
Abstract
Summary
Performing work is regarded as a key factor in the social inclusion of vulnerable persons. However, such social inclusion appears to be problematic in both mainstream and segregated settings. We aimed to examine whether volunteer work in integrated settings could be a suitable alternative. In a case study, we interviewed 13 vulnerable persons who were enabled—through a “Quarter Making” intervention—to perform volunteer work in a community setting. Data were analyzed using concepts from social epidemiology and social sciences.
Findings
Participation in the community gave respondents structure, and made them feel useful, meaningful, and proud, as well as a useful interconnected part of society. Interpersonal relationships provided them with superficial but meaningful contacts in the community, and helped them to transcend their social group, and—sometimes—build friendships. These experiences of improved social inclusion resulted in respondents reporting better mental health and wellbeing, and speaking in terms of feeling more normal and—sometimes—in terms of recovery.
Applications
To improve the social inclusion of vulnerable persons, performing volunteer work in integrated settings could be a suitable alternative for mainstream work or work in segregated settings. Interventions aimed at matching vulnerable persons to integrated settings, like Quarter Making, should preferably find a balance between creating bridging capital, to allow vulnerable persons to connect to “the normal world,” and offering bonding capital, to give them a safe place where they can “learn and relearn” to deal with the demands of modern society.
Keywords
Introduction
Performing work is seen as a key factor that enables persons with mild intellectual disabilities or mental health problems to become socially included (Abbott & Mcconkey, 2006; Hall & Wilton, 2011; Stein & Santos, 1998). Social inclusion can be defined as the interaction between being active in the community and having interpersonal relationships (Simplican et al., 2015). Social inclusion of persons with disabilities is believed to contribute to greater experienced mental health and wellbeing (Berkman et al., 2014; Schalock, 2004). Persons with mild intellectual disabilities or mental health problems who perform work are less likely to feel lonely, less likely to have money problems, and more likely to be mentally and/or physically healthy (Lippold & Burns, 2009; Meulenkamp et al., 2015; Michon et al., 2002; Stein & Santos, 1998). Even though these vulnerable groups are generally highly motivated to work (Lysaght, Ouellette-Kuntz, et al., 2009; Stanley & Regan, 2003; Tompa et al., 2006), their employment rate lies significantly below that of the general population (Brault, 2012; Evans & Repper, 2000; Hall & Wilton, 2011; Lysaght, Petner‐Arrey, et al., 2017; Meulenkamp et al., 2015). This discrepancy between the desire to work and the fulfillment of this desire is confirmed by parents of persons with mild intellectual disabilities, who report the lack of work or other productive involvement as one of the main voids in their adult child’s life (Lysaght, Petner‐Arrey, et al., 2017).
Persons with disabilities may find employment in various types of work settings (Simplican et al., 2015). However, this does not always work out well. On the one hand, performing work in mainstream work settings has remained difficult to achieve for the majority of persons with mild intellectual disabilities or mental health problems (Brault, 2012; Evans & Repper, 2000; Lysaght, Petner‐Arrey, et al., 2017; Meulenkamp et al., 2015). On the other hand, supported work in a segregated setting, i.e. sheltered work, may serve as a meaningful activity and a way to earn money (Butcher & Wilton, 2008; Hall, 2010), but is also blamed for resulting in exploitation (Hyde, 1998; Lemon & Lemon, 2003) and for perversely bringing about social segregation and stigmatization (Holmqvist, 2010; Sebrechts et al., 2018). Therefore, alternative routes are being explored to socially include these vulnerable groups through work (Hall & Wilton, 2011). Volunteer work in an integrated setting, i.e. a mainstream setting that is not limited to a specific group but where there is less focus on productivity and more on belonging (Nichols & Ralston, 2011; Simplican et al., 2015), has been presented as a more suitable road to social inclusion for vulnerable persons (Hall, 2010; Hall & Wilton, 2011; Lindsay, 2016; Nichols & Ralston, 2011). Integrated settings may include—but are not restricted to—public and non-profit-oriented workspaces. Empirical research into persons with disabilities or mental health problems working as volunteers in integrated settings, and the experiences of and benefits for these groups, e.g. in terms of social inclusion and increased wellbeing, has remained limited, so this area is in need of further research (Farrell & Bryant, 2009; Hall & Wilton, 2011; Lindsay, 2016).
In order to overcome the barriers that vulnerable persons experience in finding volunteer work (Bruce, 2006; Lindsay, 2016), an experimental program—the Quarter Table—has been developed in the Netherlands, which connects them to unpaid work in integrated settings in the community. By conducting research among participants of this Quarter Table program, we wanted to contribute to a better understanding of the role that volunteer work in integrated settings can play in improving the social inclusion of vulnerable persons.
The Quarter Table
The Quarter Table—a Quarter Making intervention that started in 2008 (see Box 1)—is a community-based intervention that provides volunteer work for persons with mild intellectual disabilities or persons with mental health problems with the aim to create a more diverse and inclusive society. The Quarter Table—active in a medium-sized Dutch city—involves meetings of professionals of different social work organizations that are active in a neighborhood. Each city district has its own Quarter Table (North, West, South, East, Center). The Quarter Table has a chairperson, who is referred to as a Quarter Maker, who chairs the meetings. The representatives of the social organizations involved “introduce” a client with a specific work-related goal. This can be a client of their own organization or a client who came to their attention in some other way. The client is not present at the Quarter Table meetings.
The attendees of the Quarter Table draw up a concrete plan to match the client with volunteer work that fits his or her work-related goal. One of the social work professionals is assigned to the case discussed. This person is responsible for contacting the local integrated work setting that is believed to be the most appropriate. Examples of such settings where clients can perform volunteer work are the local football club, a community center’s coffee place, and a public primary school. The Quarter Maker supervises the matching process and creates a “warm transfer”, for instance through accompanying a client for a longer period or assuring that there is a dedicated contact person at the work setting. Unfinished cases are discussed at each successive Quarter Table meeting until suitable volunteer work has been found for the client.
Aim of the study
The aim of our study was to find out if volunteer work in integrated settings can be a suitable alternative for performing paid work in mainstream settings or unpaid work in segregated settings. We investigated whether and how performing volunteer work in integrated settings leads to social inclusion and improved mental health and wellbeing. We did this by examining the experiences of persons with mild intellectual disabilities and persons with mental health problems who found a place to perform volunteer work with the help of the Quarter Table.
Methods
Design
We conducted a case study of the Quarter Table, which allowed us to investigate this contemporary phenomenon in its real-life context (Yin, 2017). We held semi-structured interviews with vulnerable persons who had been matched with volunteer work. When possible, KK visited the respondents at the place where they performed their volunteer work. This was done to enable the respondents to show their work-related activities. We expected that conducting the interviews at the setting could help the respondents reflect better on their experiences.
Familiarization
The principal researcher, KK, has a master’s degree in sociology, was trained and had experience in doing research with vulnerable persons, and was involved as a volunteer in a social work intervention that aimed to socially include persons with mild intellectual disabilities and mental health problems. Between April 2016 and July 2016, KK visited the Quarter Table program in three different city districts (South, Center, North) a total of eight times. This familiarization process was used to help him understand the set-up and organization of the intervention (Bryman, 2015). He took notes during the meetings. In addition, he held informal interviews with five social workers attending the Quarter Table about their working methods and experiences. Three of them were Quarter Makers, one represented a social work organization for persons with mild intellectual disabilities, and one represented a social work organization for persons with mental health problems.
Respondents
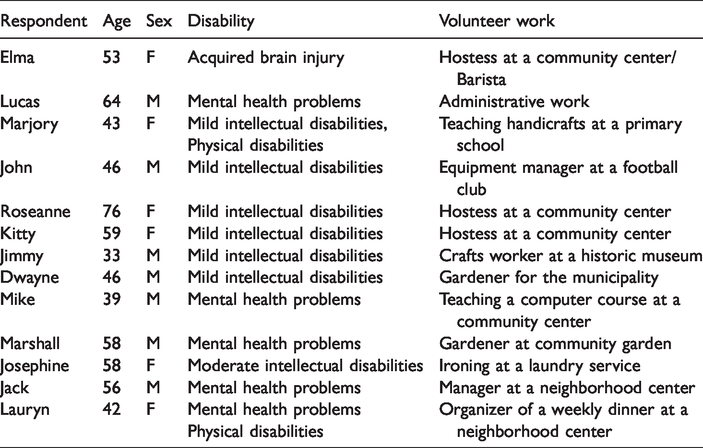
The three Quarter Makers helped to recruit clients for an interview. Thirteen vulnerable persons who had been matched with volunteer work through the Quarter Table agreed to be interviewed (see Table 1; names are fictitious). Most respondents were persons with either mild intellectual disabilities (n = 6) or mental health problems (n = 5). One respondent had acquired brain injury (n = 1) and one had moderate intellectual disabilities (n = 1). Two respondents had additional physical disabilities. Six of the respondents were female and seven male; their age varied from 33 to 76 years.
Characteristics of the respondents and the volunteer work they performed.
Interviews
KK held semi-structured interviews between May 2016 and October 2016. The main themes addressed were general experiences with volunteer work, mental health, wellbeing, benefits of volunteer work, community participation, and interpersonal relationships.
The respondents were offered a certain freedom to control the direction of the interview. If they went off-topic, this was not prevented, in order to allow them to speak in their own words about their own themes, i.e. to “Verstehen” the respondents (Weber, 1947). This approach was intended to ensure that the interviewer did not direct the interviews too much, which is considered important when interviewing vulnerable groups (Russell, 1999).
The interviews took place at the homes of the respondents (n = 5) or at the place in the community where they did their volunteer work (n = 8). Interviews took between 30 and 150 minutes, with a mean of one hour. The wide range of interview durations had to do with differences in the respondents’ cognitive abilities. For example, one respondent, who was accompanied by her personal social worker for the interview, had moderate intellectual disabilities and found it difficult to express her experiences. As a result, the interview was shorter than usual. On the other hand, some respondents, mostly the ones with mental health problems, were so happy to speak about their experiences that their interviews took longer than average.
Data analysis
The interviews were transcribed verbatim and analyzed thematically (Miles et al., 2014; Ritchie & Spencer, 1994). Thematic codes were assigned to interview excerpts (Bryman, 2015). We made use of theory-led codes (Bryman, 2015) to see how community participation and interpersonal relationships, i.e. social inclusion (Simplican et al., 2015), were related to improved wellbeing and mental health for our respondents (Berkman et al., 2014; Schalock, 2004). Other codes used were inductive: themes that were not fully accounted for but proved relevant to the respondents were coded in an open fashion (Bryman, 2015).
Informed consent
KK’s role as a researcher was discussed at each Quarter Table that he visited. Each respondent was fully informed of the aims and methods of the study, both by the Quarter Makers, who functioned as gatekeepers, and by KK before the interview. A priori oral consent was obtained and audiotaped. Respondents were de-identified by using fictitious names.
Results
The experiences of respondents reflected social inclusion (Simplican et al., 2015) and are reported for the domains of community participation and interpersonal relationships.
Community participation
Having structure
Respondents mentioned that performing volunteer work gave them structure in their lives and this helped them to learn to cope with the demands of society. Having structure made respondents feel they had a goal. It was seen as a preventive measure against feeling mentally unwell. The following quote illustrates the importance of having structure: The goal is, I guess, to be able to say that I have a goal again and that I can do all things by myself again, and that makes me happy. (…) If I didn’t have this, I would spend more time at home, and then you’d go crazy wouldn’t you. (Elma, 53: Hostess at a community center/Barista) The biggest problem of people who are in need of mental and physical help is that they waste away in their rooms. I have experienced that myself. So, if I can do something to prevent or reduce that wasting away then I immediately say yes. (Lucas, 63: Administrative work)
Being useful and feeling meaningful
Being an interconnected and useful part of society was experienced by many respondents as something important, providing them with a sense of self-worth. One respondent expressed this experience as: I want to make myself useful. My personal view is that I’m basically nothing but a burden to society. I receive a social benefit and I don’t do anything in return. For my sense of self-worth, I try to be as little of a burden as possible to others and therefore I try to do as much as I can. (…) That I can mean something for others obviously affects my self-worth. The feeling that you’re a useful part of society. (Mike, 39: Teaching a computer course at a community center) It’s very different from the daytime activity center because that’s more hobby-oriented and this is like work for me. I’m not paid for it or anything, but I don’t mind that either. I still get what I’ve already wanted for a long time. I’ve been wanting to work with children for a long time. (Marjory, 43: Teaching handicrafts at a primary school)
Being proud and overcoming stigma
All respondents felt proud about performing work. The structure it provided and the fact that they were able to do something deemed meaningful by others was often mentioned as a source of this pride. For example, a respondent mentioned how performing volunteer work helped her to fight the stigma and self-stigma that accompanied her disability. The fact that she was exceeding both her own and society’s expectations filled her with pride: You’re disabled, there are lots of negative ideas about this anyway, and then I think … Yes, I see it as a kind of proof that you can do more with your disability than you may think yourself. And I’ve experienced that myself. I can do a lot more than I used to do. (Marjory, 43: Teaching handicrafts at a primary school) “I am proud to be here [at the football club]. I will continue to do this [work as an equipment manager] until I reach sixty-five. It’s fun. My ambition is to give football training to the children as well” (John, 46: Equipment manager at a football club).
Recovery and feeling normal
All respondents mentioned improvements in their mental health and wellbeing as a result of their volunteer work. One respondent who had mental health problems explained how he was being perceived as a useful part of society again, by himself and others, and how the feeling of being valuable had helped his recovery. “Yes, what I just said, it also has to do with the cycle of recovery. Having work again, even if it’s called volunteer work. Being able to say that to yourself and to others, that’s valuable” (Lucas, 63: Administrative work).
Interpersonal relationships
Superficial but meaningful contacts
Through their volunteer work, respondents increasingly felt part of their neighborhood. They mentioned being recognized more, being greeted in the street, and having a talk about the weather with people in the neighborhood. For example, a respondent told how he was recognized and greeted in the street because of his role at the local football club: I went to the [supermarket] last night. I had to get bread and milk, and a lot of people said, “Hey John, hey John”. Yes everyone, yes. Everyone knows me. Even the [supermarket] staff sometimes come to watch the football here. (John, 46: Equipment manager at a football club) “I think if you don’t have all of that [social contacts through work], you will relapse [into feelings of depression]. You just have to keep going. Be among the people” (Elma, 53: Hostess at a community center/Barista).
Transcending one’s own social group and friendships
Respondents spoke of the importance of interpersonal interaction and of transcending their own social groups. This made the respondents feel “more normal” and more part of society. Respondents felt appreciated and this made them overcome their own self-stigmatization. For example: Yes, then you have the idea that you’re constantly among the disabled. And I can’t stand that. I’m also disabled myself, of course, but now I’m really among people and doing a good job. At least they’re always happy when I’m there [serving coffee at a community center]. (Elma, 53: Hostess at a community center/Barista) “I don’t want to linger in the disability world. That kind of constrains you, I feel. And I think this is quite a challenge” (Marjory, 43: Teaching handicrafts at a primary school). I’ve been doing it [volunteer work at the community center] for a few years now and I know everyone, so it feels a bit like a warm bath, you know. (…) I’m also kind of dating him, that old man. And he’s seventy-five, but yes, I now have that again because I’m working here [in the community center]. (Elma, 53: Hostess at a community center/Barista)
Discussion
Summary of the findings
In our case study, we investigated if and how performing volunteer work in integrated settings in the community was related to greater social inclusion and to improved mental health and wellbeing for persons with mild intellectual disabilities and mental health problems. Our respondents reported improvements in this respect through both community participation and interpersonal relationships. Community participation provided respondents with structure; made them feel useful, meaningful, and proud; and helped them feel recovered and “more normal”. Interpersonal relationships provided them with superficial but meaningful contacts in the community, helped them transcend their own social group, and helped them feel “more normal” and—sometimes—build friendships. This process of social inclusion through volunteer work was said to counteract the feeling of being stigmatized as well as self-stigmatization, and made them feel a valuable part of society.
Interpretation
We saw how performing volunteer work in an integrated setting enabled social inclusion of vulnerable persons though strengthened community participation. We argue that these findings reflect a “Durkheimian” perspective on belonging and solidarity (Durkheim, 1893/1997). Durkheim states that the more complex a society becomes, the more the tasks to be performed become differentiated. In such a society, belonging occurs because one differs from one’s group members, and one is able to perform specific tasks that are deemed meaningful to society as a whole. This is what Durkheim calls “organic solidarity,” as opposed to the “mechanical solidarity” of less complex societies, in which belonging occurs because one is similar to one’s group members (Durkheim, 1893/1997). Without support, vulnerable persons find it difficult to cope with the demands of our complex merit-based society (Kal, 2001). High expectations about issues like productivity make it impossible for these persons to perform tasks that are deemed meaningful by others, and thus to be a valuable member of—or to belong to—our society (Kal, 2001, 2012). Our results indicate that volunteer work in integrated settings can enable vulnerable persons to perform tasks that are perceived as meaningful by both themselves and others—i.e. “to give back to their community” (Choma & Ochocka, 2005)—and thus to feel an interconnected part of society.
We also saw how performing volunteer work in an integrated setting promoted the social inclusion of vulnerable persons as it altered their interpersonal relationships. We argue that such altered interpersonal relationships reflect Putnam’s concept of social capital (Putnam, 2000). We noticed that interactions with people outside their own social groups, i.e. the development of bridging capital (Putnam, 2000), helped respondents to feel included in “the normal world” instead of “lingering in the world of disabilities.” This corresponds with earlier findings showing that it is especially bridging capital which plays a role in relieving mental distress in vulnerable communities (Mitchell & LaGory, 2002), by allowing persons who feel different and excluded to find a connection with the “normal world” (Bates & Davis, 2004). Social capital derived from ties in one’s own social group, i.e. bonding capital, is important for feeling safe and forming friendships (Putnam, 2000). On its own, however, bonding capital may negatively impact on the health and wellbeing of vulnerable persons, since it may strengthen rather than lessen the exclusion they experience (Caughy et al., 2003; Kruithof et al., 2018; Ziersch & Baum, 2004).
Implications
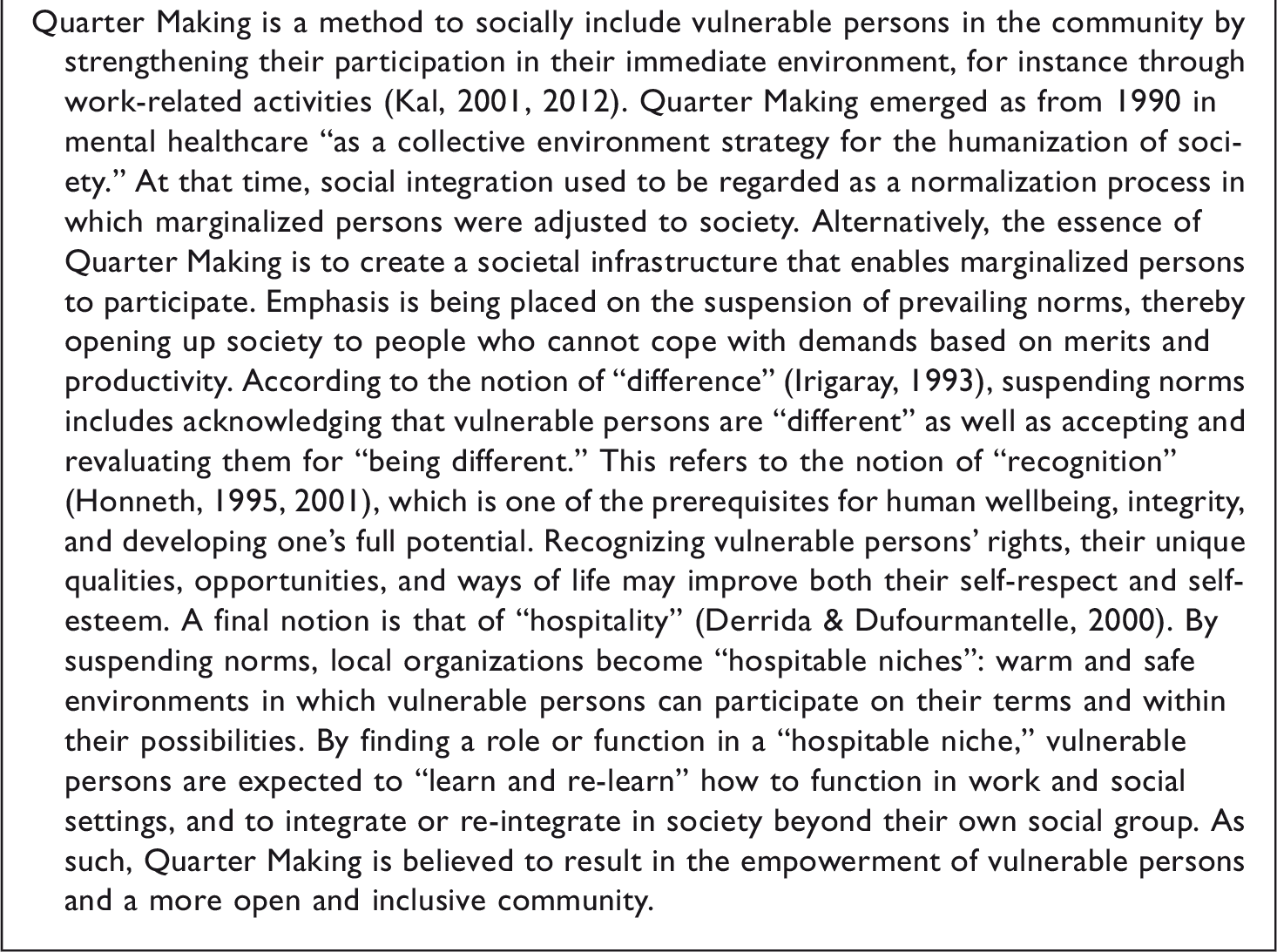
Performing volunteer work in integrated settings seems to be a suitable alternative to improve the social inclusion of persons with mild intellectual disabilities or mental health problems. Like work in segregated settings (Butcher & Wilton, 2008; Hall, 2010), volunteer work in integrated settings offered the structure necessary to prevent these vulnerable persons from “wasting away.” Our results indicate that performing volunteer work in an integrated setting may additionally be experienced as “more real” and therefore, as has also been found by others (Butcher & Wilton, 2008), “more meaningful” than performing activities, mostly taking place in segregated settings. Moreover, the bridging capital that became evident in our interviews may help to overcome the social segregation and stigmatization attached to working in segregated settings (Holmqvist, 2010; Sebrechts et al., 2018). In our study, respondents expressed the absence of such adverse effects as feeling more normal and feeling—to some extent—recovered. Crucial to these gains were the “hospitable niches” (Derrida & Dufourmantelle, 2000) created through the Quarter Making method (Kal, 2012, see Box 1). In such places, difference is accepted and prevailing norms regarding productivity are suspended so that vulnerable persons can fulfill a meaningful role in the community at their own pace. While our results may justify further investments by local authorities in the establishment of such “hospitable niches,” further research could investigate the requirements for both the integrated settings and the social work intervention needed to create them.
Two qualifications are in order here. First, it seems unlikely that commercial businesses could just as easily suspend their current norms about productivity in order to create the “hospitable niches” needed (Kal, 2001, 2012; Nichols & Ralston, 2011) as the public and non-profit-oriented work settings in our study. Second, some vulnerable persons may—at least initially—benefit more from activities in segregated settings, because they feel safer in such places (Kruithof et al., 2018). Together, these qualifications refer to the notion of learning and re-learning, meaning that excluded vulnerable persons may only gradually learn to deal with the demands of a complex society (Kal, 2001). In practice, this notion may imply that interventions aimed at socially including vulnerable groups through volunteer work should weigh up the distance between social groups that is “to be bridged” and the warmth that is to be offered by the “hospitable niche.” In other words, in Quarter Making interventions it seems paramount to find a balance between bridging capital and bonding capital. Such a balance may also help to counteract the barriers that vulnerable persons may encounter when trying to find volunteer work (Bruce, 2006; Lindsay, 2016). Future studies could examine which conditions should be met by work settings, vulnerable persons, and Quarter Makers in order to make finding and performing volunteer work in integrated settings a success.
Is has been argued that volunteer work may be perceived as more meaningful than paid work in mainstream settings, as the former can be chosen based on perceived necessity, fulfillment, and enjoyment (Nichols & Ralston, 2011). Our findings seem to support this assertion: it was the meaningfulness of the volunteer work that mattered to the respondents, rather than the payment. Yet, for other vulnerable persons such payment could be necessary to make ends meet (Butcher & Wilton, 2008; Hall, 2010). This remuneration dilemma touches upon the emerging societal debate in the Netherlands about the desirability of a “parallel labor market” (Brouwer et al., 2018). Starting from the premise that everyone deserves paid work, it is argued that voluntary work should be subsidized for those persons who cannot meet the requirements of mainstream employment. Our findings, as well as those of others (Abbott & Mcconkey, 2006; Hall & Wilton, 2011; Lindsay, 2016; Stein & Santos, 1998), support the suggested importance of performing work for the social inclusion of vulnerable persons. However, realizing the proposed “parallel labor market” would, in terms of Quarter Making (Kal, 2001, 2012), require a more profound and widespread suspension of productivity norms than was required for the Quarter Making intervention we studied. Hence, our study may be seen as a first exploration of how such a “parallel labor market” could be created in a more or less bottom-up manner. Future research could investigate whether such an approach could be introduced on a larger scale and in different welfare societies.
Strengths and limitations
Our sample (n = 13) was relatively small, especially since it comprised two sub-samples: persons with intellectual disabilities (n = 8) and persons with mental health problems (n = 5). This limits the generalizability of our findings. In addition, a bigger sample would have allowed us to make a comparison between the two groups. Inherent to the difference between two groups, for instance, is the possibility of recovery for people with mental health problems. Experiences of recovery through volunteering for people with mental health problems could be a worthwhile topic for future studies. This being said, the patterns we identified in the experienced benefits of performing voluntary work in integrated settings were fairly consistent for both groups of vulnerable persons in our study. Therefore, we regard our findings as relatively robust.
Another limitation is that we studied a selected sample. First, our respondents were selected with the help of Quarter Makers, which could mean that they represented only the success stories of the Quarter Making intervention. Second, all our respondents had a desire to perform volunteer work. In view of this selected sample, we do not know what our findings mean for the wider group of persons with mild intellectual disabilities or mental health problems. Since earlier empirical work suggests that both these groups have a strong desire to perform work (Lysaght, Ouellette-Kuntz, et al., 2009; Stanley & Regan, 2003; Tompa et al., 2006), we think that our findings may be applicable to a wider group of vulnerable persons.
A final limitation is that some respondents are quoted frequently in our “Results” section, while others are not quoted at all. This is because some of the vulnerable persons we interviewed were able to express themselves more eloquently, while others found it more difficult to verbally present their experiences. Although we selected coherent citations for publication in this manuscript, we took care that these quotations were representative of the wider group of respondents.
Conclusion
In attempts to improve the social inclusion of vulnerable persons, performing volunteer work in integrated settings could be a suitable alternative for mainstream work or work in segregated settings. Interventions aimed at matching vulnerable persons to integrated settings, like Quarter Making, should preferably find a balance between creating bridging capital, allowing vulnerable persons to connect to “the normal world,” and bonding capital, giving them a safe place where they can “learn and re-learn” to deal with the demands of modern society. Quarter Making offers food for reflection about creating a “parallel labor market.”
Footnotes
Declaration of conflicting interests
The author(s) declared potential conflicts of interest with respect to the research, authorship, and/or publication of this article: In her book Kwartiermaken. Voor mensen met een psychiatrische achtergrond [Quarter Making. For people with a history of mental health problems], author DK coined the term “Kwartiermaken [Quarter Making]” as a volunteer work concept and described its approach based on philosophical theories. She was and is not involved in any way or form with the studied and described Quarter Making intervention.
Ethics
According to the Dutch Medical Research Involving Human Subjects Act, this study did not require approval by a medical research ethics committee in the Netherlands. However, the research proposal was extensively reviewed by the funder of the study, including its ethical aspect. We followed the ethical principles for medical research involving human subjects as laid down in the Declaration of Helsinki and adopted by the ![]() . In addition, for doing research with vulnerable persons, KK applied for and received a Certificate of Conduct from the Dutch State Secretary for Justice and Security.
. In addition, for doing research with vulnerable persons, KK applied for and received a Certificate of Conduct from the Dutch State Secretary for Justice and Security.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Our research project was funded by ZonMw (The Netherlands Organization for Health Research and Development) located in the Hague (the Netherlands), under the program of “Alles is Gezondheid” (Health is Everything, Project Number: 531005003).
Acknowledgements
We like to thank all professionals, volunteers, and participants of the Quarter Table for enabling us to do research in such a meaningful setting. We like to specifically thank Eus de Wit, Alex Smits, and Sanne van der Werff for their help and support during the data collection phase of the research.