
Abstract
Indonesia, like many rapidly ageing lower-middle-income countries (LMICs), tends to portray older citizens as ‘vulnerable’ and ‘dependent’; yet the country has few public policies to support them. To this discourse, an alternative stereotype is emerging, influenced by notions of ‘successful ageing’, which promotes models of older people as healthy and contributing to families and the nation state. In this article, we argue that both stereotypes ignore the varied and context-specific conditions of later life. Importantly, the dominant representations ignore the frailty and dependence that many people in LMICs experience towards the end of their lives. This results in dependence and frailty being concealed from view and treated as a purely familial responsibility, which households living in economic, social and demographic precarity can ill afford. ‘Familism by default’ spells invisible, unsupported and unsustainable care for many older Indonesians. This article draws on ethnographic fieldwork between 2018 and 2022 from two research projects on ageing, livelihoods, vulnerability and care in disparate communities across Indonesia. By juxtaposing dominant representations with the social, economic and health realities in which lives are lived, we trace the implications for policies, values and practices around care in later life.
I. Introduction
Indonesia, a rapidly ageing lower-middle-income country (LMIC), has relatively few policies dedicated to older citizens. The dearth of public provision is at odds with dominant stereotypes of older people as ‘vulnerable’ and ‘dependent’, which were amplified during COVID-19. An emerging alternative stereotype, shaped by Western discourses of successful ageing, casts older people as ‘heroic’, ‘active’ and ‘productive’ contributors to their families, communities and wider society (Lamb, 2017). Both stereotypes deny the heterogeneous, dynamic and context-specific nature of later life and have negative effects on public and private responses to older people.
This article critically examines dominant representations of older people in the media, policies and everyday practices and juxtaposes these with ethnographic evidence on some of the social, economic and health realities in which older people’s lives are lived. The central argument is that representations (and their absence) matter for shaping policies, values and practices around material support and physical care in later life. They have implications for the allocation of resources and delivery of services, for the inclusion of older people in the labour market and for intergenerational relations. We are particularly concerned here with the impact on the quality and sustainability of physical care and access to healthcare for older care-dependent Indonesians.
In this article, we argue that the ageist model of older people as weak and domesticated best reflects middle-class notions of ‘deserved dependence’ on inter-generational familial reciprocity or civil servant pensions, rather than the common reality of dependence structured by age discrimination and the early onset of poor health. The contrasting ‘heroic’ stereotype drives state, NGO and community- based interventions aimed at older people’s economic participation, exercise regimes, health promotion and volunteer engagement. While valuable, the top-down promotion of ‘active ageing’ can be patronising to the millions of older Indonesians who have long had to be active to survive. It renders improvement and independence a citizen duty and can feed the stigma of physical dependence and cognitive infirmity. Both representations ignore the profound frailty and dependence that many people in less economically developed countries (LEDCs) experience at the end of their lives. This reality is hidden from view. We argue that the invisibilization of care-dependent older people matters. It permits the prioritization of preventive health measures over rehabilitative, palliative care and long-term care (LTC) provision (Lloyd-Sherlock et al., 2019). The latter is delegated to the domestic, family space, rather than presenting an existential human experience requiring collective engagement (Razavi, 2011). As our data show, for poor or small households, this failure often means inadequate care, unsustainable burdens or premature death.
We start our analysis by documenting the widespread assumption of vulnerability and dependence in later life and clarify the extent to which this captures lived experiences in Indonesia. We then examine the active ageing narrative and its reflection in policies and programmes for older people on the one hand, and different subgroups’ challenges in living up to this narrative on the other hand. We complete our analysis by highlighting significant realities that are rendered invisible by the dominant representations, namely frailty, dependence and precarious care.
II. Literature Review
Our review focuses on how older people have been represented in the ageing and development literature on the Global South. Scholarly and policy attention to older people in LEDCs is relatively new. For decades, Cowgill and Holmes’ (1974, 1972) Ageing and Modernization thesis dominated the debate. They took as axiomatic that older people are dependent on adult children and kin networks for material and practical support and physical care, but that this dependence only becomes problematic because declining fertility, migration and ideational changes undermine families’ willingness to provide for older members. In the absence of much empirical evidence on older people’s situation before and during ‘modernization’, Cowgill and Holmes—and countless authors subsequently—deduced older people’s imperilment from macro-level trends, such as urbanization, female labour force participation or education (Chen and Jones, 1989; Higo and Khan, 2015; Jones, 1988; Martin, 1988; Westley and Mason, 2002). This macroeconomic argument of ageing as a problem, because older people are a net ‘burden’, is reflected in the opening statements of virtually every report on ageing in LEDCs, which decry rising dependency ratios, declining fertility, increasing migration and the observation that country X is ‘growing old before growing rich’ (Johnston, 2021; Runde, 2020; Ziegenhain, 2021). 1
The narratives of older people as victims of development—caught up in demographic, social and economic changes that undermine familial support—and impediments to development (due to their dependence and supposed resistance to change) are reflected in an influential article by economists Treas and Logue (1986), written in the wake of the 1982 World Assembly on Aging. Older people in LEDCs were conceptualized as a source of development concern—a potential brake on economic growth—and humanitarian concern due to their status as a vulnerable subgroup. Treas and Logue’s early article is significant because it introduces an alternative representation—the possibility of older people being a ‘resource’ for development—which was to shape representations and policies during the 1990s and 2000s.
The view of older people as a ‘resource’ or ‘asset’ is arguably the dominant alternative representation to that of ‘dependence’ and ‘vulnerability’ in old age in LEDCs (cf. Arifin and Ananta, 2009; Bastia et al., 2022; Mehta, 2005). Its dominance owes to empirical, instrumentalist and ideological arguments. As research on older people in LEDCs has expanded, so has the recognition of their economic and social contributions (Bastia, 2009; Pang et al., 2004; Schröder-Butterfill, 2004; Vera-Sanso, 2012). Older people’s productive potential has further been instrumentalized by neoliberally informed policymakers keen on extending working lives, harnessing unpaid care and volunteer labour, and individualizing risk in later life (Gratton and Scott, 2020; International Labour Organization, 2019) and by advocacy groups arguing that investing in older people pays off. For example, the WHO’s (2020: 5) Decade of Healthy Ageing Action Plan argues that the ‘cost of caring for older populations’ can be offset by older people’s ‘economic and social benefits’ from work, taxes, volunteering, and other contributions. Yet the greatest impetus to the view of older people as a resource has come from the ‘successful ageing’ movement that emerged in the 1990s as a powerful counter-narrative to ageing as a period of decline, dependence or disengagement (Baltes and Baltes, 1990; Rowe and Kahn, 1997). Various and nuanced versions of the successful ageing paradigm exist (cf. active ageing and healthy ageing) (Beard et al., 2016; World Health Organization, 2002; Zaidi and Howse, 2017); it is impossible to review these here. Broadly, the paradigm emphasizes that high levels of later-life physical, economic, social and psychological functioning are attainable given individual efforts over the life course (e.g., exercise, diet, mental stimulation and social participation).
The contributions of successful ageing to challenging the view of old age as a period of inevitable decline and dependency and creating a positive representation of later life are undeniable. However, the paradigm has also been criticized for stigmatizing older people who fail to age ‘successfully’, for ignoring the social, economic and political inequalities that make attainment of functioning difficult and for ethnocentrically equating success with independence (Lamb, 2017; Rubinstein and de Medeiros, 2015).
To conclude, the literature typically provides two dominant stereotypes of older people as either ‘successful’ or ‘vulnerable’. In Western writing, this distinction has tended to map onto the ‘third age/fourth age’ divide (Laslett, 1996), with the former associated with activity, health, contributions and agency, the latter associated with ‘deeply embodied’ states of frailty, dependence decline and death, concentrated within a ‘narrower chronological age range’ and a ‘more marginalized social space’ (Gilleard and Higgs, 2011: 140). In the literature on ageing in LEDCs, there has been less focus on health and care dependence, and vulnerability is chiefly glossed as economic and social dependence. Having theorized vulnerabilities in later life in previous writing (Schröder-Butterfill and Marianti, 2006), Schröder-Butterfill distinguishes the use of vulnerability as a generalized shorthand for disadvantage—as found in the discourses examined here—from an analytical approach that differentiates subgroups at risk from specific forms of harm and social constructions of vulnerability over the life course (cf. Lloyd-Sherlock and Locke, 2008). For the present argument, the respective contents of the binary representations are a subordinate concern. More importantly, we seek to expose the implications of reducing later life to two monolithic representations that marginalize alternative realities and silence public response to them. As Lloyd-Sherlock has put it, ‘Generalizing about what it means to be old, either from a positive or negative perspective, leads to generalizations about the consequences of population ageing, and to generalized policy responses’ (2010: 384). Aside from mounting a critique of homogenising stereotypes, we aim to contribute to empirically grounded literature on the diversity of later life. Such an approach has recently been exemplified for a Western context by Enßle and Helbrecht (2021) juxtaposing binary public discourses and heterogeneous lived experiences of ageing in Berlin. This article attempts this for Indonesia by challenging binary representations, highlighting the elision of profound dependency that can arise from this and tracing the implications for the reliability and quality of care.
III. Methodology
This article draws on data and insights from two research projects in Indonesia. The first, Understanding Social, Economic and Health Vulnerabilities Across the Lifecourse in Indonesia (2016–2021), examines threats to well-being and livelihoods for people at different life-course stages (youth, family formation, middle age and old age) and the support available from family networks and government programmes. The second, Care Networks in Later Life (2019–2023), focuses on older people with manifest care needs and examines how their care is negotiated within family and community networks, and the nature of their access to health services and support from governmental or non-governmental sources. Both projects share a common methodology involving ethnographic fieldwork in six and five study communities, respectively, with three sites common to both projects. The sites focused on for this article include a matrilineal, Muslim highland village with extreme labour outmigration; a crowded, poor, multi-ethnic neighbourhood of Jakarta; rural and peri-urban Javanese sites in Yogyakarta and East Java with bilateral kinship systems and mixed economies; and a patrilineal, Christian fishing and farming community on the eastern Indonesian island of Alor. In the sites on Java, the availability of healthcare is good, whereas in those on Alor and Sumatra, distances to health providers are greater. None of the sites are ‘middle class’, but all encompass a range of socio-economic positions, from households reliant on extra-household support to survive to households affording consumer goods and generating surplus.
A team of Indonesian anthropologists with relevant local language skills conducted the data collection, supported during regular team meetings by the wider international research team, who speak Indonesian. For the Understanding Vulnerabilities project, life-history interviews with 10 individuals from each life-course stage were conducted in each field site, followed by randomized household surveys on household economy, health, crises and sources of support with 100 households per site. For the Care Networks project, 10 care-dependent older people per field site and members of their care networks and local stakeholders were interviewed repeatedly, and observational data on living conditions, care needs and care practices were collected. Purposive sampling was used in both projects to capture various circumstances (e.g., childless and child-rich families, female-headed households, households with migrant members and those with differently abled members and various care needs). Local leaders and existing contacts helped identify potential respondents meeting our criteria, and other individuals were recruited via network sampling. Given our interest in social, economic and health vulnerabilities and challenges arising from care dependence, our sample is skewed towards less well-off families, with approximately two-thirds being poor or ‘getting by’. Stakeholder interviews covered community leaders and representatives from local government departments (e.g., head of village, social affairs officer, N = 14), healthcare providers (N = 12), representatives from NGOs (N = 27) and community volunteers (N = 30) across five sites.
Interview notes and life histories were written up in Indonesian. Data analysis used thematic analysis for stakeholder interviews and case-study analysis—taking individuals and the networks surrounding them as the unit—for the life histories and interviews with older people and their carers. Interview data were augmented by analysis of representations of older people in media reports, governmental and NGO communications, particularly during the COVID-19 pandemic.
In this article, we draw on these representations of older people, on interview data and observational data from both projects. In the findings, we try to strike a balance between drawing out broad messages from our comparative and longitudinal qualitative evidence base and illustrating key points through case studies distilled from repeat interviews with the individuals portrayed.
IV. Older Indonesians’ Assumed Vulnerability
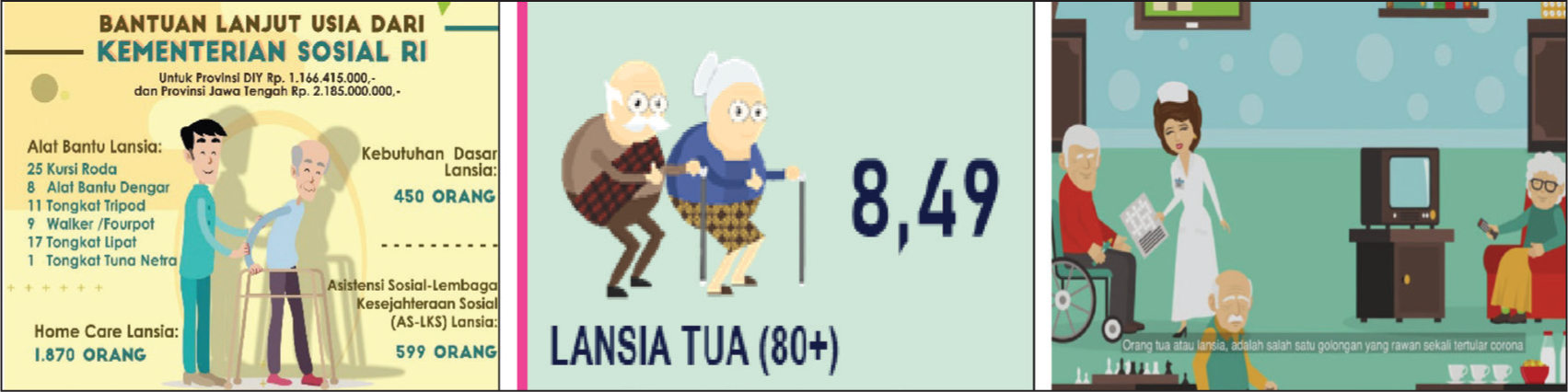
The COVID-19 pandemic in Indonesia reinforced and visualized dominant representations of older Indonesians as ‘vulnerable’, passive and in need of protection. Billboards, leaflets, social media posts and cartoon-style video clips portrayed ‘cute’ older people with white hair, bent posture and walking frames (see Figure 1). Often, they were towered over by younger people in uniforms signalling officialdom or surrounded by attentive family members. Older people’s vulnerability and a strong stay-at-home directive were emphasized (Vervaecke and Meisner, 2021). 2 The public response to these representations was overwhelming, with countless reports in the media of older Indonesians receiving support and necessities (Ekawati and Delpada, 2020; Insriani and Porath, 2020; Sare and Schröder-Butterfill, 2020; van der Ploeg, 2020).
The view of old age as a period of material and practical dependence and vulnerability predates Covid and is embedded in Indonesian policy discourse and practice. This has been clearly articulated in a recent analysis of Indonesian ageing policies by Lestari and colleagues (2022), which highlights tensions between contrasting representations at the policy level—tensions which this article seeks to substantiate at the level of lived experiences. The authors identify, on the one hand, the inherent assumptions of decline and vulnerability in later life that prompt calls for support; for example, ‘Older people are a vulnerable group of people who are entitled to receive more treatment and protection due to their special condition’ (p. 10). On the other hand, they highlight an upbeat discourse of successful and productive ageing, which is to be fostered to avoid older people becoming a burden. (We return to this alternative discourse in Section V.) The decline discourse is rendered benign in policy documents by emphasizing older people’s past contributions and their position as respected ‘role models’, ‘sources of wisdom’, people active in religion and spirituality. Their care and support are a cultural obligation that falls foremost on the family and community (Lestari et al., 2022).
An illustration of how the dominant decline or vulnerability discourse plays out at a local level can be given by introducing Darminah, one of our respondents in the Yogyakarta field site. Now in her mid-70s, Darminah had worked as an educator, raised a family and was active in a women’s organization. When she retired, she went along to the only community activity targeted at lansia (short for orang lanjut usia [people advanced age], which is the label for people aged 60 and over in Indonesia). She was dismayed at the boring and passive nature of the initiative, consisting purely of monthly measuring of blood pressure and weight. Darminah realized that this service reflected and reinforced the dominant stereotype of older people as dependent, which in fact she had shared until reaching retirement. In one of her interviews, she recalled her younger self-thinking that older people’s role in life was ‘already finished’ and no longer ‘productive’, that they ‘stay at home because they are used to feeling useless’. She had formerly told her own grandmother: ‘You don’t have to do anything, just sit and later all you need to do is eat’.
As with most stereotypes, this dominant view of a passive, domesticated, spiritual and dependent old age has partial correspondence with reality. This correspondence is examined next.
Deserved Dependence
With the emergence of a sizeable middle class in Indonesia (World Bank and Australian Government, 2019), an intergenerational model of old-age dependence and a labour-force model of retirement have gained currency. In these models, old age is imagined as a period of deserved dependence on others: older people no longer need to work; they may rest (istirahat) and concentrate on their spiritual welfare. In the familial domain, this encompasses dependence on adult children for material support and practical care. Thus, in their analysis of ageing policies, Lestari et al. (2021) find reference to older people’s ‘past contributions’, with responsibilities for care grounded in ‘cultural terms of reciprocity and familial obligation’ (p. 13). Beyond the family, for the small proportion (fewer than 10%) of older people who formerly worked as civil servants or members of the armed forces, this facilitated dependence finds expression in a low retirement age of 58 and generous government pensions (Asher and Bali, 2015). 3 The model of deserved dependence is echoed in our empirical data, but only among some better-off families.
Take Hadijah, a widow living in our Sumatran study community who has five married sons. The matrilineal Minangkabau of Sumatra have a strong tradition of labour migration (Indrizal et al., 2009; van Reenen, 1996). Hadijah’s sons all left the community after marriage, while Hadijah and her husband managed the family’s agricultural land. As Hadijah’s husband’s health declined, the sons discussed their parents’ growing support needs and nominated one son to return to the village and provide for the parents. In time, Hadijah’s husband died, and she suffered a stroke. All of her practical and material needs, including visits to healthcare services, are met by her coresident son and daughter-in-law who pride themselves on ‘forbidding’ Hadijah to worry about anything. Hadijah’s coresident son does not work, as his siblings send generous remittances to cover his costs.
Hadijah’s case epitomizes a model of family solidarity and an explicit division of labour among children to provide comprehensive and status-enhancing support and care for the older generation. This is underwritten by both demographic success (i.e., a large family, although lacking daughters) and economic success fuelled by remittances. Hadijah’s example is not unique, especially in our Sumatran study community where the matrilineal kinship system remains strong, and family reputation rests on successful migration and generous provision for the older generation (Kreager and Schröder-Butterfill, 2008). However, most of the older people we interviewed did not relish their dependence. Unless incapacitated, better-off respondents prefer making contributions, for example, by doing housework or overseeing agricultural work (cf. Norris et al., 2012). We heard frequent complaints about having to ‘sit around quietly’ (diam saja), and Darminah—introduced earlier—expressed regret at having prevented her mother from washing her clothes, despite this being an activity she enjoyed.
We argue that the benevolently ageist model of older people as vulnerable and in need of protection best reflects middle-class notions of deserved dependence, rather than the common reality of structured dependence. It is to this reality that we now turn.
Structured Dependence
Material and practical dependence in later life can be enforced not just by overattentive family members, but by discrimination, marginalization and poor health. Overt age discrimination in the Indonesian labour market starts early, with entry to many formal sector jobs restricted to people in their 20s or 30s, despite such discrimination being illegal. Ningrum and colleagues (2020) analysed nearly 9,000 Indonesian job adverts and found explicit age discrimination in two-thirds. They conclude: ‘Middle-aged adults (45–65 years old) tend to be the most vulnerable group that is frequently blocked from all job advertisement categories’ (p. 20).
Competition for work further marginalizes older workers and forces them into the least profitable roles (e.g., agricultural labour, collecting animal fodder and paid domestic work) (cf. Vera-Sanso, 2012). Our research on vulnerability across life-course stages, which included interviews with young and middle- aged adults, found that younger family members with work opportunities in the formal sector often expect older members to relinquish paid work and look after grandchildren. In peri-urban areas on Java, population growth and small industry are encroaching on agricultural land and tilting the local economy towards the service sector, which discriminates against older workers. In our East Javanese study site, for example, our survey evidence shows that local ownership of agricultural land has decreased steeply from 16% to 4% over the past 20 years, with most remaining land controlled by agribusinesses. Where village- based landowners might have employed poorer neighbours as sharecroppers into old age, agribusinesses use outside labour to complete the work efficiently and impersonally. When we first conducted research in East Java in 2000, many older women made a living as petty traders. For younger women, international labour migration was attractive at the time. Nowadays, competition in local trade is fierce, and few older women traders survive. The dramatic growth in small factories and formal-sector retail (supermarkets, department stores and petrol stations) has created opportunities for young high-school and university graduates; labour out-migration has reduced. Food trade is now a common activity for reproductive- and middle-aged women, as it is compatible with minding (grand)children. Older women have become squeezed out of this sector in the process: among better-off families into ‘deserved dependency’, among the poor into the most marginal retail positions (e.g., door-to-door sale of second-hand clothes) or unemployment. Aside from these social and economic factors, the early onset of poor health often further undermines older people’s ability to remain economically active. For example, on the island of Alor, fishing is an economic mainstay, but physically demanding. In our life history interviews, even several middle- aged respondents reported having had to give up fishing due to rheumatism or asthma.
Drawing together the evidence thus far, we see that the dominant view of older people as passive and dependent sits uneasily with more complex realities on the ground. Some older Indonesians are indeed economically inactive, and for some, this results in dependence on adequate family support, even if this dependence is experienced as disempowering. Others cease economic participation due to discrimination, lack of opportunities or ill health; yet, their economic dependence is not necessarily met by family or state support (Absor et al., 2022). In their landmark report on old-age poverty in Indonesia, Priebe and Howell noted that ‘Only about five percent to six percent of all elderly receive any sort of private or public pension’ (2014: p. 36). By 2020, this estimate had hardly shifted: fewer than 7% of households with an older person reported pension income as their main source of income (Badan Pusat Statistik, 2020). As we will see, older people’s lack of income from work or pensions impedes their access to healthcare and contributes to their care being experienced as burdensome by their families.
V. Indonesia Embraces ‘Active Ageing’
Let us bring Darminah into the picture again to introduce an alternative model of ageing in Indonesia. Having reached the official ‘old-age threshold’ of 60 years, Darminah realized the stifling limitations of the dominant stereotype of passive old age and set about challenging it. She started a community organization for older people, which became a regional showcase. The organization still runs monthly health check-ups. However, attendees now also receive training; they can use a library; and monthly meals are shared. There is an orchestra, weekly sports and annual excursions. The organization attracted regional government attention and is used to distribute benefits (e.g., livelihood grants for older people). Darminah has initiated a micro-credit scheme and hires agricultural land for older people’s use.
Darminah is interesting both for what she represents and promotes. She epitomizes an emergent alternative representation of older Indonesians as active, which is poles apart from the dominant rhetoric of passivity and vulnerability. In her leadership role, Darminah represents successful, even heroic ageing. Thousands of older people like her form the volunteer backbone of Indonesia’s welfare and health-provision landscape (Gadsden et al., 2021; Jakimow, 2018).
Through her organization, Daminah is promoting a model of later life associated with activity, productivity, engagement and health—in short, with ‘successful ageing’. This originally Western representation is gaining traction in print and social media, advertising, but also in Indonesia’s policies for older people. These include an (unevenly implemented) mandate for communities to run monthly clinics for older people (Pratono and Maharani, 2018). As Lestari et al. (2021) note in their discourse analysis of ageing policies, the call for government programmes is presented in a utilitarian way to ‘lengthen older people’s productive age … so that older people can be empowered, independent and play an active role in development’ (p. 10). This fits with Indonesia’s developmentalist ideology which sees individual citizens as having a duty to contribute to national development (Li, 2007). Current generations of older people were socialized into the ideology of development (kemajuan dan pembangunan) during President Soeharto’s leadership (1966–1998). Having reached the ranks of lansia (older people), it is again their duty to remain active so as not to become a burden on the state. Let us examine the extent to which older Indonesians achieve this.
Organized Sports Versus Necessary Activity
‘Active ageing’, with its focus on economic participation and health maintenance, is a welcome counterbalance to the dominant representation of vulnerability and decline in Indonesia. Programmes to strengthen older people’s health and livelihoods are empowering. In a country where stroke and diabetes are the leading causes of death and disability, appeals to engage in sport, improve diet and pursue health checks are important (see Figure 2). However, the top-down promotion of ‘active ageing’ can be patronising and irrelevant to the millions of Indonesians for whom this model has long had to be reality. This was captured humorously by an older man attending an NGO-led event on keeping active via exercise: ‘Does climbing a coconut tree count as 30 minutes of exercise?’

The mutually reinforcing contexts of poverty and deficiencies in social protection and family support are driving older Indonesians’ economic activity, albeit often under precarious conditions (Priebe and Howell, 2014; Utomo et al., 2019). A recent report on the status of older people by Indonesia’s statistical bureau provides clues to the pervasive necessity for them to work and their constraints on earning an adequate income (Badan Pusat Statistik, 2020). According to nationally representative data, more than half of Indonesians aged over 60 are working. The percentage is higher among men than women (65% vs 38%), but those in non-working categories are predominantly found to be ‘taking care of the household’ (31%), rather than being without employment (1%). Of those classified as working, nearly half work 35 or more hours a week. Levels of work are higher in rural than urban areas, reflecting greater opportunities for work, chiefly in agriculture, livestock and fishing, and lower access to social protection and family support (Badan Pusat Statistik, 2020). The vast majority (86%) of older workers are in the informal sector, with no social security, rights or fixed income. Being a woman, a rural dweller and/or less educated makes it more likely to work in the informal sector. Yet the report interprets these statistics by reinforcing ageist stereotypes, rather than problematising informalized work: ‘Physical and psychological abilities have decreased, making the informal sector an option for elderly workers. The formal sector prioritizes the qualifications and skills of workers, causing fewer job opportunities for the elderly in the formal sector’ (p. 62).
Older people’s work is structured not only by socio-economic position but also by family networks. As noted, many better-off Indonesian families are encouraging older parents to cease work and ‘rest’. By contrast, poorer strata often have inadequate family networks resulting from life-course interactions between poverty and demographic outcomes. For example, in earlier research, we found sizeable minorities (between 7% and 25%) of older people in our study communities to be involuntarily childless (Kreager and Schröder-Butterfill, 2007). Childlessness and de facto childlessness (i.e., having offspring but receiving no support from them) was stratified by economic status, with as many as 45% of older people in the lowest of four strata in our East Javanese site having no children to rely on (Schröder-Butterfill, 2015: 270). Among the richest group of older people, 62% had three or more children, often with some children nearby, some away and sending remittances. 4 In short, especially poor, older Indonesians often have no choice but to continue working and maintaining independence, as they lack adult children to rely on despite family support being enshrined in policy assumptions.
In addition to a lack of family support for older people, significant minorities live in skipped-generation households where they provide care and support for grandchildren whose parents are dead or absent (Beard and Kunharibowo, 2001; Schröder-Butterfill, 2004). As we see in the following section, older people sometimes act as primary carers for an incapacitated spouse or older parent. Older people with such responsibilities are unable to participate in health checks or organized sport, because they are working or caring.
Various realities described in this section underline the deficit of neoliberal and successful ageing approaches that regard experiences in later life as an individual responsibility, rather than the outcome of lifelong inequalities and threats to livelihoods and health. They feed the stigma of physical dependence and cognitive infirmity, to which we now turn.
VI. The Invisibilization of Frailty
We have shown binary representations of later life in Indonesia—one of vulnerability, passivity and deserved dependence, another of active, successful ageing. Both are limited and affect the support and recognition older people receive. More importantly, neither representation captures the reality of profound dependence and frailty which a minority of older people experiences at any time and which is a pervasive experience prior to death. The invisibilization of profound dependence matters, because it means the tacit delegation of care to the purely domestic and kinship domain, rather than representing an existential human condition requiring a collective response (Razavi, 2011). In this section, we document the neglect of frailty in media representations and policies before discussing the implications of this for older people and their carers.
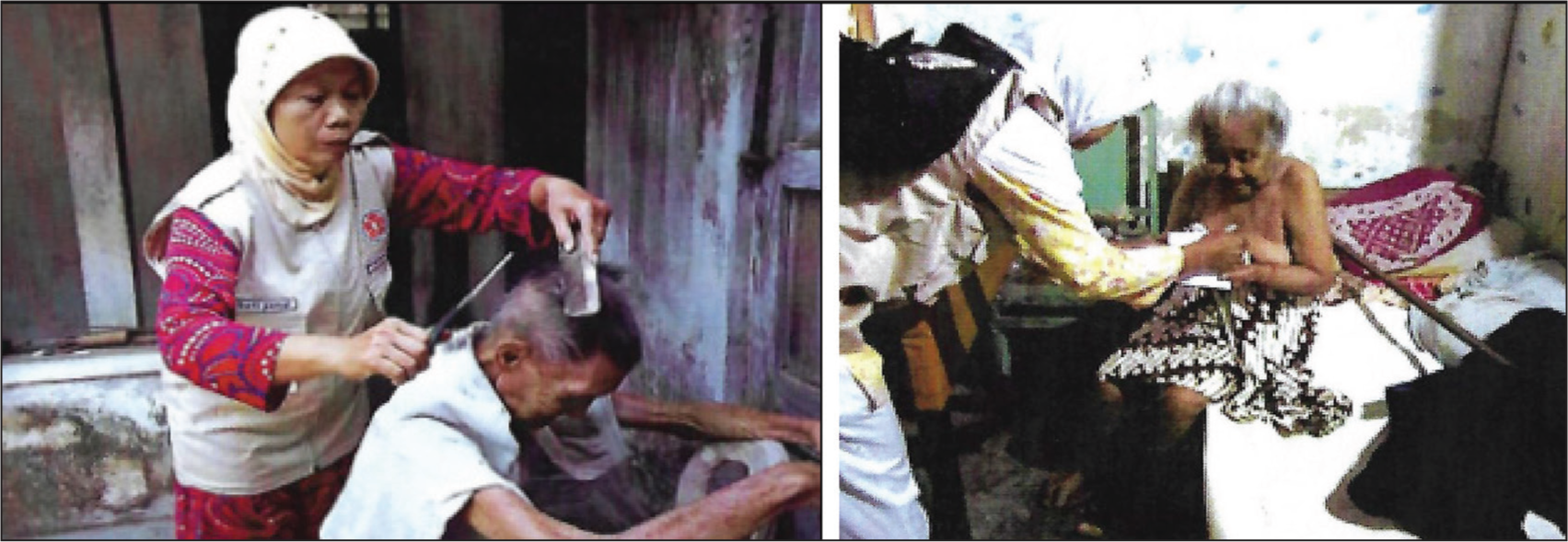
We encountered virtually no realistic representations of frailty. While cartoon-style images abound of ‘cute’ older people identified as old through markers of dependence, like walking sticks or wheelchairs, there is a dearth of representations showing the reality of physical or cognitive dependence, for example, by depicting older people who are bedridden. One exception was a Yogyakarta NGO that provides rare volunteer-based homecare to older people lacking family support. Their brochure includes photos of older people being bathed or groomed by volunteers (see Figure 3). The depictions are uncomfortable, as they juxtapose semi-clad older people with young volunteers in NGO attire. However, they are important because they capture human frailty and a positive response to this, namely care.
The lack of representation of real dependence is striking, given that more than a quarter of Indonesian households contain an older person (Badan Pusat Statistik, 2020: 19), and our household survey data suggest that between 3% and 11% of older people require help with basic activities of daily living (e.g., getting dressed, bathing and eating). In addition, cognitive impairment in later life is not uncommon. According to survey estimates from Java in 2007, between 3% and 16% of older people had dementia, with particular prevalence among rural dwellers and those with lower education (Hogervorst et al., 2021). Recent estimates from a national survey suggest nearly one-third of older Indonesians have memory impairment (Handajani et al., 2023).
Older care-dependent people are missing not only from media representations but also from policies. In the previously cited discourse analysis, Lestari et al. (2022) found a pervasive dichotomy between ‘success’ and ‘decline’ representations aligned with a dichotomy between ‘public responsibility’ and ‘familial obligation’. Significantly, for the category of ‘successful’ agers, public provision in the form of livelihood, education and health interventions was included in policies. However,
[T]he ‘successful ageing’ discourse, with its focus on prevention and health promotion, provides no space for provisions of long-term care in older people’s lives. The Indonesian of Ministry of Health has admitted that caregiving is still neglected in the national action plans on health and ageing. (Lestari et al., 2022: 16)
Instead, when it comes to care, existing policies attribute responsibility firmly to families as the natural arena: ‘The limitation of government obligation to provide care for older people is made possible by retaining the notion of familial obligation and the private sphere as the most appropriate space of caregiving’ (Lestari et al., 2022: 16).
While the recent National Strategy on Ageing (Presiden Republik Indonesia, 2021: 5) refers to ‘expanding the scope of long-term care for the elderly’, concrete targets are modest, for example, increasing community health centres that develop (undefined) LTC from 0% to 24% by 2024 or districts with pilot LTC systems from 5 to 10 (of more than 500) across Indonesia.
Finally, older care-dependent people are also marginalized in actual service provision for Indonesia’s older population. A manifestation of this is that government-implemented community health posts (posyandu lansia) run by nurses and volunteers (kader), which form the backbone of older people’s health provision across Indonesia, are premised on older people being able to attend in person (Pratono and Maharani, 2018). We observed monthly health check-ups in four of five study communities. The people who attended were able to get there independently or, in rare cases, accompanied by a relative. Even the progressive community organization headed by Darminah, which offers to collect older people from remote hamlets by motorbike or pick-up truck, requires attendees to be ambulatory. In our research evidence, with few exceptions like the NGO cited above and localized pilot programmes, there is neither LTC nor healthcare provision involving home visits. Once older people are bedridden or unable to walk outdoors, their engagement with formal services largely ceases. They also disappear from public view, which is more noticeable in Indonesia where much of social life takes place outdoors. We surmise that several factors drive the invisibilization of care dependence, chief among them that care is regarded a private responsibility. In addition, overt signs of physical and mental decline evoke fear, disgust or pity, and awareness-raising would require a public and policy response, for which Indonesia does not seem ready.
Implications of Invisible Care Dependence
Why does it matter if physical frailty and the need for care are not among contemporary representations of later life in Indonesia? After all, the two dominant representations already capture ‘opposite visions’ of later life, and promoting active ageing is important for countering pervasive stereotypes of vulnerability. Emphasising frailty and need would risk undermining the positive recasting of old age as a period when people’s contributions and independence continue. On the basis of our ethnographic evidence, we argue that it matters both for policy and humanitarian reasons. The relegation of dependence and care to the purely domestic, familial sphere is unjust, as it reinforces gender, economic and age inequalities within families; it also contributes to inadequate care for older people (Schröder-Butterfill and Fithry, 2014; van Eeuwijk, 2020); finally, it prevents engagement with frailty, decline and interdependence as fundamental parts of the human experience. We provide two indicative case studies to develop these points.
Sriamah was a woman in her early 60s living in our East Javanese study community. She suffered from diabetes and had a fall which left her with a badly broken leg. An operation was advised, but her husband worried about the cost, despite having joined the new health insurance system (Badan Penyelenggara Jaminan Sosial [BPJS]). Sriamah was taken to an alternative healer, and when her condition did not improve, she accessed no further healthcare. Sriamah lived with her husband and a married daughter who works in a factory. Most of her care was provided by Sriamah’s husband, who gave up work as a construction worker to look after her. He was visibly frustrated by his wife’s lack of progress. A nearby daughter, not in paid work but with young children, sometimes helped. Without assistance, Sriamah’s husband found it difficult to move her from bed to chair or wheelchair, so Sriamah often spent hours in the same position. One of Sriamah’s two sons provided occasional financial support, and a neighbour sometimes visited. The local volunteer-based primary health clinics do not cover home visits. After 18 months of being care dependent, Sriamah died. Her husband has not managed to resume work.
Sriamah’s case is not unusual. Many Indonesians experience the onset of care needs early, due to risk factors such as high blood pressure, diabetes and stroke (Kusuma et al., 2009; Turana et al., 2021). Her pattern of healthcare use was common, involving different providers in early stages of a health crisis, followed by disengagement from healthcare due to financial and logistical reasons (especially transport) and lack of confidence that lasting benefits will ensue (Widayanti et al., 2020). Although Indonesia’s new health insurance system (BPJS) covers treatment in community health centres and government hospitals, waiting times are long, and lack of clarity about entitlements results in hesitancy among the poor (Kharisma, 2020; Shrestha, 2021). As medical provision does not extend to home visits (bar as pilots in some locations), the family is the only source of care for Sriamah. Without help and expert guidance, Sriamah’s care was not geared towards improving her functioning or slowing her decline. Her example illustrates that the long-term provision of familial care often falls predominantly on one person, which is experienced as burdening (cf. van Eeuwijk, 2006). Sriamah’s case is slightly unusual because the main carer is a man; women are frequently lead carers in Indonesia (Absor et al., 2023). In this family, the coresident daughter’s better-paid formal-sector job ‘trumped’ Sriamah’s husband’s informal-sector work, and thus he was expected to cease work. Having been out of the labour force for two years, he has unsurprisingly not gained re-entry into a profession where competition from youth is strong. The opportunity cost of caring is thus high, in addition to the physical and mental toll that unsupported caring can take (Pot et al., 2018).
A second example, from our Sumatran field site, attests to the stigmatization and shunning of physical and mental decline in a context where these are rarely discussed.
Mutaya is a middle-aged, poor divorcée living with her elderly mother and aunt. Her mother is paralysed, while her aunt is bedridden and has dementia. Mutaya is primary carer for both. Her only brother—who used to provide material support—recently died. Her mother clearly finds her extreme dependence distressing and lamented in one of the interviews: ‘It can’t be helped, I’m paralysed now, can no longer earn money, can no longer take care of myself. Everything is taken care of by her!’
Mutaya’s relationship with her aunt, Suci, is ambivalent. Given that Suci has two local sons, it was not inevitable that her care would fall on her niece. Until her health declined, Suci lived alone in a house next to Mutaya’s. Following a stroke and onset of dementia, she was initially taken in by one of her sons. However, he feared that the smell resulting from his mother’s double incontinence was repelling customers from his food-stall. Her other son felt unable to accommodate her, as he was living with his parents-in-law: a precarious position for a man within the matrilineal kinship logic. Thus, Suci returned to her home, with relatives coming in to provide care. This arrangement failed amid growing care needs, so Mutaya—being on hand—took Suci in. She receives help from Suci’s granddaughter, who visits every other day, brings incontinence pads and helps with changing Suci. During the interview, Mutaya expressed embarrassment for her aunt, who kept asking for food. Especially the disrupted nights take a toll on Mutaya who works as an agricultural labourer and feels torn between needing to earn a living and providing care. Mutaya herself has a stigmatized health condition and is childless. She is shunned by the wider community and not included in the distribution of local government support.
On the one hand, Mutaya readily accepts her filial responsibility towards her mother and regards the care she provides as an expression of their life-long, mutual relationship. On the other hand, her poverty, poor health and lack of a wider network undermine the easy policy assumption that families can absorb the care needs of Indonesia’s rapidly ageing population. For many families that are economically and demographically precarious, the single-handed provision of care over long periods threatens livelihoods and results in arrangements that fail to foster rehabilitation, social participation or a positive social identity (World Health Organization, 2017).
The experience of Mutaya’s aunt, Suci, further highlights the avoidance and stigma that outward signs of failing bodies and minds can engender, which further contribute to their concealment and marginalization. Complaints about smell appear repeatedly in our data on care and are advanced as justifications for why care cannot be provided or sustained by a potential care network member or why visitors are unwelcome (cf. Gamburd, 2021; Mitteness and Barker, 1995; Norris et al., 2012). In a hot climate and with incontinence pads expensive relative to many families’ income, such comments are relatable. Yet the smell discourse, alongside common reference to care- dependent people’s insatiable appetite, mental confusion or past misdeeds arguably point to a deeper level of rejection. Such comments deny a valued identity for care-dependent people and contribute to their and their carer’s isolation (cf. Higgs and Gilleard, 2016). The case of Mutaya and her frail relatives bears witness to the isolation and stigma that care can entail in a context where dependence is hidden from view, never openly discussed nor problematized in public discourse.
VII. Discussion and Conclusion
This article critiqued binary representations of older people in Indonesia, examined their correspondence with heterogeneous lived realities and traced the implications of limited and narrow representations for the lives of older people and their carers. In this final section, we summarize key arguments and link them to wider debates in development studies and gerontology.
Our examination of Indonesian public discourses and ageing policies revealed the dominance of a binary model in which older people are regarded either as vulnerable or active. Although older people’s assumed vulnerability is considered problematic—a potential drain on resources—it does not encompass the imaginary of deep dependence as associated with the ‘fourth age’ in Western discourses (Gilleard and Higgs, 2011). Instead, the representations draw on benevolent ageism (Keating, 2022), emphasizing older people’s reduced resilience, their need for protection and their deserved withdrawal into a domestic sphere, where their lifetime contributions are rewarded by attentive familial care, rest and (in the case of civil servants) generous pensions. The alternative, increasingly influential representation, which owes to global discourses and programmes of successful ageing (Rowe and Kahn, 1997), promotes a model of older people as healthy, economically active and contributing. In this model, the role of the state and civil society is primarily to encourage individuals’ efforts at health maintenance (e.g., through health checks and exercise), with innovative organizations like Darminah’s also offering educational and livelihood programmes.
Our article has used developments in Indonesia as a case study for understanding how representations and policies relating to older people interact with realities on the ground. These interactions are not particular to Indonesia but are replicated across a range of LEDC contexts. Older people’s situations are more heterogeneous than binary models of vulnerability versus success, with circumstances in later life patterned by life-course experiences of work, socio-economic status and demographic events. Labour force participation by older people is often a necessity in the Global South (HelpAge International, 2019). Many older people are forced into activity not by exhortations to exercise but by lack of family support, caring responsibilities and unavailable pensions (Cameron et al., 2010; Giang and Nguyen, 2016). Conversely, for many people dependence in later life represents not so much security and attentive care but dependence structured by ageism in the labour market and a lifetime of adversities resulting in early ageing and ill health (Vera-Sanso, 2013).
For scholars and practitioners concerned with care in later life, the most important elision in the dominant representations of older people is the invisibilization of human frailty and decline. Invisibility and precarious care mutually reinforce each other: by excluding real frailty and need from public images and discourses of later life, by emphasising policies for active ageing at the expense of LTC and by promoting families as the natural locus of old-age care, the common experience of care dependence is marginalized into the domestic sphere and remains unsupported (Enríquez et al., 2021; Razavi, 2011). This ‘familism by default’ has implications for care-dependent people and their family carers (Keating, 2022). Our evidence adds to the literature that demonstrates that a purely private, familial response to human frailty and decline creates unsustainable and unjust burdens on families (Pot et al., 2018; Sabzwari et al., 2016). As our case studies illustrate, domestic care provision tends to reinforce economic, gender and age inequalities, with individuals who have the weakest attachment to the labour market and lowest social status often bearing the brunt of responsibility. This can contribute to poor quality care if individual family carers ‘muddle through’ unsupported and unrecognized, as in the cases of Mutaya and Sriamah’s husband, rather than care being shared among a larger network, as illustrated by Hadijah. Of particular concern is the often low engagement with health services by care-dependent older people because of real and perceived barriers associated with cost, logistics and shame. Healthcare professionals thus more rarely see frail older people, further contributing to their care needs not being prioritised.
We therefore argue for more nuanced and heterogeneous discourses and representations relating to ageing, and we call for policy responses that encompass frailty, deep dependence and cognitive decline. Such heterogeneity is already acknowledged in gerontological and development studies research—not least in this special issue. It is also reflected in global initiatives, such as the United Nations Decade of Healthy Ageing (2021–2030) and WHO Global Strategy and Action Plan on Ageing and Health (2017), which include explicit demands on nations to develop not only health promotion and active ageing strategies but also LTC strategies involving older people, families, communities, NGOs and the state.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Universities of Southampton and Western Australia and from LIPI in Indonesia. The first author had a foreign researcher permit from the Indonesian Ministry of Research, Technology and Higher Education for the ARC project; for the ESRC project, data collection was exclusively conducted by Indonesian researchers. Data collection for the ARC project was completed before COVID-19, whereas fieldwork for the ESRC project was delayed due to the pandemic and initially involved remote interviews with stakeholders until face-to-face interviews with older people and their informal carers became possible.
Funding
We acknowledge the generous funding from the Australian Research Council (Discovery Grant DP170101044) for the project Understanding Social, Economic and Health Vulnerabilities Across the Lifecourse in Indonesia (2016–2021) and from the Economic and Social Research Council (ES/S013407/1) for the project Care Networks in Later Life (2019–2023), on which this article is based.