
Abstract
Summary
Mindfulness and cognitive training interventions are promising models to address impacts (e.g., anxiety and stress) of cognitive impairment among older adults. Combining strategies may yield better outcomes than models offered in isolation. However, there are numerous uncertainties about these interventions, potential for combination, and implementation. Social workers are well placed to offer these interventions.
Findings
From an initial search of 3,538 records, 13 studies were included in the final review. Mindfulness studies focused on stress reduction or cognitive behavioral therapy. Cognitive training studies applied stimulation or activity approaches. Results indicate that the field is still emerging, as most studies were pilot or feasibility trials. A combination of mindfulness-based stress reduction and brain training activities may offer the most promising model for older adults with cognitive impairment, based on outcome assessments and other factors. A common limitation among the reports was detailed on engaging older adults with cognitive challenges in the design and implementation of these interventions.
Applications
This realist review deepens the understanding of how, why, for whom, and in what circumstances a combination of mindfulness and cognitive training could be most successful for social workers to address intersecting cognitive and aging needs of older adults. Building evidence on combining mindfulness-based stress reduction and brain training activities among older adults with cognitive impairment could yield promising results, and this review identifies implementation considerations. The review also found a need for psychometric scale development on the benefits of brain training activities.
Background
Aging
Industrialized countries worldwide are experiencing significant proportions of their populations aging into geriatric years and living longer—on average—than any previous generation on record (Kirkwood, 2017; Klenk et al., 2016). Increased life expectancy may be attributable to advances in medicine and healthcare (Mathers et al., 2014). Using Canada as an example, it is predicted that 25% of the total population will be aged 65 or older by 2031 (Statistics Canada, 2005). Predictive models show that the general aging population in Canada will face fewer disabilities compared to prior generations (Public Health Agency of Canada (PHAC), 2007). However, it is also predicted that the majority of seniors will live with at least one chronic disease or condition for a substantial length of time—potentially decades (PHAC, 2007; PHAC, 2010). Among these conditions (e.g., frailty, pain, diabetes, etc.), cognitive impairments are currently highly prevalent in Canadian seniors and are expected to increase in prevalence as a substantial proportion of the Canadian population continues to age into their geriatric years (PHAC, 2010; Pottie et al., 2016).
Cognitive impairments
Cognitive impairments are difficult to address with drug interventions (Lee et al., 2013; Manly et al., 2008). Attempts to reverse impairment biomedically have largely been unsuccessful, and medication—at best—seems able only to slow or delay loss of cognitive ability in older adults (Doody et al., 2009; Feldman et al., 2007). Challenges to cognitive function may be some of the most difficult geriatric comorbidities to live with (Albert et al., 2011). Individuals with cognitive impairment report severe stress, anxiety, and other negative psychosocial impacts due to a loss of mental acuity, stigma or discrimination from others about cognitive performance, and strained interactions with friends and family (Portacolone et al., 2018). As cognitive impairments, by and large, contribute to mortality over a significantly longer period of time than other geriatric comorbidities (Ganguli et al., 2005; Ravi, 2011) and given their current and impending frequency in a substantial proportion of the aging population, strategies to alleviate negative psychosocial impacts are urgently needed (Johnston & Narayanasamy, 2016).
Therapies for intersecting cognitive and aging needs
Counseling or talk therapy (i.e., focused discussion on a health or social issue between a service provider and client(s) for one or more sessions in individual or group formats) can be especially helpful for young and middle-aged adults to address issues and improve their situation (Swartz & Swanson, 2015). For older adults with cognitive impairment, however, talk therapy may be more useful when complemented by activity-based therapies, which involve non-verbal tasks and practices such as worksheets, meditation, games, etc. (Juang et al., 2017; O’Rourke et al., 2018). Such activity-based therapies for people with cognitive impairment are often labeled as “cognitive remediation therapies” as their primary purpose is to help people manage symptoms and effects of cognitive decline by teaching compensatory strategies that can help individuals cope better in their daily lives (Eaton et al., 2022; Eaton et al., 2019; Eaton et al., 2017; Fan et al., 2017)
Further, group therapies have been recommended over one-on-one interactions by this population (Eaton et al., 2017; Fan et al., 2017). Groups have the inherent ability of bringing together people who share a condition or issue (Schiff & Bargal, 2000), and this gathering may be particularly helpful for older adults with cognitive impairment who may feel isolated or as if they are alone in their experiences and struggles (O’Rourke et al., 2018). Activity-based or cognitive remediation therapies that have recently been tested to address the effects of aging with cognitive impairment in older adults can be placed in two categories: (a) mindfulness, a therapeutic approach to cultivate calmness, and (b) cognitive training, a set of activities, stimulation, or games designed for people to practice in domains of cognition, such as memory or speed of processing (Lenze & Bowie, 2018; Wong et al., 2017a).
Mindfulness and cognitive training therapies
Mindfulness and cognitive training therapies (i.e., mind–body therapies) are activity-based therapies that involve non-verbal practices, such as meditation for mindfulness and memory recall games for cognitive training. Mind–body therapies are emerging as promising strategies to address the effects of cognitive impairment in older adults, with groups emerging as the ideal format of service delivery (Russell-Williams et al., 2018; Tappen & Hain, 2014). Evidence is also emerging that combining mind–body therapy models may yield better outcomes than single-technique strategies (Ramirez-Garcia et al., 2019). Social work, as a regulated health profession with expertise in mindfulness and cognitive training models and on the frontlines of psychosocial geriatric support and care, may also contain the ideal facilitators of such interventions (Wong et al., 2017b). However, there is a literature gap regarding the implementation factors of these interventions (Birnbaum & Birnbaum, 2008) and their possible combination for social workers to support the intersecting cognitive and aging needs of older adults (Vance et al., 2022).
Realist review rationale
Selecting interventions to test in a study can be one of the most complicated aspects of intervention research, involving numerous factors (Zipfel et al., 2020). These factors include extant literature on the intervention's application in prior studies, outcomes of those studies, the population in the present study, and contextual factors (such as location) for the present study (Zipfel et al., 2020). Interventions that have been extensively researched in substantive samples are frequently summarized into systematic reviews and meta-analyses, and interventions that are more emerging are often synthesized in scoping reviews (Munn et al., 2018). When the extant literature is not substantive enough for a systematic or scoping review, or when contextual factors may be especially important for intervention selection, a realist review may be the suitable option (Cooper et al., 2017).
Realist reviews are a relatively new method of synthesis, compared to systematic and scoping reviews (Pawson et al., 2005). Realist reviews are specifically focused on interventions, and the realist perspective is based on two key assumptions. First, there is no single intervention for any population or issue that will be ideal in every case (Cooper et al., 2017; Pawson et al., 2005). Previous research should be synthesized, but contextual and circumstantial factors (such as healthcare structure) are equally important (Pawson et al., 2005; Pearson et al., 2015). Second, realist evaluations put less emphasis on measurement and outcomes than systematic and scoping reviews (Pearson et al., 2015). Outcome reporting can be biased, mixed, or conflicting, and the implementation factors (e.g., population, intervention schedule, setting, etc.) should be considered alongside outcomes to understand why an intervention did or did not work (Pawson et al., 2005). A realist review may be the most suitable form of review in this instance for three reasons. First, mind–body intervention studies with older adults are predominantly small pilots where meta-analyses are not possible (Morone & Greco, 2007). Second, there are numerous types of mindfulness and cognitive therapies that have not yet been synthesized to consider the best fit for this population (Kotecki et al., 2015). Third, the health system in industrialized countries is able to implement mind–body strategies for older adults in long-term care and assisted living settings (Capezuti et al., 2018). As such, a realist review was chosen due to its ability to synthesize small studies and consider the circumstances (how, why, for whom, and when) under which these interventions may be most beneficial (Pawson et al., 2005).
Methods
This realist review follows guidelines (Cooper et al., 2017; Pearson et al., 2015) for this method of synthesizing multiple types of interventions, including how they could be combined. As such, a search and synthesis strategy was employed to answer the following research questions:
What types of and how have mindfulness interventions been used by social workers to address intersecting cognitive and aging needs of older adults, and who (i.e., demographics) What types of and how have cognitive training interventions been used by social workers to address intersecting cognitive and aging needs of older adults, and who within this population participated?
The discussion then addresses how promising types of mindfulness and cognitive training can be combined by social workers to address intersecting cognitive and aging needs of older adults.
Search strategy
Realist review guidelines recommend multiple preliminary database search attempts to refine a final database search, followed by searching relevant professional networks and works in progress (Cooper et al., 2017; Pearson et al., 2015). Preliminary searches for mindfulness and cognitive training interventions for social work to address intersecting cognitive and aging included syntax that was very specific. Examples of this included therapy terms like “meditation” and “brain games” alongside diagnostic terms such as “dementia.” These searches yielded too few results (often 50 to 60), with relevant articles known to the screeners missing from the search. Broader preliminary searches that included the therapy types but little reference to the social work profession or population of older adults yielded too many results (often in the tens of thousands). This preliminary search process resulted in a final search on January 30, 2020, of the following search syntax: “Mindfulness” OR [“Cognitive Train*” OR “Brain Train*”] AND “Social Work*” AND “Cognit*” AND [“Older” OR “Geriatric” OR “Gerontology” OR “Senior*” OR “Aging”]. This syntax was entered into the University of Toronto Libraries search portal, which simultaneously searches Ovid, ProQuest, PubMed, Scopus, and Web of Science databases, and returned 3,536 unique results. While this is still a substantial number for screening, the availability of a screening software and the screeners’ concerns of missing key articles contributed to the decision to use this search as the basis for this realist review.
Screening
The search results were imported into Covidence screening software. Two screeners (both social workers, including the first author) contacted their professional networks and conducted an additional hand search of recently published articles, resulting in two more papers being included. The two screeners (both social workers) then independently read the resulting titles and abstracts with the screening criteria of (a) primary intervention studies, (b) mindfulness or cognitive training, (c) participants were older adults, (d) study addressed effects of cognitive impairment, and (e) study was led by a social worker and/or intervention(s) were delivered by social workers. The two screeners independently identified 14 and 13 studies, respectfully, for full-text screening. Titles and abstract screening exclusions were that 41% of articles tested an intervention for friends, family, and/or caregivers of older adults with cognitive impairment, 23% tested an intervention for children or young adults with cognitive impairments, 20% tested an intervention outside the scope of this review (predominantly art or music therapy), and 16% were non-primary (i.e., commentaries or reflective pieces of these types of therapy). Following full-text review, the two screeners agreed upon 13 studies (of 14 total or 92.9% consensus) for the final inclusion in this realist review. One study excluded during full-text review appeared to be cognitive training at title and abstract screening; however the full text illuminated that it was instead cognitive behavioral therapy (CBT), which is beyond the scope of this review (Hallis et al., 2016). Refer to Figure 1 for the screening flowchart, which lists the pre-determined reasons for exclusion (e.g., not for older adults, not a primary intervention study) alongside numbers of articles excluded for each reason.
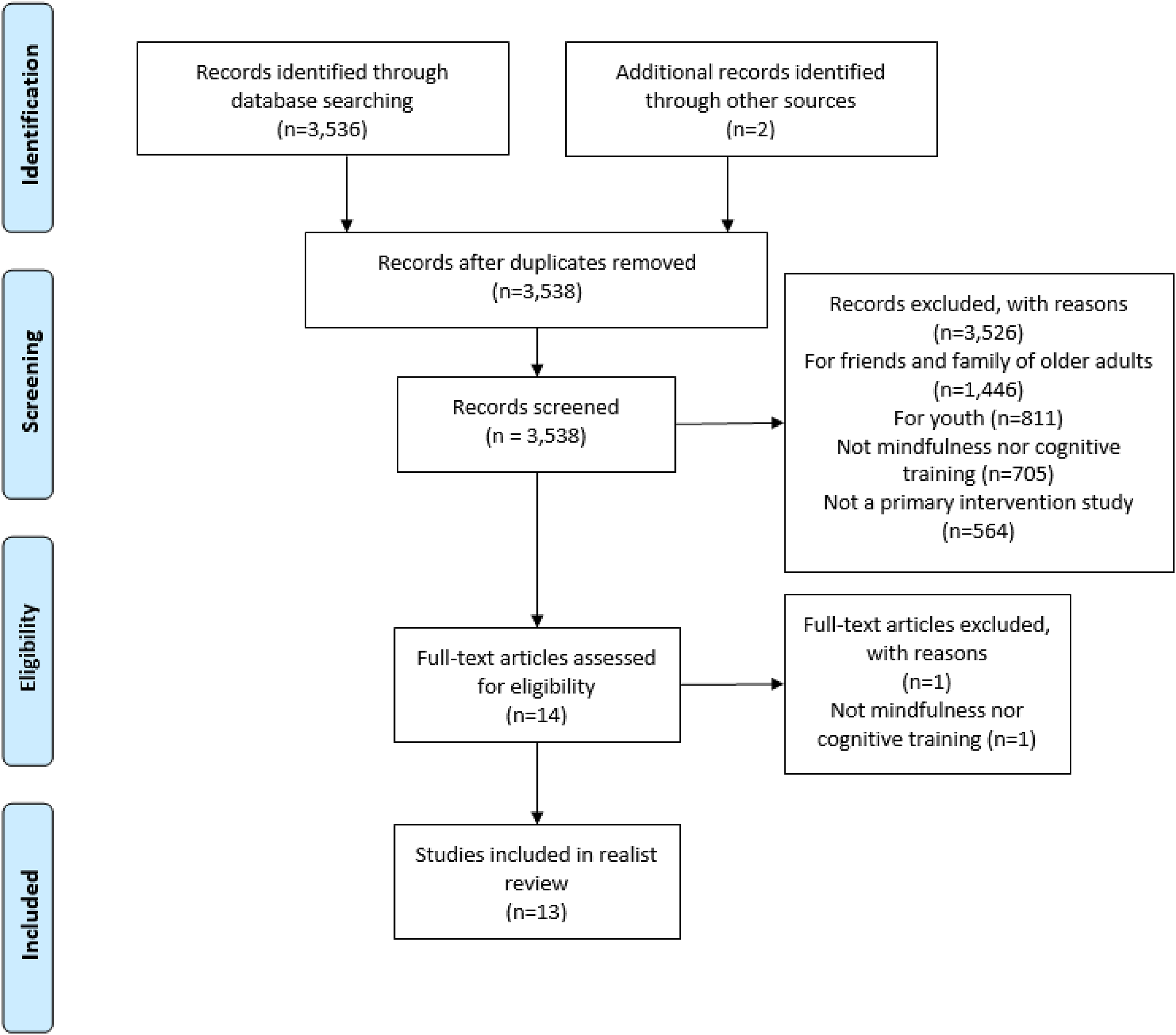
Screening flowchart.
Data analysis
As the purpose of this realist review is to synthesize mindfulness and cognitive training interventions for older adults with cognitive impairment, and to consider combining certain types of these strategies and methods of implementation, multiple phases of data analysis were necessary (Pawson et al., 2005). Initially, the first author organized the 13 studies into mindfulness and cognitive training categories to delineate specific types of each intervention category. This comprises the two subsections of the results section. The first author then used this synthesis, alongside further consideration of the full-text source material to extract considerations for combination and implementation, which comprises the discussion. A draft of this analysis and discussion was reviewed by the second screener, who had read the full text of the included studies and confirmed its accuracy of synthesis and appropriateness of conclusions.
Results
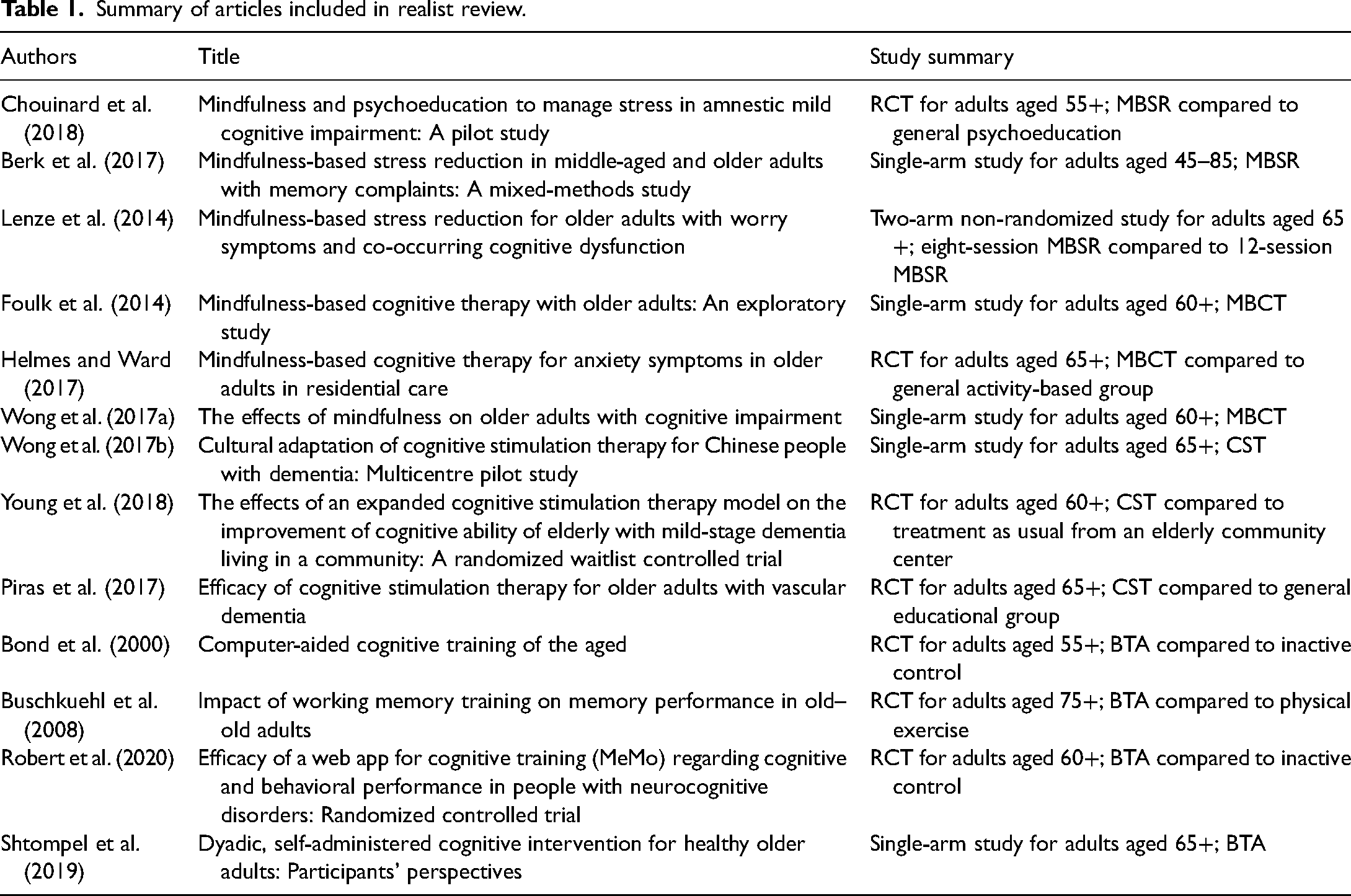
As mentioned above, the results section is split into two subsections. The first subsection addresses the first research question regarding types of mindfulness, and the second subsection addresses the second research question regarding types of cognitive training interventions used to address the intersecting cognitive and aging needs of older adults. Each subsection follows realist evaluation guidelines (Pawson et al., 2005) of presenting implementation factors (such as eligibility criteria, setting, and intervention schedule) alongside outcome reporting and concluding with synthesized facilitators and barriers of each intervention subtype. Table 1 provides further detail on the 13 studies reviewed below.
Summary of articles included in realist review.
Mindfulness therapies
Mindfulness therapies reviewed are organized into two types that have been commonly agreed upon within the field (Shapero et al., 2018): (a) mindfulness-based stress reduction (MBSR) and (b) mindfulness-based cognitive therapy (MBCT). Other mindfulness-based interventions (MBIs) also exist, but they are beyond this review's scope as discussed in the limitations section. Mindfulness meditation is a centuries-old practice. The notion of “mindfulness therapy” is a more modern construct, manualized and popularized by Dr. Jon Kabat-Zinn and colleagues in the late 20th century (Kabat-Zinn, 1990; Shapero et al., 2018).
Mindfulness-based stress reduction (MBSR)
MBSR was the first mindfulness therapy to be created and manualized by Kabat-Zinn et al. (2017) and was originally developed for the treatment of chronic pain. Studies included in this review tested MBSR to manage stress (Chouinard et al., 2018) and anxiety (Berk et al., 2017; Lenze et al., 2014) for older adults with cognitive concerns. These studies were offered to participants aged 45–85 (Berk et al., 2017), 55+ (Chouinard et al., 2018), and 65+ (Lenze et al., 2014). Cognitive concerns were diagnosed mild Alzheimer's disease (Chouinard et al., 2018) and self-report (Berk et al., 2017; Lenze et al., 2014).
All studies followed the MBSR curriculum (Kabat-Zinn et al., 2017) of an orientation plus eight 2.5-h weekly sessions with an hour of homework each week (Berk et al., 2017; Chouinard et al., 2018) with one study testing the eight-session model against a 12-session one (Lenze et al., 2014). Samples consisted of 13 (Berk et al., 2017), 34 (Lenze et al., 2014), and 48 (Chouinard et al., 2018) participants. One study was uncontrolled, and the other two compared manualized eight-session MBSR to 12-session MBSR or general psychoeducation on living with cognitive impairments (Berk et al., 2017; Chouinard et al., 2018; Lenze et al., 2014).
As these studies were pilots in nature, feasibility (i.e., proportions of recruitment and attendance), acceptability (i.e., satisfaction scale), and fidelity (i.e., ratings of video-recorded sessions or clinician reports) were primary and secondary outcomes
Recruitment proportions averaged 40% (range: 34–47%), with completion rates averaging 85% (range: 79–91%), and acceptability and fidelity findings were consistently favorable (Berk et al., 2017; Chouinard et al., 2018; Lenze et al., 2014). The small samples from these pilots limited their statistical analyses; however, eight-session manualized MBSR appeared to have a positive effect on psychosocial outcomes in all studies, and more so than controls where available (Berk et al., 2017; Chouinard et al., 2018; Lenze et al., 2014). A common difficulty among these studies was that while that MBSR positively changed stress and anxiety regarding cognition, scores on self-reported cognitive ability and performance were insignificant or unchanged (Berk et al., 2017; Chouinard et al., 2018; Lenze et al., 2014).
Mindfulness-based cognitive therapy (MBCT)
MBCT is a mindfulness therapy that combines Kabat-Zinn's mindfulness techniques with Beck's (1964; 1991) cognitive behavioral therapy (CBT) and was initially created as a prevention program for depression relapse (Segal et al., 2002). This review includes MBCT's effects on anxiety (Foulk et al., 2014; Helmes & Ward, 2017) and psychological health (Wong et al., 2017a) related to cognitive impairment. People aged 60+ (Foulk et al., 2014; Wong et al., 2017a) and 65+ (Helmes & Ward, 2017) were eligible to participate. Concerns with cognition were assessed through a diagnosis of mild cognitive impairment (Wong et al., 2017a) and via the mini-mental state examination or MMSE (Foulk et al., 2014; Helmes & Ward, 2017). The MMSE has moderate sensitivity (79%) and high specificity (95%) with test–retest reliability of 0.80 to 0.95 (Baek et al., 2016; Marioni et al., 2011).
The first edition of the MBCT manual (Segal et al., 2002)-which does not include the new 6-h retreat to the current edition (Segal et al., 2013)-comprised of an orientation session plus eight weekly 1.5-h group sessions, and 30–40 min of homework per week, was followed in all three studies (Foulk et al., 2014; Helmes & Ward, 2017; Wong et al., 2017a). The number of participants was 14 (Wong et al., 2017a), 50 (Foulk et al., 2014), and 52 (Helmes & Ward, 2017). One study was controlled by a structured activity program (Helmes & Ward, 2017); the other two studies were single-arm (Foulk et al., 2014; Wong et al., 2017a).
Similar to the MBSR pilots, these studies primarily assessed feasibility and acceptability; however, fidelity was not assessed, and only one study reported recruitment proportions (58%; Helmes & Ward, 2017) with the other studies claiming community recruitment as the reason these numbers were not reported (Foulk et al., 2014; Wong et al., 2017a).
Completion rates averaged 84% (range: 74–92%) with some participants withdrawing from the study due to not finding MBCT helpful for their symptoms associated with cognitive impairment or finding the intervention overwhelming (Foulk et al., 2014). Non-parametric Wilcoxon tests were run into studies to assess exploratory outcomes in these small samples (Foulk et al., 2014; Helmes & Ward, 2017) with the third study using analyses of variance (Wong et al., 2017a). Two of the three studies reported significant positive changes in anxiety compared to control (Foulk et al., 2014; Helmes & Ward, 2017) with one study claiming improvement in both anxiety and cognitive function (Wong et al., 2017a). Common implementation benefits of MBCT for this population were the peer support from the group format (Foulk et al., 2014; Wong et al., 2017a) and setting the groups in facilities that participants accessed on a regular basis (Foulk et al., 2014; Helmes & Ward, 2017). Downsides of implementing MBCT for older adults included the intensive focus on change processes (Wong et al., 2017a) that resulted in some attrition (Foulk et al., 2014).
Cognitive training therapies
Cognitive training therapies included in this review are divided into two commonly accepted types (Bahar-Fuchs et al., 2013; Orgeta et al., 2015): (a) cognitive stimulation therapy (CST) and (b) brain training activities (BTA).
Cognitive stimulation therapy (CST)
Cognitive stimulation therapy (CST) is a manualized group intervention (Spector et al., 2006) that involves non-pharmacological stimulation of specific domains or global cognitive and social functioning. Reviewed studies evaluated the efficacy of CST in improving cognitive functioning of older adults with mild cognitive impairment (Young et al., 2018; Wong et al., 2017b) and vascular dementia (Piras et al., 2017). These studies were offered to people aged 60+ in the community (Young et al., 2018) and to people aged 65+ in assisted living facilities (Piras et al., 2017; Wong et al., 2017b).
Two of these studies followed the CST curriculum (Spector et al., 2006) of 14 twice weekly 45-min sessions (Piras et al., 2017; Wong et al., 2017b) with one study adding twice weekly tai chi to the intervention regimen (Young et al., 2018). Participants numbered 30 (Wong et al., 2017), 56 (Piras et al., 2017), and 101 (Young et al., 2018). Two studies were controlled via a waitlist (Young et al., 2018) and a reading and discussion group (Piras et al., 2017), and one study was uncontrolled (Wong et al., 2017).
The exploratory nature of these investigations resulted in assessment of outcomes of cognitive functioning via the mini-mental state examination (MMSE) and quality of life and mood through a variety of measures, with a limited detail on rates of participation and satisfaction (Piras et al., 2017; Wong et al., 2017b; Young et al., 2018).
One study reports a recruitment proportion of 53% with 91% completion rate (Young et al., 2018). The two controlled studies found the majority of CST participants significantly improved on the MMSE compared to waitlist (Piras et al., 2017; Young et al., 2018). The uncontrolled study found 23% improved on the MMSE (Wong et al., 2017b). Quality of life and mood changes were insignificant when compared to controls and within groups (Piras et al., 2017; Wong et al., 2017b Young et al., 2018). Group discussion and skilled facilitators were identified as facilitative factors of CST (Wong et al., 2017b; Young et al., 2018) with a lack of emotional coping strategies identified as a possible reason for insignificant impact on quality of life and mood outcomes (Piras et al., 2017).
Brain training activities (BTA)
Brain training activities (BTA) are games or activities that can be completed on paper and that are increasingly being computerized into software and mobile applications (Bahar-Fuchs et al., 2013). Practicing BTA for a minimum of 2 hours per week for a minimum of 8 weeks has resulted in a self-reported positive change in coping (Vance et al., 2018), although there is a variation to this with improved performance on the MMSE (Bahar-Fuchs et al., 2013). This review found studies that tested computerized cognitive training in individual (Bond et al., 2000; Robert et al., 2020) and group (Buschkuehl et al., 2008) formats and one that tested paper-and-pencil training in dyads (Shtompel et al., 2019) for people living with cognitive impairments. Ages of participants were 55+ (Bond et al., 2000), 60+ (Robert et al., 2020), 65+ (Shtompel et al., 2019), and 75+ (Buschkuehl et al., 2008). Criteria of cognitive impairment included the MMSE (Bond et al., 2000), mild or major neurocognitive disorders (Robert et al., 2020), and neuropsychological assessment (Buschkuehl et al., 2008; Shtompel et al., 2019).
Cognitive training regimens in all four studies lasted 12 weeks, with slight differences in weekly practice varying from two to four sessions per week at 20 to 45 min per week, with no study prescribing more than 2 hours of practice in a given week (Bond et al., 2000; Buschkuehl et al., 2008; Robert et al., 2020; Shtompel et al., 2019). Sample sizes were 46 (Robert et al., 2020), 39 (Buschkuehl et al., 2008), 14, (Bond et al., 2000), and 11 (Shtompel et al., 2019). Control groups were: inactive (Robert et al., 2020); conversation sessions that mimicked the length and frequency of cognitive training (Bond et al., 2000); physical exercise (Buschkuehl et al., 2008); and non-existent (Shtompel et al., 2019).
Implementation outcomes of participation and acceptability of the intervention format were assessed alongside change in cognitive function and ability, with non-parametric Wilcoxon tests used due to small sample sizes (Buschkuehl et al., 2008; Robert et al., 2020).
Completion rates averaged 56% (range: 48–64%) in three studies (Buschkuehl et al., 2008; Robert et al., 2020; Shtompel et al., 2019) with one study only reporting the number of completers (Bond et al., 2000). Overall, BTA participants showed significantly greater improvements on the MMSE and other measures of cognitive function compared to controls, with particularly marked improvement in domains of visual memory, attention, and speed of processing (Buschkuehl et al., 2008; Robert et al., 2020; Shtompel et al., 2019). Accessibility and usability of BTA was expressed by participants as factors that facilitated their participation (Robert et al., 2020; Shtompel et al., 2019). Pitfalls in these studies included initial hesitancy to use new technology (Bond et al., 2000; Robert et al., 2020) and difficulty retaining participants in a relatively passive (i.e., app or computer-installed software) intervention (Buschkuehl et al., 2008; Robert et al., 2020).
Discussion
The results above summarize the realist evaluation components (how, why, for whom, and in what circumstances) of 13 mindfulness and cognitive training studies involving social workers to address challenges associated with cognitive impairment among older adults. These results demonstrate that this field is still emerging, as only seven studies were RCTs and all studies had fairly limited samples with primary outcomes of feasibility and acceptability rather than making efficacy or effectiveness. The paucity of this literature demonstrates that a realist review may be the only method of synthesis, as extant studies are too few and limited for a systematic or scoping review (Munn et al., 2018). A commonality across these studies was that the interventions were chosen due to contextual factors, examples of which are the host site having social workers trained in the chosen therapy model (Young et al., 2018) and the research team having conducted preliminary work on the therapy type (Wong et al., 2017b).
A realist review was possibly the ideal method of synthesis of these studies as they differed with respect to design, entry criteria, and outcomes. However, studies within a single intervention category were frequently consistent on intervention structure and schedule, such as identically structured CST (Wong et al., 2017b; Young et al., 2018). Such consistency allowed for facilitators and barriers of each intervention type to be synthesized at the end of each results subsection.
This review identified a robust outcome measure to assess the use and benefits of mindfulness activities, as the Five Facet Mindfulness Questionnaire (FFMQ) and its short form (FFMQ-SF) have both been validated across numerous MBSR and MBCT studies (Berk et al., 2017; Chouinard et al., 2018; Foulk et al., 2014; Helmes & Ward, 2017; Lenze et al., 2014; Wong et al., 2017a). Yet a similar measure to assess the use and benefits of cognitive training appears to be missing. The CST and BTA studies reviewed exported user data from the cognitive training software (Bond et al., 2000; Buschkuehl et al., 2008; Piras et al., 2017; Robert et al., 2020; Wong et al., 2017b; Young et al., 2018). This may be sufficient for pilot studies, where a Likert-style measure akin to the FFMQ is at risk of being underpowered, but a more definitive study of cognitive training would benefit from a more sophisticated measure of cognitive training's uptake and benefits than solely exporting metrics (such as number of hours used) from participant's software licenses.
Absent from these reports was detail on engaging older adults with cognitive challenges in the design and implementation of these interventions. One study detailed a workshop of 105 healthcare workers (Wong et al., 2017a); however, none of the 13 studies state that members of their target population were engaged in any manner outside of participating in the interventions. As community engagement is becoming an area of increasing priority in health and social science research (Holzer et al., 2014; Reynolds & Sariola, 2018), and as the studies reviewed were contextual in nature (i.e., choosing interventions based on the host site or team's capacity), the lack of patient engagement is surprising.
Overall, the MBSR and BTA studies had a stronger quality of evidence compared to MBCT and CST studies as more of the MBSR and BTA reports contained a comparator (and more contained an active comparator as opposed to an inactive control group) and had larger samples and better completion proportions. Further, there were fewer instances of the studies’ first author facilitating the interventions in the MBSR and BTA studies compared to the MBCT and CST studies, which partly mitigates the risk of reporting bias.
Combining mindfulness and cognitive training
The first consideration to combining mindfulness and cognitive training strategies is which types of each therapy to combine. Cognitive impairment may a constant stressor in people's lives, which activity-based therapy could help ameliorate by building coping skills rather than a problem that can be resolved through changing thought patterns, which suggests MBSR with its focus on stress reduction would be preferable to MBCT with its focus on change (Shapero et al., 2018; Wong et al., 2017a). Further, studies reviewed showed more favorable results for MBSR than MBCT with some participants withdrawing from MBCT due to the intervention's intensity and focus on change (Foulk et al., 2014). CST and BTA both have mixed results in the studies reviewed, either due to a null effect on psychosocial outcomes (CST) or on high rates of refusal to participate and loss to follow-up in individualized BTA (Buschkuehl et al., 2008; Piras et al., 2017; Robert et al., 2020; Wong et al., 2017b; Young et al., 2018). It is possible that MBSR may ameliorate attrition rates, based on reviewed MBSR studies showing strong adherence and completion rates and the fact that a group format for BTA may ease hesitations to try new technology.
Second to therapy type is therapy schedule. A combination of either MBSR or MBCT with CST would result in an intervention lasting over 5 hours per week with upward of two additional weekly hours of homework, which is far above a group intervention's usual length of 2 to 3 hours (Stewart et al., 2009). Multiple sessions per week are possible in some populations, especially those in assisted living facilities. The studies reviewed demonstrate that older adults who primarily live independently are also affected by cognitive impairments and seeking group therapy. For this population, who may maintain employment and other commitments, one session per week that blends 2 hours of weekly MBSR with an hour of BTA may be an acceptable intervention package, which also accounts for some of the required BTA practice time per week.
Thirdly, demographic characteristics are important to consider. Ages and genders were mixed and varied in the studies reviewed, suggesting that these criteria can be somewhat flexible. More rigid is the level of cognitive impairment, which is usually capped at mild-to-moderate impairment with groups closely matched based on the level of cognitive functioning (Tappen & Hain, 2014). Considering similar cognitive functioning within a group and not attempting to use these psychosocial strategies to alleviate severe impairment may also improve the feasibility and acceptability of a combined mindfulness–cognitive training intervention.
Limitations of the study
This review has several limitations. A third screener would have improved review rigor but was not possible in this instance due to resource restraints. While the two screeners had 92.9% consensus from their independent selection process, a measure of inter-rater reliability was not applied at the time of search, again due to resource restraints. Limiting article selection to social work involvement potentially excluded studies conducted solely in other professions. While other allied health professions (such as psychology or nursing) may research mindfulness and cognitive training therapies for older adults to address effects of cognitive impairment, this study focused on social work. While MBSR and MBCT are the two predominant and manualized mindfulness therapies, other MBIs have been developed that incorporate components of mindfulness and meditation (Shapero et al., 2018). Dialectical behavioral therapy (DBT) and acceptance and commitment therapy (ACT) are perhaps the two best-known MBIs, although many interventions exist under this category with varying quality of evidence and varying level of mindfulness incorporated into their regimens. This review did not include studies that assessed these other MBIs, although they appear to be less utilized with this population and problem than MBSR and MBCT. Other limitations include the heterogeneity of the samples included in this review (in age, ethnicity, location, etc.) and limiting studies to those published in English. Finally, the lack of long-term follow-up in the studies reviewed mean that the long-term impact of these interventions remains unclear.
Conclusion
Combining MBSR and BTA into a single intervention may address pitfalls associated with each therapy category, offering the emotional support of MBSR alongside the practical support of BTA. Such a combination could also be a means through which older adults—especially those living independently with other time demands—can tolerably access these two types of promising supports for alleviating the effects of cognitive impairment. Such a combination may lower attrition rates and ease the challenges of using new technology that are commonly seen in individualized cognitive training studies while offering a tactile form of support (i.e., BTA) to complement the more emotional strategies taught in MBSR. This review demonstrates that demographics and diagnoses are often contextual in mindfulness and cognitive training studies and identifies a need for older adults to be engaged in the design and implementation of these interventions. By considering community members’ needs and combining MBSR and BTA in a group format—which could be titled cognitive remediation group therapy—may provide a single intervention package that could offer promising psychosocial techniques to ameliorate the symptoms of cognitive impairment.
Footnotes
Ethical Approval
Ethics approval was not required for this review article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Planning and Dissemination Grant from the Canadian Institutes of Health Research (CIHR #478015) and a Pilot Study Grant from the CIHR Canadian HIV Trials Network (CTN #PT029).
Declarations of Conflict of Interests
The authors confirm that they have no conflict of interest in respect of the material submitted in this article.
Author contributions
ADE oversaw the review, supervised the personnel, led the analysis and interpretation of the results, and wrote the first draft of the manuscript. SBR and SLW contributed to the study design and selection criteria. All authors critically reviewed the manuscript and approved the final submitted version of the manuscript.
Acknowledgements
ADE was an Ontario HIV Treatment Network (OHTN) Endgame Leader at time of study. SLC and BAF are Canada Research Chairs. SLW is an OHTN Research Chair. The authors would like to thank Nelson Pang for his assistance with this article.