
Abstract
Summary:
An important aspect of palliative care, advance care planning, and end-of-life healthcare is the necessity to ensure that all individuals, including those in the custody of the criminal justice system, receive compassionate and efficient care. While there has been an increase in studies related to inmates’ experiences in prison, a significant gap in the literature is the lack of synthesis gained from qualitative studies. To our knowledge, this is the first qualitative interpretive meta-synthesis of inmates’ experiences who are undergoing palliative care, advance care planning, and end-of-life in prison.
Findings:
The findings resulted in four overarching themes: (1) Inadequate access to health services, (2) lack of compassion toward the inmates, (3) distrust in the system, and (4) institutional control over inmates’ end-of-life decision making. By conducting a qualitative interpretative meta-synthesis, involving seven studies with 200 incarcerated participants, it was found that dignity, death, and dying experiences of inmates were significantly impeded by the prison settings.
Application:
The study indicates absence of adequate sensitive policies around healthcare in prison, especially end-of-life care. Social workers associated with the criminal justice system across the world must therefore be trained to provide psychosocial support to their clients and their families during this difficult time. Social workers must also advocate for their patients’ rights, and train prison staff to provide quality care until more efficient systems are institutionalized.
Background
The United Nations Declaration of Human Rights asserts that all individuals possess “inherent dignity and equal and inalienable rights” (United Nations, 1948, p. 1). These rights are particularly important when considering the needs of terminally ill incarcerated individuals. Barriers to healthcare access for incarcerated individuals can be viewed as a violation of human rights (Johns et al., 2022). Providing appropriate care for incarcerated individuals suffering from chronic or advanced progressive diseases requiring palliative care and end-of-life care has emerged as a pressing global challenge (Maschi et al., 2014; Richter & Hostettler, 2017). Palliative care refers to care that is appropriate at any point in the trajectory of a serious illness or injury and is designed to relieve suffering and improve quality of life while continuing alongside curative or life-prolonging treatments. In contrast, end-of-life care refers to care provided in the period mostly for six months before death, after a decision has been made to prioritize comfort and symptom management rather than cure (American Association of Critical-Care Nurses, n.d.). Notably, the percentage of incarcerated individuals needing end-of-life care is reportedly higher than that of the general population (Pazart et al., 2018). Consequently, as of 2011, national statistics indicated that 44 out of 45 responding state Departments of Correction (DOCs; government agencies that manage prisons and correctional facilities) in the U.S. reported some implementation of palliative care and end-of-life care services within their facilities (Maruschak et al., 2016). Initial research on palliative care within prisons worldwide has identified significant gaps in service provision and a scarcity of research evidence to guide effective practices (Johns et al., 2022; Petreca, 2021). Although most Western jurisdictions have provisions for early release, these are rarely utilized (Kanbergs et al., 2019). Literature suggests this low utilization stems from a lack of awareness regarding policies, ambiguous eligibility criteria, burdensome procedures, and unrealistic timelines (Handtke et al., 2017; Pazart et al., 2018).
Life inside a prison accelerates the aging process due to adverse physical environments and inadequate healthcare, resulting in inmates often presenting physiologically 10–15 years older than their chronological age (Merkt et al., 2020). Furthermore, concerns about maintaining security and control within the prison setting can impede or delay timely access to quality healthcare, including palliative care and end-of-life care services for the incarcerated individuals (Courtwright et al., 2008; Linder & Meyers, 2007). The unique circumstances of incarceration means that inmates who are confronting advanced progressive diseases are often deprived of the choice to die at home. Upholding the human rights principle of equal rights in this context requires provisions such as the presence of an during end-of-life care or advance care planning discussions, similar to practices in the broader community (Johns et al., 2022). Advance care planning refers to the process of discussing and preparing for future decisions about medical care in the event that an individual becomes seriously ill or unable to communicate their wishes (National Institute on Aging, n.d.). Despite the necessity for optimal palliative care for seriously ill incarcerated individuals, there remains a significant lack of understanding about this population (Maschi et al., 2014; Wood, 2007). Expanding knowledge in this area is critical for improving palliative care, end-of-life and advance care planning within prison settings which could significantly inform future needs both in correctional facilities and in community hospitals, where many seriously ill inmates are transferred prior to death.
Literature Review
As of 2021, 11.2 million people were held in prisons globally, which indicates an increase by 17% since the start of the 21st century (UNODC, 2023). Countries like the U.S., El Salvador, and Cuba have the highest incarceration rates, wherein the U.S. incarcerates 541 individuals per 100,000 residents (World Population Review, 2025). It is estimated that by 2030, one third of the prison population in the U.S. will be considered aging (Reetz, 2022). Similar trends are seen in South Korea and several African countries, where overcrowding, lack of funds, and lack of adequate resources put the prison population at risk. Hospice communities have forged collaborations with prisons across the U.S., the U.K., New Zealand, and Germany. Whereas some countries have compassionate release policies, which allow terminally ill inmates to be released early on medical grounds, the specifics of the policies vary from country to country. The main challenges to such policies being implemented are bureaucratic struggles and lack of uniform frameworks. It is also evident that women prisoners across the world often receive less hospice or end-of-life care services than men (Vossel, 2025).
Human rights advocates have long fought for ensuring dignified treatment and access to healthcare for incarcerated individuals across the globe. An important aspect of palliative care, advance care planning, and end-of-life care is the necessity to ensure that all individuals, including those in the custody of the criminal justice system, receive compassionate and efficient care (Burles et al., 2019). This includes access to physical, emotional, and psychological needs of the inmates, which aligns with the international human rights framework laid down by the United Nations Standard Minimum Rules for the Treatment of Prisoners (United Nations, 1955). In 1976, the U.S. Supreme Court ruled that deliberate indifference to inmates’ healthcare needs constitutes cruel and unusual punishment (Rosenfeld, 2016). Since then, numerous policies have been passed across the country in this regard. In European countries, Australia, New Zealand, and Canada, prison hospice systems are in line with these policies (Gilbert et al., 2024). However, in Asian nations, the condition is dire. Due to the compounded social stigma around imprisonment as well as death, there is very little discussion on such services within prison. India paved the way with a cancer and hospice unit in Central Prison, but with only 55 beds, it is highly inadequate to meet present needs (Barasker et al., 2025). Countries like Japan and South Korea also do not have standardized or adequate palliative or hospice care in prison, due to challenges such as budget shortages and overcrowding in adult prisons (Bedard et al., 2017). In South Africa, the Hospice and Palliative Care Association of South Africa has implemented programs in prisons like the Westville Correctional Centre (Sithole & Dempers, 2010). Staff, including chaplains, social workers, and nurses, are trained in palliative care, and inmates are sometimes trained to assist terminally ill peers. In other countries of the continent, efforts are ongoing to integrate community resources with prison hospice care.
In a qualitative study with health professionals regarding their perceptions and experiences of providing palliative care and end-of-life care for hospitalized prisoner patients, Panozzo et al. (2020) found that they face deep moral conflict between the prison constraints and the core principles of palliative care which emphasizes patient autonomy, dignity, and comfort. Often, issues of privacy arise due to the presence of one or more security officers creating a barrier for professionals which hinders the development of trust in the patient–clinician relationship (Linder & Meyers, 2007; Panozzo et al., 2020). These barriers are also reflected in providing effective pain medications and symptom control due to concerns of prison staff about drug misuse and dispensing medications on an as-needed basis (Lin & Mathew, 2005; Linder & Meyers, 2007). Prost et al. (2020) in a national survey examining hospice and palliative care programs in U.S. state prisons found that in many states prison-based hospice and palliative care programs lack formal accreditation and display significant variation in structure, delivery, and training. The training of non-medical staff and correctional officers were often found to be inconsistent, and they receive minimal instruction in the end-of-life care principles (Prost et al., 2020). Ideally advance care planning conversations should result in the person's values and medical treatment preferences being considered in an advance care directive (Buck et al., 2019). But health professionals and inmates feel the prison policies are restrictive in the advance care planning process and the ability for healthcare workers to enact prisoners’ advance care directive as a significant barrier to advance care planning (Ekaireb et al., 2018). Moreover, the COVID-19 pandemic has heightened awareness on providing adequate healthcare to people in prison, including providing accessible palliative care, end-of-life care and advance care planning (Barnert et al., 2021). Thus, it is essential to explore the experiences of inmates relative to their palliative care, end-of-life and advance care planning which will aim to implement the policies and necessary practices among all prison populations. While there has been an increase in studies related to inmates’ palliative care, end-of-life and advance care planning experiences in prison, a significant gap in the literature is the lack of synthesis gained from qualitative studies. Thus, the research question for this study is: What are the experiences of incarcerated individuals in managing their illnesses within the prison and how has it impacted their overall well-being?
Methods
Qualitative interpretive meta-synthesis (QIMS), a methodology developed by and for social work which emphasizes participants’ lived experiences, practice and social justice implications that arise from them (Aguirre & Bolton, 2013). QIMS have been successfully implemented to inform practice ranging from suicide in U.S. jails (Frank & Aguirre, 2013), women's experiences in drug court (Gallagher et al., 2021), and minority youths’ experiences with police encounters (Nordberg et al., 2016). The purpose of this QIMS was to identify and synthesize common experiential themes from qualitative studies and disseminate participant quotes as part of the findings. The overall goal of this study was to better understand what is important for the inmates experiencing palliative care, end-of-life care and advance care planning within the prison, identify constructs that may inform policy implementation and contribute to evidence-based practice. QIMS employs the following steps: identification of studies, theme extraction, translation, and synthesis of findings (Aguirre & Bolton, 2013).
Triangulation is a critical aspect of QIMS as it ensures to establish trustworthiness and reduction of bias (Aguirre & Bolton, 2013). As recommended by Patton (2015), we used triangulation of methods, multiple data sources, and analysts. We achieved triangulation of methods by searching for original studies that utilized mixed method designs as well as purely qualitative study designs. Studies included had collected data utilizing both semi-structured and in-depth interviews. Moreover, the authors also used reference harvesting to check the references for relevant studies (Horsley et al., 2011). Triangulation of analysts was achieved by the first and second authors independently coding the data, and multiple theme review meetings. Both the authors met together via video conferencing and in-person to come to an agreement over the quotes and the final themes. The codes and themes were again independently reviewed by the third author to reduce any potential biases. All three authors have training and experience in qualitative research, in addition to supported by community-based work.
Identification of Studies
Using Academic search complete, Ageline, APA PyschArticles, APA Psychinfo, CINAHL Complete, Criminal Justice Abstracts with Full text, Global health, MEDLINE, Psychology and Behavioral sciences collection, and Social work abstracts, multiple key word searches were performed to identify relevant qualitative studies. Keywords included palliative care, palliative, palliative care, end-of-life, end-of-life care experience, and advance care planning. Each of these were separately paired with words “qualitative,” “incarceration,” “prison,” or “prison inmates.” Searches using palliative care in prison, and incarcerated people in palliative care paired with qualitative were also run. A total of 1769 results were returned across all searches. Two researchers initially reviewed studies by title and abstracts. A total of 194 relevant full text was kept after the title and abstract review and were examined according to the inclusion criteria.
Studies were inlcuded if they were: (1) a peer-reviewed article; (2) conducted with participants above 18 + years; (3) participants were in incarceration or prison or correctional facilities during the time of the study; (4) participants were undergoing palliative or end-of-life care or in advance care planning; (5) containing direct quotes of the participants; and (6) published in English. There were no limitations on published date or geographic location. Studies or quotes from caregivers, social workers, nurses, or prison staff or anyone else than the inmate was excluded from the study. The final sample included seven qualitative studies, from France (Chassagne et al., 2017), Switzerland (Handtke & Wangmo, 2014), the U.S. (Kitt-Lewis et al., 2024; Loeb et al., 2014; Sanders et al., 2018; Sanders & Stensland, 2018), and U.K. (Turner et al., 2018) (Table 1).
Studies included in the sample.

Theme Extraction, Translation, and Synthesis of Findings
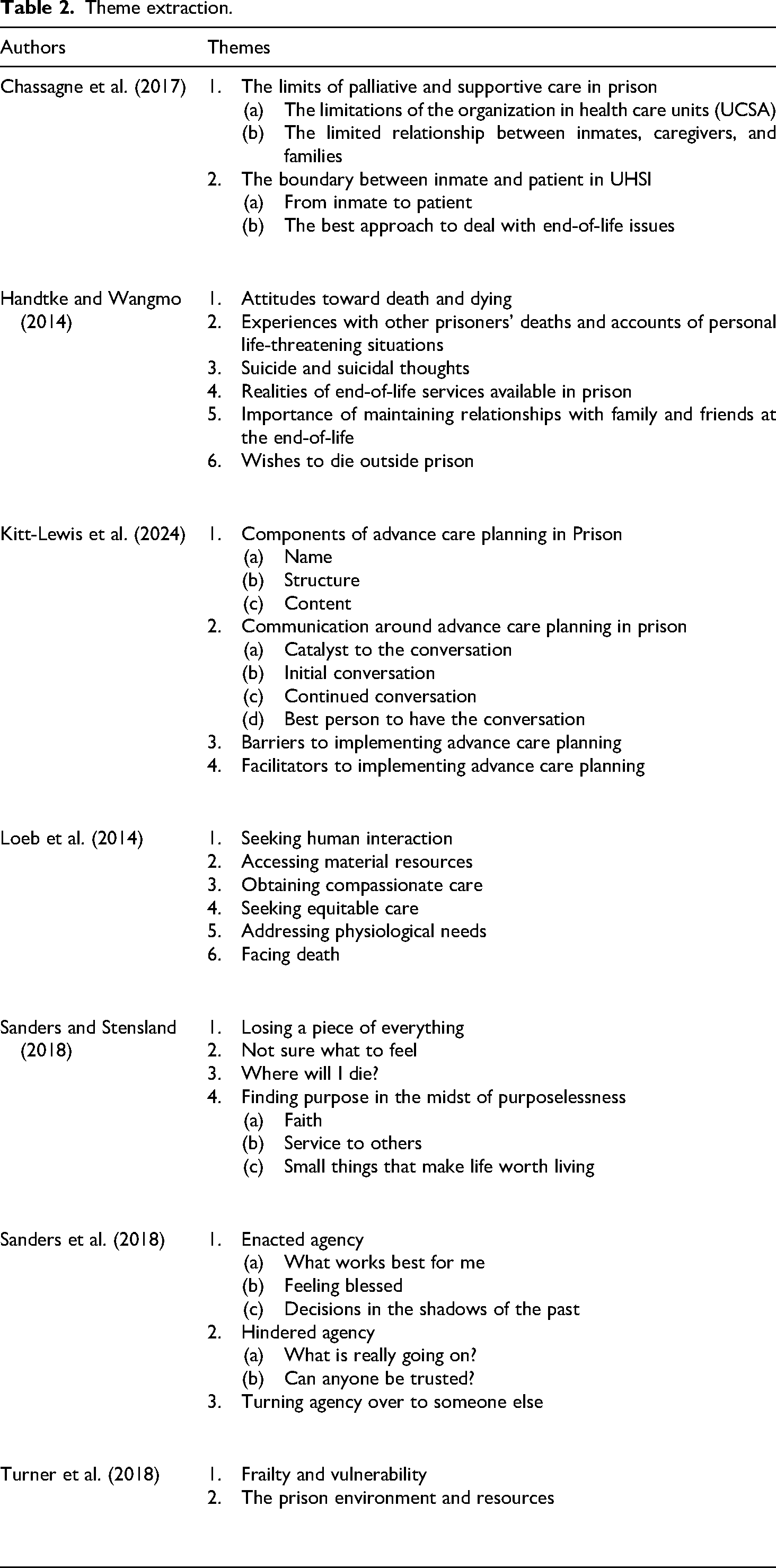
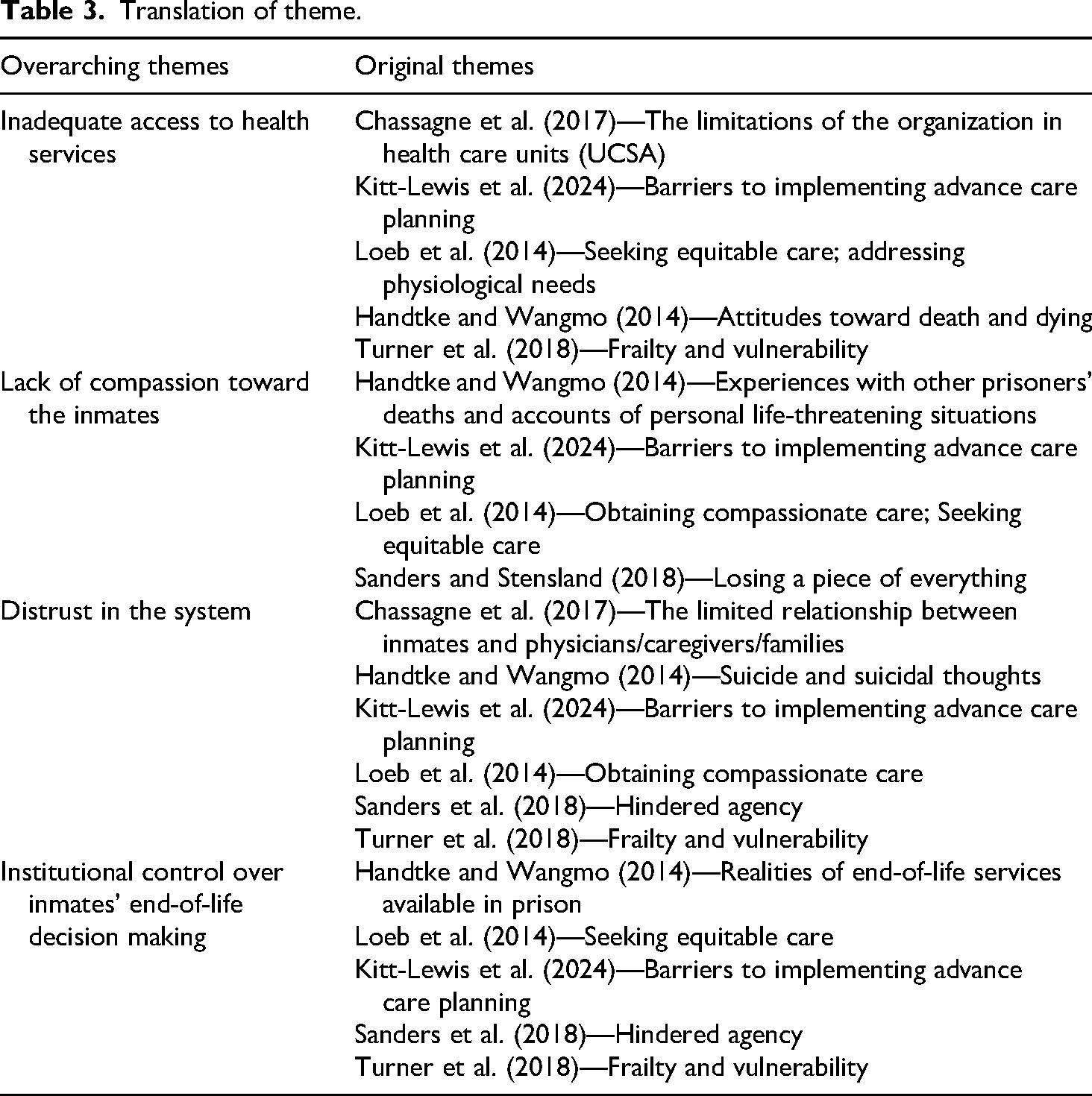
Authors of included studies identified many themes related to the palliative care, end-of-life, and advance care planning experience which are presented in Table 2 using the original language to maintain the integrity of the initial studies and researchers. All direct quotes and summary of these themes from each of the studies were extracted from the original articles by the first two authors. Using a grounded theory approach, the extracted data are analyzed. Initially, the first author analyzed the extracted data through open coding, where new overarching themes emerged. Using the constant comparative method (Fram, 2013), common themes were developed between them, with axial codes developing along with a fine tuning of themes with each additional article. These codes and themes were then reviewed by the second and third author to discuss translations to ensure shared understanding, minimizing potential bias. Table 3 provides an overview of the new themes and portrays how original themes contributed in the development of understanding.
Theme extraction.
Translation of theme.
Findings
The final sample of seven studies included a total 141 quotes from over 200 participants, with the average age of 60 years. Of the reported ethnicities, 77.2% were White, 13.64% were Black, and the others identified as Latino/Hispanic, Native American, or Asian. All the included studies collected data through interviews, except for Sanders and Stensland (2018) and Sanders et al. (2018), who collected data through mainly field notes and observations of the inmates. Four themes emerged from our analysis: Inadequate access to health services, lack of compassion toward the inmates, distrust in the system, and end-of-life decision making among inmates.
Theme 1: Inadequate Access to Health Services
Participants often reported significant challenges in accessing timely and effective health services (Kitt-Lewis et al., 2024). These experiences not only delayed appropriate treatment but increased feelings of uncertainty. As one participant recalled, “No one told me I had cancer. I went back in 2 weeks for an appointment. The nurse read my chart and said I had to do a do-not-resuscitate. Then the nurse backtracked and said, ‘No, you don't have cancer,’—not one person told me I had cancer until I went on sick call and talked with the doctor and he confirmed I had cancer” (Kitt-Lewis et al., 2024).
Beyond miscommunication, the inaccessibility of mere medical test results contributed to further feelings of helplessness. A participant expressed how he felt tired all the tame as he could not even stand. Eventually, he was sent to a hospital where he received three units of blood (Loeb et al., 2014). Furthermore, institutional protocols such as paperwork were seem to be prioritized over emergency and the need for urgent care, as one participant highlighted, “Of course the health service says that you first—you can’t just come—‘yes, fill out a form.’ … What? If you have a heart attack. you go there and fill out a form?! No, that's just petty. Always their rules” (Handtke & Wangmo, 2014). These experiences demonstrate how inefficiencies and rigid institutional policies created hurdles in accessing care which in a way undermines the basic right to health for incarcerated individuals.
Theme 2: Lack of Compassion Toward the Inmates
Across the studies, participants reported being subjected to a profound absence of compassion particularly during periods of illness and death. Suffering of the inmates were met with dismissal and dehumanization rather than empathy. A participant mentioned the feeling of casual disregard shown by staff when inmates’ health deteriorated, “when an inmate's health goes downhill, the attitude is, ‘well, it's another one gone that we don’t have to put up with no more’” (Loeb et al., 2014).
During moments of mourning, often the inmates’ grief was similarly invalidated. One participant described the absence of compassion within the prison environment, recalling that they were frequently yelled at (Kitt-Lewis et al., 2024). Additionally, participants expressed that deaths of fellow inmates were treated with coldness and absence of basic gestures of acknowledgement which reinforced their feelings of invisibility and devaluation. A participant described this instance wherein, “They don’t have to make a big fuss out of every death, be it due to age or because of a disease, but they could [at least] make an announcement, a little paper, where they say inmate so-and-so has died” (Handtke & Wangmo, 2014).
Theme 3: Distrust in the System
Across the studies, distrust toward the prison healthcare systems emerged as a persistent theme. This distrust was rooted in inmates’ lived experiences of neglect, perceived unethical practices, and breaches of confidentiality. A participant reflected that inmates’ conditions or experiences were not being cared in prison setting (Sanders & Stensland, 2018). Another participant expressed deep suspicions which were fuelled due to the neglect experienced and the histories of abuses associated with incarcerated population as, “Maybe they are testing a drug and they want to go all the way, I don’t know, or maybe I’m becoming paranoid, because I don’t feel good in my body [shakily]” (Chassagne et al., 2017).
Inmates who wished to initiate conversations about their advance planning were met with inappropriate responses which undermined their trust. A participant mentioned, “Over a decade ago, I wrote to the infirmary and asked about it, living will and advance directive. They [staff] sent me to psych because they thought I was suicidal” (Kitt-Lewis et al., 2024). Moreover, participants have consistently reported receiving conflicting health assessments from different authorities. A participant described feeling scared and confused due to contradictory diagnoses as he has gotten different information from each medical staff he encountered (Sanders et al., 2018). These instances reveal the lack of transparency, unethical and unreliable care that inmates were subjected to which created an environment of profound mistrust by the very institutions charged with their well-being.
Theme 4: Institutional Control Over Inmates’ End-of-Life Decision Making
The findings of this theme revealed that incarcerated individuals reported having little to no-knowledge on the concept of advance care planning or end-of-life care over their healthcare decisions. Inmates mentioned being unfamiliar with the concept of advance care planning despite spending decades incarcerated: “…lots of folks are in pain but they have a policy where they don’t want folks to get addicted to narcotics…they try things like extra strength Tylenol or Ultram…they’re [dying prisoners] really suffering and really in pain” (Loeb et al., 2014).
Even when inmates attempted to express their healthcare wishes, it was frequently overridden. The loss of autonomy on their own death was troubling. A participant stated how he was resuscitated against his wish after being requested on no resuscitation (Sanders et al., 2018). Beyond the physical suffering, which is visible to the eyes, a fear of dying isolated from family also tend to have a profound impact on the emotional anguish of the inmates. A participant while mentioning this about older inmates said, “One of the greatest anxieties for older prisoners is becoming terminally ill in prison, cut off from the loving support of families and subject to a regime that can be unkind” (Turner et al., 2018).
The findings of the study indicate that incarcerated individuals’ experiences with palliative care, end-of-life care, and advance care planning processes are shaped by multiple contextual factors, including security protocols, institutional culture, and interpersonal dynamics with correctional staff. Factors such as sentence length, illness progression, cultural background, and frequency of hospital transfers may influence how individuals interpret their illness and their opportunities for decision-making of their life outcomes. However, subgroup-specific insights such as gender, ethnicity, or age could not be systematically examined due to inconsistent variation in the inclusion studies. This gap indicates the need for future qualitative research that more intentionally documents and compares the experiences of diverse incarcerated individuals.
Discussion
This review study discusses the extent and nature of the evidence in access to healthcare during end-of-life situations in prison. By conducting a QIMS, with over 200 incarcerated participants, it was found that dignity, death, and dying experiences of inmates were significantly impeded by the prison settings. Many inmates reported experiencing systemic barriers to accessing timely and adequate healthcare (Handtke & Wangmo, 2014; Kitt-Lewis et al., 2024; Loeb et al., 2014). Compounded bureaucratic procedures including complicated documents, approval processes resulted in delays in the inmates’ diagnosis and treatment. While staffs in prison prioritized documents over inmates’ medical needs, many inmates experienced miscommunication and missing information were commonly reported for the reasons of medical neglect. On top of that, institutional policies led to unethical delays even during medical emergencies. The inmates’ experiences of medical neglect, even under urgent medical needs and critical health condition, heightened feelings of hopelessness, fear, and mistrust. This shows how structured healthcare system in prison failed to consider the basic human right and worsened physical and mental suffering, as well as emotional uncertainty for those going through end-of-life stages.
Participants frequently described interactions marked by dismissiveness, lack of empathy and compassion from prison staff, which led them to suffer during their diagnosis, and overall dying experiences (Handtke & Wangmo, 2014; Kitt-Lewis et al., 2024; Loeb et al., 2014; Sanders & Stensland, 2018). An individual's illness and death were often met with indifference and a sense of dehumanization. Emotional neglect, compounded by medical negligence, left many of them feeling invisible and stripped of their dignity when compassion was most needed, specifically going through end-of-life care experiences or grief of loss for another inmate. The process of managing death both logistically and emotionally, was often treated as an administrative burden, showing lack of humanity in final days of the inmates.
A pervasive theme was distrust in the institutional healthcare system. Participants reported inconsistent assessments, conflicting medical information, and fears that their concerns were minimized or misunderstood. Few inmates described long-standing institutional histories and personal experiences that shaped this mistrust, complicating interactions with healthcare providers and limiting willingness to engage in processes such as advance care planning (Kitt-Lewis et al., 2024; Sanders et al., 2018). The interpretation of advance care planning inquiries by the inmates were often seen as psychiatric crises, as illustrated in Kitt-Lewis et al. (2024) which highlights the lack of clarity, training, and structural support for such conversations inside these settings.
The inmates often faced judgement and neglected, going through the end-of-life care stages (Chassagne et al., 2017; Kitt-Lewis et al., 2024; Sanders et al., 2018). This environment fostered a deep mistrust of prison healthcare systems. Witnessing misdiagnosis, neglect, lack of medical information, and unethical treatments among inmates, brought fears of being targeted to experimental treatments without consent, even though there was no documented evidence of such occurrences. The inmates’ efforts to consider advance care planning were interpreted as mental health crises, involving suicidality, reversely showing the prison staff's distrust in inmates and conflicts the relationship between prison staff and inmates (Kitt-Lewis et al., 2024). When advance care planning is supposed to focus on the goals of human and ethical palliative practice, these incarcerated individuals encountered suspicion, control, and fear.
These compounded challenges and sufferings of inmates experiencing the final days of their lives ultimately made them feel disempowered in decision-making process, particularly about end-of-life care and advance care planning. Having education on advance care planning was not inmates’ option to manage their health condition, which shows the systemic failures in patient health education. Inmates’ preferences and wishes when it comes to death and dying were often ignored by institutional authorities. Moreover, the inmates’ feelings of loss of autonomy at end-of-life care significantly increased emotional distress, particularly when they already have fears of dying alone, and without family support. This signified the way of institutional priorities affects the inmates’ both physical and emotional suffering, by limiting self-determination, dignity, and humane treatment at the end-of-life care. This also underscore urgent reforms within prison system is needed to respect humanity and dignified palliative care and end-of-life care for incarcerated individuals. To mitigate complicated burdens and conflicts between incarcerated individuals at the end of their lives, and correctional staffs, staff training is important to uphold ethical standards of care and practice empathy and compassion when encountering palliative care and end-of-life care for incarcerated population.
Implications and Future Directions
The study indicates absence of adequate sensitive policies around healthcare in prison, especially end-of-life care. Social workers associated with the criminal justice system across the world must be trained to provide psychosocial support to their clients and their families during this difficult time. advance care planning training for prison inmates might also be an useful step in ensuring that they can exercise their agency. More sensitive policies are the need of the hour. Patient-centered policies prioritizing health needs of inmates will ensure that prisoners also get to exercise their human rights. There is a need for more transparent and democratic policy processes where timely and adequate care services are prioritized. There is a worldwide need to institutionalize policies which install end-of-life care ecosystems inside prisons, that ensures transparency and accountability. To ensure that these policies benefit the prisoners, there is a need for evidence-based policy making processes. Therefore, researchers must focus on exploring different dimensions of in prison end-of-life care through longitudinal studies, which can capture patterns of health trends over time.
Due to the huge power imbalance between prisoners and other stakeholders serving them, it is necessary to also research the ethical practices adopted by the prisons, which will highlight situations of neglect and systemic barriers to prisoners’ access to quality healthcare. Considering that health can also be impacted by the terms of the imprisonment itself, researchers must look into comparative studies between prison populations and outside populations, accounting for an intersectionality of sociodemographic factors (Strong et al., 2020). This will help researchers identify key factors leading to poor health of prisoners, which can be used to reduce the burden on the prison healthcare system. The study also highlights the need to study prison healthcare systems around the world, with country specific conceptual frameworks which account for socio-cultural and economic variations. There is also a need to recognize that inmates undergoing treatment while in custody, stand in the crossroads between the right-based healthcare system and the punitive criminal justice system, indicating a need for interdisciplinary approach in research in these areas (Thuma, 2025).
Limitations of the Study
In this QIMS review, inmates’ experiences were synthesized and interpreted from seven published studies in which a range of end-of-life care experiences were explored. One limitation is the possibility that important findings might have unintentionally left out by the search criteria, researcher bias, or human error. Since the results were limited to direct quotes from qualitative studies and demographic data were marginally reported, the findings may not be generalizable or representative of all people who experience end-of-life care in the prison. Demographic details such as gender, ethnicity, and age varied among all the included studies which prevented the authors from a detailed analysis of subgroup differences. As a result, the themes presented here should be interpreted as reflective of broad experiential patterns rather than fully representative of all incarcerated individuals receiving end-of-life care. Lastly, since this study only included articles from global north countries, the findings cannot be applicable to other countries with very different economic structures and cultural values. Even among the selected countries, the authors could not account for socio-cultural differences, due to the broad range of populations. Future studies may consider these viewpoints for a more holistic approach toward the intersection of the healthcare and criminal justice systems.
Conclusion
The findings of this study illuminate profound systemic failures in the prison healthcare system, particularly in the context of palliative care and end-of-life care for incarcerated individuals. Across multiple studies, the absence of timely, ethical, and compassionate healthcare delivery has contributed to physical suffering, emotional distress, and a deep mistrust of institutional medical services. Bureaucratic hurdles and rigid administrative processes have continuously prioritized complex long drawn-out formalities over immediate medical needs, worsening health outcomes for older inmates. Delayed diagnoses, miscommunication, and inadequate emergency responses reflect the negligence embedded in prison healthcare, directly undermining the basic human right to health. Additionally, medical neglect, whether through oversight, lack of urgency, or dismissive attitudes, has left inmates feeling unseen and abandoned during critical moments, amplifying feelings of helplessness and despair.
Beyond structural inefficiencies, the emotional and psychological impact of prison healthcare neglect is deeply troubling. A prevailing lack of compassion from prison staff has reinforced a sense of invisibility, stripping inmates of dignity when they need empathy the most. The absence of acknowledgment in moments of mourning, coupled with the cold treatment of dying inmates, further isolates them from humanity. These experiences amount to social death, where the individual loses their sense of agency and value within society. Furthermore, entrenched distrust in medical care exacerbates anxieties among incarcerated individuals, with fears of misdiagnosis, unethical treatments, and experimental medical practices looming over their healthcare experiences. The inability to participate in advance care planning and make informed decisions about their own end-of-life care further denies them autonomy, reinforcing control by prison authorities over their final moments.
Ultimately, these findings underscore an urgent need for prison healthcare reform to ensure humane treatment and uphold ethical standards in end-of-life care. Institutional policies must shift from bureaucratic rigidity to person centered healthcare, enabling incarcerated individuals to access timely and adequate medical support. Comprehensive staff training programs should emphasize empathetic and ethical palliative care, fostering a more humane environment for aging and terminally ill inmates. Additionally, advance care planning education and accessibility must be expanded, ensuring inmates have the autonomy to make informed end-of-life decisions. Without these systemic changes, incarcerated individuals will continue to endure preventable suffering, reinforcing a cycle of neglect and dehumanization. Addressing these injustices is not simply a matter of prison policy. It is a moral obligation to uphold human dignity and basic healthcare rights for all individuals, regardless of their circumstances.
Footnotes
Acknowledgements
We thank Professor Jaya B. Davis, for her mentorship and advice during the QIMS study and review of the manuscript. We also thank the research librarian, Hailey Carson, for her advice on relevant databases, and in creating search strings used in this review.
Ethics
Research ethics approval was not required as this QIMS study constitutes secondary research.
Authors’ Contributions
SH, SJ, and SDB contributed to the design of the study. SH and SJ led the initial round of coding and theme development. This was further adapted and reviewed by SDB. All authors were involved in drafting and reviewing the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.