
Abstract
Objective:
To measure patient-reported impact of orthodontic treatment in terms of pre-treatment concerns, treatment experience and treatment outcome.
Setting:
Four sites in Yorkshire, including two secondary care settings (Leeds Dental Institute and St Luke’s Hospital, Bradford) and two specialist orthodontic practices.
Design:
Cross-sectional survey.
Participants:
NHS orthodontic patients (aged 12+ years) who have completed comprehensive orthodontic treatment, excluding orthognathic surgery and craniofacial anomalies.
Methods:
Participants were opportunistically identified by the direct clinical care team during scheduled appointments and those eligible were invited to participate. Data were collected using the Orthodontic Patient Treatment Impact Questionnaire (OPTIQ), a validated 12-item measure with questions relating to pre-treatment experience, impact of treatment and outcome from treatment.
Results:
Completed questionnaires for analysis included 120 from primary care and 83 from secondary care. The most common pre-treatment concerns were alignment (89%) and being embarrassed to smile (63%). The most common expectations from orthodontic treatment were improved confidence to eat (87%) and smile (72%) in front of others, improved appearance of teeth (85%) and reduced teasing/bullying (63%). Only 67% respondents recalled receiving written information and the lowest recall related to retainer type and length of retention. The most commonly reported complications were sore mouth (68%), fixed appliance breakage (61%) and gingivitis (39%). Treatment caused greatest impact in relation to pain, limitations in eating and effect on speech. Overall satisfaction with orthodontic treatment was reported by 96% of respondents, 87% would have orthodontic treatment again (if needed) and 91% would recommend treatment to a friend.
Conclusions:
The OPTIQ is a useful patient-reported tool to identify pre-treatment concerns and expectations, treatment experience and outcome. Orthodontic treatment leads to high levels of satisfaction.
Keywords
Background
Untreated malocclusion has been shown to cause negative psychological, social and physical impacts that can lead to a reduction in oral health-related quality of life (Zhang et al., 2006). Orthodontic treatment aims to improve the appearance and function of teeth, improve psychosocial wellbeing and reduce the risk of future problems that may arise from malocclusion, such as tooth wear, gingival problems and pathology associated with impacted teeth (Linklater and Fox, 2002). Orthodontic treatment accounts for approximately one-tenth of the NHS dental primary care budget in England, which was £3.4 billion in 2015–2016 (NHS England, 2015), yet still the demand for orthodontic treatment exceeds provision. The 2013 Child Dental Health Survey found 9% of 12-year-olds and 18% of 15-year-olds were undergoing orthodontic treatment, but a further 37% and 20% of 12- and 15-year-olds, respectively, were judged to be in need of orthodontic treatment (Steele et al., 2015).
Patient-reported experience measures (PREMs) and patient-reported outcome measures (PROMs) are important for assessing quality of care (Coulter, 2017). PROMs contribute to the evaluation of the effectiveness and safety of care from a patient perspective, while PREMs provide information about the actual process of receiving care (Kingsley and Patel, 2017). Currently, orthodontic-specific PREMs and PROMs are not used routinely in clinical care; however, the inclusion of patient-reported measures in orthodontic research is increasing; these include pain during treatment, expectations of treatment and quality of life items (impact of malocclusion, acceptability of treatment, anxiety and occlusion) (Tsichlaki and O’Brien, 2014).
Patient satisfaction is one of the most commonly measured patient-reported outcomes in both research and audit. One orthodontic-specific tool developed to measure parental satisfaction with orthodontic treatment for young people includes both process and outcome (Bennett et al., 2001). A systematic review of 18 studies examining satisfaction with orthodontic treatment found an associated between satisfaction and perceived aesthetic outcomes, psychological benefits and quality of care, while dissatisfaction was associated with treatment duration, pain levels and discomfort, and the use of retention appliances (Pachêco-Pereira et al., 2015). The review highlighted that study design, setting, population and measurement tools used across the studies were highly variable. A qualitative study found adults’ satisfaction with orthodontic treatment was related to communication, staff, the physical environment, appointments and the impact of the appliance treatment (Wong et al., 2018). Although satisfaction is a popular measure, it may have a limited ability to discriminate between different aspects of care and a ‘ceiling’ effect that can mask negative experiences within the care process (Hodson et al., 2013). In this study, an orthodontic-specific patient-reported tool was used to examine pre-treatment concerns, treatment experience and treatment outcome, with the ambition of identifying areas for service improvement.
Aim
The aim of the present study was to measure patient-reported impact of NHS orthodontic treatment in primary and secondary care settings. Impact was measured in terms of pre-treatment concerns, treatment experience and treatment outcome.
Design
A cross-sectional descriptive survey using a validated questionnaire with post-treatment orthodontic patients in primary and secondary care.
Setting
Respondents were recruited from four NHS sites in Yorkshire, including two secondary care settings (Leeds Dental Institute and St Luke’s Hospital, Bradford) and two specialist orthodontic practices. These sites cover a diverse urban and rural population and were selected to provide a varied ‘real-world’ sample. Staff providing orthodontic treatment at these sites included Consultant Orthodontists, Specialist Orthodontists, Specialty Trainees in Orthodontics and Orthodontic Therapists.
Population
The study population included orthodontic patients aged 12 years and older who had completed NHS orthodontic treatment and were in orthodontic retention. Respondents were required to be able to read English and participants were allowed to complete the questionnaire with parental help if preferred. Orthognathic patients and those with cleft lip and/or palate and craniofacial anomalies were excluded because the measurement tool was not developed for these types of patients and so it may not be able to accurately capture their specific treatment experience.
Materials and methods
Ethical approval was granted by the Yorkshire and Humber Research Ethics Committee on 26 April 2018 and from the Health Research Authority on 30 April 2018 (18/YH/0161). Local approval was granted by each participating site.
Participants were opportunistically identified by the direct clinical care team during scheduled appointments. All patients who attended for a retainer review appointment were screened against the eligibility criteria; those who were found to be appropriate were invited to participate. Verbal and written information about the research was provided at the start of the appointment. Those who agreed to participate were given a questionnaire at the end of their appointment to complete in the waiting room and return to a sealed box at the reception desk.
Data were collected using the Orthodontic Patient Treatment Impact Questionnaire (OPTIQ), developed over the last five years as part of the research component of professional training at the University of Leeds (Fletcher, 2015; O’Morain, 2013). The OPTIQ contains 12 questions in three sections relating to pre-treatment experience, impact of treatment and outcome from treatment (Supplemental Table 1). Development of the OPTIQ involved focus groups with 12 pre-orthodontic treatment patients (eight aged < 16 years and four aged ⩾ 16 years) and 12 post-orthodontic treatment patients (seven aged < 16 years and five aged ⩾ 16 years) to develop a preliminary questionnaire, which was then piloted with 10 post-treatment orthodontic patients of all ages (O’Morain, 2013). The final questionnaire has been psychometrically tested and validated for the target population of this study on 142 treated patients (Fletcher, 2015). This included:
Criterion validity: correlation between the OPTIQ and a global patient satisfaction Visual Analogue Scale (statistically significant correlation);
Convergent validity: correlation between the OPTIQ and three validated questionnaires measuring related constructs (statistically significant correlation);
Discriminant validity: correlation between the OPTIQ and 14 patient variables (no statistically significant correlations);
Test–retest reliability: correlation between the OPTIQ completed at three months and four months after treatment (excellent agreement);
Internal reliability: tested with Cronbach’s alpha (acceptable);
Responsiveness: correlation between a pre-treatment group and the post-treatment group (statistically significant correlation).
A copy of the version of the OPTIQ used in this study is available from the research team on request.
The Ethics Committee advised consent was implied by completion of the questionnaire; participants were advised to leave the questionnaire blank if they did not want to participate. Instructions for survey completion were given at the start. Basic demographic information was collected at the end of the survey (gender, age, ethnicity, first language, level of education, location of treatment and source of referral). No personal data were collected. Due to the number of sites and clinicians involved in recruitment, it was not possible to accurately record the number of patients who were approached to participate.
Questionnaires were collected at the end of each week and returned to one researcher (EB) for collation. Questionnaires were assigned a study identification number and responses were transferred into Microsoft Excel 2011 v14.7.7. Data were reported descriptively in terms of respondent demographics and patient-reported pre-treatment concerns, recall of information provision, treatment experience and outcome from treatment. At the time of the study there was no validated system for converting ratings given by respondents into a meaningful score, so responses are reported descriptively as categorical data. The effect of age groups (12–15 years, 16–17 years, 18+ years) and care setting (primary or secondary) on pre-treatment concerns, treatment experience and outcome were examined for similarity in trends.
Results
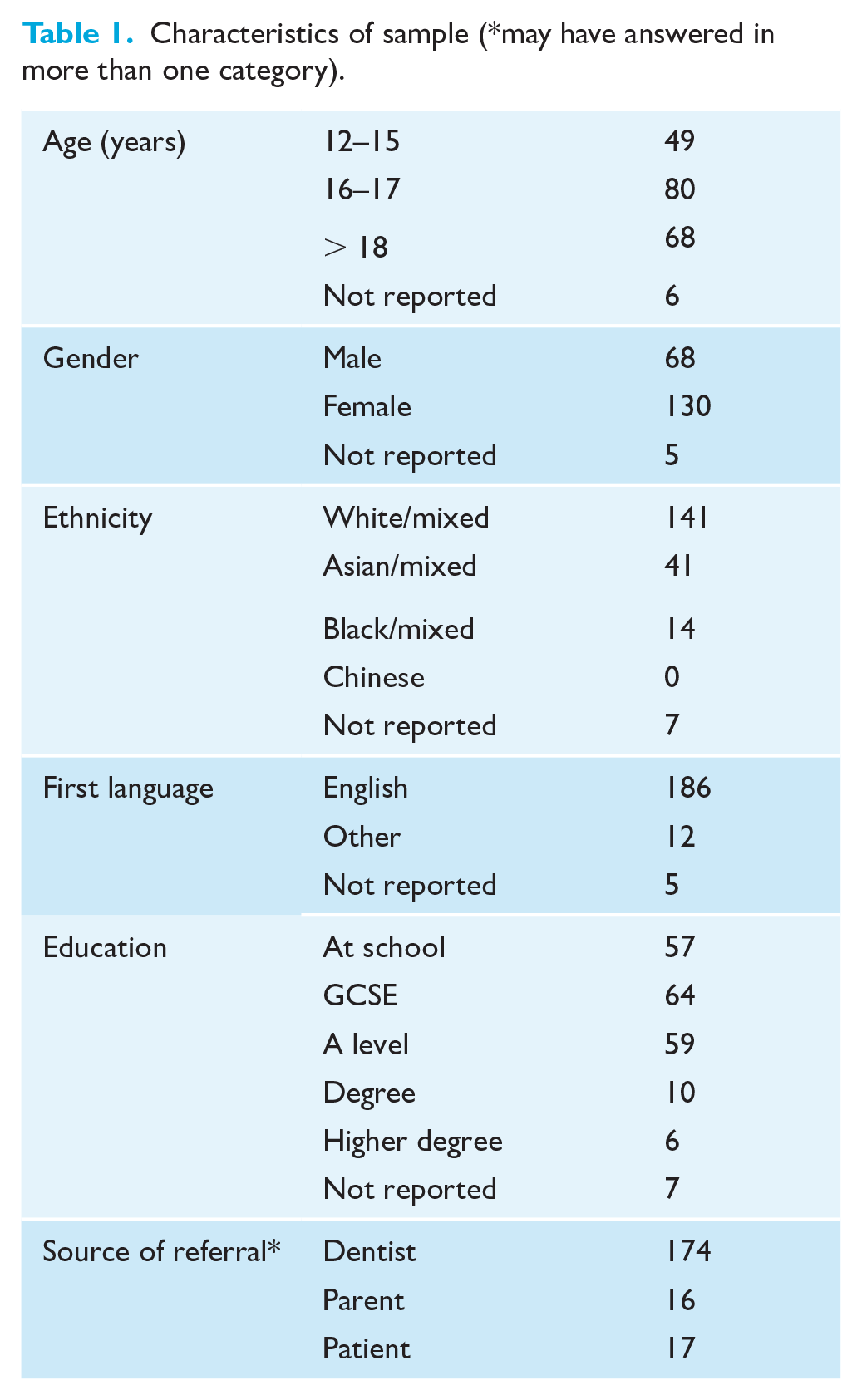
Data were collected between July 2018 and January 2019. In total, 215 questionnaires were returned, of which 203 were complete and included in the final analysis. The characteristics of the sample are given in Table 1. The respondents included 120 from primary care and 83 from secondary care. No differences in characteristics were found between the respondents from different care settings.
Characteristics of sample (*may have answered in more than one category).
Pre-treatment concerns and expectations
The frequency of self-reported pre-treatment concerns are summarised in Figure 1. The most commonly reported pre-treatment concerns were alignment of the teeth (41% ‘a lot’ and 48% ‘a bit’) and being embarrassed to smile (34% ‘a lot’ and 29% ‘a bit’), followed by overjet (22% ‘a lot’ and 27% ‘a bit’) and being sad or unhappy with teeth (22% ‘a lot’ and 34% ‘a little’). The least reported concerns related to functional issues (speech, sleeping and eating), dental health, ability to clean and missing teeth. One respondent reported no pre-treatment concerns. Similar trends were seen in patient-reported pre-treatment concerns across age groups and care setting (Supplemental Figure 1). A higher proportion of patients in primary care reported overlapped and ectopic teeth.
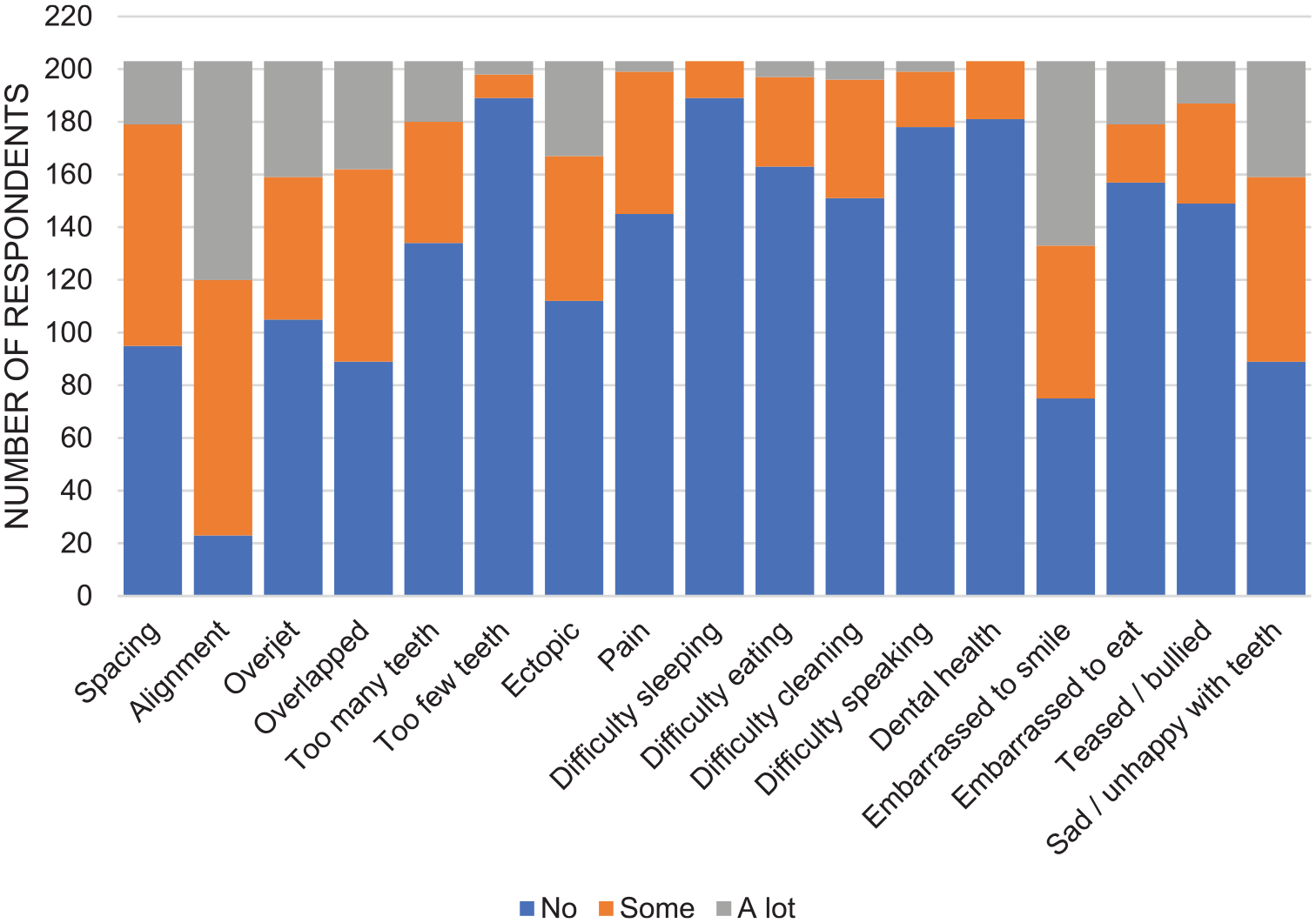
Patient-reported pre-treatment concerns.
The most common expectations from orthodontic treatment were improved confidence to eat (87%) and smile in front of others (72%), improved appearance of the teeth (85%) and reduced teasing or bullying (63%). Over half (57%) of respondents thought treatment would make brushing easier. Similar trends were seen across age groups and care setting (Supplemental Figure 2). Additional comments made by some respondents about their pre-treatment problems and motivation for treatment are given in Supplemental Table 2.
Recall of pre-treatment information
Patient-reported recall of pre-treatment information provision is shown in Figure 2. Nearly all respondents remembered receiving verbal information while only 67% recalled any written information. Greatest recall of pre-treatment information related to oral hygiene and diet advice. Retention was the area with lowest recall; 71% of respondents recalled being told about retainer type and 80% about the length of retention. Generally, adults had higher recall of being given information and leaflets were more commonly given in secondary care (Supplemental Figure 2). A higher proportion of patients from primary care recalled being told the length of treatment but fewer recalled discussing retainer type.
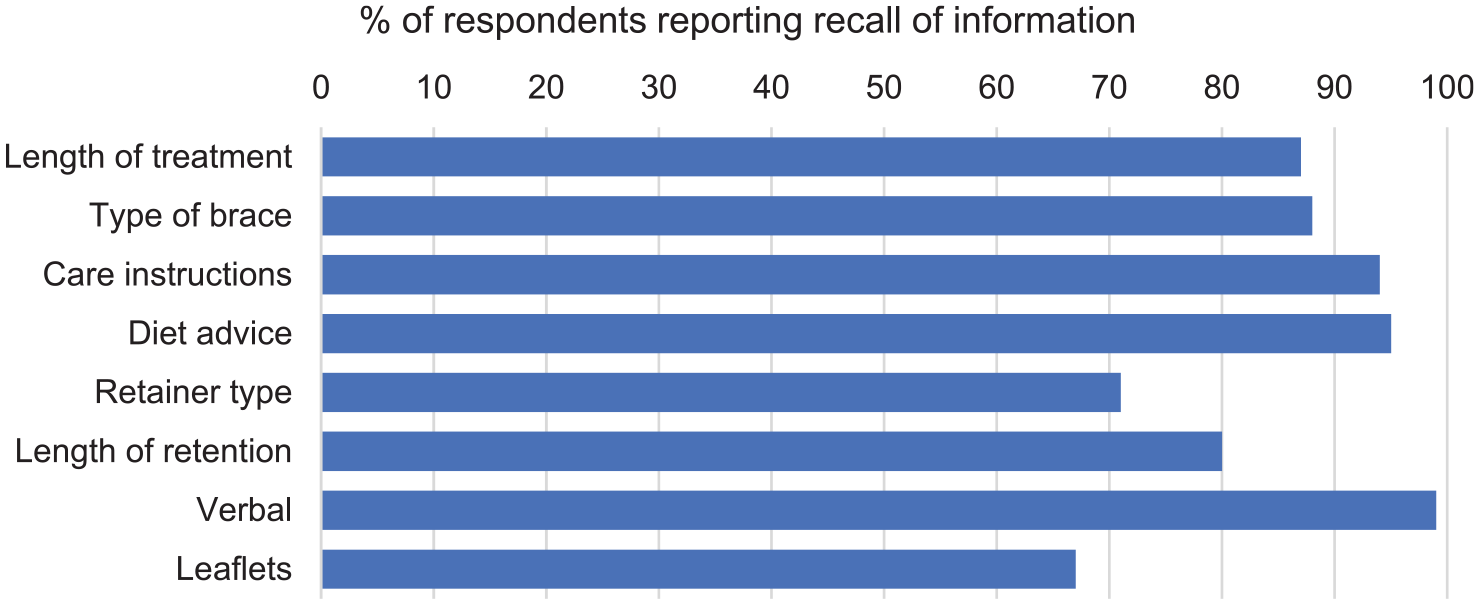
Patient-reported recall and source of information.
Treatment experience
Questions relating to the comfort of procedures identified that extractions were the least comfortable, followed by adjustments to the appliance and impressions. Appliance removal and retainer fit were the most comfortable procedures (Figure 3). Examination of differences between age groups suggested adults found extractions more uncomfortable than young but wearing removable and fixed appliances less uncomfortable compared to young people, while children (< 16 years) found removable appliances and headgear more uncomfortable than older adolescents and adults (Supplemental Figure 4). There were apparent differences in discomfort ratings between care settings, with a lower proportion of secondary care respondents generally rating procedures as uncomfortable.
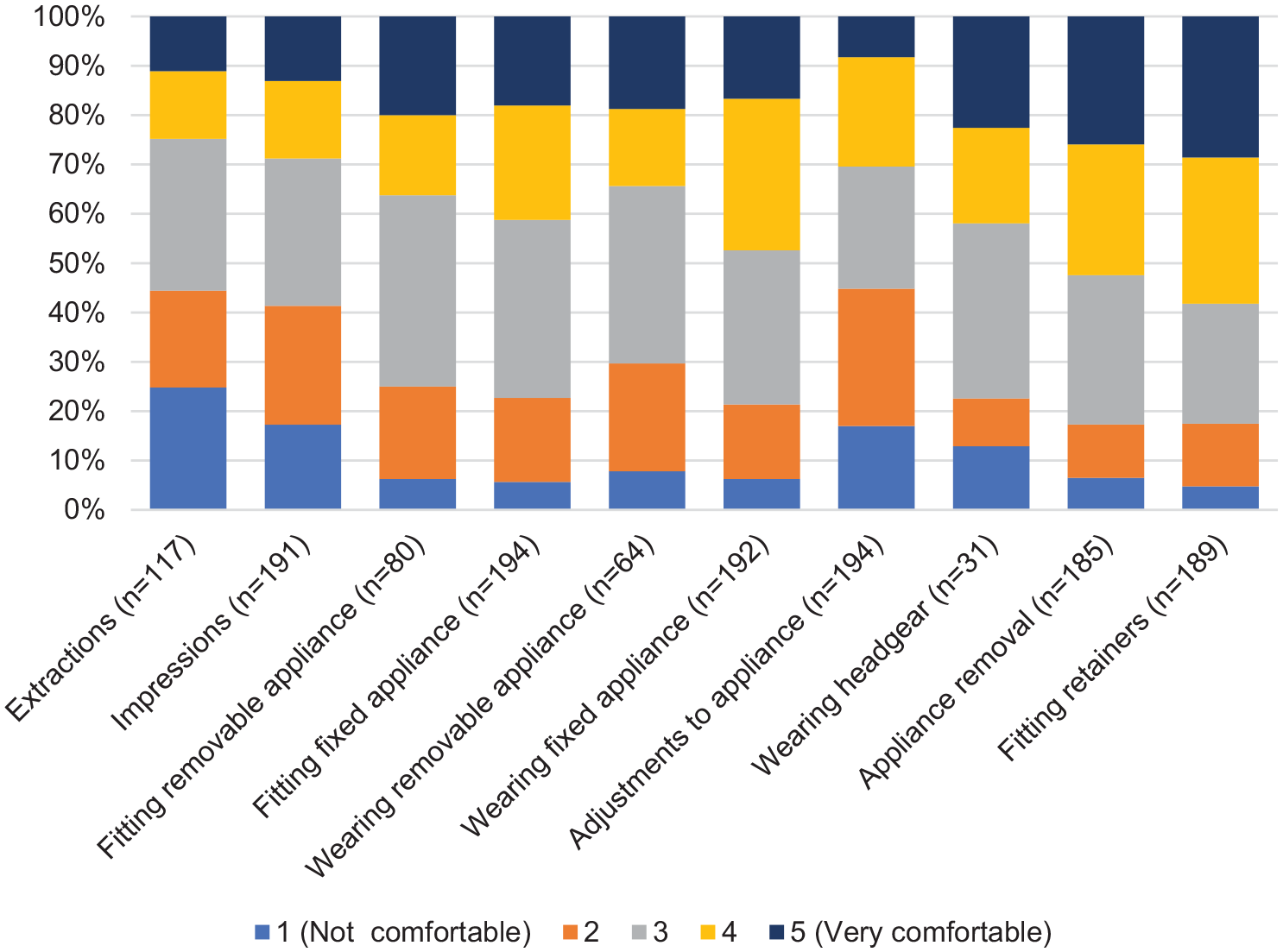
Patient-reported level of comfort of orthodontic procedures.
The most commonly reported complications related to orthodontic treatment were sore mouth (68%), fixed appliance breakage (61%) and gingivitis (39%). Impressions were repeated at the start and end of treatment for 17% and 14% of respondents, respectively. Retainer breakage was reported by 17% of respondents. Trends in complications between age groups and care settings were generally similar (Supplemental Figure 5).
The impact during treatment on respondents’ daily life is summarised in Figure 4. Treatment caused greatest impact in relation to pain, limitations in eating and effect on speech. Least impact was seen in relation to dental health, being teased or bullied, psychosocial wellbeing domains and time off school. Difference in trends were observed by age group, with children reporting greater relative impact on speech, while older adolescents reported greater impact on pain and sleeping. Adults reported more impact on time off work or school than other groups (Supplemental Figure 5a).
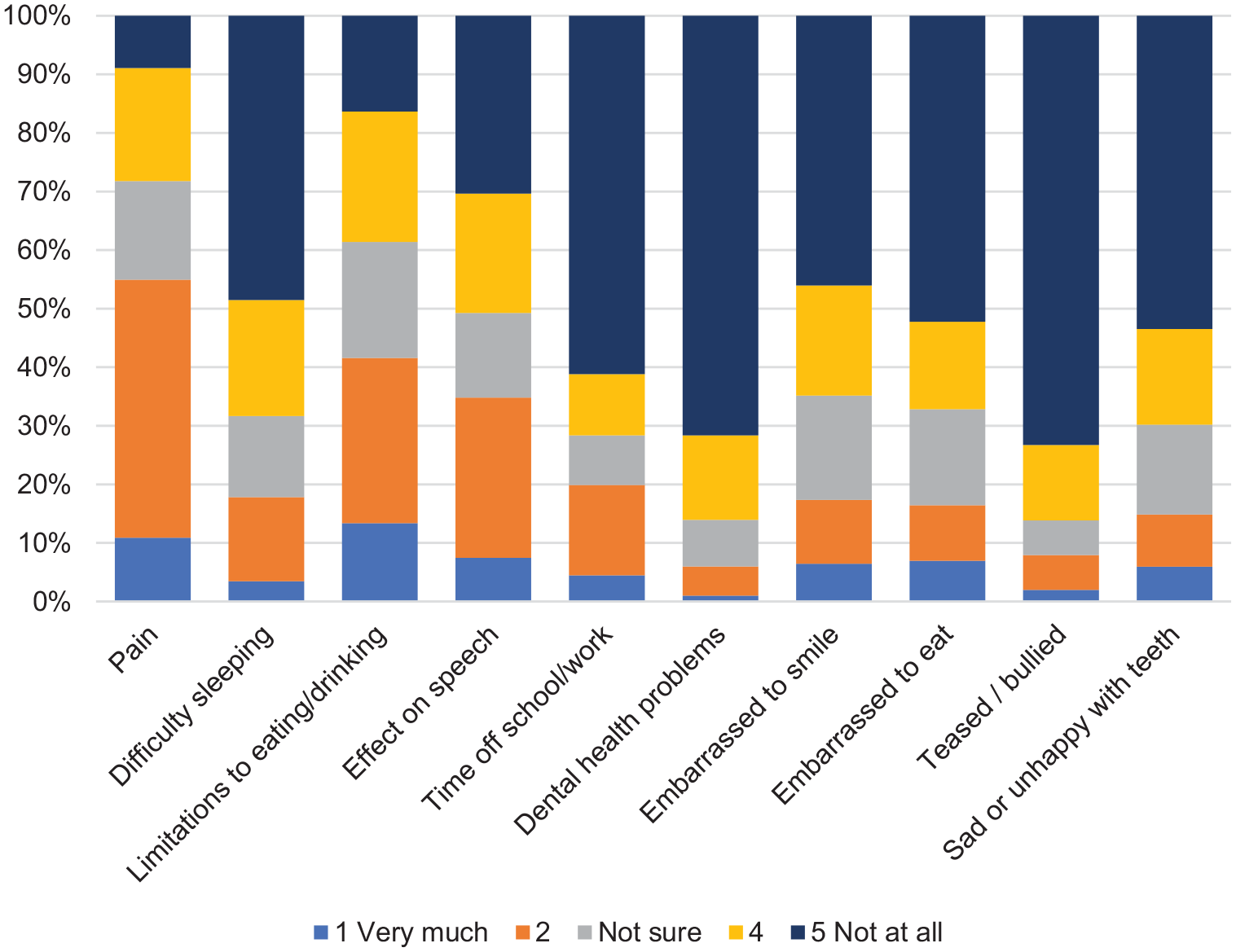
Impact of receiving orthodontic treatment on daily life.
Comments about orthodontic treatment and respondents’ experience of orthodontic services are given in Supplemental Table 2. Comments are largely positive, but some respondents highlighted the length and burden of treatment, discomfort and challenges in communication with the clinician.
Treatment outcome
Change in pre-treatment concerns following orthodontic treatment is given in Figure 5. Some respondents rated specific features of malocclusion ‘much better’, even if they had not reported pre-treatment concerns related to this feature. Dental appearance, embarrassment when smiling, confidence and happiness with teeth were reported to be much improved. The proportion of respondents suggesting ‘no change’ in pain, eating and cleaning was approximately equal to the proportion reporting improvement. Importantly, seven respondents reported worse pain at the end of treatment, and between one or two respondents reported worsening in each of the other categories. Similar trends in patient-reported outcomes were seen across the age groups and care settings, although older adolescents (16–17 years) were generally the most positive about post-treatment improvements (Supplemental Figure 7).
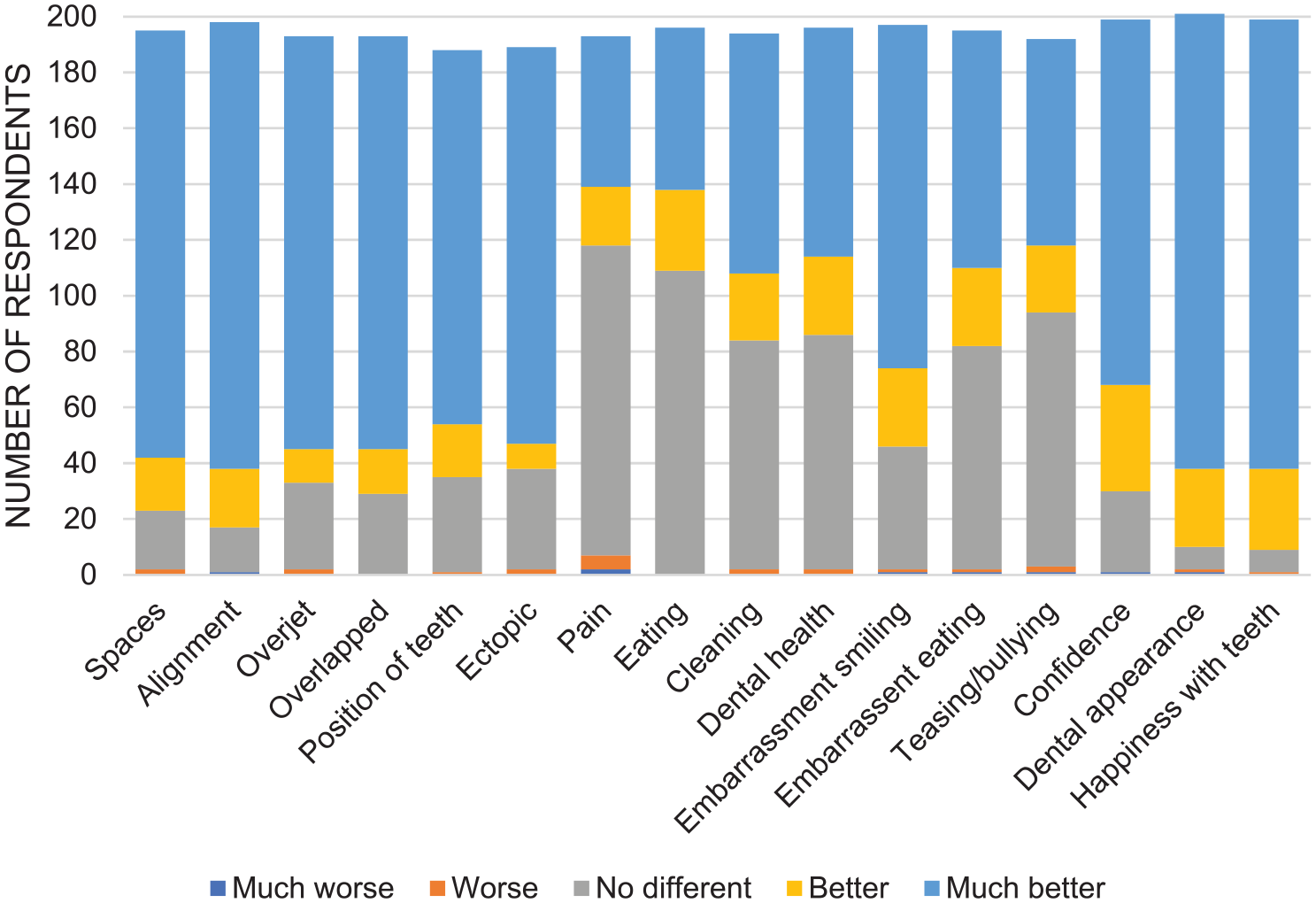
Patient-reported change in pre-treatment concerns.
Overall satisfaction with orthodontic treatment was reported by 96% of respondents, while 91% and 83% reported that family and friends respectively had commented on how well orthodontic treatment had worked; 87% would have orthodontic treatment again if needed and 91% would recommend treatment to a friend. The low number reporting dissatisfaction prevented any subgroup analysis.
Comments about treatment outcome and respondent comments to other people about their experience of orthodontic treatment are given in Supplemental Table 2. Generally respondents reported that despite challenges of treatment, they felt the outcome was worthwhile and they would recommend treatment to others.
Discussion
Specific features of malocclusion, such as alignment of the teeth and overjet, were identified as causing concerns in this study, alongside general quality of life impacts from malocclusion. This reflects previous research about the impact of malocclusion on oral health-related quality of life (Dimberg et al., 2014; Fabian et al., 2018; Johal et al., 2007; Lui et al., 2009). The higher proportion of patients in primary care reporting ectopic teeth than secondary care is somewhat surprising, as often these patients require surgical intervention provided by a multidisciplinary hospital team; however, discussion among the research team identified that this finding can be attributed to good local delivery of primary care orthodontics, by clinicians trained to consultant level, where level 3a and 3b complexity cases are being treated despite initial surgical intervention being provided by a hospital team. This highlights that the setting and sample included in this study may not be reflective of all NHS primary care orthodontics; while the gender distribution reflects reported demand for orthodontic treatment in the UK and the ethnic mix is reflective of this particular population, the sample included a high proportion of adults and possibly cases that may be referred to secondary care in other areas of the UK.
The most common expectations from orthodontic treatment were improved appearance, confidence to eat and smile in front of others, and reduced teasing or bullying. This supports previous research showing the main motivation for treatment is appearance and the associated psychosocial benefits (Pabari et al., 2014; Wędrychowska-Szulc and Syryńska, 2010). The perception by over half the respondents that treatment would make brushing easier is interesting, as although the relationship between malocclusion and oral health is complex (van Gastel et al., 2007), there is some evidence that orthodontics improves oral hygiene motivation (Feliu et al., 1982).
Effective pre-treatment information provision to improve recall is a challenging area with growing interest in more innovative and engaging methods (Ahn et al., 2019). The relatively poor recall of information about retention is important, as retention is fundamental to long-term success of treatment and adherence is a recognised issue (Aljabaa et al. 2014). Future work is warranted to test whether more innovative information provision methods specifically focussed on retention increase recall, and if this informed decision-making subsequently impacts on improved adherence.
The findings around patient experience of undergoing orthodontic treatment are perhaps the most interesting and the free text comments, in particular, highlighted areas where patients found orthodontic treatment challenging. While previous research has looked at the impact of orthodontic treatment on quality of life (da Silva et al., 2019) and behaviour (Al Jawad et al., 2012), to the authors’ knowledge there are not any orthodontic-specific PREMs routinely in use to monitor experience. It might not be possible be reduce the impact of orthodontic treatment; however, more effective pre-treatment information and support throughout treatment may promote better patient preparation for treatment and reduce worry during treatment. This is supported by another study of satisfaction with orthodontic treatment that reported pain and discomfort during treatment strongly affected treatment satisfaction (Feldmann, 2014).
Despite many patients reporting negative impacts during treatment, the study demonstrates overwhelmingly positive patient-reported outcomes. This reflects previous studies, which also found high levels of satisfaction (Pachêco-Pereira et al., 2015). Most comments suggested the challenges of undergoing orthodontic treatment were justified by the result and 96% of respondents were satisfied. This high level of satisfaction and the reported change in pre-treatment concerns supports the continuation of orthodontics in the NHS. However, it is also important to recognise that for a minority of patients, a worsening of malocclusion features or quality of life was reported. While it is outside the scope of the OPTIQ to identify the aetiology of these individual effects, it might be that a tool such as the OPTIQ could be used in routine care to identify and manage those with sub-optimal outcomes.
This study is the first to use the OPTIQ as a patient-reported measure of orthodontic treatment in routine NHS orthodontic care. The tool successfully delivered valuable information about pre-treatment concerns, experience of treatment and outcomes. This information is essential for demonstrating the value of orthodontics and for identifying areas for improved communication with patients and delivery of clinical care. While the OPTIQ was developed with NHS patients and this study was conducted in England, the domains covered in the OPTIQ and information it delivers is likely to be useful in other countries. The main limitations of the study were potential bias in sample and the application of the tool to collect all data at the end of treatment. As often happens with multicentre research involving numerous clinicians, there was variable engagement in recruiting patients so although almost all those who were invited to participate did, there may have been bias in those invited to participate. Collecting all data at the end of treatment may lead to some recall bias; in the future, it may be preferable to collect pre-treatment concerns at the start of treatment. The results of the analysis do suggest some additional modification and testing of the OPTIQ may be beneficial before its wider implementation. For example, a number of people indicated improvement in features of malocclusion that were not reported as a pre-treatment problem, so including an option of ‘I did not have this problem’ may give more accurate information about post-treatment changes. Finally, some patients were unclear about whether ‘overlapped’ referred to a deep bite or crossed teeth, so for the reporting the term ‘overlapping’ has been used. The OPTIQ authors plan to provide a glossary of terms to reduce ambiguity in the future.
Conclusions
The OPTIQ is a useful patient-reported tool to identify pre-treatment concerns and expectations, treatment experience and outcome. The impact of orthodontics on patients may be underestimated currently by services. Although outcomes are favourable and satisfaction is high, using patient experience data in pre-treatment patient information could improve patient reasoning and preparation for treatment. Integrating a patient-reported measure into quality assessment of treatment provides useful data about the overall value of treatment and can be used to identify the cost-effectiveness of orthodontic care to individual wellbeing and the NHS.
Supplemental Material
Supplemental material for Patient-reported experience and outcomes from orthodontic treatment
Supplemental material, Supplemental_material for Patient-reported experience and outcomes from orthodontic treatment by Elizabeth Bradley, Andrew Shelton, Trevor Hodge, David Morris, Hilary Bekker, Steven Fletcher and Sophy Barber in Journal of Orthodontics
Footnotes
Acknowledgements
The authors thank all the survey respondents and the clinicians involved in data collection.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
The OPTIQ is currently undergoing minor revision and it is hoped the questionnaire will soon be freely available through the British Orthodontic Society website. If you would like a copy of the OPTIQ please contact David Morris (
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.