, Cambodia, and Nepal. Participants in Zimbabwe reported that children were often reintegrated into families without counseling sessions, home visits, or opportunities to build trust with their caregivers. Similarly, poor preparatory processes in Brazil and Nepal have left reintegrated children vulnerable to neglect or re-abandonment, highlighting the critical role of pre-reintegration support in sustainable deinstitutionalization (Dahal et al., 2024). Zimbabwe's challenges, however, are uniquely shaped by its socio-economic realities. The erosion of traditional care systems due to poverty and the HIV/AIDS epidemic has left many families ill-equipped to provide stable environments for reintegrated children (Gozho et al., 2024b). Unlike Rwanda, which has successfully implemented pre-reintegration support through partnerships with UNICEF (Murthi & Jayasooriya, 2020), Zimbabwe's efforts remain underfunded and fragmented. The “capacity” and “content” dimensions of the 7Cs Framework emphasize the need for clear guidelines and adequate resources to ensure well-planned, sustainable reintegration processes. Strengthening pre-reintegration preparation will require investments in counseling services, home visits, and caregiver training tailored to Zimbabwe's unique cultural and socio-economic context. These findings reinforce the view that deinstitutionalization should not be pursued as a prescriptive model but as a context-dependent reform whose success hinges on the availability of robust, well-supported alternatives to institutional care.
Limitation of the Study
This study faced several limitations inherent to its qualitative design and the context of Zimbabwe's deinstitutionalization program. The sample size of 13 was limited by criterion purposive sampling, which, while appropriate for qualitative inquiry, restricted the diversity of perspectives and precluded broader generalizability. Additionally, statutory restrictions prevented access to children and caregivers, excluding their lived experiences—an essential component in evaluating reintegration outcomes. As the program remains in its formative stage, these exclusions were necessary to protect participant privacy and well-being. Future research should adopt longitudinal approaches that include children and caregivers to provide a more comprehensive, multi-stakeholder understanding of the long-term impacts of deinstitutionalization.
Conclusions and Recommendations
Deinstitutionalization remains a globally endorsed child protection reform; however, in Zimbabwe, it is still at a formative stage, marked by critical gaps in implementation. This study reveals a system grappling with operational inconsistencies, skill deficiencies, institutional resistance, and insufficient preparation for reintegration—issues that undermine the vision of transitioning children from institutional to family- and community-based care. While the long-term goal of deinstitutionalization remains valid, the findings suggest that a more measured and context-responsive approach is urgently required. Rather than pursuing rapid institutional closures, Zimbabwe may benefit from strengthening the quality and regulation of existing residential care while progressively building the capacity for family-based alternatives. A dual-track strategy—improving institutional care as a transitional safeguard while investing in long-term family-based solutions—may offer a more sustainable path forward. The following recommendations are grounded in the 7Cs Protocol Framework, linking challenges directly to strategic action as in Table 3.
Summary of Challenges and Strategic Directions Aligned to the 7Cs Framework.
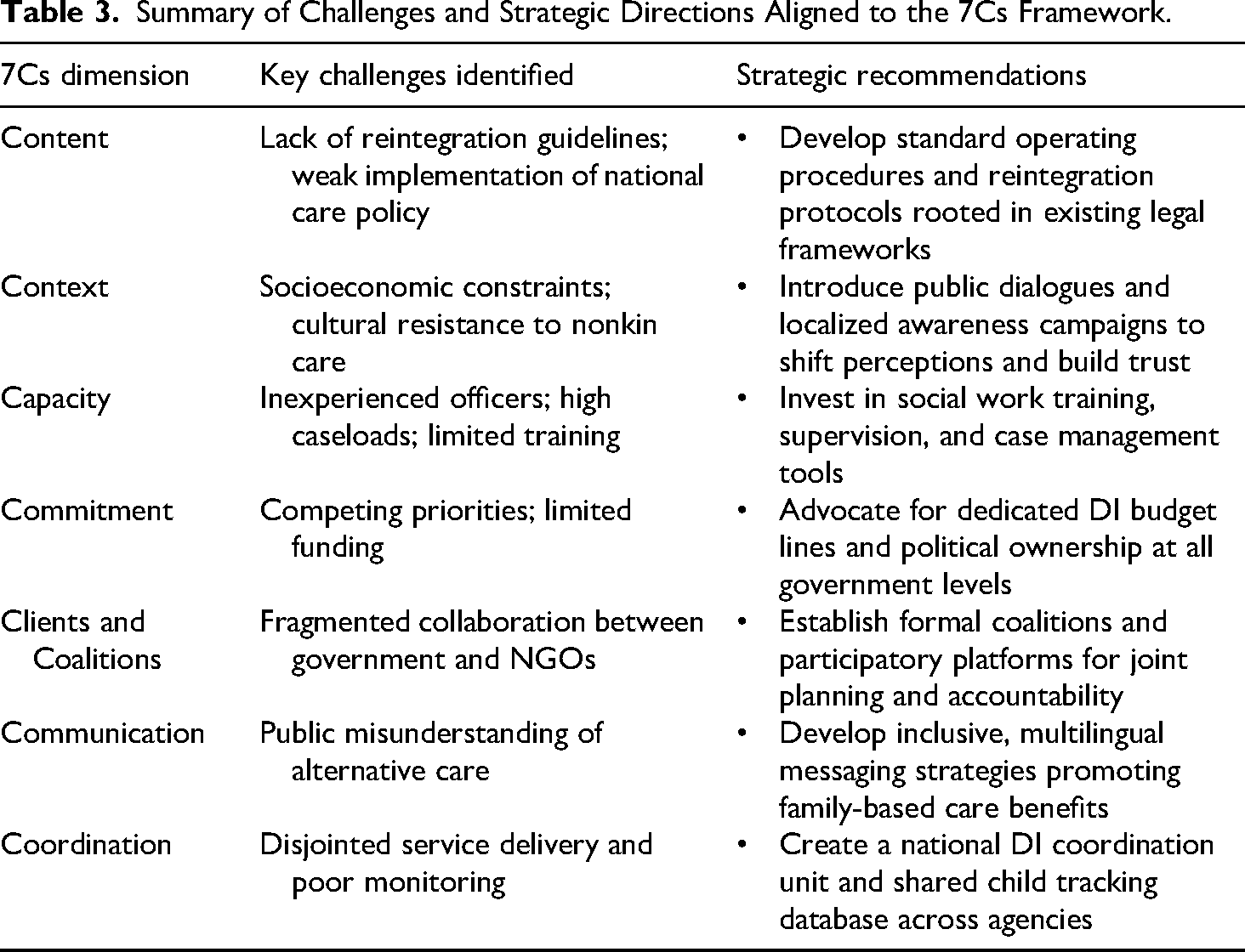
This balanced, phased strategy will allow Zimbabwe to protect children's rights today while preparing for systemic transformation tomorrow, ensuring that reforms are child-centered, contextually grounded, and practically achievable. By foregrounding these practical impediments, the study contributes to a more balanced and contextually grounded understanding of deinstitutionalization—one that recognizes both its potential and its limitations within Zimbabwe's current child protection landscape.
Footnotes
Acknowledgments
The authors express gratitude to the research participants for their willingness to participate in the data collection. Special appreciation goes to the authorities for ethical approval to conduct the study and community entry, respectively.
Ethics and Informed Consent Statements
Ethical approval for the study was obtained from Midland State University (reference number MSU-432/MSU/2024).
Consent to Participate
The researchers actively sought informed consent from the participants. Consent forms clearly outlined the study's purpose. Consent obtained involved agreement to participate and allow the publication of participants’ anonymized data.
Consent for Publication
The study participants consented to the publication of their anonymized and de-identified data.
Author Contributions
Conceptualization (CSG), data curation (TM), formal analysis (TM), funding acquisition (SM), investigation (JDSS), methodology (CSG/TM), project administration (SM), resources (SM), software ™0, supervision (CSG), validation (TM/JDSS), visualization (TM), writing–original draft (CSG), and writing–review and editing (all).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. The researchers and well-wishers solely funded it.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability Statement
Due to ethical restrictions in ethical approval protocols, the data for this study cannot be shared on public repositories. However, the transcribed, anonymized, and identified data is available.
Open Practice
The edited, cleaned, deidentified, and anonymized data presented in this study are available in the Open Science Framework online repository at osf.io/t6kws.