
Abstract
A 16-year-old female patient presented to the orthodontic department with a 2-week history of painful oral lesions that were affecting her ability to eat. Clinical examination revealed widespread oral ulceration, crusted bleeding from the lips with evidence of a herpes simplex infection in the region of the right buccal commissure. A diagnosis of oral erythema multiforme (EM) was made after a detailed clinical history and examination by the oral and maxillofacial team. Supportive care was provided alongside management with topical corticosteroids. Within 6 weeks of initial presentation, complete resolution of the lesions had occurred and the patient was able to resume active orthodontic treatment.
Keywords
Introduction
Historically, erythema multiforme (EM) has been described as a mucocutaneous disorder resulting from an allergic host response to an antigenic challenge with a range of expressions from mild (EM minor) to severe, potentially life-threatening Stevens–Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) (Ayangco and Rogers, 2003). More recently, EM, SJS and TEN have been described as separate diagnostic entities with well-defined criteria to distinguish between them (Williams and Conklin, 2005). TEN and SJS are more severe conditions than EM with widespread cutaneous and mucosal involvement, atypical target lesions, positive Nikolsky’s sign and prodromal flu-like symptoms. TEN and SJS tend to affect older patients and are associated with a significant risk of mortality (Al-Johani et al., 2007).
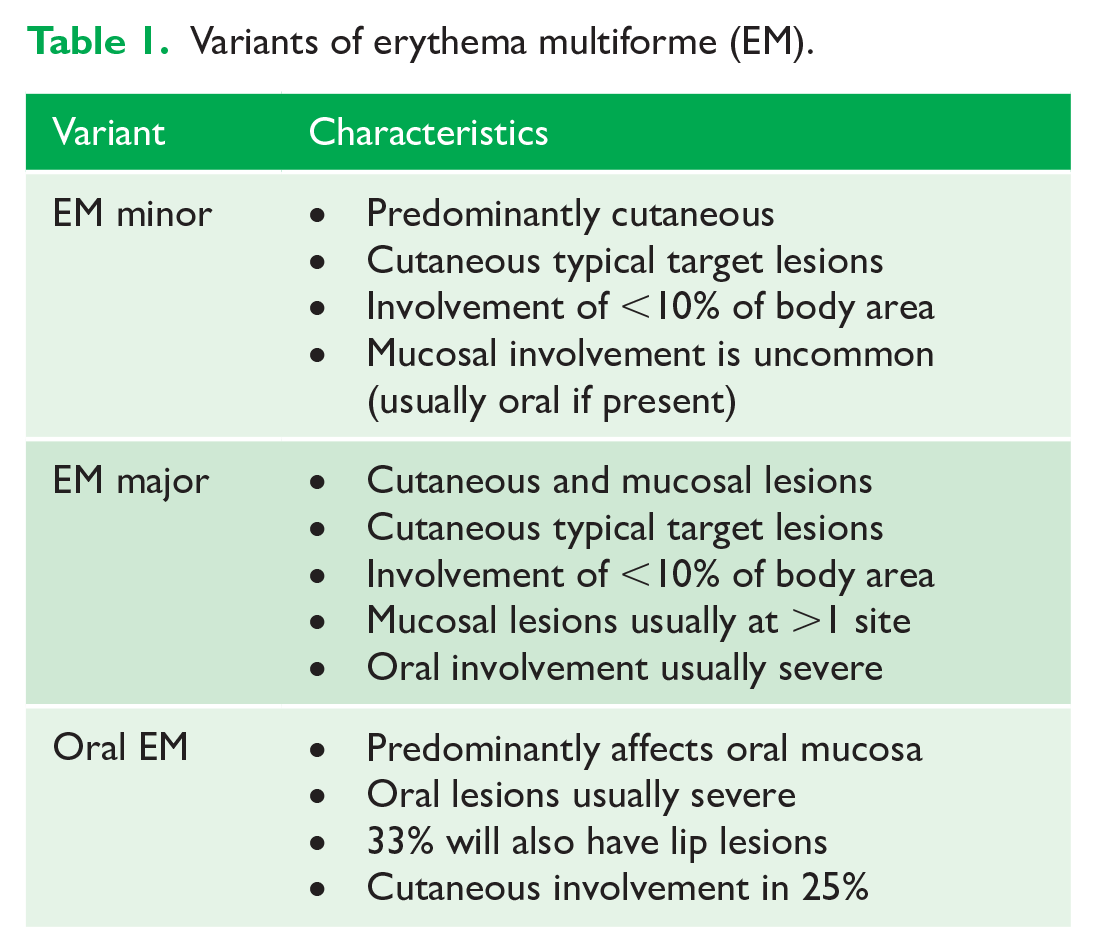
There are two variants of EM: EM minor and EM major Table 1. A third category, oral EM, has been described; however, there is debate as to whether it is a distinct condition or merely a form of EM major with a predominantly oral presentation (Ayangco and Rogers, 2003). This case describes the presentation of EM to an orthodontic clinic.
Variants of erythema multiforme (EM).
Case report
We report a case of a 16-year-old female patient who was undergoing orthodontic treatment with an upper fixed appliance, which had been fitted 9 months before presentation. The patient requested an urgent appointment complaining of discomfort associated with the appliances. The patient and her mother felt that the symptoms were a result of a reaction to her appliances.
She gave a 2-week history of progressively worsening painful lesions affecting the oral mucosa and peri-oral tissues. Her symptoms began with a small area of discomfort in the region of the right oral commissure. She sought the advice of her general medical practitioner a few days later, when it was noticed that ulceration had begun to appear on the lips and tongue.
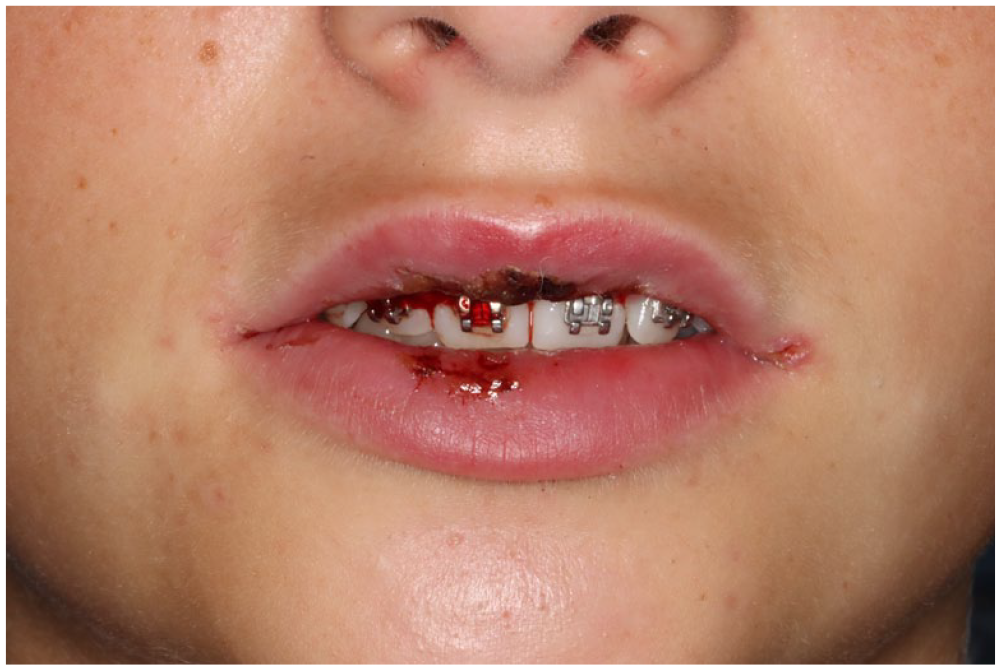
One week after the initial symptoms, the patient attended her local Accident and Emergency Department as she had developed bleeding lips and was now struggling to eat and drink. She was prescribed a 7-day course of oral co-amoxiclav and attended the orthodontic outpatient department 14 days after the onset of symptoms after showing no improvement (Figure 1).

Initial presentation.
On examination extra-orally, there was a cluster of vesicles present in the right oral commissure. The lips were crusted and blood-stained with extensive underlying ulceration, which extended to the buccal and labial mucosa intra-orally. Painful fissuring of the labial mucosa was present in a pattern commensurate with the position of the orthodontic brackets and wire. Erosions were also present on the dorsal tongue and posterior oropharynx. Oral hygiene was poor, with gross deposits of plaque around the appliance and associated gingivitis. The patient remained systemically well and had no visible skin lesions.
The patient was reviewed by a member of the oral and maxillofacial surgery team and a diagnosis of EM, secondary to a herpes simplex virus (HSV) infection, was made based on the history and clinical findings. A 5-day course of prednisolone mouth rinse alongside benzydamine hydrochloride spray and topical lidocaine was prescribed by surgical colleagues. The patient complained of multiple missing elastomeric modules so the decision was taken to remove the archwire to allow improved oral hygiene and reduce further trauma to the labial mucosa. It was not considered in the patients interests to retie a new archwire given her significant discomfort and the presence of herpetic lesions. All staff present followed the departmental cross-infection control protocol and wore personal protective equipment including a full face visor. The patient was provided with a disposable bib and full eye protection.
On review, after 7 days, the vesicles had resolved along with most of the labial lesions. The ulceration to the tongue and oropharynx had healed. Some crusting of the lips remained; however, the patient was now comfortable and able to eat and drink normally. Oral hygiene had improved markedly (Figure 2).
The patient reviewed at 1 week.
Six weeks after the start of symptoms, the patient was reviewed jointly and there was complete resolution of all lesions. Advice was given to remain vigilant to the development of new oral, or skin, lesions and an appointment was made to recommence her orthodontic treatment. The patient’s general medical practitioner was contacted and informed of the presentation and management.
Discussion
Pathogenesis
The antigenic challenge that results in EM is usually infective or pharmacological in origin and appears to be a T-cell mediated immune reaction to HSV DNA fragments or reactive drug metabolites (Scully and Bagan, 2008). In children with oral EM, a systematic review found HSV and Mycoplasma pneumoniae to be the most common causes of recurrent EM, with pharmacological causes being more common in cases of non-recurrent EM, especially in infants after vaccination. The cause was found to be idiopathic in 8.5% of non-recurrent and 25% of recurrent cases (Zoghaib et al., 2019).
In the case presented, the initial cold-sore like lesion fits with an aetiology of HSV. The patient’s lesions appear to have been misdiagnosed as a bacterial infection on initial presentation in the Accident and Emergency Department and an inappropriate prescription of antibiotics was dispensed. Accuracy in diagnosis of viral or autoimmune lesions is important as antimicrobial drugs prescribed unnecessarily not only contribute to antimicrobial resistance (Costelloe et al., 2010) but can themselves trigger EM or cause hypersensitivity reactions.
While co-amoxiclav has been identified as a drug linked to EM, the timeline of symptoms in this case does not fit with a pharmacological cause (Benjamin and Mueller, 1999).
Diagnosis
Oral EM lesions typically affect the non-keratinised mucosa and are often associated with swollen, cracked and bleeding lips. Diagnosis is largely clinical, and it may be difficult to distinguish between oral EM, bullous disorders or viral stomatitis. An acute and recurrent nature of onset, alongside a pattern of lesions affecting the lips and anterior oral mucosa, are suggestive of a diagnosis of EM (Scully and Bagan, 2008).
Cutaneous ‘target lesions’ of the extensor surfaces of the extremities can also aid with diagnosis; however, the presence of such lesions is variable (Celentano et al., 2015). Direct immunofluorescence can help to exclude auto-immune bullous disorders in cases where a diagnosis is not possible based on clinical signs and symptoms alone (Trayes et al., 2019). In this case, the pathognomonic crusted bleeding lips alongside a pattern of severe oral ulceration, which was more prominent anteriorly, was felt to fit a diagnosis of oral EM.
Management
Symptoms of oral EM are usually self-limiting; however, analgesia can be useful in helping patients to maintain oral intake of fluids and food and hospital admission for supportive care may be required in severe cases. The evidence base for the use of corticosteroids is lacking; however, their topical use may be of benefit and they are commonly prescribed (Scully and Bagan, 2008). In severe or recurrent cases, systemic corticosteroids or immunosuppressant drugs may be indicated. If concurrent herpes simplex infection is suspected, non-urgent dental treatment should be postponed to reduce the risk of spreading the infection, or more severe complications such as herpetic whitlow or keratitis (Lewis, 2004).
Prognosis
Resolution of oral EM usually occurs without complication. However, cases of lip adhesion in paediatric patients have been reported after the healing of labial lesions (Ashton et al., 2018; BaniHani et al., 2015). Surgical separation of the lips, or even local flap repair, has been required in cases where the formation of such adhesions has not been recognised in a timely manner. Recurrent EM has been shown to make up 14.3% of paediatric cases, with the predominant aetiology being HSV infection (Zoghaib et al., 2019). This risk of recurrence was highlighted to the patient in this case, who was warned to be vigilant to intra-oral and extra-oral signs of EM in the future.
Conclusion
Despite oral EM being an uncommon and largely self-limiting condition, it is an important differential diagnosis of which all dental professionals need to be aware. Cases presenting in an orthodontic setting should be urgently referred to confirm the diagnosis and initiate any supportive treatment. Close follow-up is required in the short term and patients should be made aware of the risk of recurrence, especially in cases where an infective aetiology is suspected.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.