
Abstract
Summary
Research shows that young adults with intellectual disabilities are eager to engage in conversations about sexuality and intimacy, but the nuances of these discussions from their own perspective remain unexplored. This study aims to understand the challenges, facilitators, and dynamics that influence these young adults' engagement in conversations about sexuality and intimacy with family, friends, and support networks. The data comprise 22 qualitative interviews with Swedish young adults aged 18-35 with intellectual disabilities.
Findings
Thematic analysis revealed four themes: (1) Sharing is caring-motivating and initiating conversations about sexuality and intimacy; (2) Safe spaces-facilitators of sexual and intimate communication; (3) Being overlooked and feeling unheard; and (4) Overprotection and self-blame. The findings show that young adults with intellectual disabilities encounter additional challenges when engaging in conversations about sexual or intimate matters with their broader support networks. Trust plays a pivotal role in determining with whom they choose to have conversations about these topics, and societal norms can impede the occurrence of crucial conversations. In the discussion, the findings are explored further guided by Ken Plummer's theoretical framework, which outlines four levels in the process of producing and consuming socially constructed sexual narratives.
Applications
These insights are vital for enhancing social work practices, informing policy development, and guiding the creation of supportive interventions that foster inclusive environments. By recognizing and addressing these barriers, professionals can better support the sexual health and well-being of young adults with intellectual disabilities, promoting their agency and self-determination in intimate matters.
Introduction
Conversations concerning sexuality and intimacy can be challenging for most young people, who frequently encounter insecurities, limited knowledge, cultural constraints, and difficulties in navigating communication around sensitive and personal subjects (Holmström et al., 2020). Many turn to friends and family for support and conversation (Byron, 2016; Powell, 2008), while a growing desire to talk to professionals has also been noted, primarily about sexual and reproductive health (Public Health Agency, 2017). However, for young adults with intellectual disabilities, the complexity of such conversations is heightened by cognitive impairments that impact their comprehension of sexuality and intimacy, including difficulties in interpreting sexual norms (Hart et al., 2024; Löfgren-Mårtenson, 2020). Additionally, this demographic is frequently marginalized and lacks social networks and opportunities for sharing informal knowledge with other members of society, such as peers and friends (Nelson et al., 2020). Nevertheless, many young adults with intellectual disabilities express a strong desire for social inclusion (Ferrante & Oak, 2020; McCarthy et al., 2022) and a wish to engage in conversations about romantic relationships and sexual experiences (Retznik et al., 2021). Yet, this dimension remains underrepresented in social work practice, where risk-focused or medicalized approaches tend to dominate (Bahner & Lukkerz, 2023). In this context, social work plays a pivotal role in promoting sexual well-being (Dodd, 2020; Goulden, 2021). Part of this involves recognizing and including the perspectives of young adults with intellectual disabilities when providing social support related to sexuality and intimacy (Dodd, 2020). This article explores how young adults with intellectual disabilities engage in conversations about sexuality and intimacy with family, friends, and broader social support networks (e.g., school counsellors, social workers, or staff members at group homes) in a Swedish context.
In Sweden, individuals with intellectual disabilities have the right to receive support and services to facilitate their integration into mainstream society, as stipulated by the Swedish Act on Support and Services for Persons with Certain Functional Impairments (1993:387). The law is designed to make it possible for young adults with intellectual disabilities to live their lives in alignment with the general population (Olin & Jansson, 2008). Even so, issues related to sexuality and intimacy are often overlooked (Bahner et al., 2024). Research shows that the implementation of sexuality related policies within social work remains inconsistent and insufficient, creating barriers to adequate support (Bahner, 2020; Löfgren-Mårtenson, 2020). These challenges are not confined to Sweden but are observed in broader international contexts (Bahner, 2020). In a UK setting, Maguire et al. (2019) noted that inadequate guidelines and support structures in social work hinder young people with intellectual disabilities from engaging in open and honest conversations about sexuality. Similarly, research from the USA, (Dodd, 2020) suggests that this may be due to inadequate training for social work professionals in addressing sexuality, which often results in a predominant focus on risk rather than promoting sexual advocacy.
Conversations About Sexuality
A study conducted in Spain by Gil-Llario et al. (2018) found that almost 90% of individuals aged between 19 and 55 who had intellectual disabilities expressed a desire for more frequent conversations about sexuality. Female participants who had experienced abuse reported feeling uncomfortable confiding in someone about their traumatic experiences. Only 53% felt secure enough to share their experiences, indicating significant barriers to trust within this population (Gil-Llario et al., 2018). Gil-Llario et al. (2018) therefore argued that broader societal networks need to be more open and inclusive in conversations about sexuality and intimacy with individuals with intellectual disabilities. According to Black and Kammes (2019), individuals with intellectual disabilities want friends with whom they can talk about sexuality and relationships, but knowledge on these types of conversations is still lacking. Schaafsma et al. (2017) found that attitudes toward support-seeking for sexuality-related issues varied among individuals with intellectual disabilities. Some were comfortable conversing with care providers, while others hesitated as a result of privacy and embarrassment concerns. According to Frawley and Wilson (2016), young adults with intellectual disabilities preferred having conversations about sexuality and intimacy with friends rather than parents or staff. Individuals with intellectual disabilities frequently encounter societal stigmatization and often live in paternalistic environments (Foley, 2018) characterized by restrictive sexual scripts. Löfgren-Mårtenson (2013) described these scripts as socially constructed norms that reflect society's restrictive views on this group's sexuality, reinforcing control and limitations through protective attitudes and regulation. This context often necessitates their seeking permission to engage in sexual activities (Ferrante & Oak, 2020), potentially impeding their capacity to confidently discuss positive aspects of sexuality and intimacy (McCarthy et al., 2022). This can lead to secrecy and a perpetuation of the current social silence on these issues (Bahner et al., 2024; Rushbrooke et al., 2014).
Despite an increased societal focus on sexuality, our understanding of how young adults with intellectual disabilities engage in conversations about sexuality and intimacy remains limited. This gap in knowledge highlights the need for further research to explore the complexities that characterize the experiences of young adults with intellectual disabilities and to identify factors that affect their ability to engage in transparent conversations on these crucial subjects. This study aims to provide an in-depth understanding of the challenges, facilitators, and dynamics that influence the way young adults with intellectual disabilities engage in conversations about sexuality and intimacy with their family, friends, and broader social support networks.
Theoretical Perspective
This study employs the sociologist Ken Plummer's (1995) theoretical framework on sexual storytelling as a foundational lens to investigate the experiences that young adults with intellectual disabilities have of conversations about sexuality and intimate relationships. Sexual storytelling is commonly associated with narrative analysis and life stories (Jackson & Scott, 2023). Although this study does not employ traditional narrative methods, Plummer's theoretical framework (1995) facilitates the interpretation of this demographic's experiences of engaging in sexual and intimate conversations with family, friends, and a broader support network.
As a means of comprehending the social construction of sexual stories, Plummer (1995) described four levels that are involved in the ongoing process of producing and consuming such stories. The cultural and historical level relates to the broader cultural and historical contexts that shape perspectives on sexuality. It encompasses cultural norms, values, traditions, and historical events that shape how sexuality is understood and expressed in different societies and at different times. Plummer (1995) argued that historical and cultural perspectives significantly influence views on sexuality. This is relevant to the living conditions of people with intellectual disabilities, most of whom historically grew up in single-gender institutions, socially isolated from the rest of society (Bahner, 2020). The organizational level includes the institutional and organizational structures that shape and regulate an individual's sexual narrative. Institutions such as laws, political systems, medical institutions, and religious organizations play a crucial role in shaping and regulating the understanding and expression of sexuality in society. For example, individuals with intellectual disabilities were forcibly sterilized as a result of laws that existed in Sweden during a large part of the twentieth century, and their need for sexuality and love was ignored (Altemark, 2017). The situational level focuses on the way social and physical environments shape sexual behaviors and experiences and recognizes the impact of various contexts and social interactions on individuals’ sexual actions and identities. Here, research has shown that staff members’ values regarding sexuality and intellectual disability impact on individuals’ options and obstacles relating to sexuality, love, and relationships (Löfgren-Mårtenson, 2020). Sexuality on a personal level involves an individual's subjective experiences, emotional responses, and self-identifications. These include perceptions, reactions to sexual encounters, and sexual preferences. Sexual agency is as important for people with intellectual disabilities as for others, not least due to their dependency on others and their lifelong need for support (Löfgren-Mårtenson, 2020). In the discussion section, the findings will be related to Ken Plummer's (1995) theoretical perspective on telling stories across different levels.
Method
To obtain in-depth knowledge of the way young adults with intellectual disabilities experience having conversations with others about sexuality and intimacy, this study utilized a qualitative research approach, conducting 22 semi-structured individual interviews (with five males and 17 females). The first author conducted all interviews and has long experience working with sexual health and individuals with intellectual disabilities.
Recruitment
Recruitment was conducted in Sweden during the year 2022 and involved participants between the ages of 18 and 35 who had intellectual disabilities, were able to verbally express themselves in Swedish or English, and had prior experience of talking about sexual or intimate experiences. Given the developmental variability of those with intellectual disabilities, participants up to age 35 were included. This strategic sampling approach (Creswell & Poth, 2018) ensured that participants possessed the necessary language and communication skills for interviews. In addition, those with whom the first author had been in contact in a clinical setting were excluded due to their state of dependency (Creswell & Poth, 2018). The first author initiated contact with key individuals within a number of relevant organizations (e.g., day activity centers or special needs upper secondary schools), commonly referred to as “gatekeepers,” who can either obstruct or facilitate access to research participants (Ahern, 2014). In this study, gatekeepers included staff members at the operational level who worked closely with the target group. Their insights and experiences were instrumental in the selection of interview participants. Securing the opportunity to inform potential participants about the study was challenging and required clearly and comprehensively explaining the research process and content to the staff. The intention was to provide potential participants with information in advance and to arrange a meeting with the researcher prior to the interview to foster trust and allow for any questions to be addressed (Hollomotz, 2018). In practice, however, most participants met the researcher only at the time of the interview. In some cases, participants had been informed about the study via support networks and by peers who had participated in scheduled interviews, leading to a snowball effect that increased participation. All those who agreed to participate completed the interviews. This suggests a general interest among the participants in sharing their experiences.
Interview Procedure
Participants were provided with information before the interview. Control questions were adjusted to meet individual needs and were used to confirm that participants understood and were willing to participate (Hollomotz, 2018). Participants then provided written or recorded informed consent, depending on which they felt most comfortable with. The interviews followed an interview guide that covered the research topic and prioritized reflexive and participant-centered interviews, which lasted between 20 and 60 min (most lasted an hour). Open-ended questions were strategically employed to cater to the diversity in participants’ understandings and to elicit contextualized responses (Emerson et al., 2012).
Interviewing individuals with intellectual disabilities can pose several challenges to the interviewer. For instance, participants may provide only brief responses or exhibit loyalty toward their support system, e.g., care providers (Hollomotz, 2018). The first author is aware of potential biases such as “yes-saying,” idealization, and the “interviewer effect” commonly observed in interviews with individuals with intellectual disabilities (Tøssebro, 1992). The “interviewer effect” complicates responses, since participants may hesitate to voice criticism about individuals on whom they rely (Löfgren-Mårtenson, 2012). Although verbal communication was an inclusion criterion, visual aids were prepared to facilitate communication in the interview situation. The purpose of the visual aids was twofold: first, to support improved understanding of the subject; and second, to help situate the participants within the appropriate context. The use of visual aids is an established method in research involving this group (Hollomotz, 2018). However, despite the availability of this option, the participants opted not to utilize the visual aids, instead describing their experiences in their own words. This underscores the importance of maintaining methodological rigor and critically evaluating responses to ensure the credibility and trustworthiness of the data collected (Creswell & Poth, 2018). In line with previous research, the first author ensured that the participants fully understood the implications of participating in the research project, and information was adapted to the individual's needs (Hollomotz, 2018).
The interview process began with broad introductory questions such as “Please tell me about yourself” and “How does your relationship status look at the moment?” These initial inquiries provided a foundation for conversations about experiences of having conversations related to sexuality and intimacy, allowing participants to contextualize their responses within their narratives (Hollomotz, 2018). To promote mutual understanding and facilitate potential revisions or elaborations of responses, participants’ responses were verbally summarized either during or after the interview. This approach was intended to create a collaborative and supportive environment in which participants could express themselves effectively and authentically, which is particularly important when interviewing this population (Hollomotz, 2018).
Analytical Method
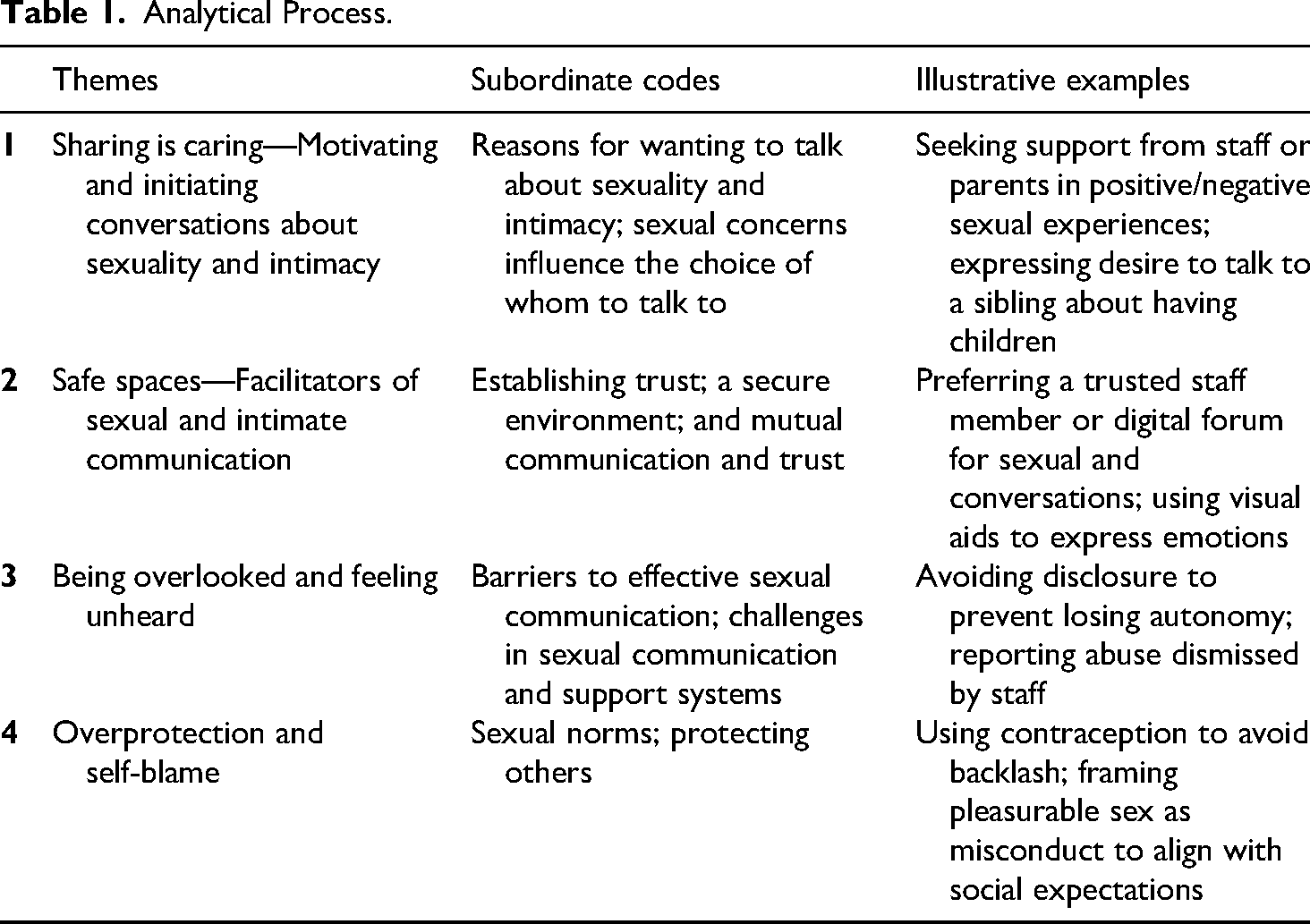
All interviews were recorded and transcribed verbatim, and the transcriptions were then imported into NVivo, a software tool used for qualitative data analysis (Dhakal, 2022). The procedures for coding and analysis adhered to the methodological guidelines established by Braun and Clarke (2022) for thematic analysis. Thematic analysis is conducted using a systematic approach to identify, interpret, and organize patterns that emerge repeatedly in qualitative data (Braun & Clarke, 2022). The coding process entailed an examination of both latent and semantic codes, encompassing both semantic content and the subtleties conveyed via non-linguistic cues (Braun & Clarke, 2022). The development of initial thematic constructs was achieved using a process of code review and refinement (Braun & Clarke, 2022). Throughout the analytical process, the authors held regular discussions to increase the credibility and rigor of the analysis (Nowell et al., 2017). The thematic analysis resulted in the following themes: (1) Sharing is caring—motivating and initiating conversations about sexuality and intimacy, (2) Safe spaces—facilitators of sexual and intimate communication, (3) Being overlooked and feeling unheard, and (4) Overprotection and self-blame. Table 1 illustrates the analytical process.
Analytical Process.
Results
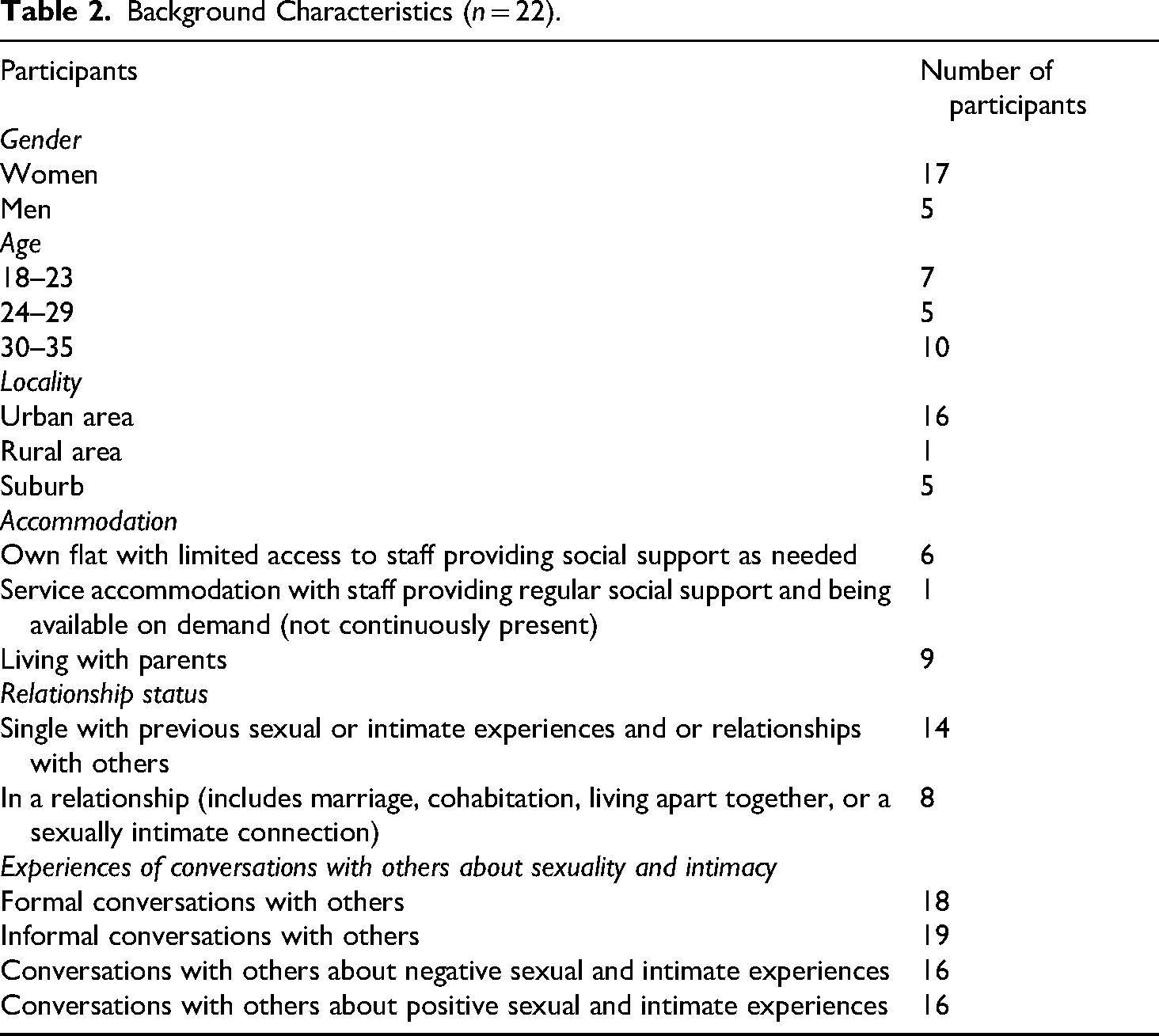
The results are based on the participants’ experiences of having conversations about sexuality and intimacy. Table 2 provides general information about the respondents. To protect the identities of the participants, pseudonyms and approximate ages have been used.
Background Characteristics (n = 22).
Sharing is Caring—Motivating and Initiating Conversations About Sexuality and Intimacy
During the interviews, it became evident that reasons for initiating conversations about sexuality and intimacy differed among the participants. For some, these conversations were driven by a need for sexual knowledge or simply a wish to share personal experiences. For others, they were initiated following experiences of sexual abuse.
The participants described encountering challenges in initiating conversations about sexuality and intimacy. Some struggled with deciding what to disclose, navigating parental concerns, and expressing their emotions verbally, which hindered their ability to initiate such conversations. For some participants, the conversation was initiated to address challenges and misunderstandings that can occur in sexual situations and that are difficult to resolve alone. This can be exemplified by Nellie, aged 30–35, who was living in accommodated housing and was in a long-term relationship: If something goes wrong [unspecified] when I have sex with my boyfriend, I don’t dare to tell him. Then I have to talk to the staff. I tell them that something is wrong. (Nellie) I told my mum after a year or so. After I told my mum, she helped me to break up. So, it ended after a year. I think I was afraid that my parents would be angry if I told them, although my mum later said that she would never be angry if I told them, but it felt like she would be angry with me. She doesn't think you should be doing things like that when you're so young. But it wasn't really like I wanted to do that kind of thing. (Tove)
Sexual concerns influenced the choice of whom to talk to; some participants were cautious, whereas others described initiating conversations to gain knowledge about sexuality and intimacy. John, a young adult aged 18–23, with limited linguistic ability, who wanted to establish an intimate relationship and sought verbal guidance from a male contact person at school, described this: Well, for example, I'll say like this, when I walk past [a girl], I would like to dare to ask. I would dare to go up and say, hello! (John)
For other participants, conversations were grounded in specific sexual interests, which determined who they talked to. Suzi, aged 30–35, provides one example. She was thinking about having children, so she turned to her sister, herself a mother. I have my mum; I have my sisters. I have one sister who has given birth to a daughter, so I can talk to her. Talk about the whole thing. (Suzy)
The participants described various reasons and needs for having conversations about sexuality and intimacy. Some sought advice for their relationships, while others wanted to share their concerns about negative sexual experiences, and some wanted to have conversations about specific intimate topics. This demonstrates that various factors influence their decisions about whom to trust in intimate conversations. For some, factors like gender and the comparative age of participants and their chosen confidants play a crucial role in influencing the depth of their conversations about sexuality and intimacy, and the level of comfort they feel having these conversations. This leads us on to the next theme, which illustrates the way participants reflected on the creation of safe spaces for sexual and intimate communication.
Safe Spaces—Facilitators of Sexual and Intimate Communication
Something that emerged clearly in the interviews was the need for the participants to have safe spaces to facilitate conversations about intimacy and sexuality. This includes both physical aspects of the spaces in question, such as ensuring a private and secure environment, and personal factors, such as the confidant's personality and the participant's trust in the confidant. The importance of these two components in creating a safe space for conversation is underscored by the findings. Feeling safe and that one is taken seriously were identified as important factors for productive sexual conversations by many participants, who described that these could differ depending on whom they had a conversation with.
Many participants described friends as being essential in creating a safe and comfortable environment for conversations, which were not always planned or formal, but integrated into social interactions. Tom, aged 18–23, who generally preferred to speak with his friends about sexuality and intimacy, also described his interactions with staff at his daily activity center, exemplifying that such conversations could also take place with staff members. The familiarity of the setting, where he had attended for several years, contributed to a sense of emotional safety and continuity. As Tom articulated: I can always talk to the staff about anything [sex and relationships]. It doesn’t have to be anything deep, just that I say something. I feel that they respond well. But I don’t talk to everyone. I just talk to my contact person. (Tom) It would be someone I feel safe with. So, it's not something that I would talk about the first time, but if you felt that you had this security with a person, you could have talked about it, then you could have asked how to do it on a date. How do I ask someone if they want to go on a date? What is a good relationship, what is not, and things like that. (Judith)
Many participants described preferring to have a trusting and established relationship with someone with whom they could openly engage in conversations about sexuality and intimacy. Nick, aged 18–23, exemplified this reliance on a specific individual for support and advice. When asked about his preferred confidant, he responded immediately: Nick: Johan [contact person]. Interviewer: Have you talked to him about relationships and sexuality? Nick: Not sexuality, but relationships. Interviewer: What makes you talk to Johan [contact person]? Nick: Because he's the one I know best. I’ve known him since I started here. I’ve been here for three years. (…) He understands me, either by nodding or by saying, ‘I understand you’. Britt: You shouldn't keep it inside. It has to come out properly. Interviewer: And could you talk to Kalle [caregiver]? Britt: It is easier with Kalle [caregiver]. He is special. We have a secret together. If I run out of yogurt, I can take one outside [from the common area]. Interviewer: But you can also talk about important things? Britt: I do. He is a good staff member. I can talk to my stepfather, but not my mother, and I don't know why. It's just my stepdad. He's as calm as can be. He understands me. He listens to me. He senses that my body is shaking and that I’m starting to hyperventilate, so his calm makes me calm. My mother becomes more like a police interrogator. (Eric)
Another perspective on trust that was described by a few of the participants vividly illustrates the profound impact that professional assistance within the support system can have on communication when attempting to share personal experiences. Daisy, aged 30–35, had been in a long-term sexually abusive relationship during high school. It broke her down mentally and led to school withdrawal. Luckily, there had been a phone call: I almost think it was her, uh, the [school] nurse who saved me otherwise, I would have, like, I didn't have anything left inside. She called and asked me where I was. She hadn't seen me for some time. Luckily, he was out shopping and then she called an ambulance in the meantime, and I had the opportunity to get away, to the psych ward. (Daisy) That you are calm and focused, not just sitting down and taking notes, but keeping eye contact. (…) Perhaps explain a bit more to ensure I am in a safe environment. You can also take a little break because then I go into more detail. (Elsa) I visited her [psychologist] every three weeks, and we had brief conversations. She would ask questions about my progress, thoughts, and feelings. She had one of those [visual aids] so I could point to my feelings, if I was feeling good, bad, disappointed, angry, or very sad. She helped me during my most difficult times. (Lina)
Being Overlooked and Feeling Unheard
Interview participants exemplified different challenges they faced when having conversations related to sexuality and intimacy. These difficulties were caused by various factors, such as feeling unheard or experiencing unequal treatment as a result of sexual norms.
Several participants encountered different barriers that hindered their ability to engage in sexual conversations, which could potentially affect their future disclosure decisions. Rosa, aged 30–35, who was living on her own, described sometimes having conversations with her mother or a friend about her sexual experiences and concerns, but revealed that she kept some things to herself. Well, sometimes it goes a little too fast [in a relationship]; I talk to my friend and sometimes to my mother (…). If I feel bad, I don't tell them. I keep everything inside. (Rosa)
Some participants had encountered bureaucratic obstacles that hindered their access to professional support, leading to adverse effects on engaging in meaningful conversations. Gunnel, aged 30–35, had struggled to secure relevant professional assistance to address her intimate experiences, prompting her to rely on her contact person for support. Gunnel expressed her frustration, stating: I want to [talk to someone]. And I've tried, but the health care system won't give it to me, so it feels hopeless. (…). I talk to my support person once a week and she helps me as much as she can. (Gunnel) (…) Every morning when I came there, he stood there, watching and waiting for me as soon as I came inside the door. Then he jumped at me straight away and started [sexual abuse], and when I was about to go home, he followed me out to the car, to dad, and started humping and wanting to get hold of me (…). Dad got angry and got out of the car [and said] “This stops now!” “Enough! I know what you’re up to!” He [the daycare attendant] ran back and cried. Then the staff got angry at me and said I was making it up. (Mona)
Overprotection and Self-Blame
Some participants described experiences of shame when having conversations concerning sexual issues with their parents, which overshadowed the positive aspects of having conversations about sexuality. Many participants lived in overly protective environments in which societal and parental expectations conflicted with their desires and experiences. This led them to feel trapped in a “surveillance bubble.” Participants demonstrated an awareness of the sensitivity of the topic of sexuality by choosing not to disclose information about their sexual experiences to their parents.
In some interviews, it was evident that participants had integrated what they perceived as “appropriate” sexual behavior, readily revealing their use of contraception during sexual encounters when having conversations about sexuality, as in this example from Britt (24–29 years): But then I must use protection. Otherwise, there's a backlash both from here [supported accommodation] and from siblings and my parents. (Britt) We’ve had sex that was protected and sex that wasn't. One time he got in his willie [penis] about nine times. That was the only time we were engaged in [sexual] misconduct [her own word]. We thought it was so nice (laughing) and cozy. It was not strange at all! (Felicia)
In other cases, the participants had chosen to shield their parents from distressing details out of a concern to avoid exacerbating parental distress, particularly details related to experiences of sexual abuse. Lina, aged 24–29, was reluctant to have conversations about her experiences of sexual abuse with her parents. Instead, she chose to confide in a psychologist: I could talk to mum and dad, but not really about this [sexual abuse]. I felt that mum and dad didn't need to know about it. I mean, they knew about it. But talking about it might (…) Dad would get even angrier than he already is, and then I thought it would be better to talk to the psychologist. (Lina) My aunt. She's the only one I can talk to about situations like this. So, I was kind of the first one to tell her that I slept with Fred [boyfriend] and that he took my virginity. Then she said he sounded like a good guy. Then I said he was cool, but I lied about not using a condom. I lied. My mom and aunt are afraid of sexually transmitted diseases, so I had to lie that we had a condom when we didn't even have one. (Lisa)
Discussion
The results show that young adults with intellectual disabilities initiate conversations about sexual and intimate issues with friends, staff members, and professionals (e.g., psychologists and social workers) for various reasons, including curiosity, limited sexual knowledge, and experiences of sexual trauma. The decision-making process regarding whom to engage in conversations with is aligned with the situational level (Plummer, 1995), wherein young adults with intellectual disabilities construct their social identity differently in a range of different contexts. The findings in our study underscore the necessity of creating supportive environments in which individuals with intellectual disabilities feel secure and acknowledged, thereby facilitating conversations regarding sexuality and intimacy. This aligns with previous international research by McCarthy et al. (2022) and Schaafsma et al. (2017), which emphasizes the importance of safe spaces for such conversations. Similarly, Swedish findings by Olin and Ringby Jansson (2008) highlight how the physical structure and social atmosphere of communal spaces in group homes shape residents’ opportunities for social engagement. Participants in this study echoed these sentiments, particularly noting the significance of engaging with non-judgmental staff members to foster an environment conducive to dialogue. While McCarthy et al. (2022) identified specific staff members as sources of safety, this study expands on this finding by illuminating conditions in accommodation settings that may promote conversations about sexuality. Notably, several participants expressed a preference for nocturnal conversations, citing increased accessibility and confidentiality because of a reduced staff presence during these hours. This underscores the role of timing and context in facilitating these conversations. This finding extends existing international research, which has primarily focused on personal chemistry (Black & Kammes, 2019; Frawley & Wilson, 2016). The findings from the present study resonate with the organizational and situational context (Plummer, 1995), including aspects such as time, space, and interpersonal dynamics. These aspects shape opportunities for individuals to express and make sense of their sexual experiences. For example, nighttime settings appeared to foster openness and intimacy, supporting conversations about sexuality and intimacy among young adults with intellectual disabilities. In addition, the study reveals how societal attitudes significantly impact young adults with intellectual disabilities in their intimate relationships. These restrictive norms can impede their ability to develop and exercise sexual consent, as noted in another Swedish study (Hart et al., 2024). The present study underscores the necessity for sensitivity, respect, and empowerment to ensure their well-being and autonomy. While previous research (Foley, 2018; Gil-Llario et al., 2018) has identified barriers to discussing sexuality with family and support systems, this study provides new insights into participants’ hesitancy and deliberate withholding of information. Some individuals expressed a reluctance to share their sexual experiences and concerns, fearing negative repercussions on their freedom and living situation. This finding reinforces the notion that societal attitudes can create a climate of fear and silence around sexual topics (Bahner et al., 2024). Furthermore, participants also faced challenges in having conversations about sexuality because of conflicting societal and parental expectations, which led to a sense of being caught in a “surveillance bubble.” The results show that participants exhibited caution in sharing their sexual experiences, often internalizing perceived norms of “appropriate” sexual behavior. The reluctance to disclose details, particularly regarding contraception, reflects a historical neglect and societal biases in sexual communication (Löfgren-Mårtenson, 2020). At the organizational level (Plummer, 1995), this underscores inadequacies within the organizational structure that have the potential to influence the confidence and willingness of young adults with intellectual disabilities to disclose such incidents in the future. These various difficulties can be attributed to power dynamics, as described by Plummer (1995), which underscore the intricate relationship between disclosing information and ensuring safety in familial contexts. Young adults with intellectual disabilities often navigate societal norms in their conversations about sexuality, adhering to specific frameworks (Ferrante & Oak, 2020). Rojas et al. (2016) argued that societal and parental overprotection can hinder individuals’ growth and autonomy, fostering vulnerability and a fear of judgment. The current study corroborates this perspective, illustrating how families can either support or impede these individuals’ ability to engage in open conversations. As previously established by Rojas et al. (2016) and Rushbrooke et al. (2014), the study also shows that an unacknowledged silence within families acts as a barrier, hindering participants from disclosing their sexual experiences and concerns. This silence reinforces misconceptions about the sexuality of young adults with intellectual disabilities, contributing to their sexual marginalization. Plummer's (1995) cultural and historical levels show how societal expectations influence sexual behavior among young adults with intellectual disabilities. These expectations include being heterosexual, practicing safe sex, and modesty. Societal norms and beliefs shape personal narratives, e.g., through the stigma associated with premarital sex. At the personal level, young adults interpret and negotiate societal expectations in light of their own desires, values, and lived experiences. This process illustrates the balance between transparency and protection within family relationships, a balance that may also be relevant in social work practice (Maguire et al., 2019).The stereotyping of young adults with intellectual disabilities as inherently sexually vulnerable perpetuates harmful narratives and impedes open and honest conversations about sexuality (Bahner et al., 2024), which in turn limits how social workers engage with issues of sexuality in practice (Goulden, 2021). It is therefore essential to consider varying levels of support within the target group's networks and link them to Plummer's (1995) different levels of producing and consuming sexual stories, particularly the organizational level in relation to supporting minority groups such as young adults with intellectual disabilities.
Limitations and Strengths of the Study
Some limitations associated with the study should be acknowledged. Firstly, challenges involving gatekeepers produced barriers to accessing participants, which prevented us from briefing potential participants prior to the interview as intended. While this introduces a possible risk of sampling bias, since gatekeepers may have influenced which individuals were approached or felt encouraged to participate, the first author successfully conducted 22 interviews, yielding substantial empirical data, which underscores the willingness of participants to share their experiences. Nevertheless, it is important to consider that the sample might differ, since participants were informed about the study by gatekeepers and may have different perspectives compared to those who were not informed. For future studies involving the same demographic, it is important to explore alternative strategies to circumvent gatekeeper barriers. It is also noteworthy that the study had a gender imbalance, with 17 of 22 participants being women, while only 5 were men. The overrepresentation of women in qualitative research on sexuality may be due to several factors. These include the researcher's gender, the dynamics inherent in face-to-face interviews, and the dissemination of information by the organizations contacted. It is important to note that this does not mean that men's sexual experiences have been neglected. However, subsequent studies should actively attempt to achieve gender balance.
Implications for Practice
The findings of the study highlight the necessity of a supportive network structure to facilitate safe dialogues about sexuality for individuals with intellectual disabilities. Social workers have a critical responsibility to create environments that encourage these conversations, which are essential to promoting sexual health and well-being. To enhance sexual support, professionals in social work and day activity centers should implement several key strategies. First, fostering conversations about sexuality and intimacy within support networks is vital (Dodd, 2020; Maguire et al., 2019). This can be achieved by establishing safe spaces that promote trust and reduce stigma (Bahner et al., 2024; Löfgren-Mårtenson, 2020). In addition, creating both formal and informal support networks will provide individuals with essential resources and emotional support (McCarthy et al., 2022). The use of podcasts, featuring young adults with intellectual disabilities, offers an innovative platform for participation, allowing individuals to share their experiences and perspectives on sexuality in a safe, structured format (Poddgruppen, 2023). Furthermore, the PLISSIT model (Annon, 1976) offers a practical framework for social workers (Bahner & Lukkerz, 2023), allowing them to provide varying levels of support based on individual needs around sexuality. The first levels, Permission and Limited Information, are especially relevant in everyday social work. They do not require specialist knowledge in sexual health but instead focus on creating a safe and open space for conversation and on providing simple and appropriate information when needed. Some social workers with additional training may have the competence to work on the Specific Suggestion as well as the Intensive Therapy level (Annon, 1976). Integrating the PLISSIT model into practice can help social workers effectively address the complexities of sexuality in their work with young adults with intellectual disabilities (Bahner & Lukkerz, 2023).
Footnotes
Acknowledgements
We would like to thank all the participants who generously contributed their experiences of conversations about sexuality and intimacy in this study.
Ethical Approval
Specific ethical considerations have been taken in all phases of this study, since individuals with intellectual disability are considered a vulnerable group and the topic of individual sexuality is sensitive. Ethical approval (reference number 2021-04974) for this project was given by the Swedish Ethical Review Authority prior to recruitment and data collection.
Consent to Participate
All participants provided full consent after receiving project information and answering control questions to confirm their understanding and voluntary participation. Written informed consent was obtained from some, while others gave verbal consent, documented via audio recording.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Research Council for Health, Working Life and Welfare (Forte).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.