
Abstract
Background:
Dental monitoring (DM) constitutes a recent technological advance for the remote monitoring of patients undergoing an orthodontic therapy. Especially in times of health emergency crisis, the possibility of relying on remote monitoring could be particularly useful.
Objectives:
To assess the effectiveness of DM in orthodontic care.
Eligibility:
Studies conducted on healthy patients undergoing orthodontic care where DM was applied, assessing a change in treatment duration, emergency appointments, in-office visits, orthodontic relapse, early detection of orthodontic emergencies and improvement of oral health status.
Information sources:
PubMed, Web of Science and Scopus were searched for publications until November 2022.
Risk of bias:
Quality assessment was performed with the STROBE Checklist.
Data extraction:
Data were extracted independently by two reviewers, and discrepancies were resolved with a third reviewer.
Included studies:
Out of 6887 records screened, 11 studies were included.
Synthesis of results:
DM implemented to the standard orthodontic care was found to significantly decrease the number of in-office visits by 1.68–3.5 visits and showed a possible trend towards improvement of aligner fit. Conversely, evidence does not support a reduction of treatment duration and emergency appointments. The assessment of the remaining variables did not allow any qualitative synthesis.
Conclusions:
This review highlighted that DM implemented to standard orthodontic care can significantly decrease the number of in-office visits and may potentially result in an improved aligner fit. Due to the low quality of most of the included studies and the heterogeneity of the orthodontic system where DM was applied, studies with different investigation team and rigorous methodology are advocated.
Introduction
Orthodontic treatments are usually characterised by a long treatment duration, with a recent systematic review summarising a mean treatment time with fixed multibracket appliance of approximately 20 months (Tsichlaki et al., 2016). Such a lengthy duration increases the risk of deterioration of oral hygiene status (Al-Anezi et al., 2011) and higher chance of demineralisation (Lundstrom and Krasse 1987), with possible discontinuation of the therapy itself (Geiger et al., 1988). With the recent orthodontic advances of self-ligating system and aligners, orthodontic therapy may not require such close in-office monitoring. Expanding appointment intervals, without increasing the treatment duration, is a powerful tool as it saves time for patients and clinicians and reduces the risk of infection transmission. On the other hand, spacing the appointments further apart from each other may increase the chance of undetected orthodontic emergencies that in turn may extend the overall treatment duration, if not identified early. With this in mind, the possibility of including remote monitoring could be particularly useful.
Dental monitoring (DM) is a relatively new tool designed for the remote monitoring of dental patients (Caruso et al., 2021; Kravitz et al., 2016). DM is a software-based programme and consists of three integrated platforms: a mobile app downloaded on the smartphone of the patient; a web-based Doctor Dashboard® managed by the provider; and a movement-tracking algorithm, which allows the analysis of the pictures regularly taken by the patient (Kravitz et al., 2016; Sangalli et al., 2021a). As a means of remote monitoring, studies have claimed that the use of DM in addition to the standard care, could allow the number of in-office visits to decrease, individualised treatment care of each patient, and early detect incidents and misfit of aligners, thus preventing possible complications such as orthodontic relapse or avoidable delays (Roisin et al., 2016).
To date, no review has summarised the effectiveness of DM in these selected outcomes. Therefore, the aim of the review was to assess the effectiveness of DM during orthodontic care in reducing treatment duration and the number of in-office visits, early detecting orthodontic emergencies, improving oral health status in patients undergoing an orthodontic treatment and decreasing the orthodontic relapse at the end of an orthodontic therapy. If a critical analysis of the available literature revealed better outcomes with the integration of DM, this technological advance could be broadly supported as part of standard orthodontic care, especially during a health emergency crisis where the use of telemonitoring has been encouraged to minimise in-person visits (Sangalli et al., 2022a).
Materials and methods
Study design
A scoping review of the published literature was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The study was registered with PROSPERO (CRD42022379902). Ethical approval was not required to conduct this systematic review.
PICO question
The current systematic review was conducted to answer the research question ‘Is the implementation of a Dental Monitoring system effective during orthodontic care?’ The following PICO question was formulated (Riva et al., 2012) and approved by all the reviewers.
(P) – healthy participants undergoing orthodontic care (children and/or adolescents and/or adults);
(I) – use of DM;
(C) – when present, comparison to a standard care group without the use of DM;
(O) – changes in the early detection of orthodontic emergencies, fitting of aligners, treatment duration, number of emergency appointments and in-office visits, oral hygiene status and orthodontic relapse.
Search strategy
PubMed (R), Web of Science and Scopus were systematically searched for articles published until 21 November 2022. The following search strategy was utilised: KEY [((((((dental monitoring)) OR (dental monitoring system)) OR (DM)) OR (dental monitoring software)) OR (dental monitoring app))] AND [(orthodontics)]. Free text was requested from the authors when not available (n = 1). EndNote X9.3.1 was used for reference management and removal of the duplicates (n = 9).
Selection process
The research was conducted independent of the year of publication. Eligible studies were selected following a two-phase process. The initial search and screening of titles and abstracts were performed by two independent reviewers (LS, AAB). Reference lists of the included studies were reviewed for potentially relevant missing sources. After duplicates were removed and irrelevant records excluded, full texts of the remaining potentially eligible studies were reviewed based on the inclusion and exclusion criteria by two independent reviewers (LS, AAB). Any discrepancies were resolved by consensus through discussion with a third reviewer (DD).
Eligibility criteria
To be included, the studies needed to: (1) be conducted in healthy participants of any age (children and/or adolescents and/or adults); (2) use DM during any phase of orthodontic care, that is during the active phase of an orthodontic treatment or during the passive phase at the end (retention); and (3) be in English language.
In order to be as inclusive as possible, all types of study were included, except for expert opinions, conference abstracts and book chapters, and those not conducted on humans.
Quality assessment of the included studies
The quality assessment was performed by one reviewer (LS), and a second reviewer was consulted in case of potential discrepancies. The STROBE Checklist was used to assess the methodological quality of the included studies except for the case reports (Supplemental Table S1). This checklist was selected in light of the first 18 items common to different study designs (Cuschieri, 2019). According to this quality assessment tool, six domains were investigated and marked as ‘yes’ in case the information was present, or ‘no’ if the information was omitted. The total score for the STROBE Checklists was calculated by summing 1 point for each ‘yes’ and zero for each ‘no’, resulting in a final score in the range of 0–25. Studies scoring 20–25 were evaluated as good, those scoring 15–19 as fair and those scoring <14 as poor.
The quality assessment of the case reports was performed following the tool proposed by Murad et al. (2018), by modifying criteria suggested by Pierson (2009), Hills (1965) and the Newcastle Ottawa scale (Wells et al., 2011) (Supplemental Table S2). As suggested by the author, an overall judgement about the methodological quality was achieved based on critical questions, rather than on a total sum of the eight binary responses of the scale (Murad et al., 2018). The most critical domains were the reproducibility of the research, the presence of explicit outcomes and an adequate follow-up.
Data extraction
The following identified data were collected for each category: first author; journal and year of publication; and title. The selected population was investigated in terms of sample size, age (mean, standard deviation and/or range) and biological sex. When the population was divided into a study group (with DM) and control group (without DM), the same domains were extracted for both groups. Other data recorded for the analysis included in which orthodontic system (aligners vs. multibracket appliances) and in which orthodontic phase (active vs. passive treatment) DM was applied. Finally, the use of DM was assessed in terms of type of DM protocol, outcomes measured and main findings.
Results
Review selection
A flowchart of the review selection according to PRISMA guidelines is displayed in Figure 1. The database search yielded a total of 6887 published articles. No additional studies were included by reviewing the reference list of the selected records. Of these, 6839 were excluded on the basis of title and abstract, because they were not relevant to the topic. After removing duplicates (n = 34), a total of 17 full texts were reviewed, and further assessed for eligibility. Of these, six studies were eliminated for the following reasons: inappropriate study design (n = 3); not conducted on humans (n = 1); not assessing the selected outcomes (n = 1); and lacking full text availability (n = 1). A list of the excluded full texts is available in Supplemental Table S3. A total of 11 studies were included in the qualitative analysis and classified according to the study design of case reports (three studies) (Table 1): retrospective (n = 2) (Table 2) and prospective (n = 6) (Table 3).
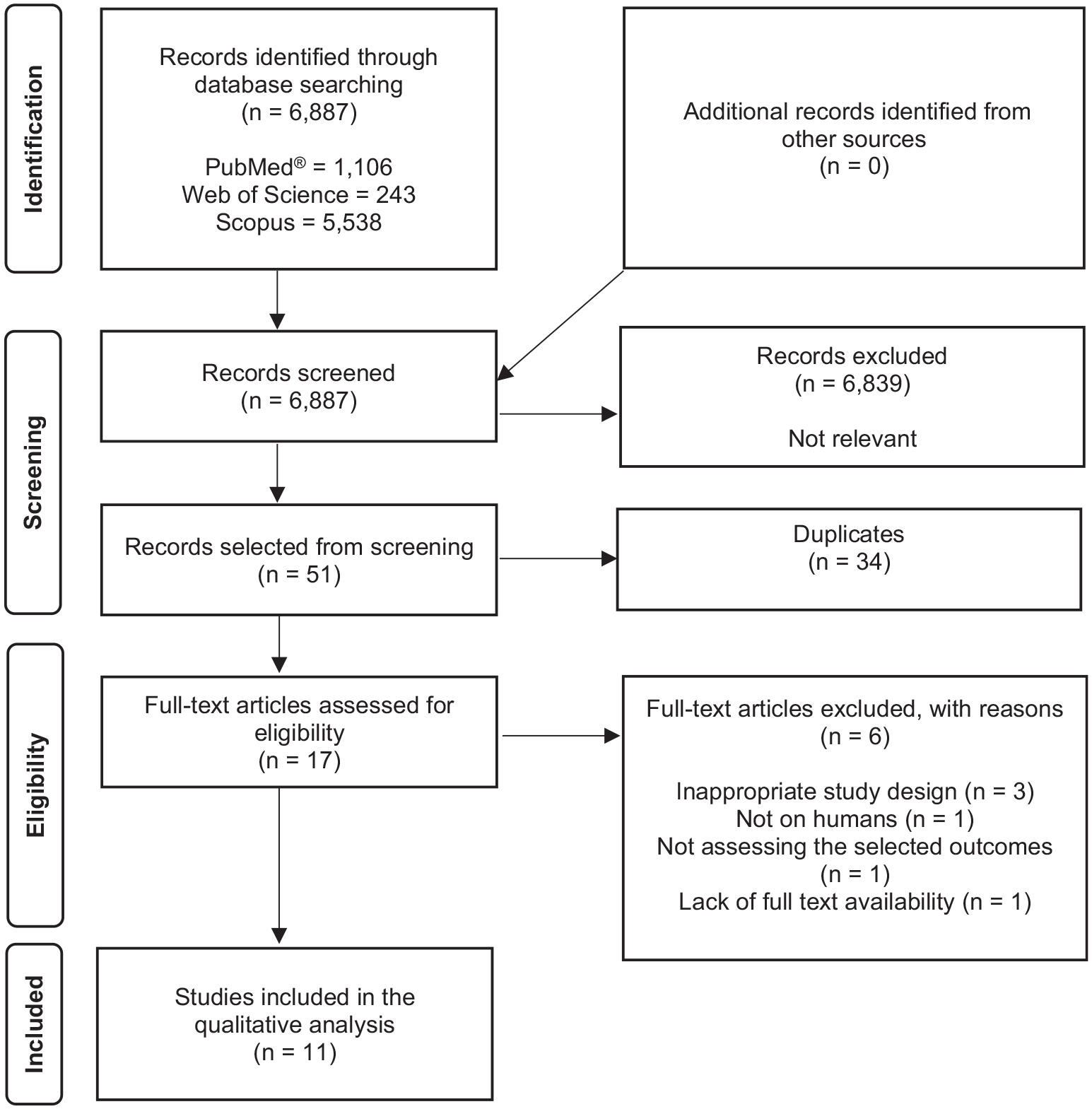
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram of study selection.
Selected characteristics and major findings of the included case reports on the use of DM in orthodontics.
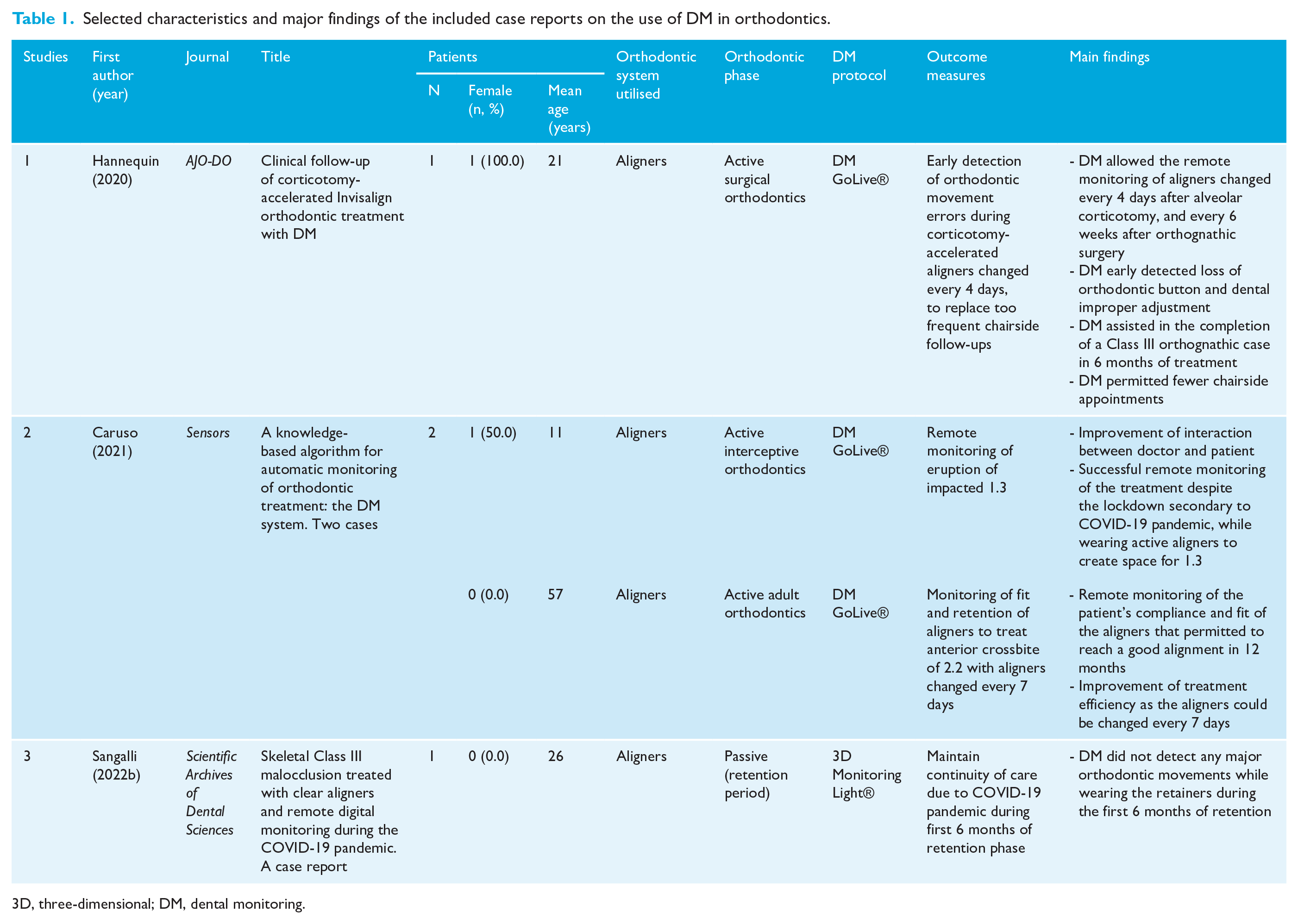
3D, three-dimensional; DM, dental monitoring.
Selected characteristics and major findings of the included retrospective studies on the use of DM in orthodontics.
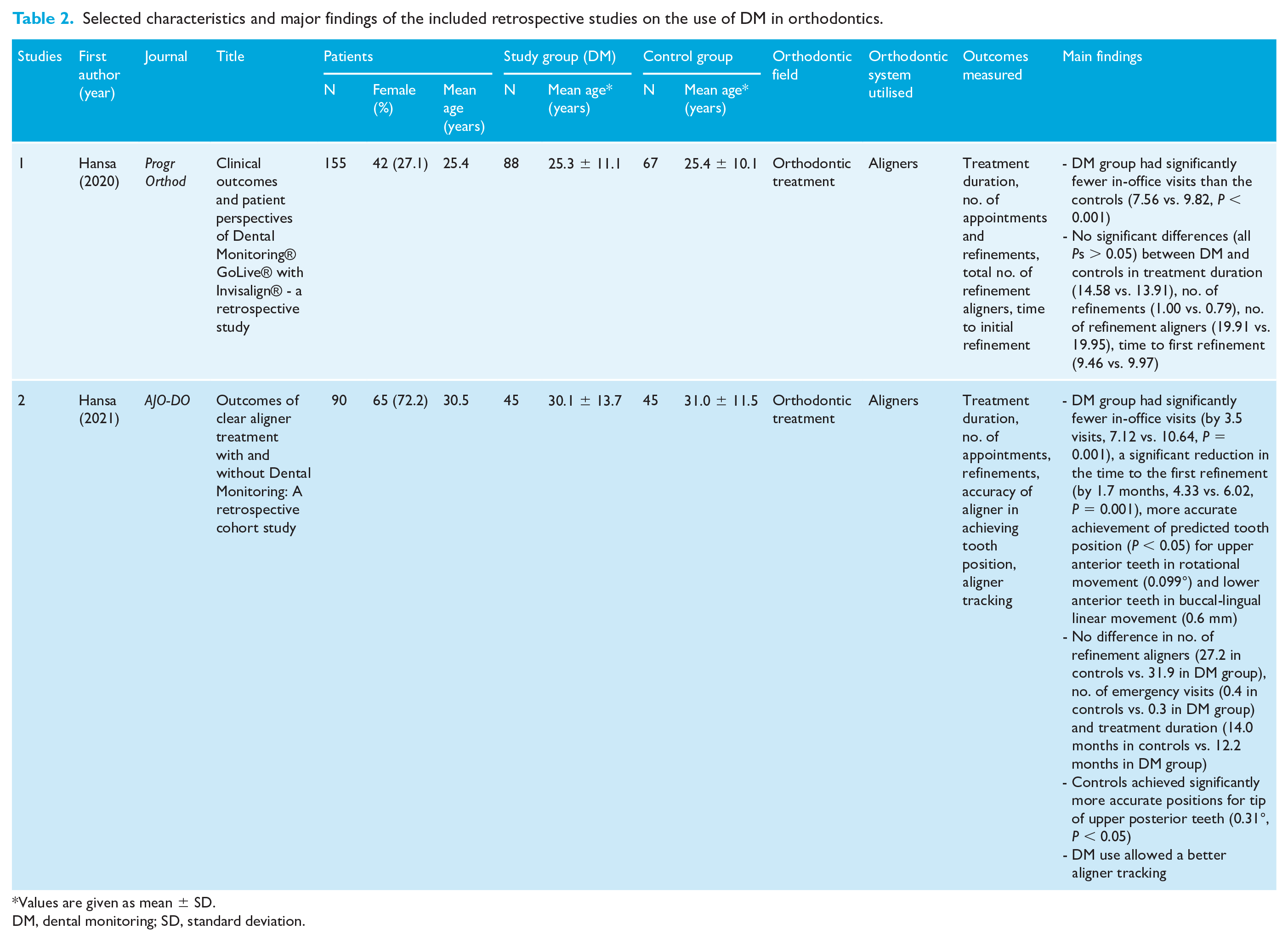
Values are given as mean ± SD.
DM, dental monitoring; SD, standard deviation.
Selected characteristics and major findings of the included prospective studies on the use of DM in orthodontics.
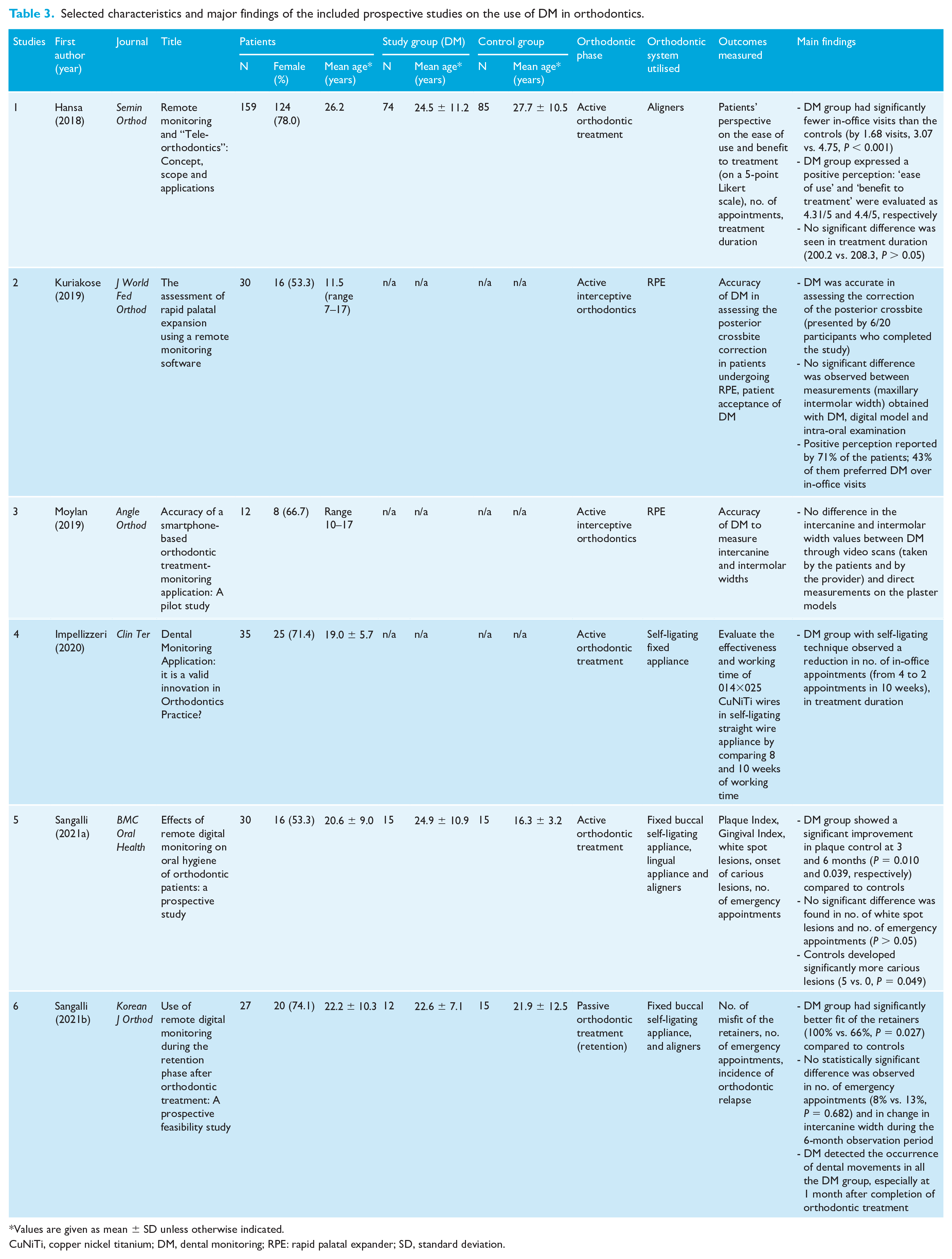
Values are given as mean ± SD unless otherwise indicated.
CuNiTi, copper nickel titanium; DM, dental monitoring; RPE: rapid palatal expander; SD, standard deviation.
Quality assessment
The assessment of methodological quality according to each domain is reported in Supplement Table S1 (for prospective and retrospective studies) and Supplement Table S2 (for case reports). The quality of the three case reports was overall considered appropriate, as they presented sufficient details to replicate the research and the outcomes were adequately explicated. In two of the three studies a relatively short follow-up for the outcomes to occur was identified.
As for the remaining eight studies, the median overall score was 18.25 (range = 15–20). Three studies were considered ‘good’ and five studies were considered ‘fair’. None of the included studies was considered ‘poor’.
Study characteristics
Characteristics of the 11 selected studies are presented in Tables 1 –3 according to the study design. The total number of included participants was 542 (range = 1–159), and of these, 315 were actively monitored with DM. The weighted mean female prevalence was 58.0% for the total sample size. Two studies were performed exclusively in children and adolescents, and two studies were conducted in adults. The remaining seven studies presented data on a mixed population.
The majority of the included studies used DM in addition to an orthodontic treatment with aligners (Caruso et al., 2021; Hannequin et al., 2020; Hansa et al., 2018, 2020, 2021; Sangalli et al., 2022b). Two studies used DM in the remote monitoring of patients undergoing treatment with a rapid palatal expander (RPE) (Kuriakose et al., 2019; Moylan et al., 2019). One study tested DM on patients undergoing treatment with a self-ligating fixed appliance (Impellizzeri et al., 2020) and the remaining two studies utilised DM in mixed orthodontic systems (Sangalli et al., 2021a, 2021b).
Due to the heterogeneity of the assessed outcomes, no meta-analysis of the retrieved findings could be performed.
Results of included studies
Early detection of orthodontic emergencies
One study (9.1%) investigated the effectiveness of DM in the early detection of orthodontic movement errors (Hannequin et al., 2020). Hannequin et al. described a case report where DM was applied to an ortho-surgical treatment where an alveolar corticotomy was performed to accelerate the orthodontic movement. Due to the rapid frequency of aligner change (e.g. every 4 days), the age of the patient (21 years) and the difficulty of performing so close in-office visits, DM was added to the standard orthodontic care to early detect potential orthodontic movement errors (e.g. incorrect orthodontic movements) and/or incidents (e.g. loss of auxiliaries or buttons). DM was effective in both early detection of an improper adjustment of the mandibular lateral incisors on an aligner as well as detecting the loss of a button, which was immediately replaced and as such did not impact the treatment evolution.
Remote monitoring of fitting of aligners
Three studies (27.3%) investigated the effectiveness of DM in monitoring the fitting of the aligners (Caruso et al., 2021; Hansa et al., 2021; Sangalli et al., 2021b). Despite the heterogeneity of the design of the studies, the use of DM showed a possible trend towards improvement in aligner fit. In the prospective study by Sangalli et al., DM was implemented to monitor the proper fit of the removable retainer during the retention phase, and revealed that those with DM maintained a significantly better fit compared to those without DM (P = 0.027) (Sangalli et al., 2021b). Similarly, in the retrospective study by Hansa et al. (2021), better aligner tracking during the active orthodontic treatment was suggested as explaining the similar accuracy of tooth movements between the two groups that was achieved in less time in the study group (e.g. the first refinement was started 1.7 months earlier, 4.33 vs. 6.02 months, P = 0.001). However, better fitting of the aligners did not prevent a more accurate mesio-distal angulation of the upper posterior teeth in the control group, compared to the predicted tooth movements. Albeit statistically significant, such movements were clinically insignificant.
Reduction of treatment duration, emergency appointments and in-office visits
Five studies (45.5%) investigated the effectiveness of DM in reducing treatment duration, number of emergency appointments and number of in-office visits.
The three studies that analysed the influence of DM on treatment duration showed no significant difference (Hansa et al., 2018, 2020, 2021). However, it should be noted that all of these studies were derived from the same group of researchers.
Similarly, three studies failed to observe any significant difference in the number of emergency appointments when DM was added to the orthodontic therapy (Hansa et al., 2021; Sangalli et al., 2021a, 2021b).
On the contrary, four demonstrated that significantly fewer in-office visits were needed when DM was integrated to the standard orthodontic care. Such reduction was in the range of 1.68–3.5 appointments for orthodontic therapy with aligners (Hansa et al., 2018, 2020, 2021). Nevertheless, the baseline characteristics of the participants were not always similar between the compared groups. For example, in the study by Hansa et al. (2018) the mean age of the DM group was 3.2 years younger (24.5 ± 11.8 vs. 27.7 ± 10.5, P < 0.05), and the proportion of female patients was significantly lower (68.4% vs. 83.3%, P < 0.05). This might have influenced the results, as female patients are known to seek treatment more often than male patients (Hunt et al., 2011). Yet, the authors did not control for these confounding factors in their analysis nor during the allocation of the participants, despite being a prospective study. Moreover, orthodontic treatment complexity was not assessed in this study, which might also have influenced the results.
Conversely, despite being retrospective in nature, the other two studies presented with homogeneous groups at baseline in terms of demographics (age, gender) and treatment complexity (Angle classification, number of initial aligners, Little’s Irregularity Index) (Hansa et al., 2020, 2021).
Finally, integrating fixed orthodontic therapy with DM was suggested to reduce by one visit (from three to two appointments) treatment of 10 weeks, when a 014×025 CuNiTi wire was inserted in self-ligating braces (Impellizzeri et al., 2020).
Improvement of oral hygiene status
One study (9.1%) investigated the effectiveness of adding DM in addition to the standard dental care in improving oral hygiene outcomes in participants undergoing orthodontic treatment (Sangalli et al., 2021a). The study was a non-randomised prospective trial where DM was implemented at the beginning of the orthodontic treatment (either with aligners, buccal or lingual fixed appliances) of 15 participants, in addition to monthly in-office visits. The results revealed a statistically significant improvement over time in plaque index in the study group during the 6-month observation period (0.51 ± 0.45 at baseline vs. 0.31 ± 0.43 at 6 months), compared to the higher plaque accumulation in the control group (0.44 ± 0.47 at baseline vs. 0.56 ± 0.43 at 6 months). The use of DM also permitted to reduce the occurrence of new cavity lesions (0 in the study group vs. 5 in the control group). As for the gingival index, this parameter dramatically improved during the observation period in the study group (from 0.88 ± 0.52 at baseline to 0.36 ± 0.42 at 6 months). However, no significant difference was seen in comparison to the control group. This finding should not undermine the improvement observed, as the two groups started with non-homogeneous values at baseline (0.88 ± 0.52 in the study group vs. 0.43 ± 0.43 in the control group). Finally, DM did not statistically influence the progression of white spot lesions between the two groups. Although the participants were treated with different orthodontic systems and, as such, possible differences could be observed, the effect size derived from the type of orthodontic systems was not provided. One reason might have been the small sample size that would have led to underpowered results.
Reduction of orthodontic relapse
Two studies, (18.2%) conducted by the same group of researchers, investigated the effectiveness of DM in reducing orthodontic relapse (Sangalli et al., 2021b, 2022b). One was a case report based on the observation of one patient in response to the lockdown imposed by the COVID-19 pandemic (Sangalli et al., 2022b); the other study was a prospective study enrolling 27 participants (Sangalli et al., 2021b), 12 of whom were monitored with DM. DM was added in addition to the standard dental care for 6 months to monitor potential tooth movements after the end of the orthodontic treatment, which was constituted by either aligners or fixed multibracket appliances. The study utilised the three-dimensional (3D) Monitoring Light® to superimpose subsequent scans performed at monthly follow-ups with the initial scan taken at the time of the removal of the appliance. The study group (n = 12) and the control group (n = 15) were compared in terms of change in intercanine width. DM detected frequent dental movements, but no statistically significant difference was observed between the two groups. Nevertheless, the study was conducted on a small sample size and the observation period was only of 6 months, which should be taken into consideration before drawing any strong conclusions.
Discussion
The current systematic review aimed to summarise the available evidence on the effectiveness of DM applied to standard orthodontic care. To our knowledge, this is the first review that systematically examines outcomes such as the early detection of orthodontic emergencies, reduction in treatment duration and number of in-office and emergency visits, improvement in oral hygiene status and aligner fit, and decrease of orthodontic relapse, when DM is utilised in addition to the standard care. To date, existent reviews on DM have either focused on the novelty of this digital technology (Kravitz et al., 2016; Maspero et al., 2020) or thoroughly explained its use (Caruso et al., 2021; Roisin et al., 2016).
The results of the available literature suggest that DM applied to the standard orthodontic care, may considerably decrease the number of in-office visits during orthodontic therapy and improve the fitting of the aligners. On the contrary, it does not seem to significantly influence the treatment duration and the number of emergency appointments. Nevertheless, critical flaws in the design of the studies might weaken the strength of such results.
Lastly, the effect on oral hygiene status, orthodontic relapse, and the early detection of orthodontic emergencies were investigated by one study only, respectively, and, as such, do not allow any comprehensive summary of the results.
Recently, the market has seen the introduction of other tele-monitoring systems, such as the Grin® digital teleorthodontic platform, an FDA-listed medical device and certified through Health Canada, and Invisalign Virtual Care AI (Align Technology, San Jose, CA, USA). Yet, their scientific validation remains to be demonstrated with clinical trials.
Effectiveness of DM in reducing in-office visits
The current review supported the evidence that when the participants were provided with DM along with standard care, the number of in-office visits was consistently reduced by 1.68–3.5 appointments for orthodontic therapy with aligners. Nevertheless, one of the studies that supported these findings did not present with homogeneous groups at baseline in terms of demographics, which might have influenced the results.
According to a previous study investigating the attitude of patients and orthodontists toward DM, the majority of the patients considered the possibility of reducing chairside visits as an advantage of this digital technology, regardless of their age (Dalessandri et al., 2021). Only a minority of patients would prefer additional office visits (Hansa et al., 2020). The reduction of in-office appointments showed that remote monitoring, such as DM, may constitute an advantage, especially for those recent orthodontic techniques that do not require such close follow-up. This is the case with self-ligating appliances (Soltani et al., 2015), where low friction brackets and light orthodontic forces allow lengthening of appointment intervals so that complete expression of the information contained in the wire is obtained (Impellizzeri et al., 2020). Other examples are orthodontic therapies carried out with aligners, that do not necessarily require a monthly interaction between patient and provider, unless an orthodontic emergency occurs. Reducing the number of in-office visits, provided that a continuity of care is preserved, is specifically helpful to minimise the risks for both patients and clinicians during time of a health emergency crisis, such as the one we experienced with COVID-19 (García-Camba et al., 2020). Interestingly, a recent investigation conducted on telehealth visits during the COVID-19 pandemic, revealed that offering telehealth service significantly increased the uptake of the intervention (Sangalli et al., 2022a) and reduced the no-show rate (7.5% for telehealth visits vs. 36.1% for in-office visits) (Drerup et al., 2021).
It should be noted that there were fewer emergency appointments in those participants where DM was implemented. Despite the fact that the difference did not reach the level of statistical significance, data can still have a clinical significance. The lack of statistical significance may be explained by the relatively short observation period (i.e. 6 months) that did not permit the outcomes to occur, by the relatively small sample size of some the included studies, or by the type of orthodontic system used in the majority of the studies (i.e. aligners), which is known to be associated with fewer emergency incidents compared to fixed multibracket appliances (Borda et al., 2020).
Effectiveness of DM in improving aligner fit
The results of the review show some support of improved aligner fit. Nevertheless, despite these preliminary encouraging findings, it is important to highlight that these results derived from the following: (1) a retrospective study, with an inevitable high risk of bias and clinically insignificant difference compared to the control group; (2) a case report, where no control group was involved; and (3) a prospective study conducted during the passive retention phase of treatment, which cannot be extrapolated to active aligner tracking.
Included studies that investigated this outcome during an active orthodontic therapy, utilised a specific option offered by DM, called the GoLive® system. This is a patented algorithm able to distinguish between seated and unseated aligners, thus suitable for aligner therapies. Specifically, when patients take pictures of their mouth with and without wearing the aligners, a signal of ‘Go’ is sent when a perfect fit is seen between the aligner and the teeth, thus indicating that they can proceed to the following aligner (Hansa et al., 2018, 2020). On the contrary, a warning of ‘No-Go’, which reflects an ill-fitting aligner, dictates that the patients should continue wearing the current aligners until a new notification is sent (Hansa et al., 2020). The possibility of remotely controlling the best time of aligner change permits personalisation of treatment care for the specific clinical need and patient condition. As shown by Hannequin et al. (2020), a rate of aligner change every 4 days was considered appropriate in a case of alveolar corticotomy, thanks to their effectiveness in accelerating orthodontic tooth movement (Aboul-Ela et al., 2011; Gil et al., 2018). Nevertheless, the orthodontic treatment was performed on an adult patient, where tooth movements occur at a slower pace compared to adolescents (Alikhani et al., 2018). This is due to the different structural composition of alveolar bone and periodontal ligament (Tanne et al., 1998), degree of biologic inflammatory markers released in response to orthodontic forces (Krishnan and Davidovitch, 2009b), systemic factors (Krishnan and Davidovitch, 2009a) and periodontal health (Okamoto et al., 2009), among others. Thus, the possibility of adding DM to remote monitoring of the correct aligner fit, is crucial for the positive progression of the therapy. By implementing DM with the GoLive® system, the patient can theoretically benefit from a more appropriate and shorter timing of aligner change, leading to the belief that the treatment duration may shorten significantly. Yet, this was not the case among the included studies; surprisingly, in one study the control group completed the treatment approximately 6 months earlier than the study group (Hansa et al., 2020). Nevertheless, the available studies lacked crucial information regarding the severity of orthodontic malocclusion at baseline between the two groups (Hansa et al., 2018). Therefore, it is possible that the non-significant difference in treatment duration may be explained by the heterogeneous clinical need rather than by a lack of effect from DM.
Finally, a possible trend towards a better aligner fit when DM was implemented was also suggested by a study performed during the retention phase (Sangalli et al., 2021b). In this instance, the protocol utilised was the 3D Monitoring Light®. This function allows remote monitoring of the fit of the retainers through two-dimensional (2D) analysis of the pictures taken monthly by the patient; in addition, it also allows an overlapping of the monthly scans to the initial 3D stereolithography (.stl) file performed at the time of the debonding of the appliance (Sangalli et al., 2021b). This additional system permits the early detection of undesirable tooth movements that could result in orthodontic relapse.
Limitations
This review has several limitations. The first and most important limitation is the limited and heterogeneous studies available in the literature on this new technology. Specifically, the 11 included papers were characterised by a relatively low number of participants (1–159), and three of them were case reports, known to have a low methodological rigor. The reason behind the inclusion of case reports was an effort to encompass all available evidence, given the relatively recent introduction of DM in the market in contrast to the lengthy duration needed for conducting high-quality research study. Nevertheless, the low-quality design of the studies involved (such as case reports and retrospective studies) increases the risk of bias and limits the strength of the evidence they provide. Another consideration is that the included studies were heterogeneous in terms of the age of patients (ranging from children to adults), of orthodontic system to which DM was applied (aligners vs. self-ligating and/or conventional fixed appliance) and of orthodontic approach (surgical vs. non-surgical). Moreover, a short observation period does not permit us to draw any long-term conclusions.
Other limitations include that the current review summarised results from published sources in an area that could face important clarifications on the basis of new scientific literature. Moreover, the search was limited to the English language, which further increases the risk of publication bias. In addition, this review revealed that the majority of the published data on DM derived from two major research groups which increases a risk of research bias. Therefore, new studies from a different investigation team are needed to replicate these findings. Finally, the present review focused on the implementation of DM within the orthodontic field; as such, these results cannot be extrapolated to any other fields of dentistry. Future studies involving all the other dental specialties are strongly advocated, as to the best of our knowledge there has been only one investigation conducted so far in patients with periodontal diseases (Shen et al., 2022).
Future direction
The present review allowed us to highlight important gaps in the data available in the literature on new remote technologies, such as DM. Thus, new studies with a rigorous design and methodology are strongly advocated. Such studies should prefer a prospective randomised controlled design, preferably with a stratified randomisation approach that assigns the participants based on specific baseline characteristics to ensure balance between the groups (e.g. age, gender, severity of malocclusion, etc.). A sample size calculation should be performed to detect a clinically relevant treatment effect. The study design should involve the comparison with a control group, to determine the effect size of the intervention and increasing the strength of causal inferences. The available studies have applied DM to heterogeneous orthodontic systems and approach; instead, limiting the application of DM to a selected technique would allow for the control for potential confounding factors. An appropriate observation period is essential to control for regression to the mean. Finally, considering the potential Hawthorne effect of participants aware of being a part of interventional studies, some additional strategies can be adopted, including a blind design or the delivery of a similar appliance to the control group with no potential of remote monitoring.
Conclusion
The results of this systematic review revealed that DM integrated into the standard orthodontic care can significantly decrease the number of in-office visits during an ongoing orthodontic therapy. The use of DM also showed some support for improved aligner fit. Nevertheless, no difference was observed in terms of treatment duration and number of emergency appointments when DM was utilised. The findings also highlight the need of new studies performed from different investigation teams, using rigorous design and methodology.
Supplemental Material
sj-docx-1-joo-10.1177_14653125231178040 – Supplemental material for Effectiveness of dental monitoring system in orthodontics: A systematic review
Supplemental material, sj-docx-1-joo-10.1177_14653125231178040 for Effectiveness of dental monitoring system in orthodontics: A systematic review by Linda Sangalli, Anna Alessandri-Bonetti and Domenico Dalessandri in Journal of Orthodontics
Supplemental Material
sj-docx-2-joo-10.1177_14653125231178040 – Supplemental material for Effectiveness of dental monitoring system in orthodontics: A systematic review
Supplemental material, sj-docx-2-joo-10.1177_14653125231178040 for Effectiveness of dental monitoring system in orthodontics: A systematic review by Linda Sangalli, Anna Alessandri-Bonetti and Domenico Dalessandri in Journal of Orthodontics
Supplemental Material
sj-docx-3-joo-10.1177_14653125231178040 – Supplemental material for Effectiveness of dental monitoring system in orthodontics: A systematic review
Supplemental material, sj-docx-3-joo-10.1177_14653125231178040 for Effectiveness of dental monitoring system in orthodontics: A systematic review by Linda Sangalli, Anna Alessandri-Bonetti and Domenico Dalessandri in Journal of Orthodontics
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.