
Abstract
Summary
This article presents a review and map of program theories used in mental health and well-being interventions tested with care-experienced children and young people (foster care, kinship care, residential care). Program theories are important in knowing how interventions should bring about change, how they might be implemented, and how they will be influenced by contextual factors. Currently, we do not fully understand if and how interventions are using program theories. We synthesized the international evidence base for interventions targeting subjective well-being, mental health, and suicide-related outcomes among care-experienced individuals aged ≤ 25 years. We identified interventions’ theories of change, implementation theories, and context theories. Study reports were retrieved through 16 electronic databases and 22 websites, expert recommendations, citation tracking, and screening of systematic reviews. We charted interventions and their associated theories, constructing narrative, and visual summaries. We further conducted stakeholder consultations to identify which theories should be prioritized in the UK.
Findings
The review identified 13 interventions, with 24 study reports. Most interventions primarily drew on interpersonal theories of change (n = 12), notably Attachment, Positive Youth Development, and Social Learning Theory. These targeted mental health, behavioral, or neurodevelopmental disorders, with minimal focus on well-being or suicide-related outcomes. Reports were limited by a lack of theoretical clarity and coherency, scare implementation and context theories, and minimal stakeholder involvement in theory development.
Applications
Future interventions need to explicitly articulate their program theory. Stakeholders suggested drawing on theories that will help interventions strengthen relationships and bring about structural change.
Introduction
Care-experienced children and young people can include those who have resided in foster care, kinship care, and residential care or have had parental rights legally transferred to another adult. They report a higher prevalence rate of poor mental health and well-being compared to non-care-experienced populations (Bronsard et al., 2016; Engler et al., 2022; Ford et al., 2018; Long et al., 2017) and are nearly five times as likely to have at least one psychiatric diagnosis (Ford et al., 2018). They are more than four times as likely to attempt suicide than the general population (Evans et al., 2017). Individuals who report prior care experience have excess mortality in adulthood, attributable to the non-natural causes of self-harm, accidents, and other mental health and behavioral risks (Murray et al., 2020).
There has been an expansion in the number of mental health interventions tested with this population, with a parallel growth in evidence syntheses (Barnett et al., 2019; Bergström et al., 2019; Everson-Hock et al., 2012; Greeson et al., 2020; Hambrick et al., 2016; Kerr & Cossar, 2014; Luke et al., 2014; Marsh, 2017; National Insitute for Health and Care Excellence, 2021; National Institute for Health and Care Excellence, 2021; Solomon et al., 2017; Sullivan & Simonson, 2016). Programs can range from targeted approaches to universal interventions that consider care-experienced individuals as a population sub-group. They can operate across different socio-ecological domains, from the individual to the societal level. However, despite progress in the evidence base, there is limited understanding of how these interventions actually work to bring about intended change.
Methodological guidance and empirical case studies on intervention development foreground the importance of having a clearly articulated program theory explaining how it functions (Fraser et al., 2009; Maden et al., 2017; Moore et al., 2021; Moore & Evans, 2017; O'Cathain et al., 2019; Prestwich et al., 2014; Skivington et al., 2021; Thomas & Rothman, 2013). This can include a theory of the causal mechanism through which outcomes are reached, a theory of implementation describing how the causal mechanisms are activated through intervention delivery, and a theory of how mechanisms interact with and are influenced by wider context factors. Without such a clear, logical, and contextually sensitive theory, intervention effectiveness can become reliant on serendipity. An inability to describe intervention functioning can also make it difficult to replicate or scale-up an effective approach or deliver it in new contexts.
To date, we are not aware of any existing evidence syntheses of mental health interventions tested with care-experienced populations that explore if program theories are explicitly used and to what extent. As such we drew upon principles and methods linked to scoping reviews to construct a theory map describing the theories that are currently being emloyed (Arksey & O'Malley, 2005; Levac et al., 2010). In identifying these theories, the map provides a useful tool in demonstrating the limitations of current approaches to intervention development and description and where further work is needed. To note, while we did not set out to conduct a theory synthesis, which would have associated methods to support the development of a composite theory (Bonell et al., 2015; Pound & Campbell, 2015; Tancred et al., 2018), this may serve as a relevant next phase of study.
CHIMES systematic review
The present study was undertaken as part of a larger mixed-method systematic review, the care-experienced children and young people's Interventions to improve Mental health and well-being outcomes systematic review (CHIMES) (Evans, Macdonald, Trubey, Noyes, et al., 2024). The overarching review aimed to synthesize international evidence on interventions to understand what approaches are effective, how they are delivered in different social care systems, whether they mitigate or exacerbate inequities, and if they are cost-effective (Evans et al., 2021; Evans, Macdonald, Trubey, Melendez-Torres, et al., 2024).
The CHIMES review comprised three phases. First was the construction of an evidence map, which charted the interventions to identify the clusters and gaps in the existing evidence base (Evans et al., 2023). Second was method-level syntheses: meta-analysis of outcome evaluations using randomized-controlled trials and quasi-experimental design studies (Trubey et al., 2024); thematic synthesis of implementation and acceptability evaluations (MacDonald et al., 2024); narrative synthesis of inequities in intervention outcomes (Evans, Trubey, et al., 2024); and narrative synthesis of economic evaluations. Third was stakeholder consultation to reflect on the review findings and identify interventions for future development, evaluation, and implementation in the UK.
In this article, we report findings from Phase 1 and Phase 3. As part of Phase 1, we charted interventions’ program theories. We addressed the following research question: What are the theories tested in mental health and well-being interventions for care-experienced children and young people?
For the purpose of the review, we adopted an inclusive approach to program theory, considering theories of change, theories of implementation, and theories of context (Maden et al., 2017). The underpinning theory of change explains the hypothesized causal processes or mechanisms that link intervention components to outcomes. Theories of implementation explain how the intervention will deliver the change mechanisms, although this should probably be differentiated from an implementation strategy, which pragmatically describes intended delivery. With the expansion of complex systems perspectives in intervention development and evaluation, there is also an increased emphasis on context theories, which seek to understand features of the context, and theorize how these features are expected to interact with mechanisms, and be influenced by them in return (Skivington et al., 2021).
As part of Phase 3, we asked stakeholders to discuss the program theories identified by the review. We invited stakeholders to consider which theories should be prioritized for delivery moving forward based on perceived effectiveness, feasibility, and acceptability. Alternatively, if no theories were deemed suitable, which novel approaches should be considered. Following the presentation of our theory map, our article reflects upon the program theories that stakeholders would like to see in the future.
Methods
We report the methodology of the CHIMES review in the protocol (Evans et al., 2021) and the PROSPERO registry of systematic reviews (CRD42020177478). As reporting guidelines are not developed for theory maps, the present methods are presented with reference to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Reviews (PRISMA-ScR) (Tricco et al., 2018) and the Cochrane reporting guidelines for qualitative, implementation, and process evaluation evidence syntheses (Flemming et al., 2018).
The methods section first describes the process of study retrieval, data extraction, quality appraisal, and stakeholder engagement for the overarching CHIMES review, while providing more specific detail on processes related to studies reporting program theories where relevant. It then outlines how the extracted data on program theory were integrated with stakeholder priorities.
Eligibility criteria
We defined the parameters of the review in accordance with the Population, Intervention, Comparator, Outcome, and Study Design (PICOS) framework:
Population
The target intervention population could be care-experienced children and young people (≤25 years old) or the individuals, organizations, and communities that might impact them. We defined care as formal kinship care, foster care, residential care, or statutory transfer of parental responsibility to another adult. The amount of time in care was not restricted. We excluded the following populations: general population, children and young people in need (i.e., defined by Section 17 Children Act 1989, whereby an individual requires Local Authority provision to achieve reasonable health and development, or they experience impairment or disability), individuals at the edge of care (i.e., at risk of needing care but can currently be supported to stay with family), care without statutory involvement (e.g., informal kinship care), adoption, or unaccompanied asylum seekers and refugees.
Intervention
We defined interventions as a system disruption, which we understood as any activity intended to redirect the course of action(s) in a social system (Hawe et al., 2009). They could be mono-component or multi-component and operate across one or multiple socio-ecological domains: intrapersonal, interpersonal, organizational, community, and policy. Interventions could be targeted at care-experienced individuals specifically or could be universal but tested with this population group. We did not specify a priori criteria for delivery (i.e., delivery agent, delivery mode, and delivery setting). We excluded the following intervention type: pharmacological.
Comparator
For outcomes evaluations, a comparator had to be specified and could include treatment as usual, other active treatment, or no specified treatment.
Outcomes
We defined three domains of primary outcomes: subjective well-being (inclusive of life satisfaction, quality of life, and well-being); mental, behavioral, or neurodevelopmental disorders as specified by the International Classification of Disease-11; and suicide-related outcomes (inclusive of self-harm, suicidal ideation, and suicide). We excluded the following outcomes: substance misuse, euthanasia or assisted suicide, accidental death, and biomedical markers of mental health problems (e.g., cortisol level).
Study design
For program theory reports, there had to be a description of the theory of change, implementation theory, or context theory. Study reports could draw upon established grand or mid-range theories to support the articulation of the intervention's theoretical basis, but theories could also be developed inductively. Theories could be described narratively, presented in a logic model, and/or tested through mediator analysis. Moderator analysis could be relevant in understanding how the theory worked for different populations in different contexts. All forms of presentation were eligible, and empirical testing was not mandatory. To be included, a theory report had to have a linked outcome evaluation in the CHIMES review as we were interested in establishing which theories contributed to effective, ineffective, or potentially harmful approaches. The theory description and outcome evaluation could be published in separate study reports. We excluded reports that described intervention components without explanation of how they would enact change.
Search strategy and study retrieval
We developed a search strategy in Ovid MEDLINE before adapting it to the functionality of each database (Supplement A). Study reports were identified from 16 electronic bibliographic databases: Applied Social Sciences Index and Abstracts; British Education Index; Child Development & Adolescent Studies; CINAHL; Embase; Education Resources Information Center; Cochrane Central Register of Controlled Trials; Cochrane Database of Systematic Reviews; Health Management Information Consortium; International Bibliography of the Social Sciences; Medline; PsycINFO; Scopus; Social Policy & Practice; Sociological Abstracts; and Web of Science. We searched the websites of 22 relevant social and health care organizations. We conducted searches between May and June 2020, before updating them from April to May 2022. We contacted 32 subject experts and 17 governmental and charity organizations for recommendations, particularly regarding gray literature and in-progress studies. We screened relevant systematic reviews and undertook forward and backward citation tracking with included study reports. Searches were conducted in databases from 1990, in accordance with the ratification of the United Nations Convention on the Rights of the Child (UNICEF, 1989), which marked an expansion in children's social care provision internationally. Searches were not restricted by language.
Data management and study selection
We exported retrieved study reports to EndNote for deduplication and then imported them to the Evidence for Policy and Practice Information and Co-ordinating Centre's review software (EPPI Reviewer version 4.0) for storage and management. Study titles were screened for clearly irrelevant retrievals by one reviewer, with irrelevant reports checked by a second. Title and abstracts were screened independently and in duplicate by two reviewers. Where there was a conflict in decision or insufficient information, the study report progressed to the next stage of screening. Full texts were screened independently and in duplicate with conflicts resolved through discussion or recourse to a third reviewer. We made eligibility assessments with a screening form, which was tested and calibrated with a subset of reports.
Data extraction
We coded all eligible study reports according to country, publication date, intervention type, target population, intervention name, intervention characteristics, evidence type, study design, and intervention outcome domains. Intervention characteristics were coded in accordance with the Template for Intervention Description and Replication Checklist for Intervention Development (van Vliet et al., 2016). For program theory, we developed and calibrated a data coding tool for extraction with relevant study reports. Extracted items were processes for theory development, name of theory, socio-ecological domain of theory, type of theory (e.g., implementation or context), discipline of theory, description of theory, presentation of a logic model, and if the theory was empirically tested (e.g., mediation analysis). All extracted items were qualitative. Two reviewers independently extracted and coded data for 10% of reports, discussing discrepancies. The remainder were extracted by one reviewer and checked by a second.
Quality appraisal and risk of bias
We appraised theory study reports using a tailored appraisal tool developed for a previous theory synthesis (Tancred et al., 2019). While the theory map focused on charting theories, we felt that appraisal was useful in assessing the quality of current practice and identifying how the development and evaluation of theory-driven intervention may progress moving forward. Domains of assessment were clarity, plausibility and feasibility, testability, ownership (e.g., developed with target populations), and generalizability. We modified the original appraisal tool to meet the needs of the CHIMES review by including two ownership domains (one for children and young people and one for other stakeholders), whereas the original version included just one. This was due to our awareness that current research and practice tend not to foreground the voices of care-experienced children and young people. As such, we wanted to have an explicit assessment of the extent to which this stakeholder group was engaged in the development of program theory. Two reviewers appraised study reports independently and in duplicate. Domains were rated according to a binary assessment of yes or no. The percentage for each reviewer was calculated as the proportion of domains rated as yes.
Stakeholder consultation
Following the conduct of the review, we undertook seven consultations to consider if the interventions, and associated theories, that have been evaluated to date align with intervention priorities in the UK context. Stakeholders were identified as being potential funders, delivery agents, or target participants in a possible future intervention.
Two consultations were held with care-experienced young people (n = 8 participants). Young people were drawn from CASCADE Voices and The Fostering Network in Wales Young Person Forum. Recruitment to these consultations was challenging, reflecting reported barriers to engagement with this group during the COVID-19 pandemic (Roberts et al., 2021). One consultation was held with foster carers from the Wales Foster Carer Advisory Forum facilitated by The Fostering Network in Wales (n = 7 participants). Four consultations were held with social care and health professionals working in the area: Public Health Wales NHS National Safeguarding Network, Welsh Government Social Services and Integration Directorate, Welsh Medical Group Fostering and Adoption Special Interest Group, and Public Health Wales Looked-After Children Steering Group. Rates of attendance were high due to consultations often being embedded in professional network events (n = 47).
We conducted consultations between April and September 2022. They lasted between 30 and 90 min. Each consultation commenced with a 15- to 30-min PowerPoint presentation by the CHIMES review team. This presentation provided an overview of the types of interventions and theories included in the review, alongside their effectiveness and context of implementation. Stakeholders were asked to consider which interventions, and program theories, they would prioritize for delivery in the UK based on perceived effectiveness, feasibility, and acceptability. We generated summaries of the key themes explored by each group.
Theory map and integration with stakeholder priorities
We constructed narrative summaries of the qualitative extractions describing program theories, with accompanying tables presenting each intervention and their theoretical basis. We organized these according to the primary socio-ecological domain in which they operated. We further clustered theories according to the different types identified: theory of change, implementation theories, and context theories. We described stakeholder program theory priorities with a narrative summary. Subsequently, we constructed an infographic to map the intervention components, theories, and outcomes included in study reports against the theories identified as priorities by stakeholders, to understand if the current evidence base is meeting their needs. While the thoery mapping process did cover the additional outcomes targeted in the existing evidence base (e.g., those beyond the well-being, mental health, and suicide-related outcomes a priori specified by the review scope), these were not systematically considered in the stakeholder consultations and so are not explicitly addressed in the infographic. The process of mapping results was conducted by a subset of the review team (SM, RT, RE, and SV) and then confirmed by the wider team.
Results
Overview of study reports and intervention characteristics
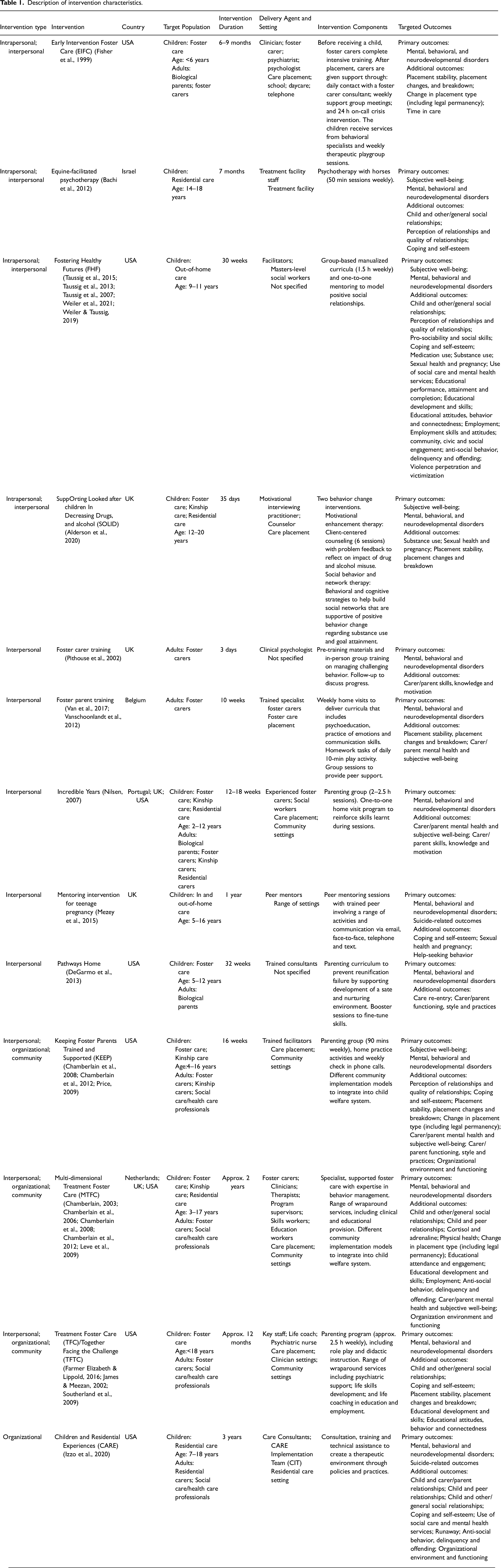
The PRISMA flow diagram for study report retrieval is presented in Figure 1. In total, 64 interventions, with 124 study reports, were eligible for inclusion in the overarching CHIMES review. Of these, 13 interventions linked to 24 study reports presented a program theory (Table 1). They were published between 1999 and 2021. Reports were from the USA (n = 18), the UK (n = 3), Belgium (n = 2), and Israel (n = 1).
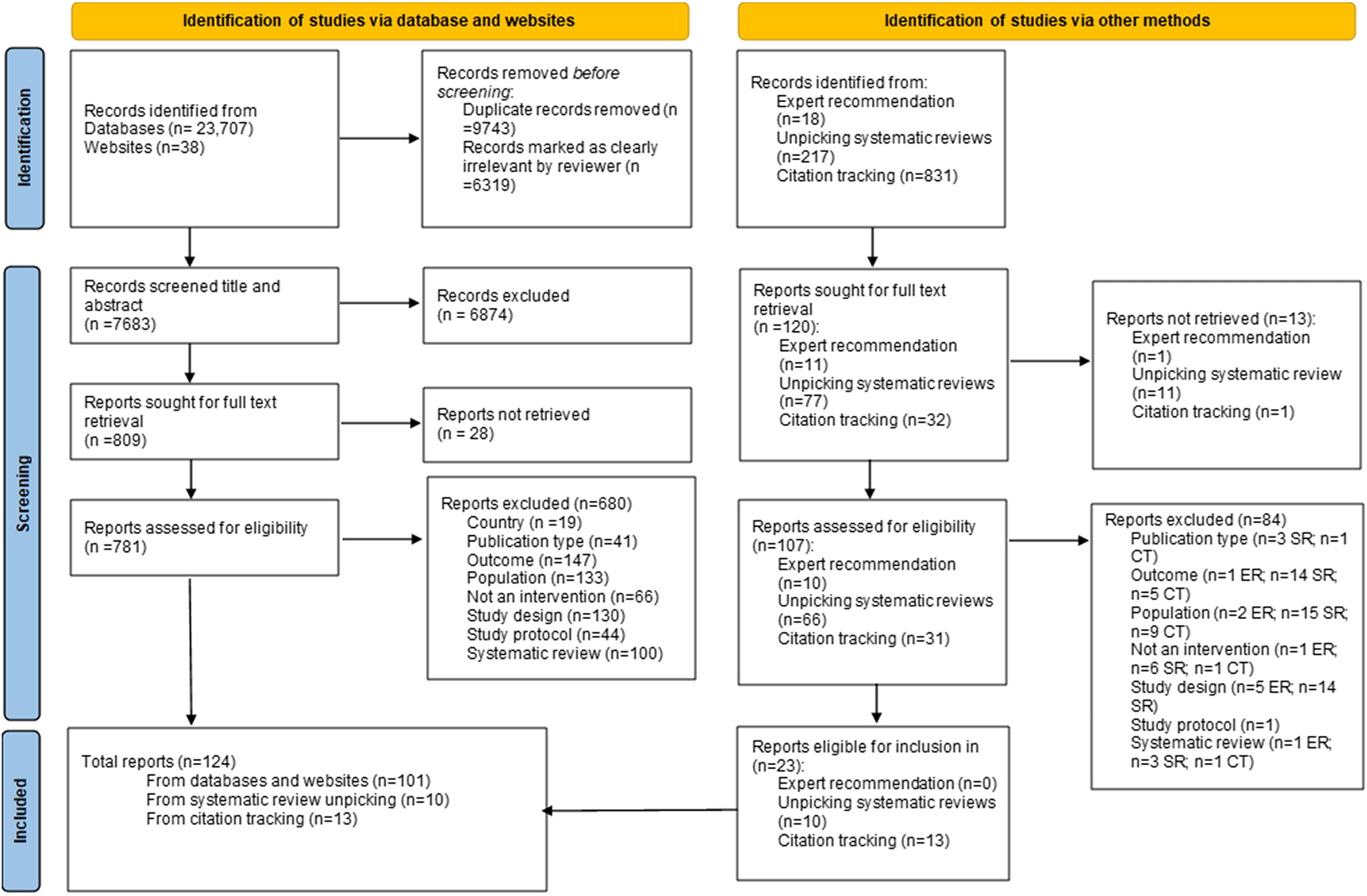
PRISMA flow diagram of study retrieval.
Description of intervention characteristics.
All 24 study reports included a narrative description of a theory or theories. Seven presented a logic model or similar conceptual map (Alderson et al., 2020; Izzo et al., 2020; James & Meezan, 2002; Leve et al., 2009; Mezey et al., 2015; Taussig et al., 2015; Van et al., 2017). Four provided mediator analysis (Chamberlain et al., 2008; DeGarmo et al., 2013; Farmer Elizabeth & Lippold, 2016; Nilsen, 2007) and six reported moderation or interaction effects that helped to understand how intervention mechanisms worked differentially for different populations (DeGarmo et al., 2013; Farmer Elizabeth & Lippold, 2016; Southerland et al., 2009; Taussig et al., 2013; Weiler et al., 2021; Weiler & Taussig, 2019).
We classified the 13 interventions according to the primary socio-ecological domain or domains across which they operated: intrapersonal, interpersonal, organizational, community, and policy (Table 1).
Four interventions operated across the intrapersonal and interpersonal domains. Early Intervention Foster Care (EIFC) provided parenting coaching and group support to foster carers alongside behavioral specialist services and weekly therapy playgroup sessions for children (Fisher et al., 1999). Equine-facilitated psychotherapy (EEP) provided 7 months of weekly equine sessions with young people in residential care, building a therapeutic alliance, developing adaptability, and providing a healing experience (Bachi et al., 2012). Fostering Healthy Futures delivered 30 weeks of group-based curricula and mentoring for children and young people in out-of-home care (Taussig et al., 2015; Taussig et al., 2013; Taussig et al., 2007; Weiler et al., 2021; Weiler & Taussig, 2019). Supporting Looked after children In Decreasing Drugs and alcohol (SOLID) provided six sessions of two interventions to prevent and reduce drug and alcohol use: motivational enhancement therapy delivered client-centered counseling to reflect on the impact of substance use and behavioral and cognitive strategies developed social networks to encourage positive behavior change (Alderson et al., 2020).
Five interventions targeted the interpersonal domain. Two were focused on providing training curricula and support to foster carers to develop their behavioral management practices (Pithouse et al., 2002; Van et al., 2017; Vanschoonlandt et al., 2012). Incredible Years provided a trauma-informed group parenting program to biological, foster, kinship, and residential carers to support positive parenting and engagement in child-serving systems (Nilsen, 2007). Pathways Home sought to prevent reunification failure, offering parenting curricula and booster sessions to biological parents to ensure a safe and nurturing environment (DeGarmo et al., 2013). One intervention offered a peer mentoring program for girls at risk of pregnancy, with mentors engaging mentees in a range of face-to-face meetings and activities, email, telephone conversations, and texts over the course of a year (Mezey et al., 2015).
One intervention operated at the organizational level. Children and Residential Experiences (CARE) provided consultation, coaching, and technical assistance in residential placement settings to create therapeutically informed policies and practices (Izzo et al., 2020).
Three interventions targeted the interpersonal, organizational, and community level. Multi-dimensional Treatment Foster Care (MTFC), Keeping Foster Parents Trained and Supported (KEEP), and Treatment Foster Care (TFC) are derived from the same approach and principles. MTFC focused on placing young people in specialist, supervised foster care placements with expertise in positive behavioral management (Chamberlain, 2003; Chamberlain et al., 2006, 2012; Leve et al., 2009). Meanwhile, KEEP utilized components of MTFC for delivery with “regular” foster and kinship carers, with weekly training and support meetings, and twice weekly calls with a MTFC para-professional (Chamberlain et al., 2008, 2012). For both MTFC and KEEP, additional delivery models were tested, such as train the trainer, to optimize implementation and integrate the intervention into the wider social care system. TFC was a parenting program incorporated into a suite of wraparound services (Farmer Elizabeth & Lippold, 2016; James & Meezan, 2002).
Quality appraisal of study reports
The quality appraisal assessment is presented in Table 2. We assessed each study report on a case-by-case basis. Reports linked to the same intervention could have a different quality assessment across the same quality domain.
Quality appraisal of study reports.
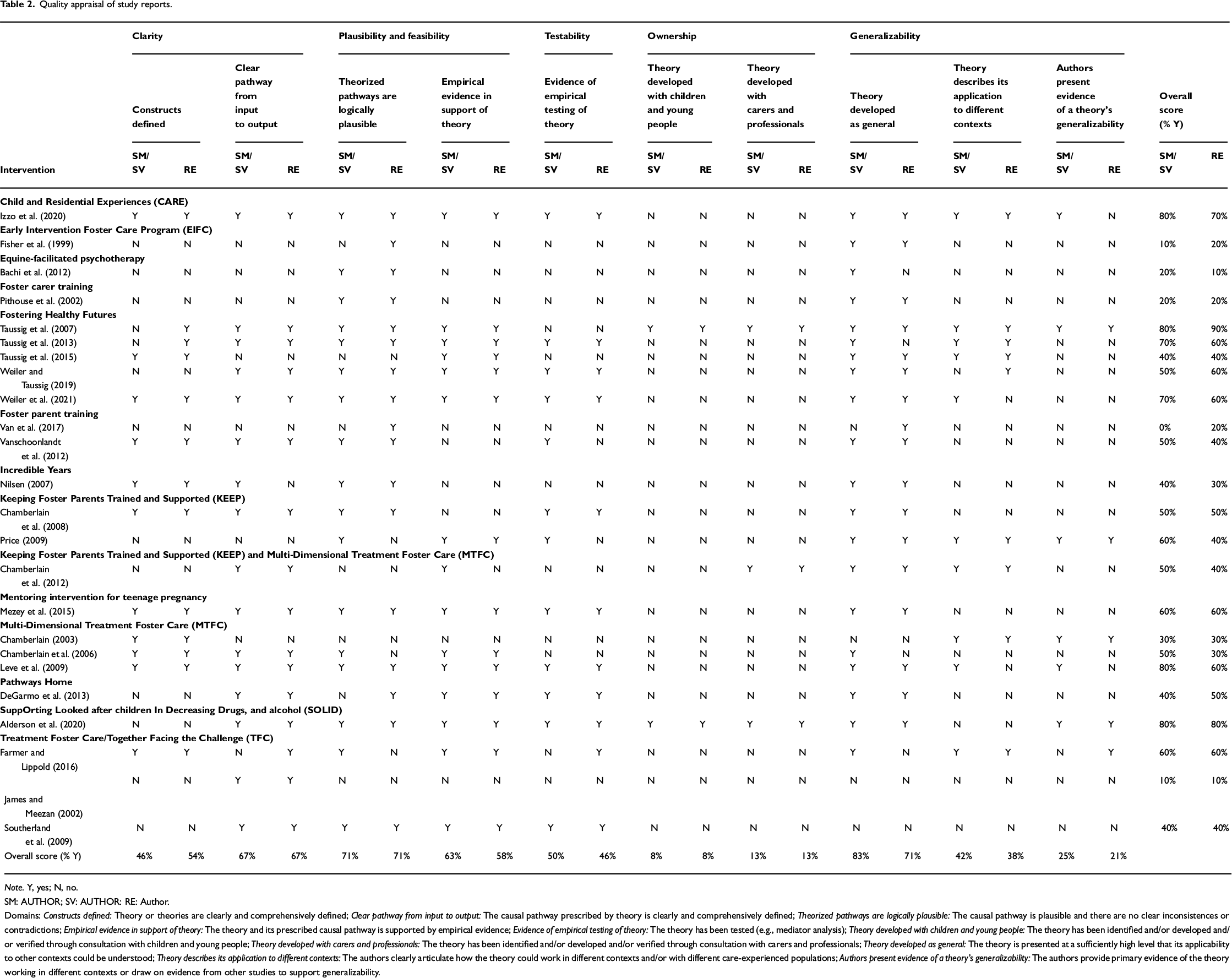
Note. Y, yes; N, no.
SM: AUTHOR; SV: AUTHOR: RE: Author.
Domains: Constructs defined: Theory or theories are clearly and comprehensively defined; Clear pathway from input to output: The causal pathway prescribed by theory is clearly and comprehensively defined; Theorized pathways are logically plausible: The causal pathway is plausible and there are no clear inconsistences or contradictions; Empirical evidence in support of theory: The theory and its prescribed causal pathway is supported by empirical evidence; Evidence of empirical testing of theory: The theory has been tested (e.g., mediator analysis); Theory developed with children and young people: The theory has been identified and/or developed and/or verified through consultation with children and young people; Theory developed with carers and professionals: The theory has been identified and/or developed and/or verified through consultation with carers and professionals; Theory developed as general: The theory is presented at a sufficiently high level that its applicability to other contexts could be understood; Theory describes its application to different contexts: The authors clearly articulate how the theory could work in different contexts and/or with different care-experienced populations; Authors present evidence of a theory's generalizability: The authors provide primary evidence of the theory working in different contexts or draw on evidence from other studies to support generalizability.
We identified two central limitations with study reports. First, there was a lack of involvement or engagement with children and young people, parents and carers, and professional stakeholders, in the development of the theoretical basis of interventions, which reflects widely reported limitations in the development of social care innovation (Müller & Pihl-Thingvad, 2019). Only two interventions indicated explicit involvement of care-experienced individuals (Alderson et al., 2020; Taussig et al., 2007).
Second, there was a lack of theoretical clarity and coherency. Reports often provided extensive description of middle-range theories commonly employed across social work and public health (e.g., Positive Youth Development) but did not always integrate them into a comprehensive and reasoned explanation of how an intervention would bring about intended changes. Specifically, study reports tended to describe theories in the background section, with the description of interventions centering on components and implementation strategies. As such, there was a lack of clear linkage between components, theory, and outcomes. Furthermore, there was a general absence of logic models or other diagrammatic representations. Additional limitations identified were a lack of consideration of the generalizability of the theory to other contexts, combined with a lack of testing of the theory.
Map of program theories
We charted program theories in terms of the socio-ecological domain in which they operated: intrapersonal, interpersonal, and organization and community (Table 3; Figure 2). There were no policy-level theories. There was a predominant focus on the theory of change. However, a small number of interventions, primarily operating across the organizational and community domains, also specified implementation and context theories.
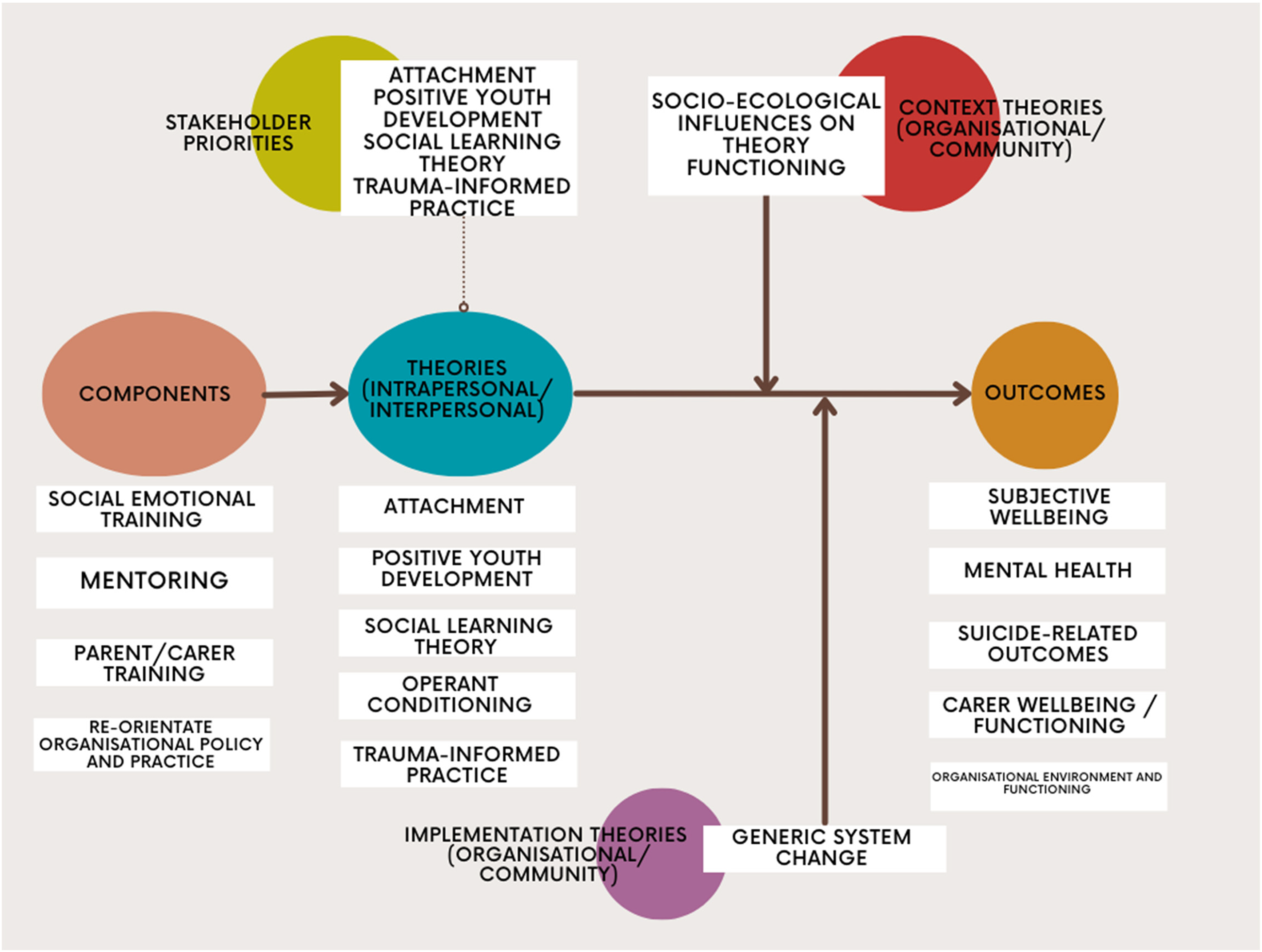
Map of intervention components, theories, outcomes, and stakeholder priorities
Description of program theories.
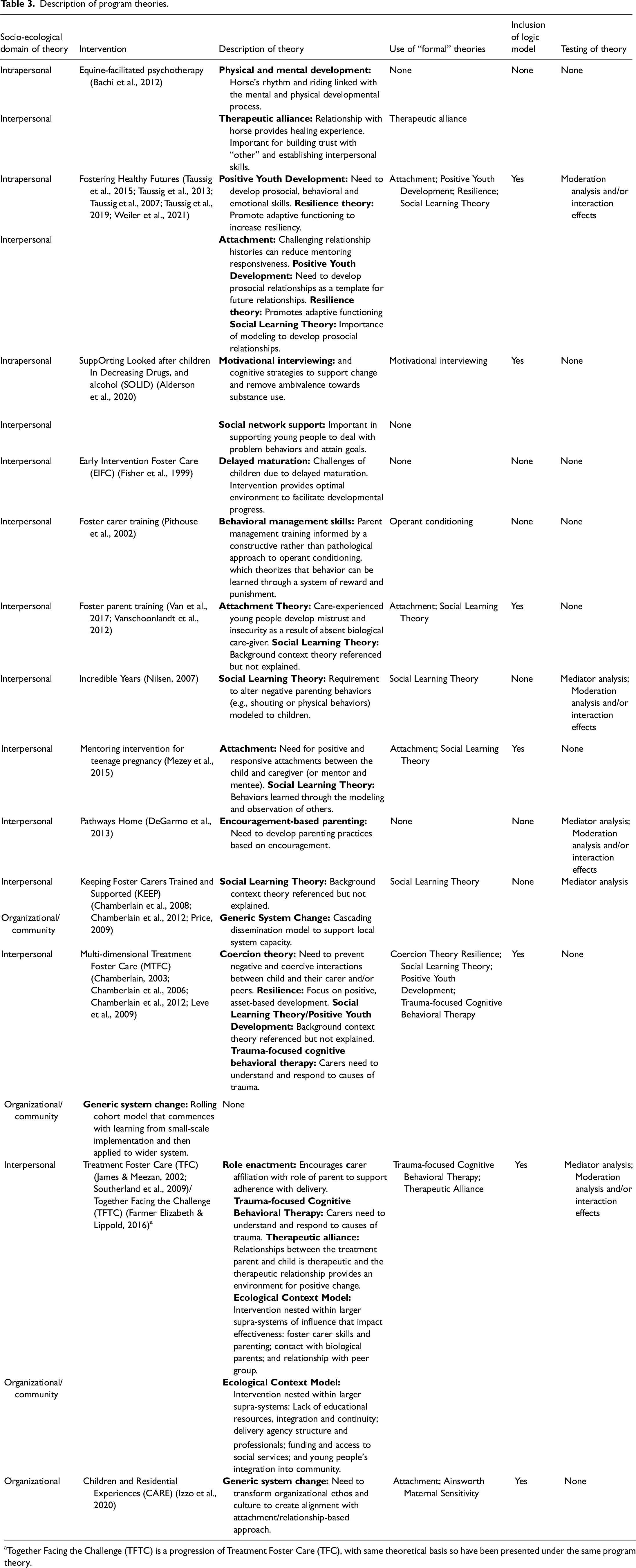
Together Facing the Challenge (TFTC) is a progression of Treatment Foster Care (TFC), with same theoretical basis so have been presented under the same program theory.
Intrapersonal: children and young peoples’ skills, knowledge, and resilience
Three interventions, with five associated study reports, included theories of change linked to transforming the skills, knowledge and resilience of care-experienced children and young people. Fostering Healthy Futures included a skills-building curriculum informed by Positive Youth Development (Waid & Uhrich, 2020), encouraging young people to develop emotional and behavioral regulation and a positive sense of self so that they may enter into prosocial relationships that support their well-being (Taussig et al., 2015; Taussig et al., 2007; Weiler et al., 2021). The intervention further referenced resilience theory, with the need to practice adaptive functioning to ensure resilience to challenging life events.
The SOLID intervention, which targeted alcohol and substance use, employed motivational interviewing to engage care-experienced young people in behavioral and cognitive strategies intended to remove ambivalence about the risk of substance use behaviors and orientate them to positive action (Alderson et al., 2020). Equine-facilitated psychotherapy, while less explicit in its theoretical basis, hypothesized that young people's exposure to a horse's rhythms and riding could encourage their own mental and physical development (Bachi et al., 2012). While EIFC had intervention components that targeted children and young people directly, we did not consider these to have an associated theoretical basis (Fisher et al., 1999).
Interpersonal: positive relationships with parents, carers, and key figures
Twelve interventions, with 23 study reports, included an interpersonal theory of change. These were linked to three sets of causal mechanisms. First, three interventions focused on developing a therapeutic context that was supportive of personal growth. Equine-facilitated psychotherapy centered on building a therapeutic alliance, whereby care-experienced young people created a trusting relationship with the horse (or “other”), which served as a template for future positive relationships (Bachi et al., 2012). EIFC and TFC worked according to a relational set of assumptions, with a therapeutic alliance with foster carers serving as a supportive developmental context (Fisher et al., 1999; Southerland et al., 2009), which could help to address delayed maturation (Southerland et al., 2009).
Second, eight interventions, with 13 associated study reports, focused on enhancing parent and carer knowledge, skills, and functioning in order to modify their relationship with the care-experienced young person (Chamberlain, 2003; Chamberlain et al., 2006; Chamberlain et al., 2012; DeGarmo et al., 2013; Farmer Elizabeth & Lippold, 2016; Fisher et al., 1999; James & Meezan, 2002; Leve et al., 2009; Nilsen, 2007; Pithouse et al., 2002; Price, 2009; Van et al., 2017; Vanschoonlandt et al., 2012). Training curricula were predominantly guided by the middle-range theories of: Bowlby's Attachment (Bowlby & Ainsworth, 2013); Positive Youth Development (Waid & Uhrich, 2020); Social Learning Theory (Bandura & Walters, 1977); and to a lesser extent the resilience of the carer/parent and child/young person.
Across study reports, these theories were used to foreground the significance of developing positive relationships. Attachment emphasizes the importance of consistent caregiving and security in developing social and emotional functioning, especially among care-experienced individuals who might have had unavailable biological caregivers (Van et al., 2017; Vanschoonlandt et al., 2012). Positive attachments offer a context conducive to social learning, with individuals learning pro-social behavioral repertoires observationally through modeling and replication (Chamberlain, 2003; Chamberlain et al., 2006; Nilsen, 2007; Price, 2009; Van et al., 2017; Vanschoonlandt et al., 2012). Wider pro-social networks can reinforce the dynamics of positive caring relationships. Interventions further integrated learning for carers about the causes and impacts of trauma within relationships, largely by teaching trauma-focused cognitive behavioral therapy (Chamberlain, 2003; Chamberlain et al., 2006; Farmer Elizabeth & Lippold, 2016).
Interventions also included specific theories of change related to behavioral management and parenting techniques, namely coercion and operant conditioning (Chamberlain, 2003; Chamberlain et al., 2006; Pithouse et al., 2002). These worked to minimize coercive interactions between the child and their carer, while enhancing the management of negative behavior through positive reinforcement and non-harsh disciplinary methods. Mediation analysis conducted with the KEEP intervention reported that reduction in children and young people's problem behaviors was partly attributable to an increase in positive reinforcement (Chamberlain et al., 2008). Similarly, the Pathways Home intervention, which targeted re-unification with biological families, operated through encouragement-based parenting strategies (DeGarmo et al., 2013). However, the evaluation tested this hypothesized theoretical pathway, reporting that while the intervention increased parents’ use of encouragement-based practices, it did not translate into a reduction in total problem behaviors.
As part of the emphasis on modifying parenting knowledge, skills, and practices, TFC further theorized the relevance of carer characteristics in activating intervention mechanisms. One study report cited the importance of role satisfaction, motivation, and identity perception in the delivery of newly acquired parenting techniques (James & Meezan, 2002). Meanwhile, TFTC explored the significance of role enactment in the use of behavioral management skills (Farmer Elizabeth & Lippold, 2016). In the evaluation analysis, participating foster carers were asked if they identified as parent or professional. Those more closely aligned with being a parent were more likely to enact the postulated causal processes associated with Trauma-Focused Cognitive Behavioral Theory.
Third, two interventions described in six study reports, reported mentoring interventions that also operated through the theoretical approaches of Attachment theory, Positive Youth Development, and Social Learning Theory (Mezey et al., 2015; Taussig et al., 2015; Taussig et al., 2013; Taussig et al., 2007; Taussig et al., 2019; Weiler et al., 2021). These interventions emphasized the need for positive relationships across multiple contexts to help young people's development, and how pro-social modeling by mentors could support behaviors conducive to good mental health and well-being. Meanwhile, the SOLID intervention focused on wider positive social networks, and their role in supporting young people in coping with their problems in a positive and effective manner, while also encouraging them to attain their goals (Alderson et al., 2020).
Fostering Healthy Futures was the only intervention to theorize iatrogenic causal pathways (Taussig et al., 2015; Taussig et al., 2013; Taussig et al., 2007; Taussig et al., 2019; Weiler et al., 2021). The group-based curriculum risked reinforcing non-pro-social skill sets, encouraging the negative labeling of young people, and potentiating the learning of disruptive behaviors (i.e., deviancy training). Groups were constructed to mitigate these risks by including heterogeneous participants, notably “pro-social” young people. Pro-social skills were also practiced and reinforced within the mentoring relationship.
Organizational-level and community-level: system change
Four interventions, with five linked study reports, presented system-level theories that worked across the organizational and community domains (Chamberlain et al., 2012; Izzo et al., 2020; James & Meezan, 2002; Leve et al., 2009; Price, 2009). There were three types of theory. First, the CARE intervention provided a theory of change, aiming to transform the organizational ethos and approach of social care agencies. Specifically, it provided consultation, training, and technical assistance in residential care placements, working to reconfigure organizational policies and practices so that they aligned with a trauma-informed therapeutic ethos, which was considered to be conducive to promoting positive mental health among residents (Izzo et al., 2020).
Second, the TFC presented a context theory, mapping the wider system factors that could interact with an intervention's intrapersonal or interpersonal theory of change, potentially serving as inhibitors of intervention functioning. For example, the authors suggested that the capacity to improve young people's mental health through placement with a specialist foster carer could be complicated by educational disruption, which could adversely impact emotional development, or by being placed away from social networks, which could reduce opportunities for forming pro-social relationships (James & Meezan, 2002)
Third, KEEP and MTFC described implementation theories, focused on restructuring local and regional contexts, largely to optimize the theory of change underpinning parenting curricula (Chamberlain et al., 2012; Izzo et al., 2020; Leve et al., 2009; Price, 2009). Commonly, there was no named theory, and as such we defined it as “generic system change.” The interventions described two specific theories of implementation (Chamberlain et al., 2012; Leve et al., 2009; Price, 2009). Cascading Dissemination sought to reduce the role of intervention developers in delivery, building capacity through local Community Development Teams. Meanwhile, the Rolling Cohort model introduced a training sequence, starting with a small number of delivery sites, before taking learning from these sites to inform and support wider roll-out.
Map of intervention outcomes
We mapped the outcomes theorized to be targeted by interventions, and their theories, according to the three outcome domains specified by the review: subjective well-being; mental, neurodevelopmental, and behavioral disorders; and suicide-related outcomes (Table 1; Figure 2). On occasion, study reports linked to the same intervention theorized targeting different outcomes. In some instances, an individual study report did not specify a targeted outcome domain, but this was included in related reports for the same intervention.
Intrapersonal-level outcomes
All three interventions with theories operating at the intrapersonal level targeted measures of subjective well-being (Alderson et al., 2020; Bachi et al., 2012; Taussig et al., 2015; Taussig et al., 2013; Weiler et al., 2021). They all intended to address mental health, most commonly total social, emotional, and behavioral problems (Alderson et al., 2020; Taussig et al., 2015; Taussig et al., 2013; Taussig et al., 2007; Weiler et al., 2021; Weiler & Taussig, 2019). No interventions targeted suicide-related outcomes.
We mapped additional outcomes targeted by these theories. As might be expected, they largely focused on individual behavior change, notably in relation to substance use and sexual health (Alderson et al., 2020; Taussig et al., 2015). There was also a measurement of: children and young people's relationships (Bachi et al., 2012; Taussig et al., 2015; Taussig et al., 2013; Weiler & Taussig, 2019); social care placement stability and breakdown (Alderson et al., 2020; Pithouse et al., 2002); education and employment (Taussig et al., 2015; Taussig et al., 2007); and offending and victimization (Taussig et al., 2015).
Interpersonal-level outcomes
Of the 12 interventions that included an interpersonal theory of change, three theorized impacting domains of subjective well-being (Alderson et al., 2020; Bachi et al., 2012; Taussig et al., 2015; Taussig et al., 2013; Weiler et al., 2021). These three interventions were the approaches that all also included intrapersonal theories of change (Chamberlain et al., 2006; Chamberlain et al., 2008; DeGarmo et al., 2013; Farmer Elizabeth & Lippold, 2016; Fisher et al., 1999). All interventions targeted mental health, and again the most common outcome domain was total social, emotional, and behavioral problems (Alderson et al., 2020; James & Meezan, 2002; Leve et al., 2009; Mezey et al., 2015; Pithouse et al., 2002; Price, 2009; Taussig et al., 2015; Taussig et al., 2013; Taussig et al., 2007; Taussig et al., 2019; Van et al., 2017; Vanschoonlandt et al., 2012; Weiler et al., 2021). One of the interventions targeted suicide-related outcomes (Mezey et al., 2015).
In mapping additional outcomes, there was an emphasis on targeting relationship-based outcomes. Four interventions targeted aspects of children and young people's relationships with peers, parents and carers, and a range of other significant others (Bachi et al., 2012; Chamberlain et al., 2006; Farmer Elizabeth & Lippold, 2016; James & Meezan, 2002; Leve et al., 2009; Taussig et al., 2015; Taussig et al., 2013). Theories within this domain were also routinely linked to outcomes related to parent and carer mental health and well-being, in addition to their parenting skill, knowledge and functioning (Chamberlain et al., 2008; DeGarmo et al., 2013; Farmer Elizabeth & Lippold, 2016; Leve et al., 2009; Nilsen, 2007; Pithouse et al., 2002; Southerland et al., 2009; Van et al., 2017; Vanschoonlandt et al., 2012).
Organizational-level and community-level outcomes
All interventions with organizational and community theories targeted mental health, specifically total social, emotional and behavioral problems (Izzo et al., 2020; James & Meezan, 2002; Price, 2009) and social-emotional functioning problems (James & Meezan, 2002; Leve et al., 2009). None were hypothesized to address subjective well-being. One addressed suicide-related outcomes (Izzo et al., 2020). As interventions across these domains had a focus on theories of change e that emphasized a change to organizational ethos, and implementation theories that modified delivery approaches, they included outcomes related to organizational environment and functioning (Chamberlain et al., 2012; Izzo et al., 2020).
Stakeholder priority program theories
We asked participants to reflect on which interventions, and associated program theories, they felt would most likely be effective, feasible, and acceptable in the UK and should be prioritized. They further explored novel theories they hoped to see integrated into interventions moving forward. Stakeholders’ priorities, and how they compare with the evidence base is presented in Figure 2.
Generally, the discussion focused on the type of intervention rather than the underpinning theory. However, there were two clusters of theories of change that stakeholders felt would be most relevant. First, stakeholders expressed a preference for interpersonal theories that focused on social support and building positive relationships between care-experienced young people and significant others, especially care-experienced others. As such, there was some resonance with: Attachment theory (Bowlby & Ainsworth, 2013); Positive Youth Development (Waid & Uhrich, 2020); and Social Learning Theory (Bandura & Walters, 1977). Importantly, the care-experienced young people groups expressed concern about interpersonal theories that linked to parental management and constructs such as operant conditioning. They felt such approaches could drift into harsh discipline and control when the evident need was for supportive and understanding relationships with carers.
Second, there was support for organizational-, community-, and policy-level theories of change, that had a specific focus on transforming the ethos of social care, such as in the case of the CARE intervention (Izzo et al., 2020). This involved developing a practice culture that was clearly informed by an understanding of attachment and trauma. Indeed, young people felt all professional groups should be trained in such an approach. Meanwhile, foster carers felt that facilitation of a shared language and ethos could ensure more effective multi-agency working as part of a wrap-around package of support for young people.
Discussion
The discussion provides an overview of the key results of the theory map while reflecting on the methodological quality of current practice in the field. It then integrates the results of the map with findings from another part of the overarching CHIMES systematic review, namely the synthesis of outcome evaluations, to consider if the identified program theories have any evidence for being effective, ineffective, or even harmful. If further considers where there is a lack of intervention, particularly in terms of meeting stakeholders’ needs, and how this might be addressed moving forward.
Overview of results
The present theory map shows the theories currently used to target the mental health and well-being of care-experienced children and young people. Centrally there was a paucity of theoretically informed interventions eligible for the review. Of the 64 interventions identified, only 13 interventions presented a theory of change, implementation theory, or context theory. There may be several explanations, from the fact that the development and description of program theory has not yet gained traction in the field, to publishing constraints around limited journal word lengths. Regardless, there remains a need to bring intervention and evaluation practice in this field into alignment with current methodological frameworks, which recommend clear explication of program theory (Maden et al., 2017; Moore et al., 2021; Moore & Evans, 2017; O'Cathain et al., 2019; Prestwich et al., 2014; Skivington et al., 2021).
Intervention theories clustered around interpersonal theories of change, largely focused on modifying children and young people's relationships with carers, peers, or additional significant others. These were often established middle-range theories, frequently used across the academic disciplines of child development, social work, criminology, and psychology: Attachment theory (Bowlby, 1978); Positive Youth Development (Waid & Uhrich, 2020); and Social Learning Theory (Bandura & Walters, 1977). Together, they suggested the importance of healthy attachments, that enact positive modeling and replication of social behaviors, within a pro-social context. For parenting interventions, theories of change such as operant conditioning specified parenting techniques around positive behavioral reinforcement to encourage pro-sociality. There were more limited theories at the organizational and community level, and only a couple of interventions integrated implementation theories to maximize functioning or context theories to understand system influences on causal mechanisms. These latter theories tended not to be clearly linked to middle-range theories, often inductively building theory from empirical findings from the current or previous research.
We also considered the outcomes hypothesized to be targeted by different intervention theories. It is evident that there is not currently a common set of outcomes linked to each theory. Indeed, theories of change across socio-ecological domains variously targeted different dimensions of mental health, neurodevelopmental, and behavioral disorders. This may suggest a lack of clarity as to how these theories might function in the types of interventions we have considered. The only exception was that interventions that coupled intrapersonal and interpersonal theories of change, were the only approaches to target subjective well-being (Alderson et al., 2020; Bachi et al., 2012; Taussig et al., 2015; Taussig et al., 2013; Weiler et al., 2021). However, there was no detailed explanation as to why these multi-level interventions would be specifically relevant to improving well-being, and given the small number of interventions in question, this finding should be treated cautiously. Theories of change also targeted a range of additional outcomes, with implementation theories being linked to changes in organizational functioning and environment (Chamberlain et al., 2012; Izzo et al., 2020).
Quality of program theory development and description
It is important to reflect on the process of theory development. For the large part, this was unspecified in study reports. Generally, theories were detailed as relevant by authors, who often also served as the intervention originators. There was minimal rationale for their inclusion or clear explication of how they mapped onto the drivers of the problem. This approach sits in contrast to a range of methodological recommendations, which maintain that theories should not be “off the shelf” but clearly attend to the contextually relevant, modifiable risk factors that have the most leverage in achieving change (Fraser et al., 2009; Moore & Evans, 2017; Skivington et al., 2021).
There was a notable lack of stakeholder involvement in the generation of program theory, especially among care-experienced children and young people. Guidance on intervention development foregrounds the importance of theorizing interventions through co-production with local stakeholders, ensuring that it responds to their conceptualization of the problem and its determinants (Hawkins et al., 2017; O’Cathain et al., 2019).
Our quality appraisal of the interventions’ theoretical basis also offers useful direction as to how theories may be better articulated. Methodological reflections have maintained that it is inadequate to simply cite an intervention's theory (Moore & Evans, 2017), and this was a central issue. All types of theory lacked a clear and coherent description. Some interventions integrated theories of change across multiple socio-ecological domains (e.g., intrapersonal and interpersonal), and there was limited exploration of how these interacted in the generation of outcomes. Logic models were also under-utilized as a diagrammatic presentation of program theory. Recent progress in complex-systems-informed logic models may be supportive in the future as they offer a structure for presenting a program theory that integrates a theory of change, implementation theory, and context theory (Rehfuess et al., 2018). Furthermore, there was limited empirical testing of theories, primarily through mediation analysis or moderator analysis, where insights may be offered into how interventions work for different populations across contexts. Theory testing within intervention evaluation will help in generating an evidence base for which theories can effectively address postulated outcomes.
Evidence for the effectiveness of program theories
Following the construction of the theory map, we cross-referenced the theories against the findings of the outcome synthesis to understand if there is empirical support for them being effective, ineffective, or even harmful approaches. The outcome synthesis was conducted as part of the overarching CHIMES review and is published elsewhere (Evans, Macdonald, Trubey, Melendez-Torres, et al., 2024; Trubey et al., 2024). There was mixed evidence of the effectiveness for theories, although evaluations were often subject to limitations.
There was some evidence for Fostering Healthy Futures, which drew upon theories of change linked to Attachment, Positive Youth Development, and Resilience, effectively improving subjective well-being and total social, neurodevelopmental, and behavioral disorders (Taussig et al., 2015; Taussig et al., 2013; Taussig et al., 2007; Taussig & Culhane, 2010; Taussig et al., 2019). However, despite the promise of their effectiveness, interventions that use interpersonal theories have shown numerous implementation issues (Alderson et al., 2020; Mezey et al., 2015). There was also limited evidence for these theories when integrated into parenting training curricula, such as KEEP or MTFC (Chamberlain et al., 2008; Price et al., 2015).
In terms of organizational theories of change, especially when focused on modifying ethos and the theoretical orientation of social care practice, the evidence was mixed, with evaluation of the CARE intervention only showing reductions in incidents in self-harm for within-study cohorts rather than the whole study sample (Izzo et al., 2016).
Evidence gaps in program theory
In identifying the current use of program theory, we were able to map extant gaps. Primarily, it should be noted that the wealth of theory development and testing is from the USA, and hence we currently know little about how theories operate in other international contexts.
Evidently, there was limited use of intrapersonal-level theories of change, targeting children and young people themselves. While this arguably avoids individualizing responsibility for mental health, it potentially means young people's needs, skills, and experiences are being overlooked. There was also a paucity of theories of change targeting the structural determinants of outcomes at the organizational, community, or policy level. In the wider CHIMES study, a small number of policy-level interventions were identified, such as the re-prioritization of different types of care placement (e.g., foster care vs. residential care), but these did not have a clear theoretical basis (Portwood et al., 2018). Given evidence reporting that care entry and experiences are linked to socio-economic deprivation (Bywaters et al., 2016; Bywaters et al., 2018), there is significant scope for developing theoretically informed structural-level interventions. Policy-level intervention that tackles lack of resources for care-experienced individuals, such as the universal basic income for care-leavers pilot in Wales, offers a potential example for future direction (Welsh Government, 2022). There was also a clear lack in implementation theories and context theories.
We further identified gaps in the outcomes targeted bytheories, beyond mental health, behavioral and neurodevelopmental disorders. Only three included interventions targeted subjective well-being (Alderson et al., 2020; Bachi et al., 2012; Taussig et al., 2015; Taussig et al., 2013; Weiler et al., 2021) and two targeted suicide-related outcomes (Izzo et al., 2020; Mezey et al., 2015). Given that well-being is reported to be poorer in this population compared to non-care-experienced populations (Long et al., 2017), and they have a higher prevalence rate of suicide attempts (Evans et al., 2017), developing theories to address these outcomes is vital.
Future research and practice recommendations
Following the construction of the theory map, consultation with children and young people, carers and parents, and professional stakeholder groups offered useful direction in prioritizing how the evidence gaps are addressed and which theories should be taken forward as part of future work. There was endorsement of interpersonal theories of change: Attachment (Bowlby & Ainsworth, 2013); Positive Youth Development (Waid & Uhrich, 2020); and Social Learning Theory (Bandura & Walters, 1977). Stakeholders also expressed concern about the lack of structural-level interventions that target the culture and practices of organizations, rather than individual professionals. As such, a priority may be working to develop interventions with a theory of change around attachment or trauma-informed practice, that can construct a shared ethos and language across agencies to facilitate interprofessional collaboration.
Limitations of the study
The review has a number of limitations that should be taken into account when interpreting the results. First, we only included theory reports where there was an associated outcome evaluation, as we wanted to understand which theories were potentially effective. As such, there may be comprehensive theory descriptions that have not yet been tested via an outcome evaluation. Future maps and syntheses may capture this growing evidence base. Second, we experienced challenges in defining what constitutes a theoretical report. For the purposes of the review, we stated that a theory of change had to have a fully explicated causal pathway and be clearly linked to an outcome domain, while recognizing that the linkage to outcomes could sometimes be reported in related reports of the same intervention. We also specified that implementation and context theories were within remit. While we did reach consensus as a review team, there was extensive discussion, and replication of the review may not necessarily reach the same decision on eligibility. Third, there were challenges in applying the appraisal tool, as the binary assessment could be difficult where the presence of relevant information wasn’t always evident, and the lack of continuous scoring meant some nuance could be lost.
Conclusion
The mental health and well-being of care-experienced children and young people remain a public health and social care priority. Despite methodological recommendations to develop theoretically informed interventions, our theory map has identified a lack of interventions with a clear and coherent theoretical basis. Where available, intervention theories of change largely targeted the interpersonal domain, focusing on modifying the relationship between children and young people, their carers/parents, and other key figures. There was a lack of theories of change targeting the organizational-, community-, and policy-level drivers of the problem, or implementation and context theories. Few interventions theorized how they might impact subjective well-being and suicide-related outcomes. Future intervention and evaluation research should focus on ensuring that approaches have a clear, comprehensible, and relevant theoretical basis, preferably co-produced with stakeholders, to maximize the likelihood of effectiveness.
Supplemental Material
sj-docx-1-jsw-10.1177_14680173251336997 - Supplemental material for How might we improve the mental health and well-being of care-experienced children and young people? Review and map of intervention theories
Supplemental material, sj-docx-1-jsw-10.1177_14680173251336997 for How might we improve the mental health and well-being of care-experienced children and young people? Review and map of intervention theories by Rhiannon Evans, Sarah MacDonald, Rob Trubey, Jane Noyes, Mike Robling, Simone Willis, Maria Boffey and Charlotte Wooders in Journal of Social Work
Footnotes
Ethical approval
Ethical approval for this project was given by: The CHIMES review was exempted from ethical approval from Cardiff University School of Social Sciences Research Ethics Committee.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the NIHR-PHR grant number NIHR129113. The work was supported by The Centre for Development, Evaluation, Complexity and Implementation in Public Health Improvement (DECIPHer) funded by the Welsh Government through Health and Care Research Wales. The Centre for Trials Research receives funding from Health and Care Research Wales and Cancer Research UK.
Declaration of conflict of interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors confirm that they have no conflict of interest in respect of the material submitted in this article.
Author contributions
Conception of the study design was conducted by RE, GJMT, MR, and JN. Searches were designed and conducted by SW. Screening, extraction, and appraisal were conducted by RE, SM, RT, GJMT, and SV. Mapping was conducted by RE, SM, RT, GJMT, and SV. Stakeholder consultations were led by RE, SM, MB, and CW. The publication was drafted by RE. The publication was confirmed by all authors.
Acknowledgements
The Authors acknowledge the following for their contribution to this article: The CHIMES review acknowledges the support of the Project Advisory Group, participants of stakeholder consultations, Dr Asmaa El-Banna, Dr Helen Morgan, Lindsey Allan, Clare Olson, Payton Ramsey, Rohen Renold, Lorna Stabler, and Rachael Vaughan.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.