
Abstract
Objective:
To investigate: (1) orthodontists’ training experience in the psychological assessment of orthognathic patients and their wish for training/further training; (2) the availability of psychological support, referral patterns and outcomes after referral; (3) and adverse incidents prompting orthodontists to refer patients for psychological assessment.
Design:
Prospective cross-sectional study.
Methods:
A 25-item questionnaire was designed to investigate the above mentioned aims. After a pilot study, the questionnaire was distributed to all members of the Consultant Orthodontist Group, British Orthodontic Society.
Results:
Based on a 29.1% response rate (n = 102), 76.5% of respondents had undertaken training in identifying orthognathic patients who may benefit from psychological assessment. However, 90.2% favoured further training. All respondents believed that some orthognathic patients would benefit from referral; however, 31.3% of units referred no patients at all, mostly due to limited/no access (66.7%). Most referrals (68.9%) were to psychiatrists/psychologists with dentofacial deformity expertise, with 28.9% of units having such services onsite (14 different units). Psychological referrals had potentially useful outcomes, with 36.4% of respondents sometimes changing treatment plans following referral. Clinical incidents were experienced by 35.1% of respondents, prompting referral of patients for psychological assessment; such incidents included patient suicides (n = 4).
Conclusion:
Most respondents had trained in psychological assessment of orthognathic patients; however there was a large demand for further training. Clinicians value the psychological services available; however, limited availability may affect referrals for some respondents. Adverse incidents are of real concern and highlight the need to ensure that training and resources are provided to support orthognathic patients and teams.
Keywords
Introduction
Psychological evaluation of patients requesting orthognathic treatment is an essential part of the assessment process, which may identify potential concerns and allow management strategies to be put in place in order to provide the best care for patients and reduce patient dissatisfaction (Cunningham and Feinmann, 1998; Heldt et al., 1982). Assessing psychological distress requires detailed psychological assessment by a trained mental health professional, either a liaison psychiatrist 1 or a clinical psychologist 2 . However, orthognathic team members need to be able to identify patients who require onward referral to a mental health professional for further support that is outside their competency (Benkimoun, 2005).
People with dentofacial deformities may encounter psychological stress, either directly from external reactions, such as teasing, or indirectly from sociocultural preconceptions or stereotyping (Phillips et al., 1998). There may also be internal psychological issues based on the patient’s own response to their visible difference (Cunningham, 1999). Evidence suggests that up to 50% of patients referred to an orthognathic assessment clinic experience what would be classified as ‘psychological distress’ (Rivera et al., 2000). Cunningham et al. (2000) conducted a comprehensive multicentre study involving 81 orthognathic patients, investigating their psychological profile and comparing them with a control group of 95 non-patients. This study concluded that orthognathic patients demonstrated significantly higher levels of state anxiety than non-patients 3 (P < 0.001). Collins et al. (2014) also noted that 42% of patients requesting orthognathic surgery reported depressive symptoms and 23% reported anxiety.
Another potential condition that must be recognised in orthognathic patients is body dysmorphic disorder (BDD), which is defined as body image disturbance associated with a preoccupation with perceived but minor or non-existent flaws or abnormalities in one’s appearance (American Psychiatric Association, 2013). However, the diagnosis of BDD is not as clear-cut as that definition may appear and it is possible to have a diagnosis of BDD even where there is a clear physical deficit present if the level of distress and diminished functioning are sufficient (Sarwer et al., 1998). A recent systematic review by Veale et al. (2016) estimated that the prevalence of BDD in orthognathic patients is 11.2%, considerably greater than the 1.8% quoted for the general adult population (Buhlmann et al., 2010). A study by Veale et al. (1996) involving 50 patients who fulfilled the criteria for BDD, found that 24% had attempted suicide, highlighting BDD as a serious handicapping disorder. Therefore, it is vital that conditions such as depression, anxiety and BDD must be recognised in orthognathic patients.
There is currently no research available investigating clinical incidents, such as self-harm and suicide, in orthognathic patients but those seeking aesthetic procedures have been identified to be at higher risk of these incidents than the general population (Lipworth and McLaughlin, 2010; Veale, 2018). With such serious clinical implications in other areas of medicine, these aspects need to be investigated in relation to orthognathic patients. According to RCS guidelines (2013, 2016), clinicians must:
consider their patients’ vulnerabilities and emotional requirements;
discuss possible unfavourable physical and emotional impacts of orthognathic treatment;
avoid or defer treatment pending psychological evaluation, where there are concerns.
It is therefore not surprising that NICE (2005) guidelines recommend that any clinician involved in a specialty where they may encounter patients suffering from BDD should have an established referral pathway to a mental health professional experienced in the management of BDD.
In order to recognise those patients that need additional psychological support, all members of the orthognathic team need training in this area to be able to refer patients appropriately. In a previous questionnaire-based study distributed to all consultant orthodontists in the UK, Juggins et al. (2006) identified that approximately 10.7% of respondents did not believe that any of their patients would benefit from referral for psychological assessment. Furthermore, 30.5% of respondents did not refer any orthognathic patients, as they had nobody to refer to.
Juggins et al. (2006) identified a lack of training experience in the UK; 80.8% of the respondents had no formal teaching in psychological assessment/ management of orthognathic patients. The importance of providing appropriate training in these areas has been recognised more recently in the Post CCST training guidelines (Joint Committee for Postgraduate Training in Dentistry Specialty Advisory Committee in Orthodontics, 2012). This document describes training related to psychology in relation to craniofacial abnormality and multidisciplinary management of facial deformity and specifies that trainees must possess a detailed understanding and clinical experience of the multidisciplinary approach for the treatment of patients requiring orthognathic treatment. There is clearly a training need in this area; however, there is no literature available which describes the format of training experience which orthodontists would value, nor any specific areas of interest in this field to orthodontists.
Aims and objectives
The aim of the present study was to develop an online questionnaire to investigate:
Training: including the format of training undertaken and respondents’ thoughts on future training needs.
Referral patterns for psychological assessment of orthognathic patients: this included the percentage of patients whom orthodontists believe would benefit from psychological referral, the actual percentage referred, reasons for referring/not referring, the support available, how often treatment plans are changed following referral and orthodontists’ perceptions of the service available.
Adverse incidents: which may have made orthodontists more likely to refer patients.
Materials and method
Data protection and ethical approval (reference number Z6364106/2018/08/46) were granted from UCL Data Protection and Ethics Committees and a ‘Privacy Notice’ was placed at the start of the questionnaire in compliance with the General Data Protection Regulation. The questionnaire was developed through a number of different approaches, starting with the eight-item questionnaire utilised by Juggins et al. (2006) and building on that through a thorough search of the literature, discussions within the research team and with other interested parties; a 25-item questionnaire was developed using this approach.
The questionnaire was divided into five main areas:
Demographics
Training experience and perceptions of further training
Referral patterns
Recipients of referrals for psychological evaluation
Orthodontists’ perceptions of the service available
A pre-pilot of the questionnaire involved members of the research team testing the questionnaire and making appropriate adjustments. Seven consultants with a known interest in this aspect of patient care were then contacted to participate in a further pilot through a link to SurveyMonkey®, an online survey site.
Once the final version of the questionnaire was agreed, a link to the SurveyMonkey survey was distributed to all members of the Consultant Orthodontist Group of the British Orthodontic Society (BOS). The initial email was sent on 5 November 2018 followed by two reminder emails; the survey closed on 21 December 2018.
Results
A total of 107/350 (30.6%) responses were received. Five respondents were excluded due to incomplete data, leaving 102 (29.1%) responses included in the final analysis. Analysis of the data was performed using SPSS for Windows package Version 22+. Of the 102 respondents, a number worked in more than one unit. Therefore, the total number of units represented was 131. All of the respondents had completed their training in the UK or Republic of Ireland and also currently worked in these areas.
Aim 1: Training
The majority of orthodontists (n = 78; 76.5%) had undertaken some form of training in the identification of orthognathic patients who may benefit from psychological assessment. Of these, 52.0% underwent informal teaching, such as mental health professionals advising on patient management skills in a clinical situation, and 35.3% had formal teaching as a postgraduate. The format of training primarily involved clinical teaching (55.1%) and one-off teaching episodes (34.6%). The majority of orthodontists (90.2%) felt that they would benefit from further training and the most commonly selected area of interest (84.8%) was how to discuss psychological referrals with their patients (Table 1).
Respondents’ interest in different aspects of further training.*
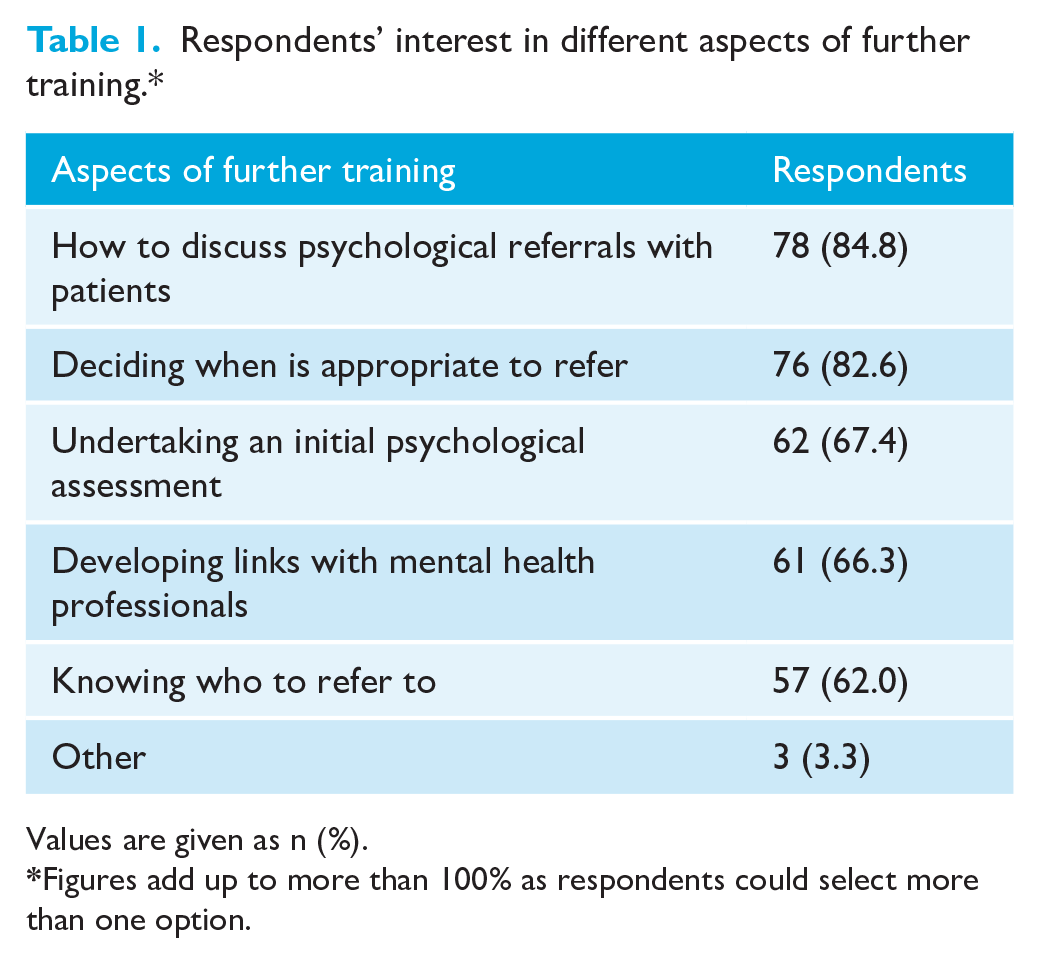
Values are given as n (%).
Figures add up to more than 100% as respondents could select more than one option.
Aim 2: Referral patterns
All of the units represented had some patients who were perceived to be in need of referral for psychological assessment (Figure 1). Of those orthodontists who said that they actually refer patients for psychological assessment (n = 77), by far the most common reason for referral was that ‘the patient’s concern was out of proportion to their dentofacial problem’ (63.6%) (Table 2). All units who referred patients reported doing so before treatment, rather than during or after treatment. A variation existed in the recipients of referrals; but the majority of units referred to psychologists (61.1%), rather than psychiatrists (38.9%). Of the units, 54.4% referred to offsite mental health professionals, while 43.4% referred to specialists who were on-site; the remaining respondents were unsure. The majority of units (68.9%) referred to mental health professionals who had expertise in managing patients with dentofacial deformity, with 28.9% of units fortunate in having such a colleague onsite (14 different units).
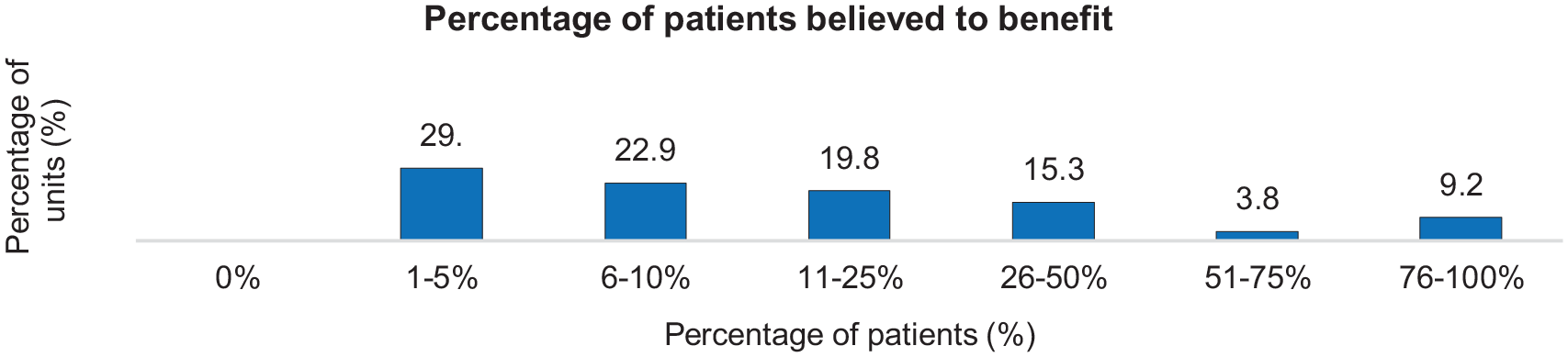
Percentage of orthognathic patients believed to benefit from psychological referral.
Single most common reason for referral of patients for psychiatric assessment.
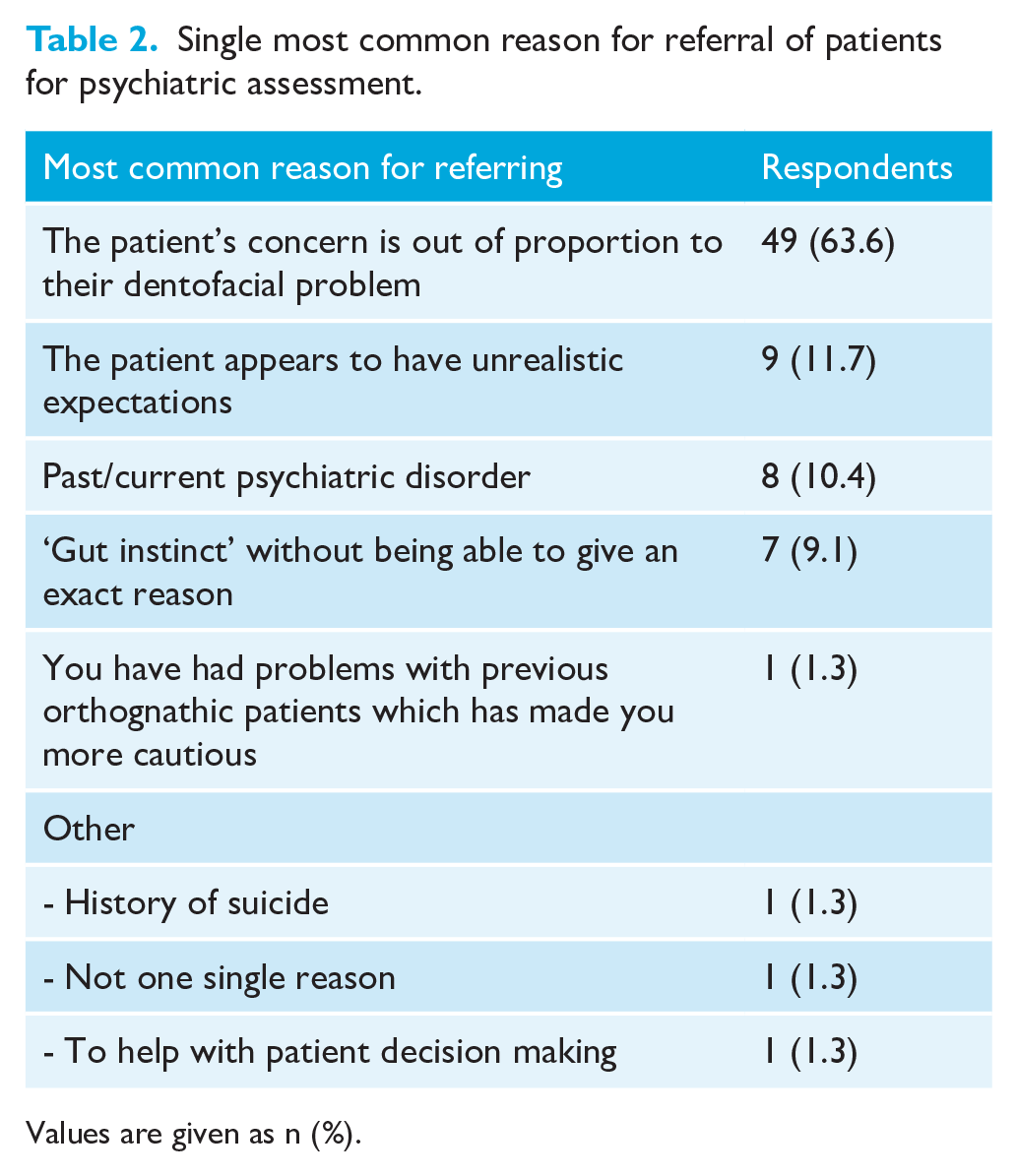
Values are given as n (%).
Of the orthodontists who said they did refer patients (n = 77), half (50.6%) reported rarely changing treatment plans after a psychological referral, 36.4% reported sometimes changing treatment plans and 13.0% reported never changing plans.
In the majority of units (68.7%), some patients were referred for psychological assessments. However, in 31.3% of units, no patients were referred (Figure 2). The most common reason preventing respondents from referring was that they had nobody to refer to or had limited access. Other reasons for not referring are displayed by Table 3.
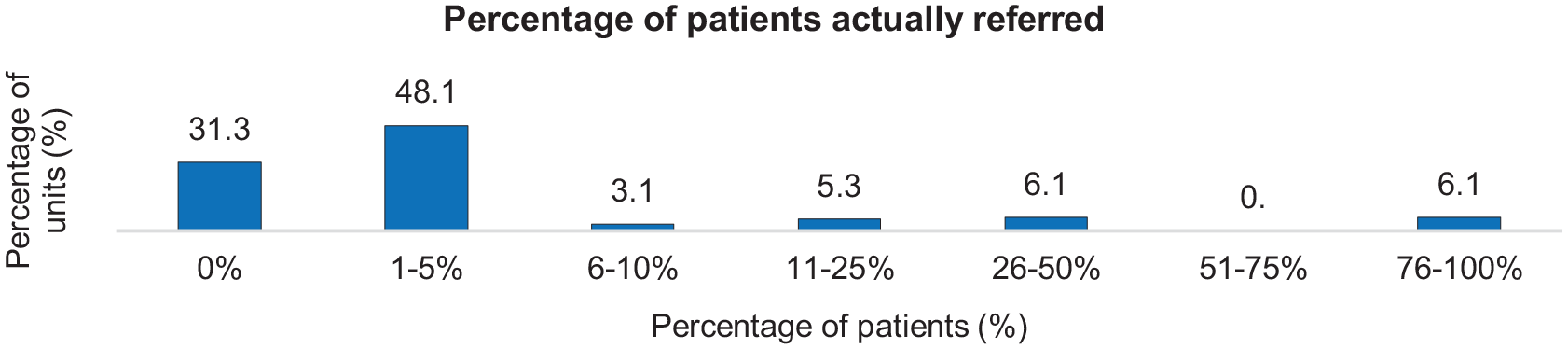
Percentage of orthognathic patients actually referred.
Respondents’ most common reasons for not referring for psychological assessment.
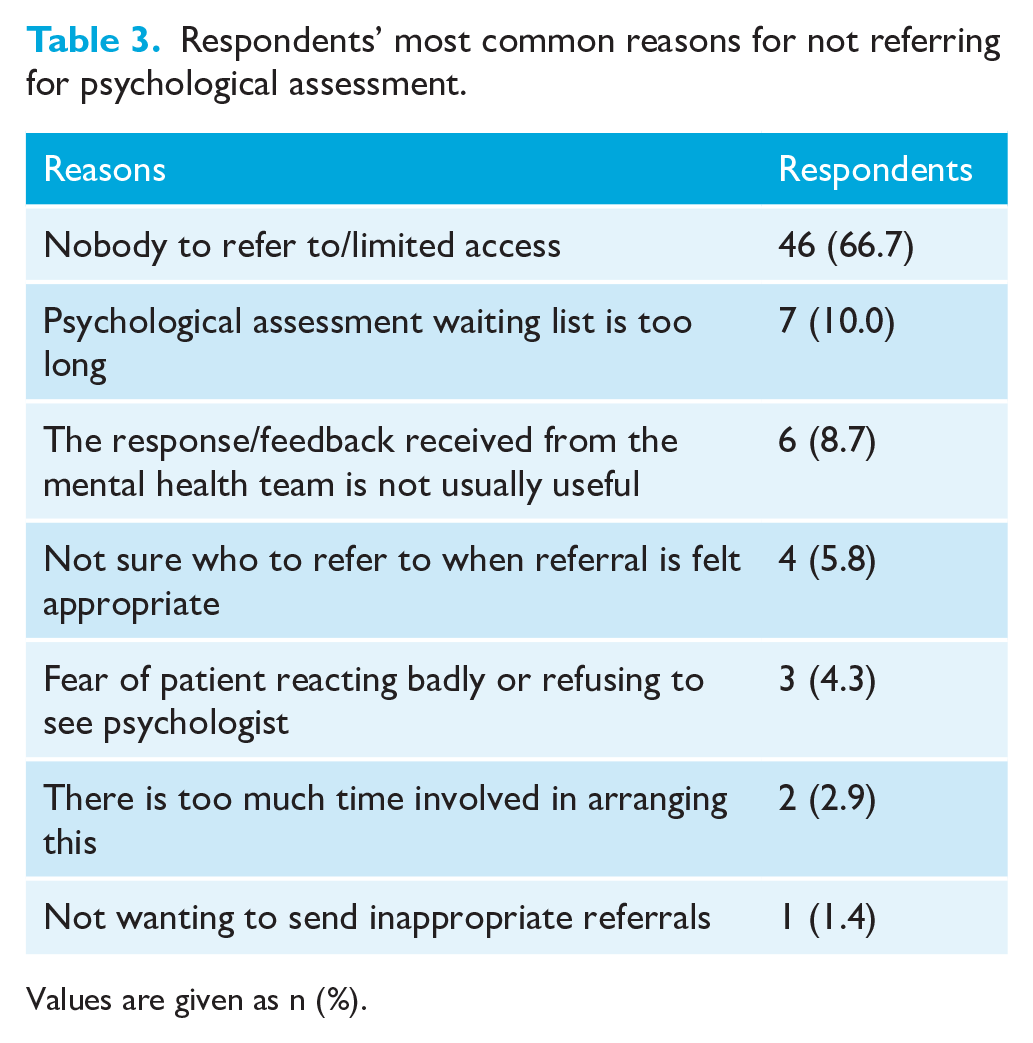
Values are given as n (%).
The psychological service available locally was rated as good by 27.5% of units; however, in 14.5% of units the service was rated as poor. Comments regarding available services are displayed in Table 4. With only 28.9% of units having a mental health professional attend their orthognathic clinics, the majority of respondents are dependent on psychological reports provided and these were rated as good by 28.2% of units, but poor by 13.0%.
Examples of comments regarding psychological services provided.
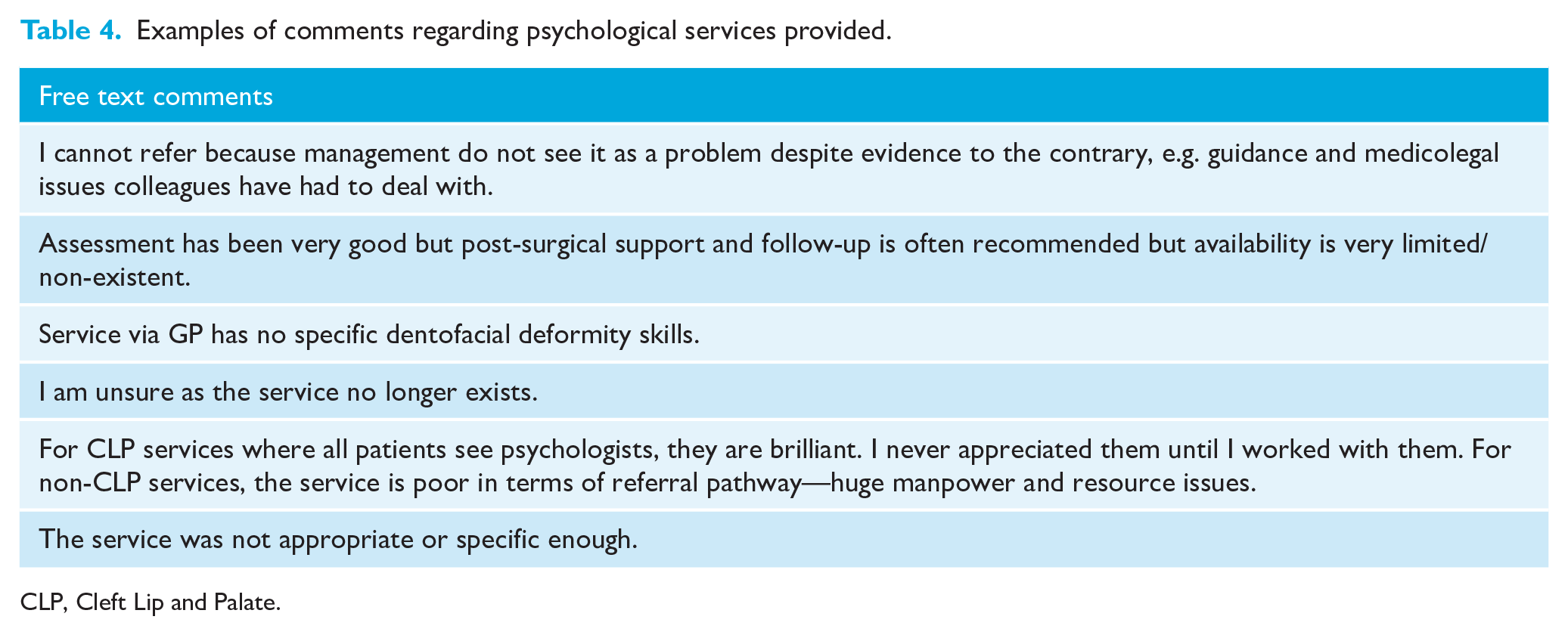
CLP, Cleft Lip and Palate.
The data were analysed to determine whether the number of years since qualification was significant in affecting the percentage of patients whom respondents believed would benefit from referral; however, this was not found to be significant (P = 0.22). Therefore, those who were less experienced did not appear to refer more or less frequently. Nor did the number of orthognathic patients assessed by a clinician each year significantly affect the number of patients perceived to be in need of referral (P = 0.32). Thus, those who saw fewer patients did not appear to refer patients more frequently.
Aim 3: Adverse incidents
Of those orthodontists who referred orthognathic patients, 35.1% (n = 27) had experienced incidents which made them more likely to refer patients for psychological assessment. Table 5 details some of the incidents reported, including patients who had committed suicide or made suicide attempts (n = 4).
Details of incidents making respondents more likely to refer their orthognathic patients.
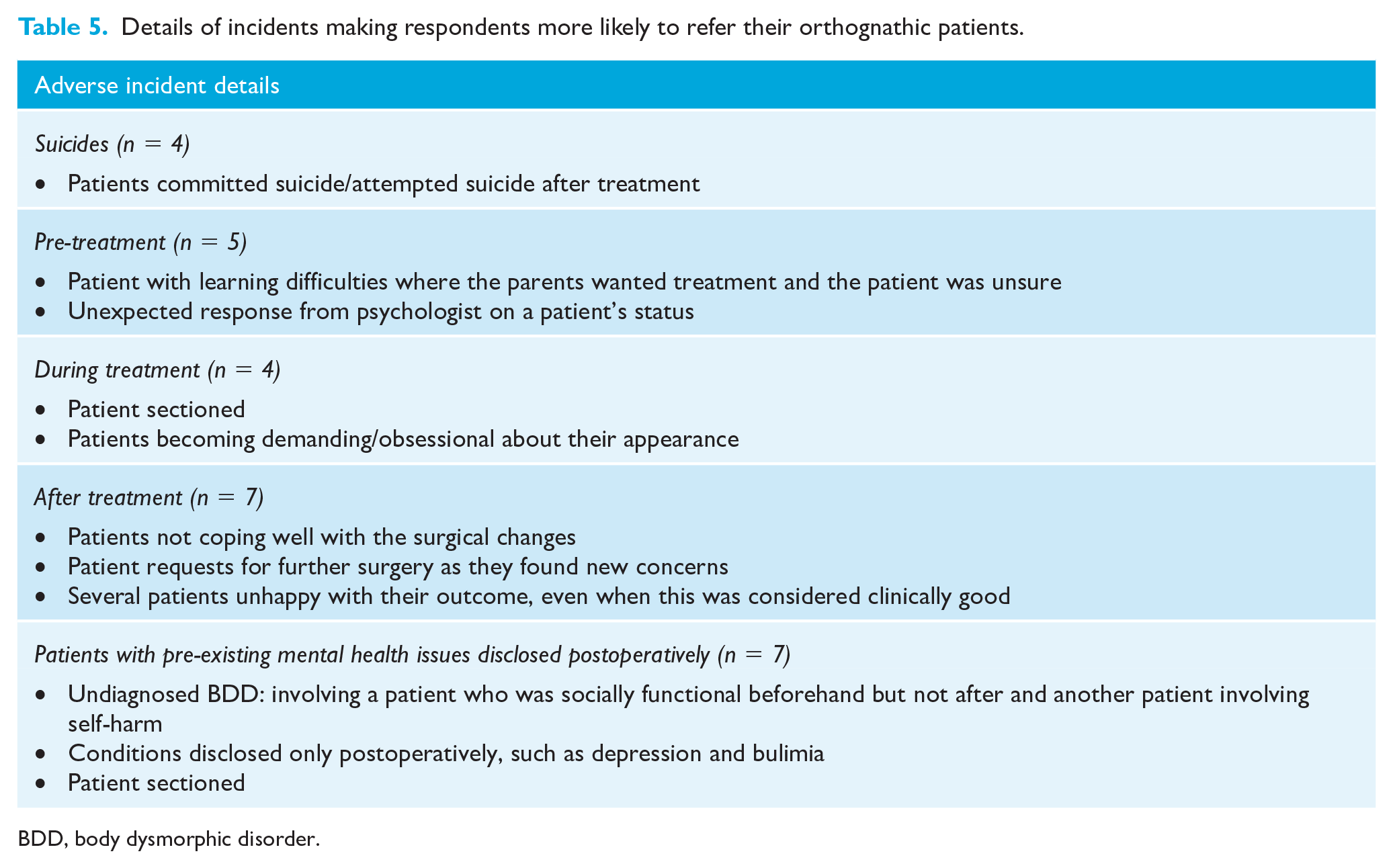
BDD, body dysmorphic disorder.
Discussion
A relatively low response of 29.1% was achieved, in comparison with the postal survey by Juggins et al. (2006) where an excellent response rate of 75% was achieved. The current response was also lower than some previous BOS online studies where responses in the range of 77%–86% have been cited (Bussell and Barreto, 2014; Stephens and Cook, 2002). There are many potential reasons for this lower than expected response, but it may well be that survey fatigue played a part as recent years have seen a rise in online questionnaires. The low response is clearly a limitation of the study, although useful conclusions can still be drawn from those who did respond. The selection of an online survey did however ensure questionnaire completion by setting mandatory responses, the ability to export survey responses directly to statistical software thus reducing the potential for error in data entry, and made the questionnaire as succinct as possible by applying logic systems.
This study focussed specifically on consultant orthodontists in order to allow comparison with the previous study by Juggins et al. (2006); however, it is acknowledged that the referral decision involves the whole orthognathic team, including maxillofacial surgeons who have had specific training in psychiatry and this may influence these clinical decisions. The perspective of other team members would be interesting to consider in future studies of this type.
Access to training has improved compared with that reported by Juggins et al. (2006) and exposure to postgraduate level training in this area has more than doubled (16.9% to 35.3%). However, there remains considerable demand for further training, with 90.2% of orthodontists in the present study perceiving a benefit from further training. Of those orthodontists who had undertaken previous training, there appeared to be a large variation in training format. It may be beneficial to consider a standardised teaching program for orthodontic trainees in the UK, particularly for those undertaking post-CCST training, and CPD courses for qualified orthodontists also appear to be valued. Respondents were also particularly interested in training in aspects such as undertaking an initial psychological assessment; this is in keeping with the NICE guidance (2006) which endorsed screening for BDD and recommended that three areas should be assessed during the initial consultation: (1) preoperative motivations and expectations; (2) physical appearance and body image; and (3) psychiatric status and history.
There appears to have been a definite positive shift in respondents’ opinions regarding the benefits of referral for psychological assessment. In the present study, all orthodontists believed that there were occasions where referral for psychological assessment was appropriate, compared with the previous study where 31.0% of respondents said they did not think that any of their orthognathic patients would benefit from psychological referral or were unsure of the proportion of patients who would benefit. It is likely that this positive shift in perceptions may be due to the increased discussion of this topic at conferences/meetings and more literature being available in the area, leading to increased awareness of mental health problems and the potential complications during treatment.
Orthognathic teams need pathways in place for onward referral of patients who require psychological services, but this is evidently not always readily available and the most common reason for units making no referrals was lack of/limited access to mental health support. Consequently, there may be unidentified concerns or mental health issues increasing the risk of patient dissatisfaction and harm. Clarke et al. (2005) described a model in which they evaluated the impact of a psychology service in a large plastic surgery unit in London. This model set out core requirements which patients must satisfy, together with the evidence on which this judgement was made. The introduction of this screening model resulted in substantially reduced numbers of patients proceeding to surgical waiting lists. The associated cost savings provided funding for a psychologist, which enabled psychological assessment to become part of routine care. Such innovative strategies are useful in circumstances with access issues and it may be beneficial to look into novel ways of providing better access to mental health support for orthognathic patients.
More than one-third of respondents reported sometimes changing treatment plans after referral for psychological assessment. Studies in cosmetic and plastic surgery suggest that if a higher number of patients were referred for psychological assessment, fewer patients may undergo surgical interventions (Clarke et al., 2013; Kellett et al., 2008). Psychological assessments should not be seen as a way of rationing treatment but instead to identify those who may require more support or a different form of treatment (Ryan et al., 2012).
The quality of psychological services and reports received mixed reviews. This information is subjective as many of the respondents may have very little with which to compare their experience of the service to which they refer. Many of the free text comments (Table 4) related to access and particularly the importance of a mental health professional having dentofacial expertise. In an effort to standardise procedures and maximise patient safety, UK commissioners of plastic surgery services established a special interest group for psychologists/psychiatrists working in this area which then provides ongoing training and peer support, a model that also works well in other aspects of clinical psychology (National Health Service Modernisation Agency, 2005). To ensure adequate support, a national programme could be established providing a special interest group of mental health professionals with dentofacial expertise.
Adverse incidents (Table 5) in the psychological domain were experienced by more than one-third of respondents in relation to their orthognathic patients. This is of real concern and emphasises the importance of comprehensive patient assessment and psychological referral where necessary; it also highlights the importance of support for teams working with orthognathic patients when faced with such complex issues
Conclusions and recommendations
The findings of this study suggest that:
Training experience: Has increased in the last 13 years; however, there is large variation and no clear standardisation.
Recommendation 1: In order to standardise training: a teaching programme for orthodontic trainees, especially at post-CCST level, and a CPD requirement for existing consultant orthodontists could be introduced.
Referrals: All respondents believed that at least some of their patients would benefit from referral. However, 31.3% of units referred no patients, mainly due to resource issues.
Recommendation 2: In order to reduce the inequality of mental health service access for orthognathic patients, innovative approaches need to be considered to enhance access. This could potentially involve mental health professionals being appointed to posts that cover several orthognathic units where there is currently limited access or the development of a national programme similar to the one developed in plastic surgery to ensure dentofacial expertise is available.
Adverse incidents: Of the respondents, 35.1% had patients who experienced incidents that prompted respondents to refer more orthognathic patients for psychological assessment.
Recommendation 3: Potential complications with orthognathic patients may be resolved through more training in this area and funding for mental health professionals; therefore, it is important that recommendations 1 and 2 are actioned.
Footnotes
Acknowledgements
The authors thank all of the consultant orthodontists around the United Kingdom and Republic of Ireland who gave up their time and opinions so willingly to complete this questionnaire and without whom this study would not have been possible; the British Orthodontic Society, especially Ann Wright, for distributing the questionnaire; and Dr Elinor Jones who kindly provided statistical advice.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.