
Abstract
Background:
Good communication is fundamental to provision of information and patient engagement in orthodontic treatment. Images can be used to support verbal and written information, but little is known about how laypeople interpret orthodontic images.
Objective:
To explore laypeople’s understanding and preferences for images (clinical photographs and medical illustrations) relating to orthodontic diagnoses and treatments.
Design:
Cross-sectional survey.
Setting:
UK.
Population:
Laypeople aged ⩾16 years.
Methods:
Participants were recruited through social media to complete an online questionnaire containing six pairs of images (clinical photograph and medical illustration) relating to orthodontic diagnoses and treatment. Photographs were selected from a bank with input from laypeople, then a matching medical illustration was created. Images were presented with questions relating to interpretation, preferences and reasons for preferences.
Results:
A total of 898 people completed the questionnaire. Interpretation of images by laypeople was variable and, in some cases, normal intra-oral features and image orientation caused confusion. A combination of photograph and illustration were preferred for images representing diagnosis (by 41%–50% participants), whereas the illustration alone or both photograph and illustration together was preferred for explaining treatment (43%–48% and 35%–44%, respectively). Photographs were liked for their realism and relatability, while illustrations were often found to be clearer. Arrows aided participants’ understanding of the images, but annotations were requested to further improve the value of images. Only 26% of participants reported having previously been shown dental images, but 96% felt they would be helpful to support verbal and written information.
Conclusion:
Laypeople may not interpret orthodontic images in the way that professionals expect, and unfamiliar intra-oral features may distract people from the intended focus of the image. A combination of photographs and illustrations together may improve the usefulness of images, alongside annotation or explanation.
Introduction
Good communication and effective sharing of information between the clinician and patient is fundamental to patient engagement in treatment decisions and informed choices (Mulley et al., 2012). Effectively engaging patients in care choices has been shown to improve knowledge, risk perception and communication, while reducing overtreatment and decisional regret (Hoffman et al., 2014).
Orthodontic consultations are often heavy with new information, and it is recognised that patients and parents may struggle to understand or utilise this information effectively. Multiple interventions have been developed to try to improve understanding and recall of information or engagement in care choices (Shelswell et al., 2021) to facilitate informed patient choices and shared decision making. The NHS (2021) is committed to improving the quality and accessibility of health information to improve health literacy and promote patient involvement in choices. Patient information leaflets (PILs) are commonly used to support verbal provision of information; however, examination of orthodontic-related PILs found they are variable in content, dense with complicated language and often not able to promote patient engagement in treatment choice (Barber et al., 2018 ; Bekker et al., 2010; Harwood and Harrison, 2004; Seehra et al., 2016).
Visual aids may be useful in supporting verbal information provided by the orthodontist to support the consultation process and improve patient understanding of what treatment will entail. There is evidence that information presented audio-visually may be better retained by orthodontic patients (Al-Silwadi et al., 2015; Anderson and Freer, 2005; Patel et al., 2008); however, patients’ perception of images, both within written information and as an adjunct to verbal information during consultation, has not yet been explored in orthodontics.
A review of pictures used in health communication found they can increase attention and recall of information and improve understanding of concepts and spatial relationships. The benefit was especially marked for people with low literacy. Interestingly, it was also found that the emotional response to pictures moderates their effect on target behaviours and adherence (Houts et al., 2006). No existing evidence could be found that examines laypeople’s emotional response to dental clinical photographs.
The aim of the present study was to explore laypeople’s understanding and preferences for images (clinical photographs or medical illustrations) relating to orthodontic diagnoses and treatments.
Design
A cross-sectional survey of laypeople was conducted using an online questionnaire. Ethical approval was granted by the University of Leeds Dental Research Ethics Committee (approved 7 October 2020) before commencing the study.
The target population was laypeople, including all adults aged ⩾16 years. Participants were stratified by age and level of education, and it was assumed that a large enough sample would include people with variable experience of orthodontics, dental care and health literacy. There is no precedent for sample size so a target of 200 responses was agreed by the research team.
Materials
The questionnaire (included in full in the supplemental material) consisted of:
Introduction and consent
Six pairs of orthodontic images (clinical photograph and illustration). Participants were asked their understanding of the images then their preference for images once an explanation had been provided. A free-text box was provided to allow participants to give additional information about their interpretation and preferences
Questions about participant’s experience of dental information provision, the perceived usefulness of images and their general preference for written or visual information
Non-identifiable demographics (age, gender, geographical location, highest educational level, ethnicity) based on the categories used by the Office for National Statistics
Three cases were presented relating to diagnosis of a dental anomaly (Class III malocclusion, anterior open bite, enamel opacity on a central incisor) and three relating to orthodontic treatment (dual arch fixed appliance with intra-arch class II elastics, a quadhelix appliance, orthodontic closed exposure of an unerupted central incisor with gold chain) (Figure 1). Images were selected from an orthodontic photograph bank with the appropriate level of consent.
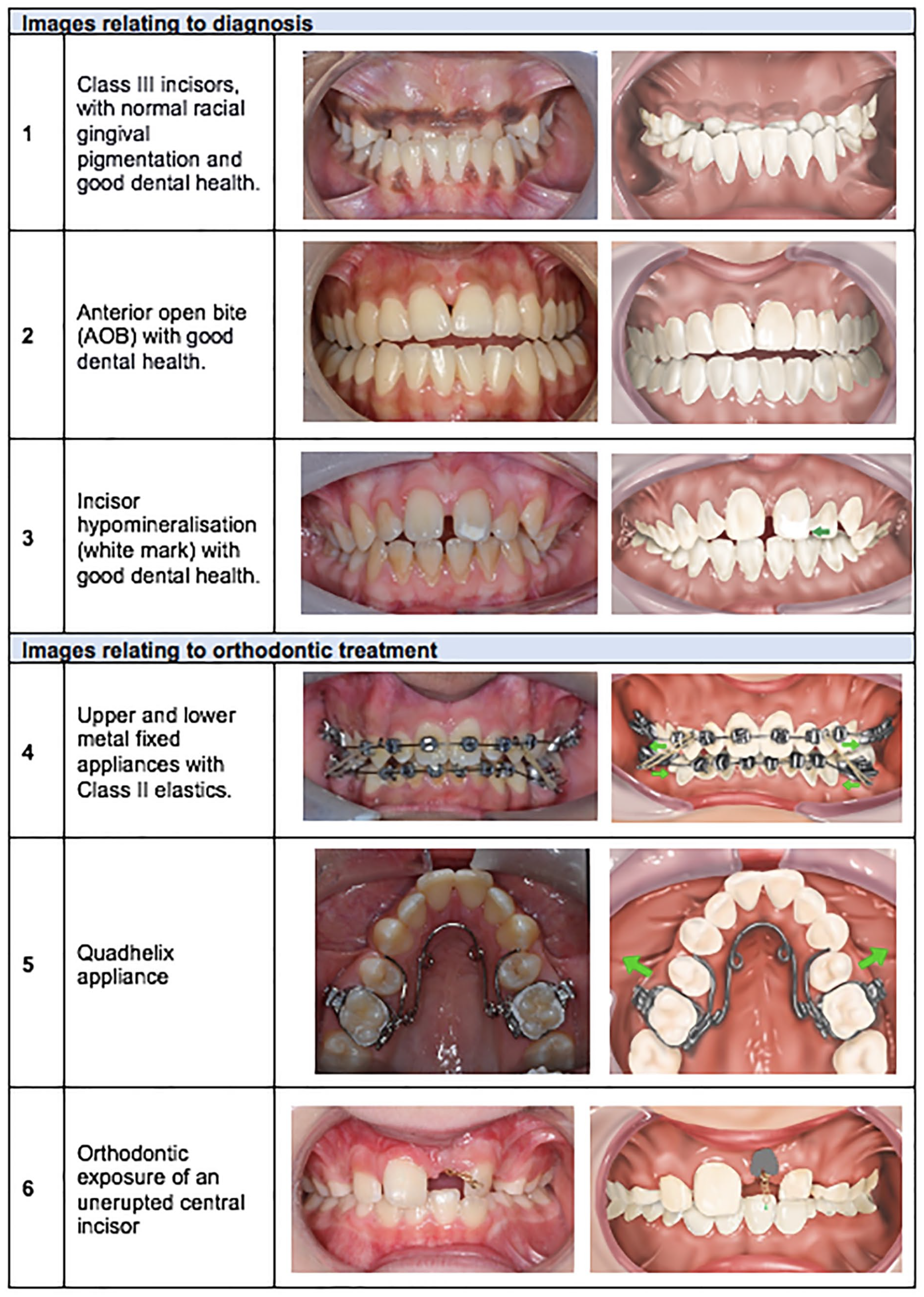
Summary of the pairs of images used.
Images were chosen to show conditions with variable frequency, with the expectation that at least some of the subjects would be new to participants. Feedback was obtained from a small group of laypeople during the selection of images and creation of the illustration by a medical illustrator. This was a convenience sample of people known to the researchers, who were selected to give diversity in age, level of education and dental experience. Feedback led to arrows being added to the illustration and colour balance adjustments in both photographs and illustrations.
The questionnaire was created and programmed using a UK-based GDPR-compliant online survey tool (www.OnlineSurveys.co.uk). The preliminary questionnaire was piloted by the same four laypeople with a researcher present to allow real-time feedback about the design, language and format. In response to feedback, labels were added to the photograph and illustration, changes were made to phrasing and an explanation was added to confirm what the images were designed to show.
Methods
Participants were recruited from social media via a post in several Facebook groups, which were selected with the intention of capturing a range of different people in terms of age, education and dental experience. The groups included a staff group at one bar, a staff group of a supermarket (Iceland) and members of an independent gym with a moderate-to-high cost of membership. A recruitment post was shared on the groups along with an information sheet that described the background and aim of the research. Members were asked to reshare the link to the questionnaire to promote snowball sampling. It was planned that the post would be repeated after four weeks and the questionnaire would be open for a total of eight weeks.
The recruitment post contained a link to the questionnaire. Responses were automatically anonymised and collated by the survey tool then exported into a Microsoft Excel spreadsheet via a secure portal.
Free-text answers were categorised to describe the following: (1) how the images were interpreted; (2) preferences for the different images; and (3) general experience and opinion of use of images.
Results
Data were collected from 7 October 2020 to 28 November 2020 and included a total of 900 participants. Data collection closed slightly earlier than planned because a sufficient number of responses had been collected. Two participants were excluded because their answers were nonsensical joke answers that were judged to be inauthentic, resulting in 898 responses for analysis. The sample consisted of mostly White women with varied levels of education and ages (Table 1). Most participants were based in England.
Characteristics of sample.
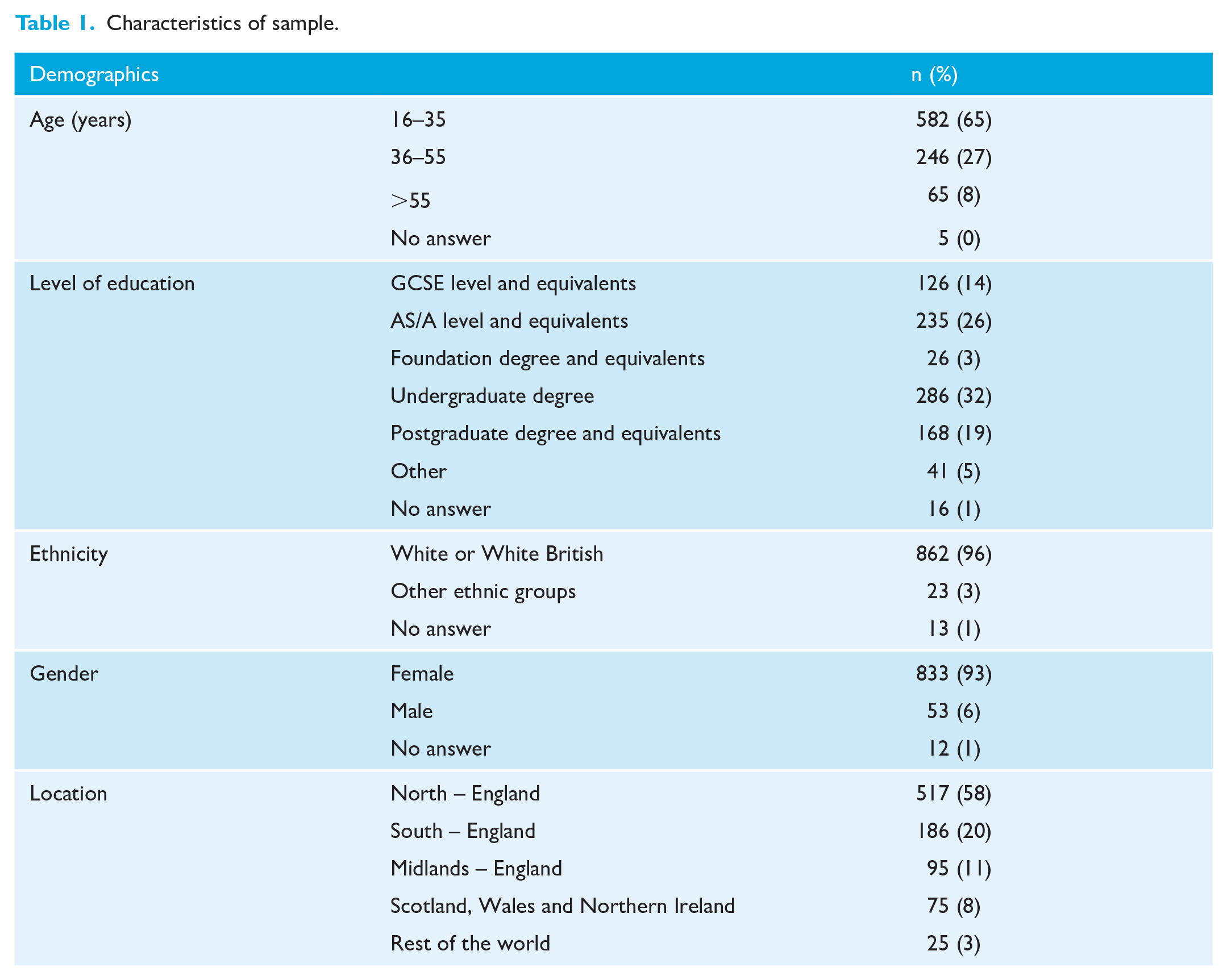
Table 2 summarises how the images were interpreted by participants. For all the images relating to diagnosis, the majority of participants identified the correct diagnosis but used common non-dental terminology, such as ‘underbite’ for the Class III incisors, or gave a description, such as ‘gap between the front teeth’ for anterior open bite. In describing the images, it was apparent that certain features were misinterpreted or distracted from the intended feature. For example, one image demonstrated good oral hygiene and normal physiological pigmentation, but this colouring was commonly misinterpreted as gingival pathology, with 44% participants mentioning ‘gum disease’ within their answer. The upper occlusal image used to show a quadhelix appliance caused confusion about orientation, with a large number of participants commenting on the lower teeth. The unerupted central incisor with gold chain was the most difficult image to interpret, with 21% of participants stating that they did not understand what the image showed.
Laypeople’s interpretation of the images.
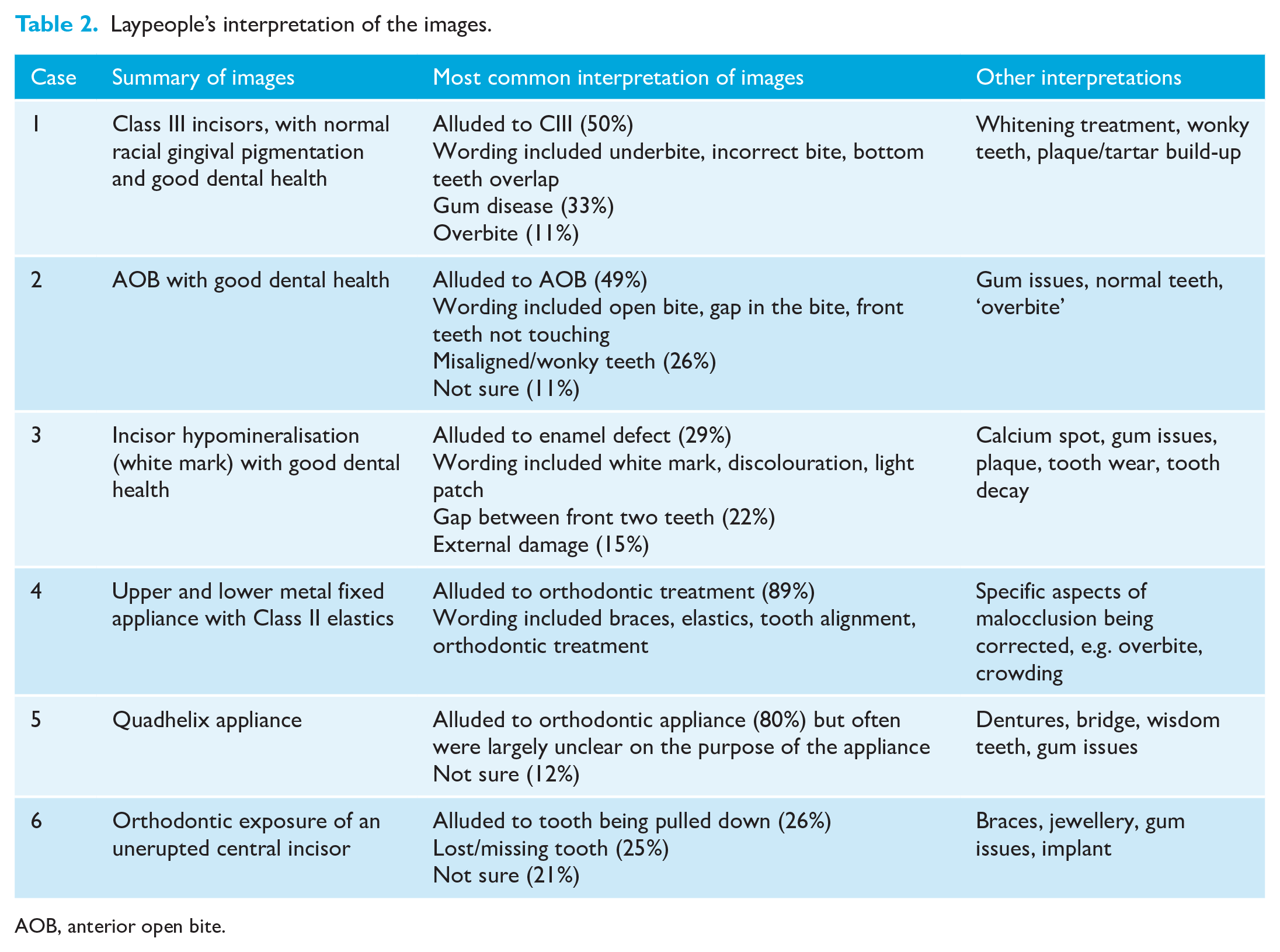
AOB, anterior open bite.
Table 3 summarises participants’ preferences for images. When images related to diagnosis, the majority of participants expressed a preference for having both a clinical photograph and medical illustration together. In contrast, when images showed treatment, there was a greater preference for illustration alone or both images together, but few preferred the photograph alone. This was widely attributed to the inclusion of arrows, which participants thought gave clarity on what the image was demonstrating. When asked about which features influenced their preferences, participants often reported that the photograph was more relatable or realistic. The most favoured aspect of the illustration were the arrows, and some felt that illustrations offered fewer distractions. The ability to combine the reality of the photograph alongside the clarity of the illustration was often the reason for preferring both images together. Those who did not like either image reported this to be because either the images were not clear or they wanted a verbal explanation or annotation alongside the image. Further examples of comments given by participants are included in Supplemental Tables 1 and 2
Laypeople’s preferences for images.
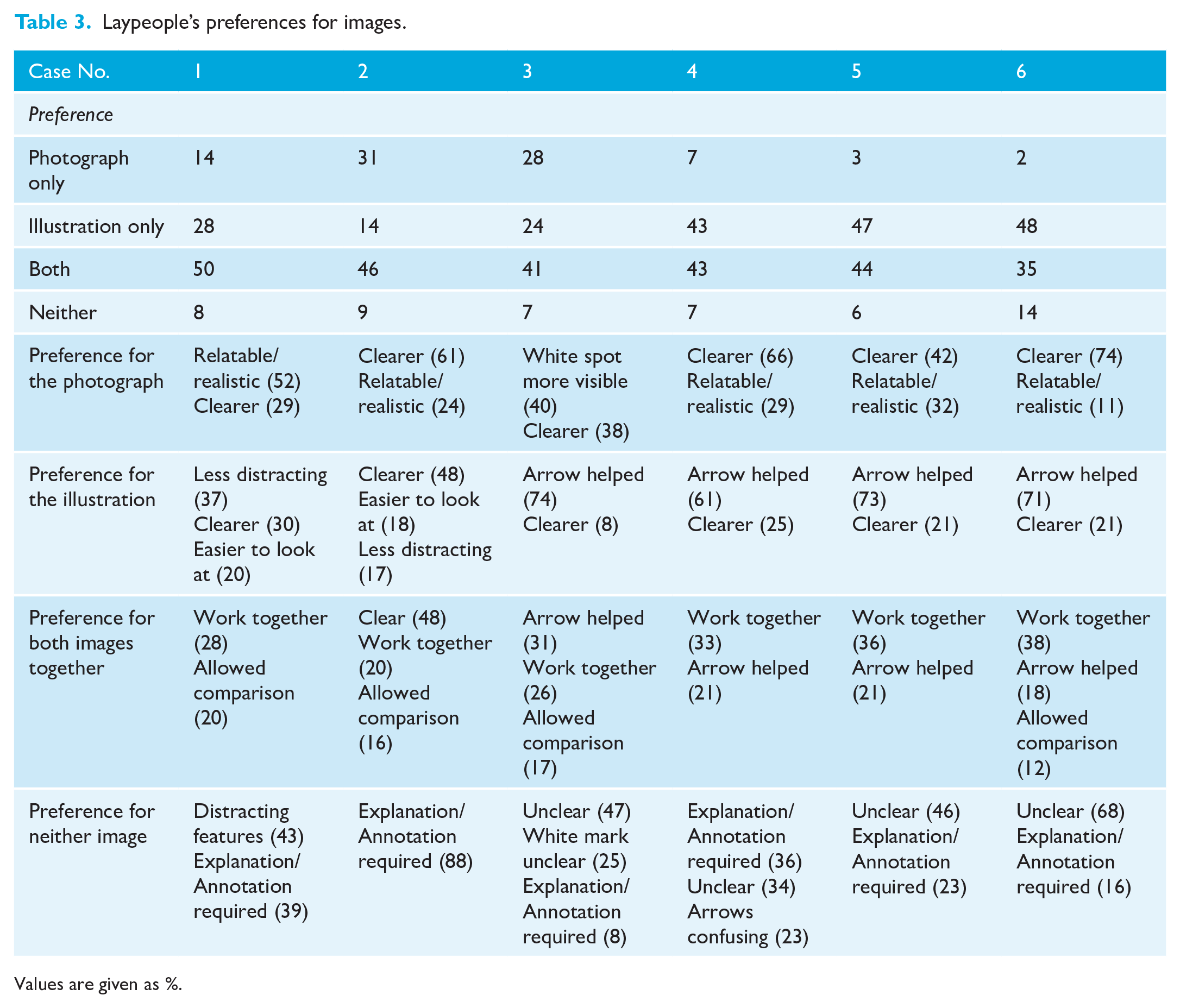
Values are given as %.
Of the participants, 26% recalled that they had previously been shown images when discussing dental treatment, while the majority (59%) reported no use of images and 14% could not remember. The majority of participants (96%) felt that their understanding of treatments and diagnoses would benefit from the use of images to support information delivery. One potential criticism of images was that they may promote procedural anxiety.
When asked about general preferences for receiving information, most people (74%) preferred a combination of written and visual, with one-quarter preferring visual only and a small minority (2%) preferring written information only. A preference for written information was more pronounced in older age groups, although the overall preference was still for images or images alongside written information. Participant preference for images or written information was not affected by level of education.
Discussion
The first important finding from this research is that people may not interpret images as dentists expect and certain features in images may be misunderstood or cause confusion. Gingival pigmentation and a median diastema were found to detract from the intended focus of images, while presenting an occlusal view caused issues with orientation. There was evidence that some photographs evoked an emotional response for some participants, which may affect information processing (Houts et al., 2005). Clinical photographs are widely used in consultations and PILs, so these findings indicate there is value in further exploring reactions to images and how this impacts decision making and behaviour.
Often participants misinterpreted normal variation in physiological pigmentation, which can vary by race, as the main focus of the image. Ensuring diversity and representation in clinical images is important to patients (Hernandez et al., 2021; Murphy et al., 2000) and this raises an important question about how this can be facilitated without introducing confusion. The fact that the majority of participants in this research identified as White/British and were potentially unaware of physiological variation common to other ethnic groups serves to demonstrate the importance of how familiarity and our own experience will influence our perspective. Clinicians have an important role in highlighting the important features of an image and orientating viewers when using unfamiliar images to avoid misunderstanding. Participants highlighted the importance of annotation or verbal explanation to maximise the usefulness of images, suggesting images without explanation will not be helpful, for example, in standalone PILs.
The language used by laypeople to describe what they see may differ to the terminology used by dental professionals. It is widely acknowledged that medical terms can be confusing (Fields et al., 2008) and adults often have a limited understanding of medical jargon (Rau et al., 2020). A lack of shared language between patient and dental professional may be a barrier to effective communication, particularly when discussing concerns and expectations from treatment. Patients may adopt dental terminology to facilitate discussion with their dental professional, but this may conceal misunderstanding about the diagnosis or treatment options. Clarifying patients’ understanding of the diagnosis and treatment, particularly what they mean by specific dental terms, is essential.
The second important finding is that people have varying preferences for different images, so there may not be a single approach to information delivery that suits everyone. Generally, photographs were seen as being more realistic and relatable, while illustrations provided clarity, which suggests a combination of different types of images may be useful. Arrows were incorporated in the illustrations, for example, to show the direction of tooth movement, and commonly participants reported that these arrows aided their understanding. This is supported by other research that found arrows are useful for communicating complex visual information (Wong, 2011). The use of arrows on the illustrations but not the photographs in this study may have created an unfair comparison so it would be useful to assess if arrows are also helpful on photographs. The differing views on the usefulness of images and specific features within the images highlights the important of involving users in the development of resources to ensure their relevance and accessibility (Patient Information Forum, 2021).
The third important finding was that many people do not recall images being routinely to support verbal and written information; however, the majority of participants feel they would find this useful. The low use of images is surprising and may be a consequence of recall bias; however, it is still interesting that in this sample the use of images was not remembered. The sheer volume of studies looking at methods to improve patient engagement, knowledge and information recall across different areas of healthcare emphasises the recognised challenge of effective communication. This is a timely study, given communication between patients and the dental team was identified as a top 10 research topic (James Lind Alliance, 2019). The use of a questionnaire allowed a large number of opinions to be sought, while open questions were included to give an opportunity to elaborate. This has provided rich and useful data about laypeople’s perspective.
There are, however, limitations in the method that must be acknowledged. The sample was predominantly White and female, so the perspective is limited to this population and differing opinions from other groups may not be represented, which has implications for the generalisability of findings. It is debatable whether individual characteristics, such as gender, race and geographical location, would have a significant impact on understanding and preferences. The authors could find no existing evidence or a sound theoretical basis to suggest this is the case, but a more diverse sample would allow the effect of individual characteristics to be explored.
It was assumed that a sample of this size would capture those with variable experience of dental care and orthodontics, but this was not explicitly established and, in hindsight, a question asking about previous dental and orthodontic experience would have been useful. Using social media to distribute the questionnaire to the general public and utilising snowball sampling means the sample may not reflect the intended target audience; however, a high proportion of participants reflected on their own dental experiences in their responses, suggesting they did have experience of being a patient. The decision to sample the general public was made to capture the perspectives of those who may not otherwise have the opportunity to share their opinions; this is important given the inequity in those accessing orthodontic care and the fact most UK orthodontic research is primarily undertaken in secondary care settings.
Considerable thought was given to the particular images and photographs presented to participants. Six images were chosen to avoid excessive demands on participant’s time based on feedback from piloting. The style of image used, diagrammatic similarity between photograph and image, and use of explanatory arrows or labels are all design choices likely to impact on participant preferences. Our choices reflect our own preferences, and it is important to recognise that different images may elicit alternative findings. Is it also true that the types of treatments presented or the severity of malocclusion may have an impact on participants’ responses.
This exploratory research presents some interesting insights into an expansive field and is the first work focussed specifically on orthodontic needs; however, it does not provide sufficient evidence to formulate recommendations for practice. Further research should explore the impact of different images and design choices on patient preferences, as well as examining how images and photographs can be utilised effectively to increase patient involvement in medical decision-making and to support those with low health literacy. A qualitative approach, such as interviews or focus groups, would allow in-depth exploration of opinion and this may be a useful direction for future research.
Conclusion
Laypeople may not interpret orthodontic images in the way that professionals expect.
Unfamiliar intra-oral features and image orientation can distract people from the intended focus of the image.
Arrows may help to emphasise the important features and using a combination of photographs and illustrations together might aid interpretation of information provided in written leaflets.
Only a minority of participants recalled being shown images in the dental setting to support verbal and written information, but the majority felt this would be useful.
Supplemental Material
sj-docx-1-joo-10.1177_14653125221085983 – Supplemental material for Laypeople’s interpretation of, and preference for, orthodontic images
Supplemental material, sj-docx-1-joo-10.1177_14653125221085983 for Laypeople’s interpretation of, and preference for, orthodontic images by Lauren Berry, Adam Jones and Sophy Barber in Journal of Orthodontics
Footnotes
Acknowledgements
Our gratitude to Colin Sullivan for creating the illustrations used in this study. Thank you to the four individuals who piloted the questionnaire and to all participants who completed and shared the survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.