
Abstract
Summary
Children's social care services can be a challenging place to work, with staff regularly reporting higher stress levels relative to the general population and other public sector settings. Thus, it is important to provide staff with good support. Previously, we completed a randomised controlled trial (RCT) of Schwartz Rounds (SRs) and reported a series of non-statistically significant differences between intervention and comparison groups. We also undertook a process evaluation, to identify enablers and barriers to the successful implementation of SRs in children's social care.
Findings
Compared with studies of SRs in healthcare settings, we identified several similar enablers, such as senior management buy-in and effective administrative support, and some similar barriers, such as high workloads and poor publicity. We also identified specific enablers and barriers for social care settings, including the synergy between existing practice models and SRs, the nature of trauma in social care compared with healthcare, and some related to the different nature of organisational and workload pressures.
Applications
Understanding the differences between SRs in healthcare and social care will be useful for local authorities who may want to support their staff via the provision of SRs. They should also be useful in any future definitive evaluation of SRs for social care by helping to maximise the possibility for a successful implementation.
Background
‘It's Sunday mid-morning and I can already feel the anxiety rising in my chest’.
(Anonymous child and family social worker, quoted in Community Care, 2022).
Statutory child and family social work typically involves working with people in difficult life circumstances including those dealing with issues of abuse, discrimination, domestic violence, mental health problems, poverty, and substance use (Hood et al., 2021). It also often means high workloads, role ambiguity, and limited resources (McFadden et al., 2014). Thus, it is unsurprising that people working in social care report higher stress levels than the general population and by comparison with many other public sector workers (Antonopoulou et al., 2017; Coffey et al., 2004; Kinman & Grant, 2010; Ravalier, 2018). Heightened workplace stress has a negative impact on individual wellbeing (Ravalier et al., 2020; Ravalier et al., 2022), staff retention (Houston & Knox, 2012; Renner & Preister, 2009; Turley et al., 2021) and the quality of services provided (Barak et al., 2009; Kapoulitsas & Corcoran, 2014).
It is vital to support all social care staff to reduce and mitigate these problems. A systematic review of interventions to promote the wellbeing of social workers included fifteen studies (Turley et al., 2020). Three evaluated individual-level interventions (e.g., journaling or resilience skills training). Eleven evaluated organisational-level interventions (e.g., supervision). And one evaluated a community-level intervention (e.g., integrating social work with other services). While the review concluded there is ‘very little high quality or consistent evidence available’ (p. 6), it also found ‘tentative suggestions that interventions may be more effective when delivered at the organisational level’ (ibid).
Schwartz Rounds are one such intervention, used extensively within healthcare settings in England (Robert et al., 2017). They aim to provide a mechanism for supporting staff well-being and enhancing service delivery by promoting understanding, empathy, and collaboration among professionals (Pepper et al., 2012; Thompson, 2013). Schwartz Rounds offer a unique space for staff from different roles and all levels of the organisation to come together on a monthly basis. Lasting about an hour, each Schwartz Round centres on a theme or revolves around experiences with specific individuals or families. During these sessions, a selected panel of volunteers share their personal narratives, emphasising the emotional and social challenges they face in their roles. These stories are not just about clinical decisions or outcomes but focus on the human side of healthcare work, touching on feelings, moral dilemmas, and the impact on personal well-being.
These stories are then followed by a guided reflective discussion, facilitated by individuals trained to encourage open and empathetic dialogue. The environment is designed to be non-judgmental and supportive, allowing participants to explore and share their own responses to what they’ve heard. This process fosters a culture of mutual support and understanding across different roles within the healthcare setting, promoting empathy, compassion, and a sense of community among staff. To ensure the effective implementation of Schwartz Rounds, organisations need to establish certain key roles: a clinical or practice lead to champion the initiative, multiple facilitators to guide the discussions, an administrator to manage logistics, and a steering group that represents a cross-section of the organisation, including management, frontline staff, and support personnel. This infrastructure supports the regular and meaningful execution of Schwartz Rounds, contributing to their potential to enhance well-being and improve interprofessional collaboration.
Following an evaluation of Schwartz Rounds in healthcare settings, Maben et al. (2018) said they represent a ‘unique organisation-wide ‘all staff’ forum’ (p. vi). They also found that regular attendance was associated with a statistically significant improvement (p < 0.05) in psychological well-being, measured using the 12-item General Health Questionnaire (Goldberg & Williams, 2000) – albeit Maben et al. did not use a randomised design, meaning that a definitive relationship between cause-and-effect has not been established. Flanagan et al. (2019) completed another study in forty-seven NHS trusts and found that ‘the overall experience of Schwartz Rounds was very positive across all settings…and regardless of [professional] background’ (p. 140). Several studies have reported similar findings, while noting the importance of effective implementation (Adamson et al., 2018; Goodrich, 2012; Hewitt et al., 2012; Ng et al., 2023).
Farr and Barker (2017) explored the implementation of Schwartz Rounds in healthcare and identified several common enablers and barriers. Enablers included (i) a core group of committed staff, (ii) senior management support, (iii) an organisational culture that values reflection and well-being, and (iv) accessible and well-advertised Schwartz Rounds. Barriers included (i) limited administrative support, (ii) high workloads, (iii) non-reflective and managerialist organisational cultures, (iv) inaccessible Schwartz Rounds, and (v) wider service pressures. Maben et al. (2018) identified similar enablers, including (i) the need for senior management support, and (ii) the synergy between the principles of Schwartz Rounds and the existing organisational culture. They also identified some additional factors, including (i) the credibility and expertise of the facilitators, (ii) the organisation's motivations for adopting Schwartz Rounds, and (iii) a commitment to persevere even if Schwartz Rounds are not immediately successful.
Beyond their origins in healthcare, Schwartz Rounds have shown versatility and effectiveness in other settings, reflecting their fundamental value in addressing the emotional and social dimensions of caregiving. In palliative and hospice care environments, for example, Schwartz Rounds have been implemented to help teams navigate the complex emotional landscapes encountered when providing end-of-life care (Vaughan, 2018). Similarly, Schwartz Rounds have been used in forensic mental health services, with one study finding the experience to be emotionally challenging but ultimately rewarding, with the potential to enhance teamworking and well-being (Groves et al., 2022). The veterinary field has also seen the piloting of Schwartz Rounds, acknowledging the emotional challenges inherent in veterinary practice, including dealing with sick animals, euthanasia decisions, and the distress of pet owners. In one veterinary practice, over 90% of attendees were positive about the benefits of Schwartz Rounds and planned to attend again in future (Martin, 2024). These examples suggest that Schwartz Rounds can be adapted for use beyond the healthcare settings for which they were originally developed.
In England, local authorities (public administration organisations) have primary responsibility for delivering social care services for children and families in specific areas. We have previously reported the results of a randomised controlled trial (RCT) of Schwartz Rounds in English local authorities (Wilkins et al., 2023). This study took place in two phases between 2019 and 2021. In phase one, six Local Authorities took part, and staff members were randomly allocated to an intervention or comparison group. Those in the intervention group were invited to attend six Schwartz Rounds. A further four Local Authorities took part in phase two, with the same design as phase one. However, in March 2020 the UK government announced the first COVID-19 lockdown, and the study was paused. In summer 2020, the study was re-started with online Schwartz Rounds. Thus, phase one involved only in-person Schwartz Rounds, while phase two included some in-person and some online Schwartz Rounds.
In the RCT protocol (Wilkins & Forrester, 2019), we provided an initial logic model (figure 1). Based on Maben et al. (2018), we hypothesised that the implementation of Schwartz Rounds would require (i) senior management support, (ii) suitable logistical arrangements, (iii) skilled facilitators and (iv) an effective steering group. With these pre-requisites, Schwartz Rounds could result in the creation of a reflective (counter-cultural) space, enabling staff to share their social and emotional experiences, leading to greater trust, empathy, and connectedness. This should lead to improved psychological well-being, and reduced rates of sickness and staff turnover.
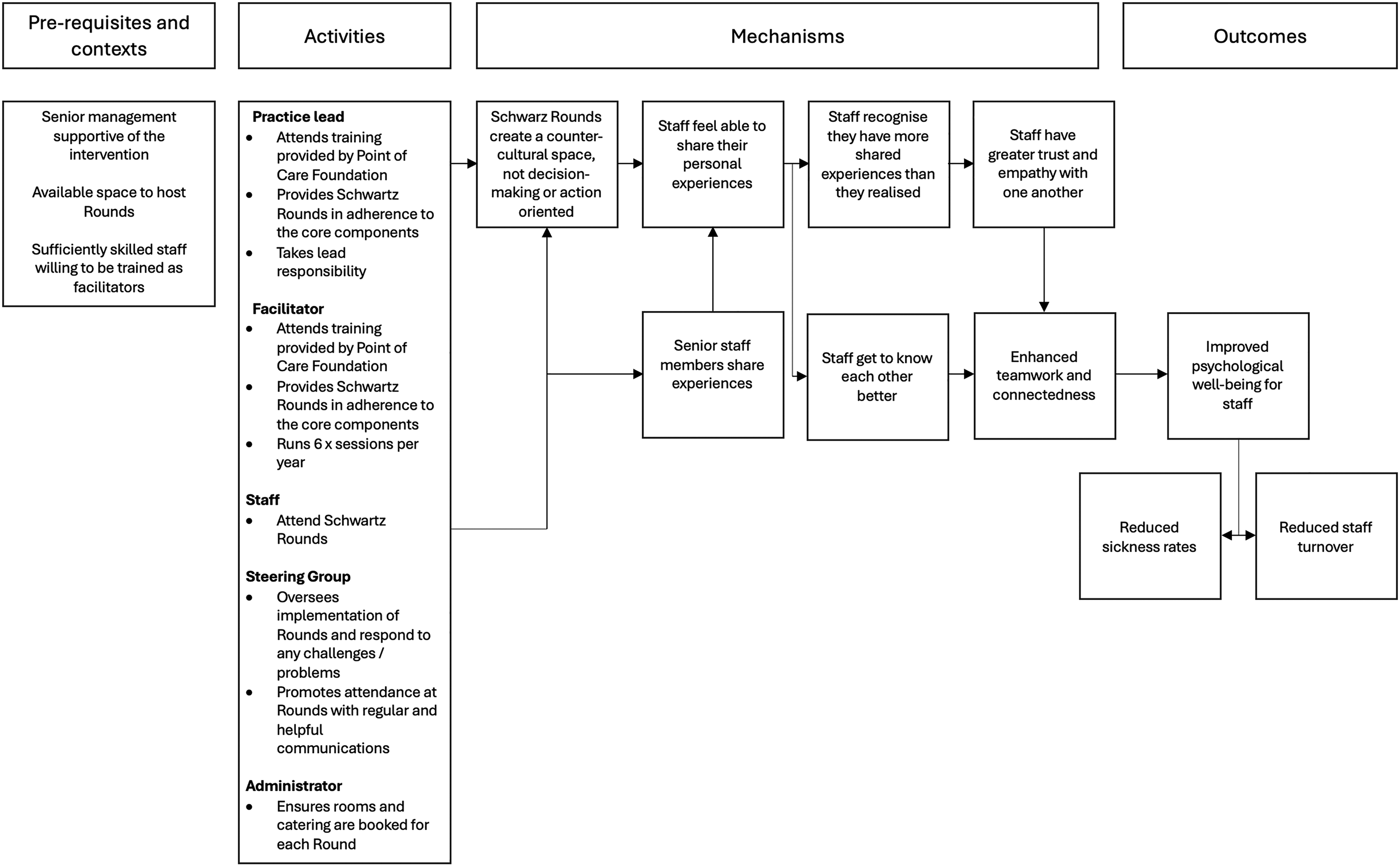
An initial logic model for Schwartz Rounds in children's social care (Wilkins & Forrester, 2019).
The main outcome for the RCT was the psychological well-being of staff measured via the GHQ-12, comparing between participants in the intervention and comparison groups, and within the intervention group between individuals who attended regularly (3+ Schwartz Rounds), irregularly (1–2 Schwartz Rounds) or not at all (zero Schwartz Rounds). None of these comparisons resulted in a statistically significant difference (p < 0.05) although we did find that regular attendance was associated with lower GHQ-12 scores.
These findings raise questions about the transferability and effectiveness of Schwartz Rounds to and in social care settings. In addition to the primary outcome, we collected a wealth of positive feedback from staff via surveys, interviews and focus groups. Based on standard feedback forms (n = 493) completed at the end of each Schwartz Round, 96.2% of respondents rated their experience as exceptional (19.3%), excellent (51.7%) or good (25.2%). A majority (91.3%) said they would attend more Schwartz Rounds and recommend Schwartz Rounds to their colleagues (90.8%). In interviews and focus groups, respondents commonly – if not uniformly – said they experienced greater empathy and connection with colleagues. We also calculated that in-person Schwartz Rounds costed £22.53 per attendee, and £19.36 when held online (authors own).
In summary, Schwartz Rounds are widely used in English healthcare settings, and may have positive benefits for staff and people using services. In our study of Schwartz Rounds in children's social care, we found some evidence of similar benefits, albeit none that were statistically significant (p < 0.05). This may be explained by the differences between social care and healthcare, and hence the enablers and barriers for implementation may also be different. Given the very positive feedback from staff, and their relatively low-cost, it is worth addressing questions of implementation in more detail. Thus, our research questions for this article were as follows:
Why did people attend or not attend Schwartz Round meetings? What are the enablers and barriers for the implementation of Schwartz Rounds in children's social care?
Methodology
Our approach to research is informed by the concept of theory-oriented evaluation (Weiss & Weiss, 1998). This means developing descriptions of ‘practice’ and theorising how different components may interact to produce ‘outcomes’. To achieve this, we used a mixed-method design including surveys, qualitative interviews with key stakeholders, and staff focus groups. A mixed-methods approach is advantageous as it allows for the inclusion of quantitative and qualitative data, and a triangulated exploration of the research question (Jick, 1979).
Recruitment of participants
All Local Authorities in England (n = 152) were eligible to take part in the original RCT. In total, twelve applied, of which eleven were selected, and ten provided Schwartz Rounds to their staff. The data reported in this article relate to these ten Local Authorities. To recruit participants for the survey and focus groups, emails were circulated to all staff including social workers, managers, family workers, and administrators. Two reminder emails were sent at varying intervals to increase response rates. Surveys were administered online and included an informed consent procedure. Additional informed consent procedures were used during focus groups, including a reminder to respect confidentiality. Key stakeholders were recruited for interview via targeted emails to senior staff and those directly involved in delivering Schwartz Rounds, including practice leads and facilitators. Informed consent was obtained prior to each interview.
Data collection (survey, interviews and focus groups)
To collect data in relation to our first research question, an online Qualtrics survey was distributed following the sixth Schwartz Round in each Local Authority (copyright © 2022, Provo, UT; https://www.qualtrics.com). None of the questions forced a response, so respondents could skip those they preferred not to answer. To collect data in relation to both of our research questions, interview respondents were asked about (i) their involvement with the implementation of Schwartz Rounds, (ii) their views and experiences of what makes for a successful Schwartz Round, (iii) what had gone well and less well with Schwartz Rounds in their Local Authority, (iv) any adaptations they made to Schwartz Rounds and (v) the effect of Schwartz Rounds on the wider organisation. Focus group respondents were similarly asked about (i) their experiences of attending Schwartz Rounds, (ii) motivations and barriers for attending, (iii) the effect of attending Schwartz Rounds for them and the wider organisation and (iv) (where applicable) preferences for attending Schwartz Rounds online or in-person.
Analysis
Interviews and focus groups were audio-recorded and then transcribed by an independent company. These were analysed using NVivo (v12) and Excel (v16 for Mac) via recursive abstraction (Polkinghorne and Arnold, 2014). This involves a sequential process in which transcripts are read several times, and then transfigured into an Excel spreadsheet, organised by (i) respondent and (ii) question. Responses to each question are then paraphrased for concision, while seeking to maintain the original meaning. Responses are combined between respondents to form initial themes, which are then refined via a process of further thematic coding and re-coding. The process is iterative, with each stage repeated until a final set of themes is created and agreed upon (figure 2). For our study, all team members initially and independently reviewed the data, noting initial impressions and potential themes. These individual analyses were then discussed collectively, fostering a preliminary set of themes based on consensus. This iterative process was repeated multiple times, with the data being revisited and reinterpreted considering emerging insights. Through this recursive abstraction, we were able to refine our thematic categories, ultimately identifying five distinct themes that encapsulated the core barriers and enablers as perceived by participants.
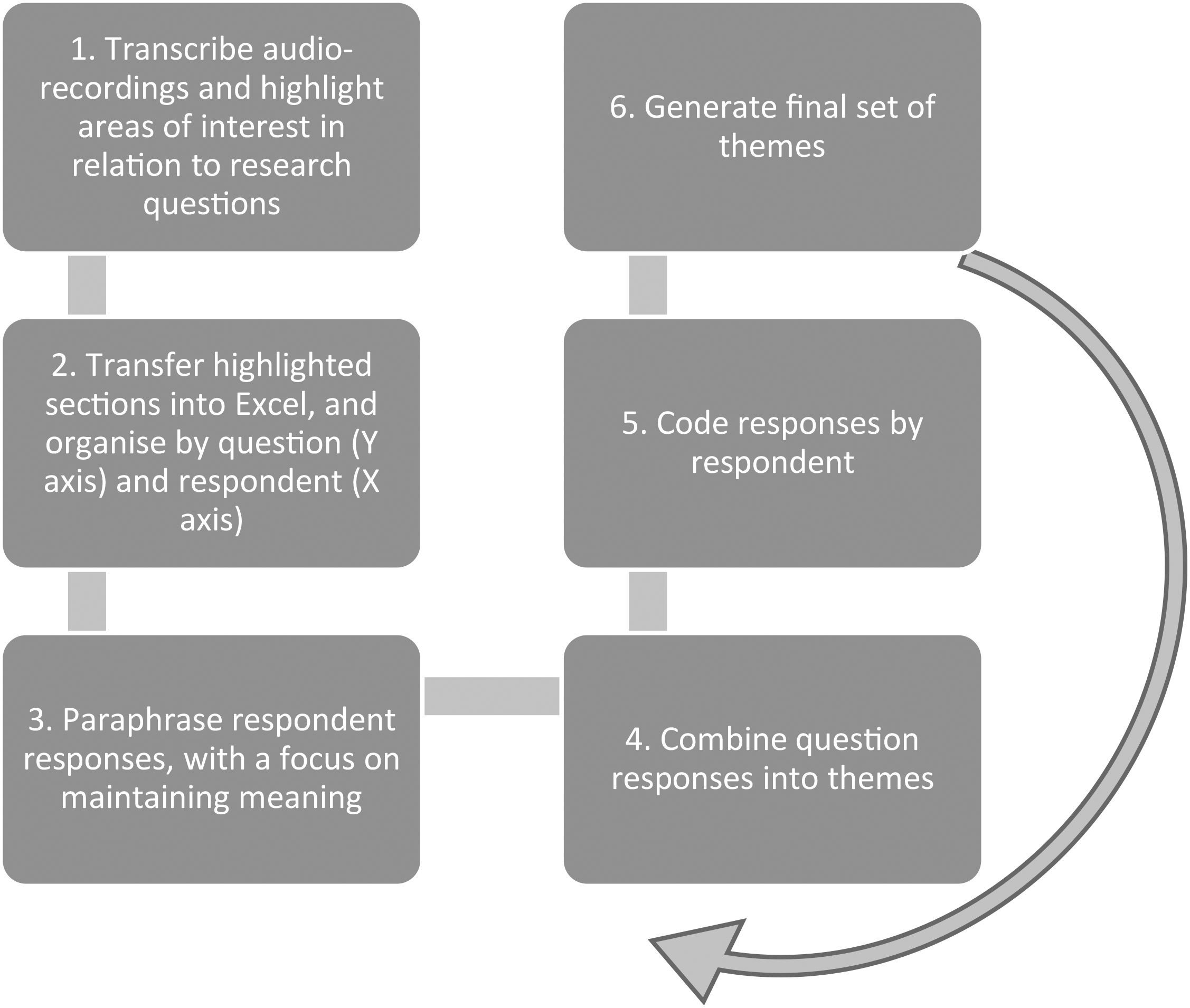
Overview of the stages of recursive abstraction.
Regarding the integration of data from focus groups and interviews, we initially analysed these data sets separately to preserve the unique contexts and dynamics of each method. This separate analysis allowed us to identify any method-specific patterns or themes. Following this individual analysis, we merged the data sets, looking for overarching themes and patterns that were consistent across both methods. This approach ensured that our thematic analysis was robust, capturing a comprehensive view of participants’ experiences while also allowing for the identification of method-specific insights.
For the survey, descriptive statistics including response frequency and percentage of respondents selecting each option were calculated via SPSS (v24).
Ethics
The RCT of Schwartz Rounds was given ethical approval via the School of Social Sciences at [our] University (SREC/3170). Participation in the study was voluntary and respondents were asked to provide written consent before taking part.
Findings
For this article we used data collected from 16 focus groups (involving 57 participants), 22 semi-structured interviews (involving 13 participants, some of whom were interviewed more than once) and 378 surveys (in which the participant provided at least some data).
Interviews and focus groups findings
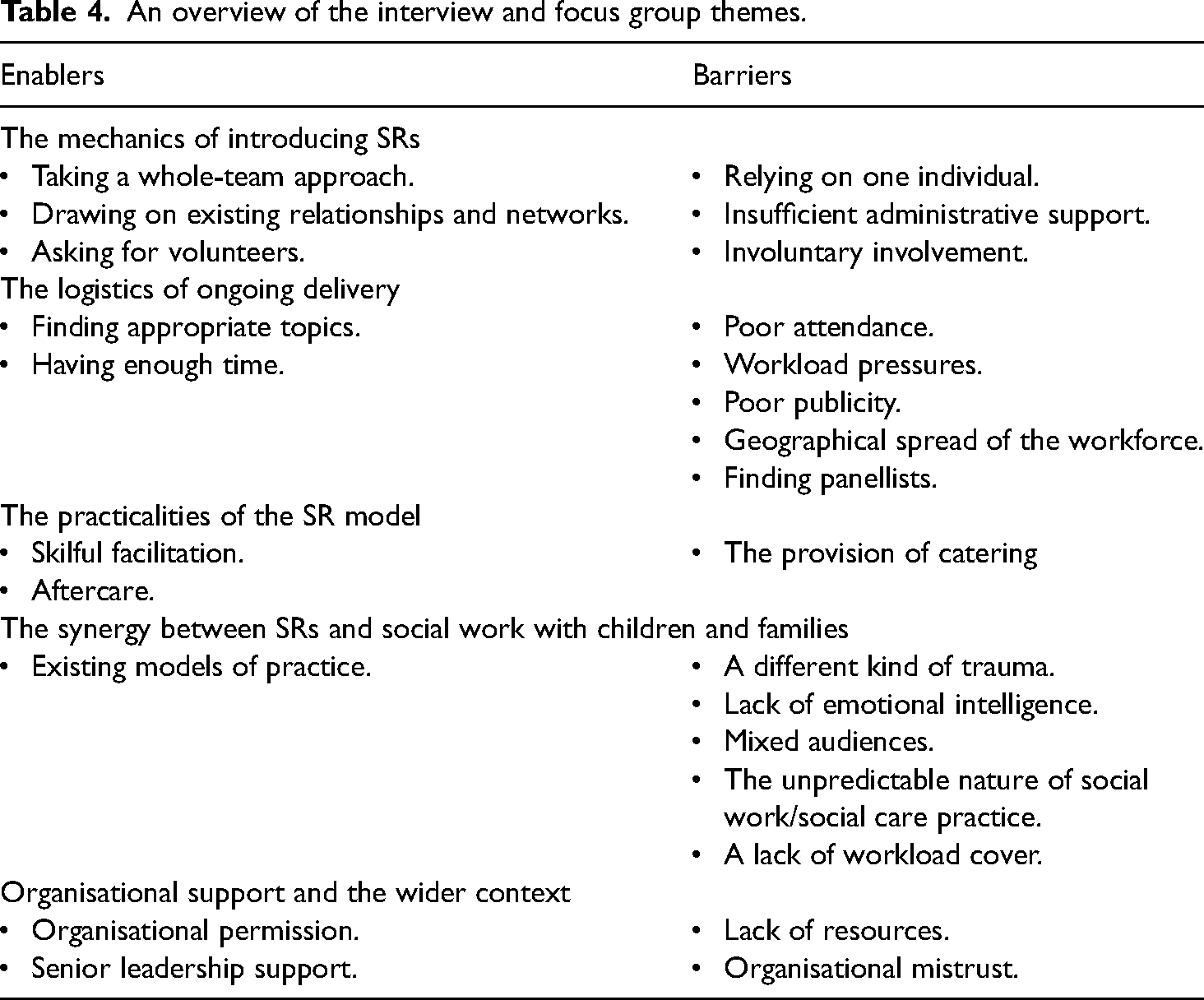
From the interview and focus group data, we identified five themes, with sub-themes identified as either enablers or barriers (Table 4).
The mechanics of introducing Schwartz Rounds
Respondents, particularly those involved in leading and facilitating Schwartz Rounds, identified the importance of team working, and the problem of relying on individuals. One interview respondent described their experience of having ‘quite a lot of responsibility on me, on my shoulders because of capacity from other people’ (practice lead, Local Authority 7). Another said, ‘there is senior management buy-in verbally [laughs] but nobody has offered any practical or real support…what I really need is to be part of a team’ (practice lead, Local Authority 1). A team-based approach to implementation worked especially well when it included administrative support to help manage essential logistical tasks such as booking rooms and publicising Schwartz Rounds. As well as having an effective steering group and administrative support, several interview respondents noted the importance of having motivated volunteers. In some Local Authorities, people were mandated to help, and this impacted on how much responsibility they felt and were prepared to accept, and in some Local Authorities this meant that ‘none of them stayed on when they were told they could stop’ (practice lead, Local Authority 6).
The logistics of ongoing delivery
Respondents also described barriers and enablers for the ongoing provision of Schwartz Rounds. A key enabler was having sufficient time to attend the Schwartz Rounds. Conversely, many of the barriers related to a lack of time, because of high workloads or the geographic spread of teams. Several respondents made similar points about high workloads. In larger Local Authorities, the geographical spread of the workforce was another barrier, due to the distances involved and because some Local Authorities discouraged staff from travelling to save money. In one Local Authority, this meant ‘people are less likely to attend if they’re not based in the building. Some people do, but the majority is from the base where it's being held’ (practice lead, Local Authority 6). Another respondent noted that the Schwartz Round model ‘is being translated…from institutional settings like hospitals where you have one big building and everyone is more or less on site [whereas in this Local Authority] we discourage people from travelling because its ineffective in terms of resources…it's an hour and a bit from top to bottom [of the Local Authority] which is very different from going down six floors in a lift in a hospital, isn’t it?’ (practice lead, Local Authority 9).
Another barrier was publicity. Getting ‘the basics’ right, to ensure staff knew when and where Schwartz Rounds were taking place, was often achieved through trial and error. Most project leads found they needed to take a multimodal approach, as not all staff will read an email, look at a poster, hear about Schwartz Rounds through word of mouth, or follow Local Authority social media accounts. Good publicity also meant telling people what Schwartz Rounds involve, so they knew what to expect from attending. A key enabler was the identification of relevant topics that could resonate with a wide range of people in different roles without being too emotionally over-whelming.
Several respondents identified as a barrier the challenge of finding people to be panellists. One interview respondent said this was ‘one of our biggest challenges to begin with…[finding people] who kind of fit the brief of a panellist…people who had a bit of gravitas, a bit of status within the Local Authority…people who had stories, who would grip people…and just getting people to volunteer for it’ (practice lead, Local Authority 8). Some people did not want to be panellists because of the pressure involved with speaking in front of a group of colleagues. Another issue was identified in relation to catering. Several respondents said this was an enabling factor because it made people feel valued, while others said it was barrier, because ‘its public funds being spent on lunch for staff, [and] that is a big issue for us particularly in the shadow of austerity’ (senior manager, Local Authority 5).
Some interview respondents also noted the importance of holding Schwartz Rounds at various times, to enable more people to attend. For example, one interview respondent said, ‘what we have learnt is that some people can find it a bit tiring to return to work after a Round, so we’ve got a couple of morning sessions in’ (practice lead, Local Authority 6). In this case, the Schwartz Round was held at the start of the day, so that people did not have to start work, then go to a Schwartz Round, and then come back to work. Other practical issues included how best to arrange the seating (for in-person Schwartz Rounds). In healthcare settings, panel members mostly sit at the front of the room with the audience in rows. Some interview respondents said this made their staff feel uncomfortable, so they tried other arrangements such as a horseshoe or more circular layout. One focus group respondent said this was not a trivial issue, because ‘people wanted to be able to make eye-contact’ with each other when they were talking (social worker, Local Authority 9).
Other enablers were identified in relation to facilitation and post-Schwartz Round support. For example, having facilitators who can coach panel members to tell a good story, provide psychological safety and containment, and manage silences. As one facilitator said, you need to ‘hold your own emotions as well, because I remember vividly…feeling quite [an] impact as a facilitator in terms of the emotion…I wasn’t expecting that level of emotion to pour out, and it poured out of all three of them in the same Round’ (Local Authority 7). Some interview respondents felt that having a social work background was helpful, because being a facilitator involves some similar communication skills. In general, focus group respondents commented positively on the skilfulness of their facilitators. One respondent said, ‘I did like the facilitators, [they] controlled what was…allowed to be said, and, and you were [able] to talk for yourself. You weren’t to offer solutions or to problem solve, I thought that was really good containment’ (social worker, Local Authority 10).
Respondents also identified the need for good aftercare. This could be a debriefing session for everyone at the end of the Schwartz Round, or something more individual. This was more evident in phase two, where some interview respondents worried about the nature of back-to-back online meetings, and people being alone in their homes, rather than in the office with colleagues. One Local Authority provided catering after the Schwartz Round instead of beforehand so that people could ‘have a bit of a debrief…because I think a lot of the time there's those thoughts and feelings that come up that are often sort of…quite unresolved at times’ (facilitator, Local Authority 8).
The synergy between Schwartz Rounds and social care organisations
When there was a perceived synergy between the values of Schwartz Rounds and those of the organisation, this was noted to be a key enabler. One interview respondent said, ‘We think [Schwartz Rounds] really fit…with some of the other things we are implementing, increased use of reflection, strengths-based practice, relationship-based practice’ (practice lead, Local Authority 6). In another Local Authority, an interview respondent said, ‘we’re trying to create a culture of sort of listening and support…and I think [Schwartz Rounds fit] in very well…we’ve got trauma-informed practice training…and certain aspects of signs of safety training, [and] appreciative inquiry, and whilst Schwartz is obviously different, it complements’ (senior manager, Local Authority 1).
Other respondents felt that Schwartz Rounds represented a departure from their typical approach to practice. For example, in a focus group one respondent said, ‘[Schwartz Rounds] were a space to hear other people's experiences and…be reflective and talk about how that made you feel [but] that's something I think as social workers we are not every good at. We’re good at talking very factual about things but we’re not talking about how things make you feel’ (social worker, Local Authority 10). In another Local Authority, some respondents identified a contradiction between Schwartz Rounds and their model of restorative practice with one interview respondent saying, ‘they’re doing two different things’ (supervisor, Local Authority 9).
Some respondents suggested more fundamentally that social care workers experience a different kind of trauma from healthcare workers, and this meant Schwartz Rounds would be less helpful for the former. For example, that there is a difference between the trauma one might experience from seeing an immediate physical injury and the kind of longer-term and less visible harm that social workers might observe from working with a family over many months or even years. As one focus group respondent said, ‘we see people again [and again] when they have other children, or more babies, so we never say goodbye. We end up seeing people as parents, as grandparents. I’ve seen grandparents. That's, that's the nature of the work we do’ (social worker, Local Authority 9). The same respondent also noted that social care workers are often dealing with historical trauma, about which they cannot do anything directly to help, but nonetheless need to know about – ‘The kind of things we get traumatised by [are] people dropping in deeply distressing information about their life, such as talking about historically sexual abuse for example’.
On a more operational level, some respondents identified a lack of fit between Schwartz Rounds and social care because of how work is allocated. As one interview respondent said, ‘there is something about the nature of work in social work that is different to health, in social work there is no cover if you’re not at work or if you take a few hours out’ (supervisor, Local Authority 9). Here, the respondent was suggesting that on a hospital ward, nurses can ‘cover’ one another's patients whereas in social care, you cannot cover each other's families. Others made similar points in relation to the unpredictability of social care, for example in relation to court and child protection work especially. No doubt healthcare also involves a degree of unpredictability, nonetheless these respondents understood such issues to be barriers within social care for the implementation of Schwartz Rounds.
Finally, several respondents wondered about the mix of attendees at Schwartz Rounds. For some, the openness of Schwartz Rounds was a key enabler (and benefit). One focus group respondent said, ‘[we’ve had] an incredibly diverse group…absolutely cross-directorate, and people did connect and relate, even though they’re from very different parts of, of the organisation’ (practice lead, Local Authority 2). Some were less convinced about these benefits and identified two main concerns – the relevance of Schwartz Rounds for administrative staff and the presence of senior managers. In some focus groups, respondents queried why administrators would attend. One respondent thought it might be harmful – ‘if you remember some of these people aren’t qualified social workers, like, like we are, where we’re used to supervision. These are admin, no offence, but they’re admin people, they’re not, they’re not trained in the way we are to deal with that emotional trauma, so I didn’t feel it was protective of my admin colleagues personally’ (social worker, Local Authority 9). However, a business support officer who attended Schwartz Rounds said in a focus group that, ‘Within my job, I do all the notetaking within the child protection conferences, so I listen on a daily basis to a lot of very sensitive and distressing information. That stays with me. And that's multiple times a week, every week, week in, week out. There are things built within our team to have a chat, but there's nothing formally based, and I think most people now have an accumulative effect of maybe many years of working within these arenas’ (Local Authority 7). Thus, although some respondents said they thought Schwartz Rounds would not be suitable for non-social workers, others felt differently, including at least some administrators.
In relation to senior managers, there was a similar divergence of views. Some managers felt uncomfortable attending Schwartz Rounds because ‘I don’t want my social workers to hear…lots of these things about me’ (supervisor, Local Authority 9). Others said they needed to maintain a certain image of being ‘calm, collected, [and] making quick decisions’, and attending Schwartz Rounds would mean acknowledging feeling ‘stressed, overwhelmed, [at times] on my knees, crying’. This could result in practitioners ‘not [having] faith in me and that's going to impact them’ (supervisor, Local Authority 9). Other managers found it helpful to attend Schwartz Rounds, saying the experience was ‘really powerful and [I’ve] reflected a lot’ (supervisor, Local Authority 6).
On the other hand, some practitioners said it was especially helpful to have managers attend. One focus group respondent said, ‘I quite liked to see that vulnerability, especially in [my manager] when he was talking, I’ve never seen him in that light before…and for me, it was like yeah, you’re a human, you’re not a machine…you’re still a leader but I actually quite liked that’ (social worker, Local Authority 9). Other respondents talked about the equalising nature of Schwartz Rounds and how they enabled colleagues to see one another as people first, rather than as ‘managers’ or ‘social workers’ or ‘administrators’. One interview respondent said, ‘people have seen that their managers have the same struggles that they do. Because I think before it was very much like you discuss with your own peer group how you may be feeling, but this is very much now people are talking about it, spanning different areas of the hierarchy’ (social worker, Local Authority 6). Other respondents disagreed and said that having senior managers present was a barrier, because they often reverted to problem-solving, which left some respondents feeling invalidated in terms of their own emotional and social responses to the work.
Organisational support and the wider context
When considering the influence of organisational and contextual factors, some respondents identified the importance of organisational ‘permission’ and support for staff to attend. As one focus group respondent said, ‘it kind of feels that the organisation needs to give permission…and say this is an important time and space’ (Local Authority 10). This ‘permission’ needed to be genuine, rather than something that is just written down in a policy. Sometimes this took the form of modelling: some senior managers made a point of attending as a way of encouraging others to attend, because ‘it's probably good PR if I go to them as well, and we do want to encourage people to attend’ (senior manager, Local Authority 6).
The flipside of organisational support might be organisational mistrust, which operated as a barrier in some places. Some respondents felt that Schwartz Rounds were just a ‘tick box exercise’ and wanted to know ‘Are they actually going to be a catalyst for something?’ (Local Authority 2). Thus, some respondents were sceptical about the reasons for having Schwartz Rounds and whether they would lead to any subsequent change to make things better for staff.
Survey results
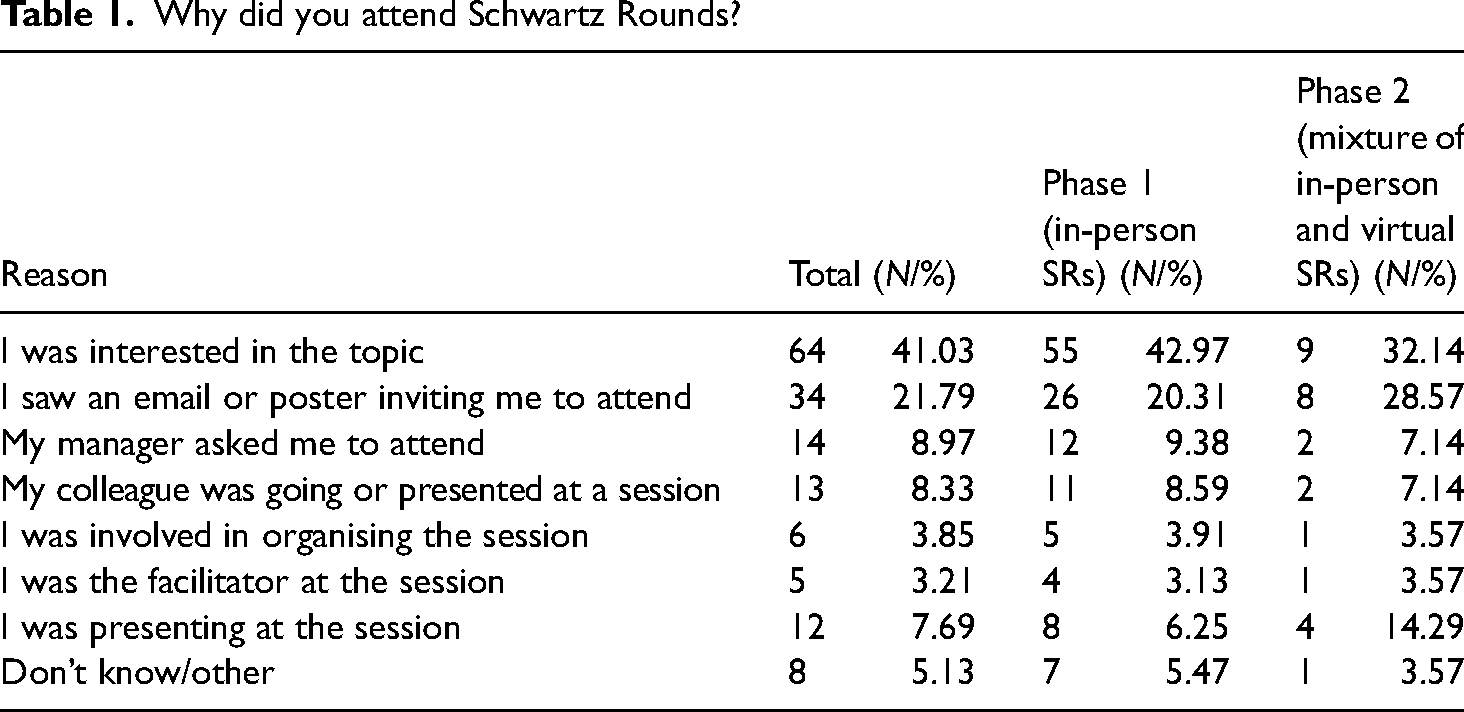
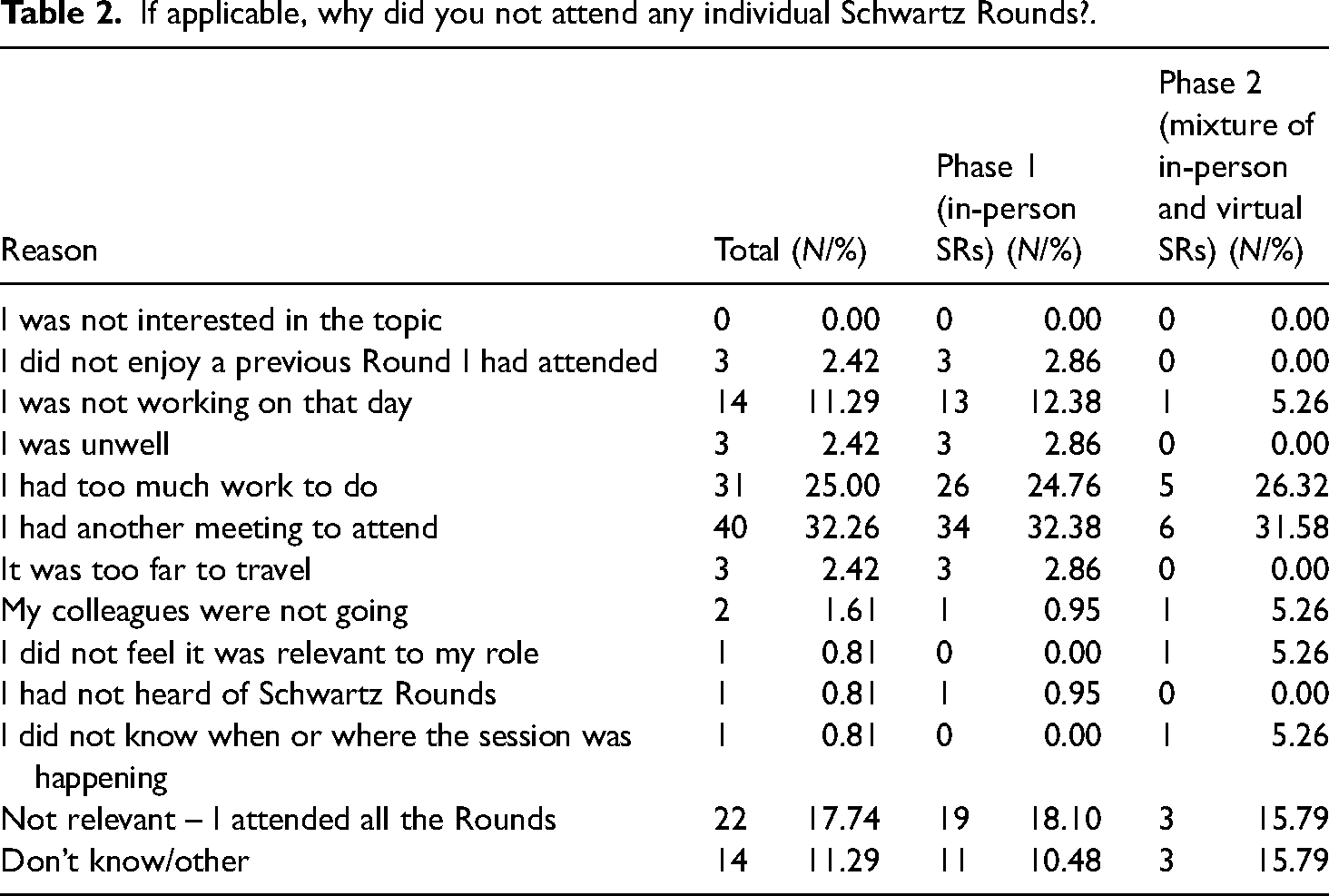
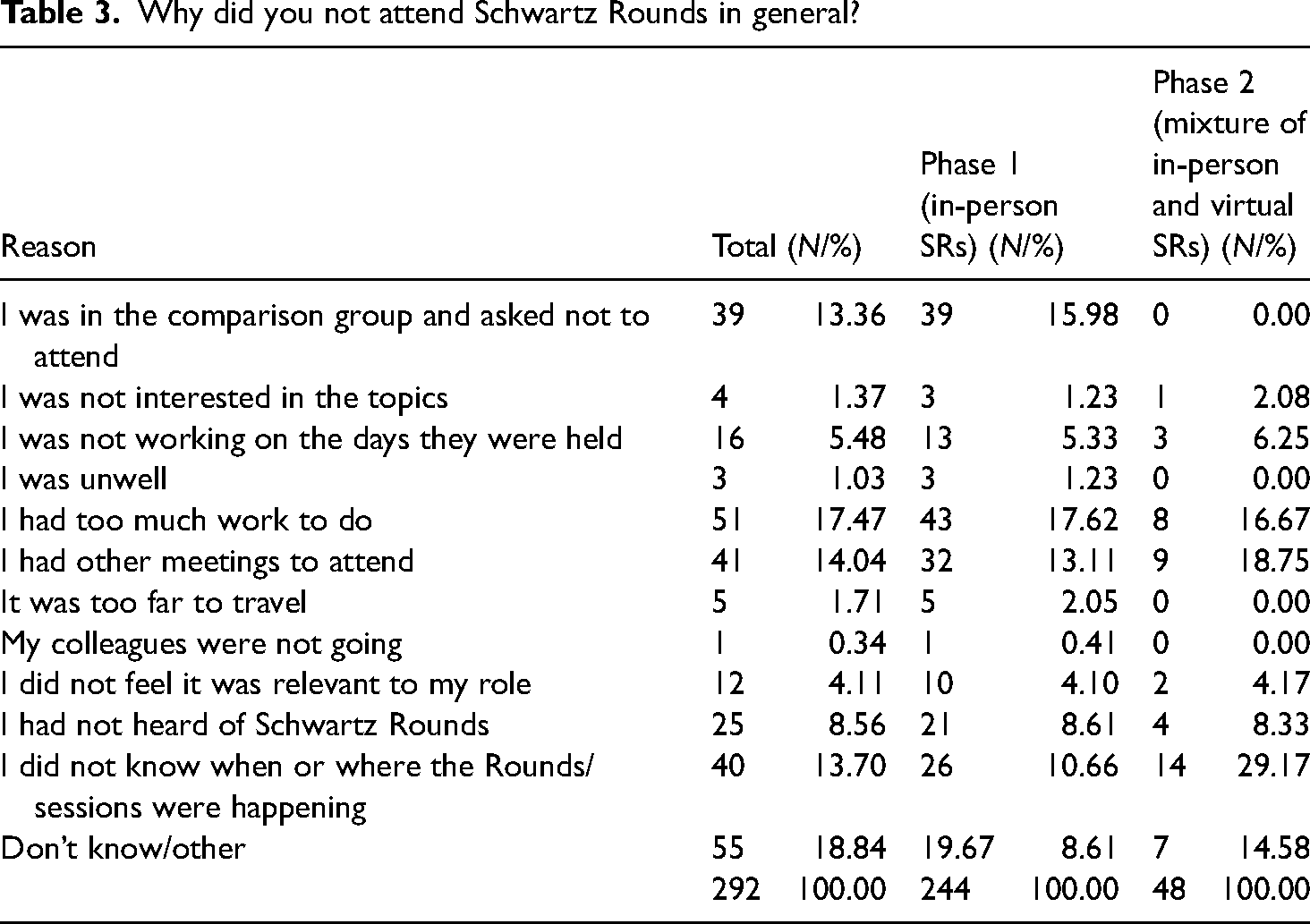
The most common reasons for attending Schwartz Rounds included interest in the topic and being invited (Table 1). The most common reasons for not attending are related to workloads and work patterns (Tables 2 and 3).
Why did you attend Schwartz Rounds?
If applicable, why did you not attend any individual Schwartz Rounds?.
Why did you not attend Schwartz Rounds in general?
An overview of the interview and focus group themes.
Discussion
The reasons why any complex intervention may be implemented successfully or unsuccessfully are themselves complicated and multifaceted (Bauer & Kirchner, 2020). Through our study, we have identified several key barriers and enablers for the provision of Schwartz Rounds in social care. Some of these are like those previously identified in relation to healthcare, while some are subtly or more obviously different.
Common enablers between healthcare and social care include (i) having a committed group of core staff, including an effective steering group, (ii) support from managers, both senior and less senior, (iii) good communication and publicity about Schwartz Rounds, including the benefits of attending, (iv) physically accessible Schwartz Rounds and (v) a good ‘fit’ between the wider culture of the organisation and the reflective nature of Schwartz Rounds. Common barriers include (i) high workloads and competing priorities, (ii) logistical difficulties in accessing Schwartz Rounds, (iii) less interesting and relevant topics, (iv) poor publicity, (v) insufficient staff to help implement and run Schwartz Rounds, (vi) a lack of support from managers and (vii) a poor ‘fit’ between the wider organisational culture and the reflective nature of Schwartz Rounds.
For some of these, despite their obvious similarities, they may operate with subtle differences between healthcare and social care settings. For example, many Local Authorities have teams and staff working across large geographical areas (much larger than any single hospital building). And while it is not always true that attending a Schwartz Round within a hospital is as easy as taking a lift from one floor to another, this is a specific barrier for some Local Authorities such that they will probably never be able to make a single Schwartz Round equally accessible for all staff. Likewise, although high workloads are a common barrier, at least in some healthcare settings it is possible to cover work between colleagues. This is not always the case in social care. While it may not make too much difference to a patient whether one nurse or another fits a canula, so long as it is done with care and technical skill, it matters a great deal to a child whether they are visited by a social worker they already know, or one who is ‘covering’ on behalf of a colleague. This may result in (even) less flexibility in social care, relative to some healthcare settings, and provides a different kind of barrier for attending Schwartz Rounds.
In addition to these common enablers and barriers between healthcare and social care settings, through our focus groups and interviews we also identified some distinctive enablers and barriers for social care – (i) a different experience of trauma, (ii) the challenges of a mixed audience, and (iii) the nature of practice models. Starting with the first of these, according to our respondents, the causes of secondary or vicarious trauma in social care are different compared to healthcare (Jenkins & Baird, 2002). For example, in healthcare you are more likely to encounter physical problems (including illness and injury), while in social care you are more likely to encounter emotional and behavioural problems (Michalopoulos & Aparicio, 2012). While this binary may not be entirely accurate – not least because many patients in healthcare settings will have mental health problems instead or as well as physical health problems – it is plausible that the nature of the work is different in some important ways. According to Cunningham (2003), vicarious trauma occurs more often for those working with sexual abuse than it does for those working with cancer. Then there is the longer-term nature of work in social care, at least in some cases. For example, child maltreatment can occur across two or more generations in the same family (Oliver, 1988), some mothers experience repeated child removals (Broadhurst et al., 2015) and a relatively high proportion of children in care, if they become parents themselves in later life, end up having their children removed (Roberts, 2016; Roberts et al., 2017). As suggested by some of our respondents, this may result in a particular experience of trauma (Khan, 1963), quite different from that experienced in healthcare. In relation to Schwartz Rounds, perhaps this means that while healthcare workers can reflect on specific incidents, social care workers find it harder to craft meaningful narratives to encapsulate and reflect their social and emotional experiences at work.
Another specific barrier in social care relates to the challenge of mixed audiences. While Schwartz Rounds were generally seen by our respondents as very suitable for social workers, there were mixed views in relation to administrators and managers. For the former, the question was straightforward – are Schwartz Rounds helpful or not? Some respondents said not, because of a perception that administrative staff are not directly involved in day-to-day work with children and families. For others, the inclusion of administrative staff was a real benefit, and served to acknowledge the emotional and social impact of social care work on everyone. It is notable that the respondents who said Schwartz Rounds were not suitable for administrative staff were not themselves in administrative roles, while several who were in such roles said how helpful they found it to attend. Indeed, one of the benefits of Schwartz Rounds is that they help people understand more about one another's roles, such that social workers could learn more about the social and emotional impact on administrative staff by attending Schwartz Rounds with them. In healthcare settings, administrative staff often attend Schwartz Rounds (Ng et al., 2023) and we have not seen any similar concerns raised. Likewise, some social workers raised concerns about managers attending Schwartz Rounds, and some managers felt uncomfortable expressing their ‘vulnerability’ in front of practitioners. Again, it is not uncommon for healthcare managers to attend Schwartz Rounds (Hughes et al., 2017), so the issue is not unique for social care. What may be different is the extent to which practitioners feel they are not trusted to do their jobs in social care without management oversight (Butler & Drakeford, 2005; Smith, 2001) and how expressions of emotional vulnerability may be interpreted as weakness (Corlett et al., 2019; Newcomb, 2021). A related issue is whether Schwartz Rounds should operate as a feedback mechanism for organisational change. In some Local Authorities, staff seemed to expect that they would. And yet, Schwartz Rounds are meant to provide counter-cultural reflective spaces. If they become a forum for problem-solving, this would represent a significant diversion from their underlying ethos. Thus, the presence of managers may be beneficial, in so far as it helps normalise the display of emotional and social vulnerability (Wolfensberger & Tullman, 1982) or undermining, if it prompts a cultural turn away from reflection and towards problem-solving.
Finally, there has been a trend in England since 2010 towards the use of defined social work practice models. Despite a general lack of evidence for their effectiveness, it is rare now to find a Local Authority without one (Isokuortti et al., 2020). Thus, while studies in healthcare have considered the synergy between Schwartz Rounds and existing organisational cultures, in social care the issue may be more complicated, or at least different. For Schwartz Rounds to be implemented effectively, the organisational culture in general should value reflection, but there may be an additional criterion for social care – namely, the perceived synergy between the Local Authority's practice model and Schwartz Round principles. For example, while the model of restorative practice places a heavy emphasis on reflection (Williams, 2019), it also includes other elements such as promoting a sense of community, removing barriers to participation, and shared accountability. While in our view, these aspects of restorative practice fit well with Schwartz Rounds, not all our respondents agreed. Thus, the Local Authority's practice model may present a barrier for the implementation of Schwartz Rounds if insufficient attention is given to showing how they relate to one another.
Implications for the implementation of Schwartz Rounds in children's social care
Given our findings and the unique challenges and differences between healthcare and social care settings, in this final part of the discussion we provide some high-level comments in relation to adaptation and implementation. In relation to practice, it is important that social care organisations tailor the provision of Rounds to address the specific emotional and social challenges faced by social care professionals, considering the distinct nature of trauma and the relational complexities inherent in social work with children and families. Efforts should be made to ensure that Schwartz Rounds are accessible and relevant to all staff members, including those in administrative roles, by selecting themes that resonate across different job functions and by facilitating sessions in a way that values all contributions. Given the critical role of facilitators, investing in specialised training that equips them to navigate the unique dynamics of social care settings will also help enhance the effectiveness of Schwartz Rounds. In relation to policy, senior managers need to explicitly recognise and demonstrate the value of interventions like Schwartz Rounds for improving staff well-being and retention. In addition, policy guidance should help staff understand how Schwartz Rounds complement and enhance existing models of practice.
Limitations of the study
The present study is marked by several inherent limitations that merit careful consideration when interpreting the findings. First, we have to some extent a self-selected sample, meaning it may not be representative of the broader population under investigation. This introduces potential selection bias, limiting the generalisability of the study's conclusions. Second, the variability in participant responses poses a challenge to the internal validity of the study. Notably, participants were afforded the option to abstain from specific survey items, leading to a disparate response rate across different questions. This variance, possibly exacerbated by survey fatigue, introduces uncertainty regarding the comprehensive nature of the data and complicates the synthesis of meaningful patterns. Furthermore, the study encountered inconsistent sample sizes across various local authorities, independent of their actual demographic proportions and the size of their organisation. And finally, it is imperative to again acknowledge that the study was conducted, at least partially, against the backdrop of the COVID-19 pandemic and associated lockdowns in the UK. Although the precise influence of these unprecedented circumstances on the study remains elusive, the potential for a significant impact cannot be discounted. Consequently, interpretations should be made with caution, recognising the multifaceted contextual influences that may have shaped participant responses during this extraordinary period.
Conclusion
Following our previous evaluation of Schwartz Rounds, we concluded that ‘[there are] signs of promise in relation to the use of Schwartz Rounds in children's services, especially for regular attendees…the intervention is relatively inexpensive… [and benefits may include] lower psychological distress and fewer sickness-related absences from work [and] improved subjective wellbeing and relationships with colleagues’ (Wilkins et al., 2023). The contribution of this article does not strengthen or challenge this conclusion. However, we have sought to explore in greater depth the barriers and enablers for implanting Schwartz Rounds in social care. All responsible social care organisations take seriously the challenge of staff welfare, and while no single approach will work for everyone, there is evidence that organisational-level interventions may be more effective than individual-level interventions (Turley et al., 2020). As such, Schwartz Rounds may represent a potentially promising intervention for social care, especially if the contextual differences with healthcare settings are given due attention.
Footnotes
Ethical approval
Ethical approval for this project was given by the School of Social Sciences at Cardiff University (SREC/3170).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Foundations (formerly What Work's for Children's Social Care). CASCADE research centre is supported by infrastructure funding from Health and Care Research Wales.
Declarations of Conflict of Interests
The authors declare that there is no conflict of interest.
Authors’ contributions
DW wrote the first draft of the article, with subsequent and significant input from ST, RJ, ZB and VB. ST, RJ and ZB collected most of the data. VB provided statistical expertise and help with quantitative analysis and DW led the overall study.