
Abstract
This article theorises a group of mothers’ experiences of shame as a result of feeding infant formula to their children. Drawing on interviews with formula and breastfeeding mothers, the author brings together insights from scholarship on shame, feminist scholarship on reproductive labour and the Marxist notion of estranged labour to demonstrate that shame causes the formula-feeding mothers in this study, who initially wanted to breastfeed, to be estranged in their labour as mothers. The article addresses a gap in qualitative infant-feeding scholarship, which focuses primarily on breastfeeding. It provides an empathic account framing breastfeeding and formula-feeding mothers as potential allies against ‘controlling images’ of motherhood who face different facets of the same pressure to fulfil idealised roles. Both scholarly work on reproductive labour, and public programmes supporting new mothers, should account more seriously for the experiences of formula feeding mothers.
‘I’m in a yoga class. I did a post-baby mama yoga class. And one day I was getting ready to leave and the girls were talking about how bad formula was, and I came home and I started to cry’. 1 Sally shares this anecdote with me in her living room, where we are accompanied by Sally's contented, sleeping baby, and surrounded by many signs of care and attention: toys, baby blankets, bouncer and baby books. Sally is a devoted mother, yet struggles with feelings of guilt and shame because formula is part of her baby's diet. Sally has her reasons for using formula. I do not list them here, because doing so might suggest that she needs to explain herself. Instead, let us focus on the yoga class, the other mums and Sally's tears. Sally felt ‘shamed’ and suffered from feelings of guilt related to formula use. How can we make sense of Sally's feelings of guilt and shame when she is clearly a competent and attentive mother? Like the other mothers that appear in these pages, Sally is a well-educated, middle-class, urban mother, for whom spaces such as the yoga studio and the organic market play an important role in communicating culturally dominant notions of idealised motherhood. The message that ‘breast is best’ is part of how these mothers envision healthy, natural childrearing – a practice they sometimes frame using the idiom of ‘crunchy’ motherhood, an idiom which they feel pressure to embody. All of the mothers discussed here intended to breastfeed, and began breastfeeding when their children were born, with only half exclusively breastfeeding for the first six months of their child's life. In this article, I use Karl Marx's notion of ‘estranged labour’ to theorise the isolation and shame experienced by the mothers whose breastfeeding was interrupted. In recent years, extensive public campaigns have been made to re-value breastfeeding. Feminist theorists have also successfully established that breastfeeding work is productive, valuable work (Galtry, 1997: 2–3; Lee, 2018), and that care-work and waged-work are combined in complex and often problematic ways (Hays, 1996; Hochschild, 1997; Boyer, 2014). But what about the reproductive labour of formula-feeding mothers? Their experiences are under-theorised at best, and their reproductive labour is not adequately acknowledged.
Infant feeding is a highly politicised topic, not least because it regrettably operates as a social test of sorts, grounds for evaluating how good mothers are. This article seeks to contribute to infant-feeding debates by offering a different angle from which to consider infant feeding. The article makes two contributions to the literature on infant feeding. The first is empirical, the second theoretical. First, while there are numerous accounts of the experiences of breastfeeding mothers, often admirable and beautiful (e.g. van Amsterdam, 2015; Mathews, 2019), there are comparatively few qualitative, descriptively thick scholarly accounts of formula-feeding mothers’ experiences. This article contributes to correcting this gap in the literature, which is important, because it has material consequences. Descriptive, evocative accounts of the struggles faced by breastfeeding mothers can be used to advocate for increased services and to support for them. Formula-feeding mothers also require support and affirmation.
The second contribution is a theoretical move in which I locate formula-feeding mothers analytically and politically in the same boat as breastfeeding mothers. All mothers are subject to ‘controlling images’ (Hill Collins, 2014) against which they are judged. The nature of these images depends upon one's social location, as established by factors such as social class, racialised identity, age and abilities. Some images are group specific, such as Hill Collins’ ‘strong Black mother’ (p. 174), and some, being culturally dominant, affect all mothers, although they may articulate differently with different identities – provoking compliance in some, and resistance in others. The breastfeeding mother is typically held up as an icon of idealised motherhood; however breastfeeding and formula feeding are often juxtaposed antagonistically. Think only of Time Magazine's cover from 21 May 2012, which featured a defiant-looking woman breastfeeding her three-year-old son, overlaid with the question in bold red font: ‘Are you mom enough?’ (Pickert, 2012), or of the blaming of breastfeeding promotion for the suicide of Canadian mother Florence Leung in 2017 (see for example Tuteur, 2017). Most of what we hear about infant feeding evokes such deep divides between formula-feeding and breastfeeding mothers. In this climate, scholarly critiques of breastfeeding promotion on one hand, or of formula feeding on the other, are likely to appear to take sides, regardless of their intention. The incredible amount of effort, knowledge and attention that breastfeeding requires has been well established at this point (e.g. Galtry, 1997; Dykes, 2005; Bartlett, 2005). By bringing to bear the notion of estrangement, and by acknowledging and foregrounding some of the struggles of formula-feeding mothers, I demonstrate that formula-feeding mothers are subject to the same erasure of their labour under patriarchal culture as breastfeeding mothers. I affirm that formula feeding, like breastfeeding, falls under the umbrella of reproductive labour. Like breastfeeding, formula feeding can be estranged under certain circumstances. This draws our attention away from divides between breast vs. formula feeders, and to the fact that mothers are all contending with controlling images developed within the context of a misogynistic culture. Focusing on their commonalities opens the possibility of framing them as potential allies against controlling images of motherhood and advocating for inclusive supports, a refreshing alternative to the tiresome notion that they are adversaries.
The Marxist feminist interpretation of the notion of estranged labour that I develop illustrates that although formula feeding constitutes part of the labour of childrearing, feelings of shame for using infant formula instead of breastmilk can introduce into women's labour of infant feeding an experience of estrangement that is analogous to Marx's four-part typology of estrangement as experienced by waged labour under capitalism. In the next section, I describe the research on which this argument is founded. Following this, I lay down some theoretical underpinnings to help us understand why shame might emerge in the infant-feeding encounter. Finally, I devote the majority of the article to the third section, where I use the experience of shame in formula feeding to bolster the argument that all infant feeding is labour – and formula feeding is sometimes estranged labour.
Context: the study
I develop this argument by drawing on interviews conducted in 2016 with twelve mothers in the metropolitan region of St. John's, which is the capital city of the province of Newfoundland and Labrador, Canada. An island in the North-Atlantic Ocean, the province is sparsely populated (529,426), with roughly half of the province's population (211,003) residing in the St. John's metropolitan region as of 2016 (Newfoundland and Labrador Statistics Agency, 2021). In 2016 Young et al. reported that Newfoundland has low breastfeeding rates – with the provincial breastfeeding initiation rate at 70 per cent, compared to a Canadian national average of 89 per cent. The province, and St. John's in particular (because it is urban and thus far more accessible in terms of services for its inhabitants), has benefitted in recent years from an intensified campaign to promote breastfeeding, including video commercials and billboards featuring local celebrities who encourage mothers to breastfeed, posters normalising breastfeeding in public, the provincial Breastfeeding Coalition's promotion of the World Health Organization's (WHO) ‘Baby Friendly Initiative’ and the naming of the local infant weigh-in clinics as ‘breastfeeding support groups’. Therefore, St. John's reflects both the international trend of the past two decades to encourage breastfeeding, but also a prominent practice of formula feeding informed by myths about breastmilk, and discomfort with the practice of breastfeeding (Temple Newhook et al., 2013: 33–40; Young et al., 2016: 226).
From January to July 2016, I sought interview participants via purposive random sampling (local posters, word of mouth, email and social media), including adult (age nineteen and over) mothers of children aged three and under, raising their children in the St. John's region. I actively sought to include both breastfeeding mothers and formula-feeding mothers (including exclusive formula feeding and mixed feeding of breastmilk and formula). Participants took part in a semi-structured interview of approximately one hour, in a location of their choosing. Interviews were recorded and transcribed by the author and analysed via repeated sessions of interpretive coding (‘thematic analysis’) (Gilgun, 2014: 662; Saldaña, 2016). Insights were also compared against fieldnotes and analytic memos kept throughout the research period, and against clarifying questions asked of participants throughout the research process. All names used in this article are pseudonyms chosen by the research participants, and this research was approved by an institutional interdisciplinary committee on ethics in human research at the author's place of employment.
Newfoundland is relatively homogeneous in terms of its racial and ethnic composition, with over ‘95% of Newfoundlanders identify[ing] themselves as either of Canadian, English, or Irish origin’ (Statistics Canada, quoted in Young et al., 2016: 225), and, when coupled with the fact that infant feeding is a sensitive and highly fraught topic, recruiting a diversity of participants was a challenge. Asking parents how they feed their children, and why, may appear as an unwanted opportunity to be scrutinised and judged. The difficulty of recruiting participants to be interviewed on this topic thus became one of the predominant themes of this research. All participants were white, well educated, middle class and in committed relationships with men. Initially, only women who had managed, in their view, to breastfeed ‘successfully’ presented themselves as participants. Although most of them spoke of local friends and relations who formula feed, they typically acknowledged that it is a sensitive topic, and that it would be difficult to talk with them about formula feeding.
I began to doubt after the first three months that I would manage to conduct interviews with any formula-feeding mothers. This state of affairs only changed six months into my research when I met Kathleen, who volunteered to participate after hearing about the study by word of mouth. Kathleen was a formula-feeding mother who served as something of a ‘gateway’ informant. Unbeknownst to me, after her interview, Kathleen endorsed my study on a closed social media group for formula-feeding mothers. Thus, the day after her interview, I woke up to several emails from formula-feeding mothers who were keen to participate. So it was that I came into contact with several of the formula-feeding mothers in this study. While I draw on responses from all twelve participants, this article focuses primarily on the experiences of the seven formula-feeding mothers, in an attempt to understand the lived experience of this group in a province where breastfeeding rates are the lowest in Canada and where there is a visible pro-breastfeeding campaign.
The qualitative, interview-based research undertaken here is ideal for ‘examining individuals within their cultural frameworks’ (Morrow, 2005: 253). My approach was to be an empathic listener, with open-ended questions that allowed research participants to direct the conversation towards what they felt was important. With respect to sample size, Morrow has noted that a rule of ‘“the magic number 12” is as good as any’ (2005: 255), though a good guide for choosing a sample size is when answers become redundant. The repeatedly articulated concern from mothers about the need for inclusive support demanded my attention. Within the group of twelve participants, a notable repetition emerged from participants surrounding the need for support for all mothers, including formula-feeding mothers. The smaller sample allows respectful attention to the accounts of participants. I see the effort to understand the experiences of this small group of urban-dwelling mothers in terms similar to van Amsterdam's description of the goal of her autoethnography: trying to ‘create an empathic understanding of those groups or stories that are underrepresented and/or marginalized’ (2015: 270). In short, I am not attempting to make large inferences from this research. It cannot capture the broad range of formula-feeding experiences. I believe that the participants’ experiences are inherently valuable and worth understanding for their own sake. Large inferences, rather, must come from taking multitudes of small studies such as this one, and considering them in relation to each other. Woollard and Porter (2017: 515), for example, note that several studies have reported an association between formula feeding and guilt, blame and failure. This study can contribute one example to that larger body of literature.
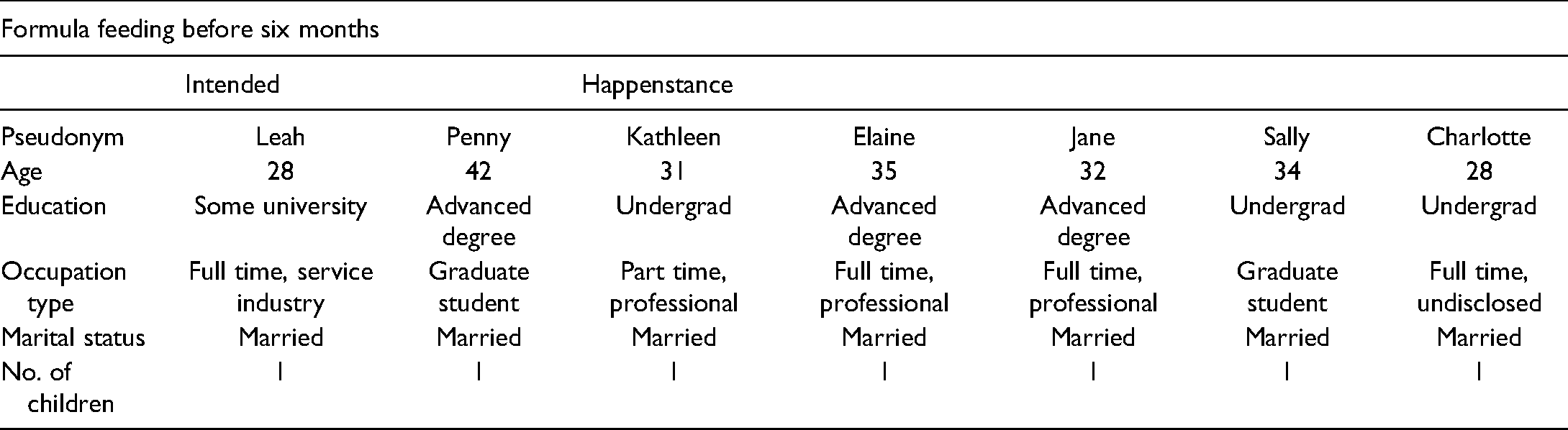
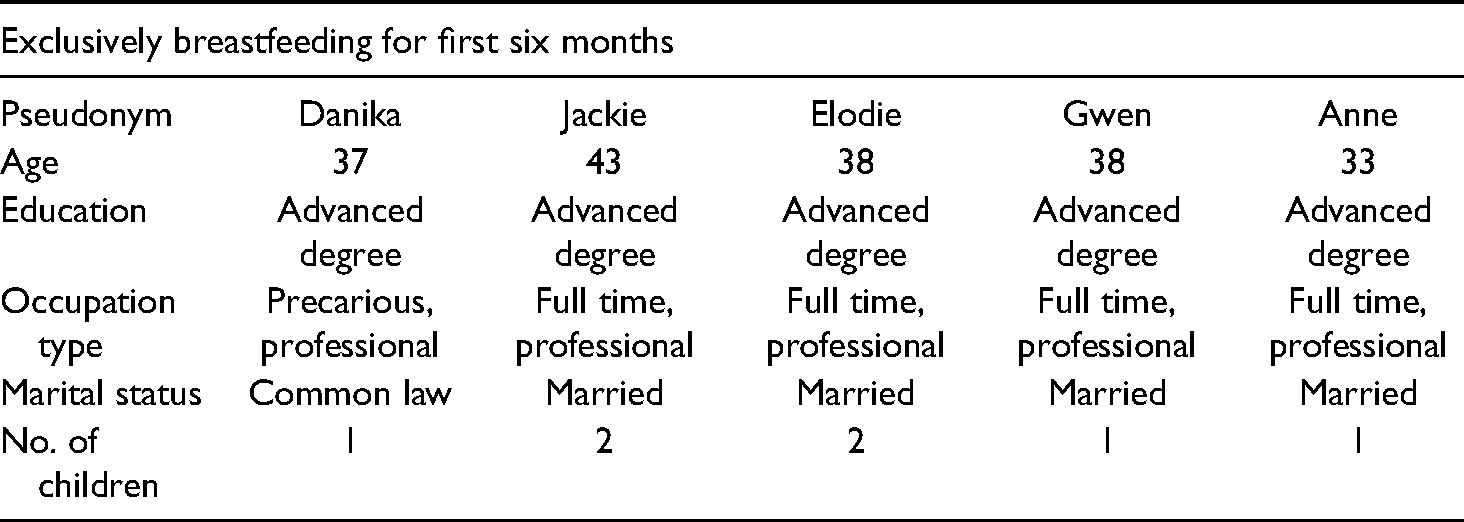
Although many parents choose to use formula exclusively from birth onwards, and for a variety of reasons, all of the women who participated in this research intended to breastfeed and attempted to initiate it. Seven out of the twelve research participants formula fed their children in some capacity within the first six months, while five exclusively breastfed for the first six months (see Tables 1 and 2 for life course information). Most of those who used formula did so as a secondary option, typically in the face of unforeseen circumstances (Kathleen, Elaine, Jane, Sally and Charlotte). I refer to this situation as ‘happenstance’ formula feeding as opposed to a situation where formula is a parent's first choice, which I refer to as ‘intended’ formula feeding. 2 One mother (Penny) took up intended formula feeding when her child reached four months of age and she returned to waged work. One mother (Leah) intensely disliked breastfeeding and thus switched to intended formula feeding after twelve days. Like the five mothers who exclusively breastfed for six months, in accordance with their own initial wishes (Danika, Jackie, Anne, Elodie and Gwen), Penny and Leah, having intentionally ceased breastfeeding, convey far more positive feelings about formula feeding and do not appear to feel shame or guilt. However, they do experience aspects of the shaming of formula-feeding mothers that I discuss below, notably a lack of support and a sense of not fitting into idealised stereotypes. However, among this group of participants, the acute cases of distress seem to be experienced by mothers who felt they were unable to breastfeed despite wanting to. This makes the theory of estranged labour – which is a theory of unfree labour – all the more compelling.
Life course information for formula-feeding mothers.
Life course information for exclusively breastfeeding mothers.
With a long cultural history of using breastmilk alternatives, and a strong contemporary movement to increase breastfeeding rates, local mothers tend to report a ‘damned if you do, damned if you don’t’ dynamic in relation to breastfeeding, which I will comment on at greater length below. Since opinion is deeply divided on the subject, both breastfeeding and formula-feeding mothers report feeling uncomfortable and subject to unwanted judgment and scrutiny regarding their infant-feeding practices. With this in mind, I now turn my attention to explaining why the infant-feeding experience is rife with opportunities for mothers to feel shame.
The infant feeding encounter: fertile ground for shame
There has been fairly significant scholarship over the past two decades on the issue of motherhood and shame and/or guilt – especially as it relates to feeding children. Dealing directly with notions of ideal womanhood and ideal mothering, the issue of infant feeding creates a multitude of interconnected expectations. Formula-feeding mothers, especially, convey feelings that they sometimes describe as guilt, and sometimes as shame, with regards to their choice to formula feed. Some have ascribed these feelings to the focus on formula use as ‘risk’ behaviour associated with some breastfeeding promotion campaigns (Kukla, 2006: 173–175; Knaak, 2010: 345–346; Taylor and Wallace, 2012: 80–81). Others have noted the coercive nature of some breastfeeding advocacy strategies (Jung, 2015: 97–124). Most convincingly, Elizabeth Murphy explains the guilt- and shame-inducing pressure on mothers by reference to Foucault's description of biopower – those invisible, ‘disciplinary technologies whose aim was to produce a “docile body that may be subjected, used, transformed and improved”’ (Murphy 2003: 436). The point of improving the docile body is largely to improve the health of the population. Murphy (2003: 436–442) points out that medicine is key to these technologies, playing a significant role in shaping what is considered to be normal and morally upright. Biopower is not coercive, but relies on tools like dominant medical discourses to encourage self-policing. Deviations from medical prescription can therefore be read by the self and others as abnormal or morally wrong. Thus, mothers who formula feed with shame are mobilising both dominant medical discourse regarding what is right and normal, and their own ‘counter-discourse’ (Knaak, 2010: 351) that arises from the specificity of their experience as mothers. Murphy (2003) demonstrates that in the prenatal context, mothers frame themselves as inexpert and reliant on (trusting of) medical advice, however postnatally as they become more experienced with respect to their baby's particular context, they are more likely to see themselves as expert and to diminish the expertise of medical professionals. Thus, the power of their counter-discourse may increase with time and diminish their shame. As I discuss later in this article, I observed this phenomenon among my research participants.
Women often appear caught in a lose-lose situation when it comes to infant feeding. This article describes the struggles of a group of mothers who adopted formula feeding as a secondary choice to breastfeeding. However, even breastfeeding mothers face obstacles, specifically in public, where their exposed breasts are often seen as offensive, transgressive or inappropriate (Acker, 2009; Lane, 2014; Mathews, 2019), and who find they must ‘whisper and tiptoe with nervous discretion’ (McNish, 2013) in order make themselves as invisible and unobtrusive as possible. This sense of discomfort and lack of support is certainly echoed in the experiences of the exclusively breastfeeding mothers who spoke with me. Jackie, for instance, remembers breastfeeding on a lakeside bench when a bystander ‘came up and said to me “can’t you take that inside”? I was like inside where? Where would you like me to take this? My car?’.
While formula-feeding mothers may suffer because of the dominant discourse that makes breastfeeding a core test for good motherhood, breastfeeding mothers struggle against the conflicting expectations between this ‘good motherhood’ which is expected to be performed in private and what it means to be a ‘good worker’ in their (public) place of employment. In recent ‘netnographic’ research, Gatrell (2019; see also Lee, 2018) finds that breastfeeding women are deliberately made unwelcome in the workplace, as evidenced by colleagues ‘mooing’ at them as if they are cows, drinking their bottled breastmilk on a dare and without permission and explicitly stating that they are making other people uncomfortable. Even in ostensibly supportive workplaces, attempts to accommodate breastfeeding women are often lacklustre or insensitive, as evoked so well in van Amsterdam’s (2015) heartfelt account of breastfeeding as a teaching assistant and the multiple barriers and discomforts that attended it. The lack of support for breastfeeding makes it difficult for breastfeeding women, who as good workers face the contradictory expectations of being always on-call, working long hours and making personal sacrifices for the benefit of the organisation – all while being present for their children (Turner and Norwood, 2013: 400). It is therefore clear from research into the experiences of breastfeeding and breast-pumping women that they have negative experiences as well. On the other hand, as I have indicated above, not all experiences of formula feeding are happenstance or negative. It is the norm in many communities, often planned in advance, and mothers who engage in intended formula use may characterise their experience in positive terms. Regrettably, no matter what practices they adopt with respect to infant feeding, women can expect pushback. What seems clear is that the types of negative experiences are different depending upon one's method of infant feeding. As I will consider in my discussion of estrangement, all aspects of reproductive labour have the potential to be estranged. My focus in this article, however, is the role of shame/guilt specifically in the experience of estrangement of formula-feeding mothers who intended to breastfeed. I now turn to a consideration of this phenomenon.
Manion (2003) has distinguished guilt from shame, the former involving actions harming another and the latter involving failure to meet certain expectations (Locke, 2007: 149). As will become clear in the course of this article, mothers sometimes use the word ‘guilt’ and sometimes the word ‘shame’ to describe their feelings. Although I use the word shame for the sake of simplicity, there is likely much overlap between feelings of guilt and shame – they are not neatly fixed in lived experience. Certainly, the mothers who engaged in happenstance formula feeding felt that they were not living up to a notion of idealised motherhood conveyed to them by others. However, they had also been exposed to the message that formula feeding posed potential harms to the baby, making guilt a factor as well. Kukla (2006) has traced how campaigns which focus on formula's harm to the baby may play a role in this guilt-inducing process. There is often no singular or even specific source of this shame or guilt; it is rather amorphous – what Anne Drapkin Lyerly (2006: 111–115) has called ‘the culpable Other’ following Sandra Bartky's analysis that many women carry an imaginary internal audience which is subtly shaped by society's patriarchal values. Infant feeding provides fertile ground for experiencing shame because motherhood is highly scrutinised, from without (society in general) and from within (other mothers, and self). Dominant notions of good motherhood, such as ‘intensive mothering’ (Hays, 1996: 115) require of mothers great absorption and stoicism. They must visibly perform this absorption and self-sacrifice intensively and flawlessly in order to be seen to be good mothers. Yet, given trends in childrearing in which middle- and upper-class children's time is highly scheduled, and trends in the workplace which have demanded more time from employees in recent decades, the promise of perfect motherhood is a false one. Women are expected to be ‘all in’ as both mothers and paid workers, both of which are full-time tasks (Hays, 1996; Douglas and Michaels, 2004; Henderson et al., 2010: 233). As others have indicated, and as research participants in this study reaffirm, breastfeeding is one of the primary elements associated with being a good mother (Knaak, 2010: 349; Temple Newhook et al., 2013: 40).
Of course, as I discuss in further detail below, the expectations of intensive mothering are confronted differently by women depending, among other things, on their racialised identity and social class. Despite its prominent place in the line-up of good mothering practices, exclusive breastfeeding is actually not the global norm (Global Breastfeeding Collective, 2018). Instead, as Elizabeth Currid-Halkett argues with respect to other food products, like providing quinoa crackers and organic fruit in a child's lunch box, breastfeeding ‘has become a shorthand through which the new elite signal their cultural capital to one another’ (Currid-Halkett, 2017). Thus, for the well-educated, middle-class mothers in this study, who are among those most likely to internalise its message (Henderson et al., 2010: 234), one would expect idealised motherhood to have a powerful impact on their experience – a negative one if they feel they have failed to live up to it. Indeed, given a cultural context where most people tend to find meaning and validation in their paid employment or ‘work’ rather than at home (Hochschild, 1997), the opportunities for gaining validation and meaning within the largely invisible space of the home are few and far between. The intensive motherhood ideal is one area where the high value placed on a mother's role gives it a perilous weight, making it fraught. Estranged labour for the formula-feeding mother occurs in the space where the overvalued notion of breastfeeding as a labour of love meets the devalued role of the domestic labourer (Weeks, 2011: 124). Breastfeeding stands out from other forms of reproductive labour as a glittering gold nugget in the riverbed of undervalued work in the home and family. As such, for these middle-class mothers, there is a lot riding on getting that one golden aspect of reproductive labour ‘right’.
Finally, shame is ever-hovering around the issue of infant feeding because shame is a moral emotion, and ‘the situations about which women are most prone to feeling shame are those of a decidedly moral nature’ (Manion, 2003: 26). Parents certainly have a moral responsibility towards their children. Broadly conceived, this responsibility might be understood as having two parts: firstly, the imperative to do their best by their children by providing for their basic needs such as sustenance, shelter, clothing, stimulation and love/affection (i.e. so-called ‘positive’ rights); and secondly, to do this whilst not infringing upon the child's rights to such things as bodily integrity and personal security (so-called ‘negative’ rights). Of course, a parent's ability to meet these responsibilities can be severely circumscribed if institutional structures that empower and support parents are lacking. A parent's responsibility, then, particularly with respect to positive rights, can only extend as far as social and political structures allow it. Assuming a parent's good faith, due consideration must always be given to those constraints. As concerns infant feeding, the medically recognised gold standard as articulated by the World Health Organisation is exclusive breastfeeding for the first six months of a child's life, and extended breastfeeding as part of a child's diet to age two and beyond. As the presumed milk-producing entity, responsibility for fulfilling this benchmark for children's health and nutrition seems to fall squarely within the mother's sphere of responsibility. Indeed, some assert that mothers have a qualified ‘moral responsibility to breastfeed’ (Overall and Bernard, 2012).
Many breastfeeding advocates recognise the social and economic structures that can either inhibit or encourage breastfeeding, and the manifold reasons that women either choose not to, or cannot, breastfeed (e.g. Smith et al., 2012). Murphy et al. (1998), for instance, note that optimising a child's long-term health may not be the primary consideration in infant-feeding decisions. Competing, and compelling, considerations such as the interests of the family as a whole may lead to decisions that run counter to official prescription. Nevertheless, the failure, for whatever reason, to achieve the perceived gold standard is often felt as a personal failing by mothers who wanted to breastfeed. The potential benefits to be had from breastmilk must therefore be separated from an evaluation of individual mothers. As Woollard and Porter rightly insist, one can be ‘happy to recognise that the public health benefits of improved breastfeeding rates would be significant’ (2017: 517) without insisting that mothers have a duty to breastfeed. Instead, the ‘duty to help others can be multiply realised’ (Woollard and Porter, 2017: 516). Mothers have to assess for themselves how to fulfil the duty to benefit, and should be trusted to make this decision. In this absence of such trust, a sense of personal failure emerges and elicits shame. And when formula-feeding mothers experience shame in the course of their infant-feeding labour, the experience they describe appears analogous to Marx's fourfold notion of estranged labour, to which I turn below.
Ashamed formula feeding as estranged labour
In Estranged Labour (1844), Karl Marx laid out four ways in which waged workers are estranged, or alienated, under capitalism. Marx held that the working up of crude nature, ‘the sensuous, external world’ (Marx, 1997: 289), into something new is the path through which individuals realise their full humanity. He traced the process by which the life-giving, self-actualising behaviour of work (i.e. free, uncoerced labour) becomes a mere means of subsistence that strips the individual of humanity under capitalism and makes a person distinctly unfree. Specifically, waged labour, which is undertaken as a mere means to survival, estranges workers from nature; from the self; from their species-being; and from other individuals. Briefly, the worker is estranged from nature when the object of labour is given to the worker, who interacts with it only as a means of subsistence. Therefore, the worker has no relationship with what they have created. It is both determined by another and used by another. The waged worker is estranged from the self because waged labour requires the suppression of the worker's interests, curiosities and particularities. Instead, ‘the activity of the worker is not his own spontaneous activity. It belongs to another. It is the loss of his own self’ (Marx, 1997: 292). The worker is alienated from the species-being (that which differentiates humans from animals), in that human life activity is about will and consciousness, not bare necessity and instinct. Waged labour by contrast, distorts that life activity such that labour is only a ‘means to satisfy a need’ (Marx, 1997: 294). Finally, if the worker cannot recognise their own own self and humanity, it becomes impossible to recognise and make connections with others. In all of the aforementioned aspects of labour, the worker feels alien, not ‘at home’ as workers should feel if their labour were meaningful and fulfilling. This four-part scheme for analysing the loss of meaning in work can be helpfully applied to the labour of infant feeding when shame is involved, but first we must assert the reproductive labour of infant feeding as labour.
In making the argument that the Marxist notion of estrangement applies to formula-feeding mothers, I am making a broader point that all unwaged, reproductive work is subject to the possibility of estrangement. Those familiar with the concept will notice immediately that Marx himself did not apply this argument to unwaged work but to waged work, i.e. ‘labour’ or ‘social production’. My thesis is not therefore consistent with an orthodox adherence to Marx's vision, but to a Marxist feminist tradition which has for the past five decades convincingly insisted that Marx's analysis was incomplete, and that capitalism exploits unwaged reproductive work as much (indeed, perhaps more) as waged labour – the difference being that the former is naturalised and invisible. The Marxist feminist project has been described by Kathi Weeks and Nancy Hartsock as ‘reoccupying Marxism as feminism' (Hartsock, 1998: 401). This project uses Marxist methodologies and insights as tools, but adopts alternative standpoints (of the oppressed, exploited, and marginalized) to broaden the scope of Marx's analysis and overcome its limits (Hartsock, 1998: 401).
Marx held that all that was required to reproduce waged workers was their wage, which purchased necessary commodities (e.g. food and clothes) for consumption, thus ensuring the continued existence of the working classes daily and generationally (Seccombe, 1974: 14; Federici, 2013: 86). This account ignores the food preparation, mending, cleaning and washing that intervenes to make commodities consumable, and the caring labour involved in birthing and raising new generations of workers. In short, it ignores the ‘work that goes into preparing these commodities for consumption and the non-waged labour which is essential to reproducing the worker’ (Hartsock, 2004: 14–15). Without such foundational work, waged workers could not earn a wage. Federici points out that this oversight is partly explained by the fact that before 1870, capitalism's need for waged labour had so eroded the lives of workers, with virtually all family members engaged in waged labour, that very little reproductive work occurred, with life expectancy falling to twenty years of age as a result. Thus, Marx observed a social context in which reproductive work was severely and unsustainably eroded, which hampered his ability to theorise it adequately (Federici, 2013: 88). 3 Marxist feminist scholarship has filled in many of these gaps.
The ‘Wages for Housework’ movement beginning in the 1970s argued that capitalism relies on ‘a particular type of worker—and therefore a particular type of family, sexuality, procreation—and thus [Wages for Housework redefined] the private sphere as a sphere of relations of production and a terrain of anti-capitalist struggle’ (Federici, 2013: 90). One of the crucial insights of this movement, and within Marxist feminism more broadly, is that domestic work is every bit as unfree under capitalism as waged labour. Within the context of housework, labour is given, not freely chosen, and is undertaken as a means of subsistence (hence its famous status as a source of domestic conflict); personal interests and curiosities must be suppressed to ensure that domestic work is completed. Thus, distance from one's species-being and from others follows just as surely for the unwaged reproductive worker as for the waged worker. Moreover, the assumption that unwaged work within the home is women's task by nature and that it is always fulfilling has historically justified its unwaged status, and pre-empted rebellion against it (Federici, 2013: 92; Mies, 2014: 47). Marx's theory of estranged labour is fundamentally a theory that applies to unfree labour. In short, since ‘decades of feminist writing and campaigning have removed any doubt that producing human beings is work, and work that capitalism depends upon’ (Federici, 2014: xi), it is a consistent move to apply Marx's theory of alienation to unpaid reproductive work. This could include many forms of unpaid reproductive work, including breastfeeding.4,5 As I suggest here, however, because breastfeeding is consistent with dominant discourses of good motherhood, while it may be experienced as isolating, lonely, frustrating or depressing (among other things), it is less likely to evoke the kind of shame that produces the estrangement experienced by the well-educated and middle-class happenstance formula-feeding mothers in this study. To return to Hartsock's vision of reoccupying Marxism as feminism, consider this brief reflection she offered on the notion of estrangement (interchangeable with ‘alienation’) almost two decades ago: The concept of alienation has enabled a powerful account of the consequences of the separation of the worker from his labour power in both its form as activity and its form as product. Women are separated from their humanity in different and perhaps more thoroughgoing ways. Yet for women this is a contradictory situation, since at the same time as they are treated as commodities themselves, they are also involved in the provisioning of human needs outside the market. This situation could allow for a much more complex understanding of the concept of alienation (2004: 17; emphasis mine).
Feminist scholarship has taken up this challenge and moved past Marx's focus on physical, waged labour. In doing so, it has drawn upon the whole self, including thought and emotions in the context of labour, and thus opened the door to this more complex understanding of alienation/estrangement.
In her cultural analysis of reproduction, Emily Martin draws on the Marxist language of production and estrangement to unpack the operation of the industrial-age productivity metaphor at various scales. This includes medical textbooks which describe menstruation as ‘failed production’, and women's narratives about their own experience of childbirth which overwhelmingly depict labour as a passive, involuntary process and the resulting child[ren] as the product of their labours. She regrets that ‘we are still a long way from seeing quintessentially female functions as acts women do with body, mind, and emotional states working together or at least affecting one another’ (Martin, 1992: 89). Martin frames reproduction in terms of the inseparability of self and body. In her view, the production metaphor is what causes women to experience alienation, inviting them to see their bodies as machines and ignoring other facets of the self, including emotions and relations with other people (Martin, 1992: 19–20). The consequences of failing to account for all aspects of the self and to think only in terms of production are laid out strikingly when mothers describe their experiences of caesarean section by comparison to rape, assault and crucifixion, leaving many mothers feeling disconnected from their children and sometimes doubting the child is even theirs. ‘These women are putting into words a feeling of alienation between themselves and the event of a cesarean [sic] section, akin to the alienation of the laborer from his or her work, but beside which the separation of laborer and work pales’ (Martin, 1992: 84–85). This insistence on taking women's reproductive activities seriously as encompassing mind, body and emotional state is echoed in the work of Sara Ruddick, for whom motherhood is skilled and thoughtful if approached consciously, as ‘maternal thinking’. For Ruddick (2007), mothering (which, she clarifies, can be performed by anyone) entails preserving life, fostering growth and shaping acceptability with clear-sightedness, respect, responsibility and attentive love. The red thread running through these feminist theorisations of women's reproductive activities is the refusal to concede that these tasks are natural, automatic or unthinking. Because they are thoughtful and conscious activities, they can be estranged. Assuming these activities are natural and unthinking results from failing to account for all aspects of the self, including sexuality, love and emotions.
Even within the domain of paid labour, Arlie Russell Hochschild reveals that Marx's theory of labour does not account for all aspects of the self. Specifically, she points out that it is based on an outmoded mode of production, under which labourers sell primarily their physical labour. Marx's concept of productivity is somewhat crude in the sense that it only captures one relationship: the direct line between the physical work of the labourer and the wage received (a linear, this-for-that relationship). Not all lines are straight, however. Not all relationships are immediate. For her part, Hochschild (2012) focuses on the service industry, which has largely supplanted industrial labour, illustrating how a worker's ability to evoke and suppress certain emotions is integral to their ability to deliver their product: a service which is a pleasant experience for the customer. While the physical task of pushing a tray of snacks and drinks up and down the aisle or helping to load overhead lockers is certainly the flight attendant's labour, their attitude (friendliness, calm, reassurance) is far more important to the product they deliver (a pleasant flight) than their physical labour. Hochschild calls this work of evoking and suppressing emotions in return for a wage ‘emotional labour’. Like physical labour, it can be alienated.
Since it is often used inaccurately, the concept of ‘emotional labour’ requires clarification. Hochschild is clear that emotional ‘labour’ refers strictly to labour which is exchanged for a wage. It does not refer to unwaged reproductive labour, even though this work also involves evoking and suppressing emotions. When it is unwaged, Hochschild (2012) uses the terms ‘emotion work’ or ‘emotion management’. This distinction flags that the work performed for loved ones is different from a commodity, which is subject to the laws of supply and demand. That does not mean that it is unimportant or unproductive. It simply means that, unlike the wage, it is not a crude, mechanistic, linear exchange. It means that there are motives involved which are often mixed in with, but not the same as, the need for a wage or the imperative to stay alive. One of Hochschild's important contributions for the purposes of thinking about estrangement is that the possibility for estrangement does not hinge upon the wage. Although she does not say this specifically, the implication of her work is that the wage is simply one way that labour can become unfree. Hochschild signals that reproductive and immaterial emotion work is indeed work by describing it as ‘shifts’, alongside the paid-work shift. Contemporary women have the first shift, which is paid work, the second shift, which is home work, and the third shift: ‘noticing, understanding, and coping with the emotional consequences of the compressed second shift’ (Hochschild, 1997: 215). Therefore, one's work of emotion management in a private context can also be estranged. Estrangement is a lack of freedom and context. By attending to immaterial aspects of the self, we resist the assumption that they are natural. Seemingly natural human interactions between flight attendants and passengers, or between mother and child, are revealed as the product of effort and thought. Given its directionality, intentionality and effort (Hochschild, 2013: 27), this type of activity is work.
To summarise, feminist theories of production and reproduction make a compelling case for taking seriously the unpaid work historically performed, overwhelmingly, by women. By spelling out its contributions to the generation of surplus value, by demanding a wage, by refusing it outright, by speaking to its historical importance and by chronicling the thought, skill and effort it requires of mind, body and emotions, they have destabilised the false divide between production and reproduction and reclaimed reproductive work from the realm of the natural and automatic. This work widens the scope and potential for a Marxist theory of estrangement.
In recent years, this thread has been taken up more specifically with reference to breastfeeding. With concepts such as ‘breastwork’ and ‘breastspeak’, Alison Bartlett draws our attention to how the body registers knowledge corporeally. We can choose to acknowledge or to ignore corporeal signals; however, denying the body has consequences. For Bartlett (2005: 60–61) as a breastfeeding woman, her breasts are barometers of physical and mental health, becoming sore when she is overtaxing herself, and proceeding to stabbing pains if she does not rest. She frames breastfeeding as an embodied activity that includes cognitive thought: ‘Loosening the differences between mind and body means that our bodies are mindful and intelligent’ (Bartlett, 2005: 62). In her own way, Charlotte Faircloth's anthropological work on breastfeeding demonstrates that no form of child-rearing is ‘natural’ – it is all mediated by culture. There are myriad options when it comes to mothering styles, and mothers are expected to do their research, consider their options and seek expert guidance. In making choices about parenting, and carrying out the programmes they adopt, including infant feeding, mothers carry out ‘identity work’ (Faircloth, 2013: 17–18) which is much like a vocation (Faircloth, 2014: 26). Whether or not one is seen as a responsible and ‘good mother’ depends upon one's style of parenting, through which mothers signal who they are.
Returning to the notion of re-valuing reproductive labour, then, we acknowledge infant feeding is part of the reproductive labour of caring for a child. More specifically, the experience of nourishing a child from one's breast is often held up in terms that are analogous to fulfilling, self-actualising, ‘connected’ labour, while the experience of feeding an infant formula, given the shame that many mothers feel, by contrast, can be estranging. In what follows I will describe how formula-feeding mothers in this study conveyed their feelings of shame and disappointment in terms that follow Marx's framework of estranged labour: estrangement from nature, from self, from species-being and from other people.
Estrangement from nature: breastmilk as health food
In Marx's theory of estranged labour, workers are first estranged from nature, in that the object of their labour is given to them rather than freely chosen from the world around them and thus is unfree. Likewise, the happenstance formula-feeding mothers I spoke with reflected disappointment that their first ‘choice’ (breastfeeding) had not gone according to plan, necessitating formula use. They also seemed to fear that they were pursuing an ‘unnatural’ feeding method, or perhaps that others perceived their feeding choice as unnatural. Normatively loaded as ‘wrong’ because it ran contrary to public health prescriptions, their adoption of the perceived ‘unnatural’ behaviour weighed heavily on them. In short, they would have preferred to breastfeed, and the option left to them seemed to run contrary to nature – thus making it appear unfree and unnatural. Let us begin by considering the relative moral weight of breastmilk versus formula.
At least some, perhaps all, foods appear to be morally weighted. Indeed, in the current battle against overweight, individuals’ moral integrity is linked to their ability to take control of their weight (e.g. Inthorn and Boyce, 2010), and failure in this regard evokes shaming. Those foods deemed healthy according to various factors (natural; organic; pesticide-free; unsweetened; from-scratch; wholegrain) appear to lend their perceived positive qualities to those who consume them or feed them to children. Morally, formula is suspect. Every mother interviewed, regardless of how she fed her child, when asked about her perception of the benefits of breastfeeding, listed ‘natural’ as the chief benefit. 6 The moral rectitude of breastfeeding is sometimes expressed within a food idiom. Mothers, both formula feeding and breastfeeding, often associated breastmilk with holistic mothering, which appears as part and parcel of holistic health practices in general. Mothers sometimes refer to this kind of mothering using a food metaphor: ‘crunchiness’, a reference to granola, as in ‘crunchy granola’. For example, consider the following reflection from Kathleen, who wanted to breastfeed but found it physically impossible due to lack of milk supply: ‘I want this new tiny human to have the best that I could possibly provide … I never thought for two seconds I’d do anything else. I was very … a bit of a crunchy pregnant woman. I was really looking forward to breastfeeding’. Although Kathleen feeds her baby formula, a state of affairs that was dictated more by circumstances outside her control than by her choice, she makes clear that she is a responsible mother who feels that breast would have been the best option, if possible. She asserts her adherence to the philosophy of crunchy (natural) mothering, even though it proved impossible for her to breastfeed.
Another mother, Anne, for whom extended and exclusive breastfeeding was successful despite challenges of lip tie, conveys the sense that breastfeeding is a normalised behaviour in the health-conscious circles she frequents, while it may not be elsewhere: I had always really intended to breastfeed. Knowing that it's the healthiest choice … When a lot of the people you hang out with tend to eat organic, and you run into them at the organic supermarket … You find yourself in places where people are openly breastfeeding … and more likely to be there among those kind of ‘crunchy folk’ as I call them.
Anne's self-association with a healthy, organic community means that breastfeeding is a ‘no-brainer’ for her. Crunchiness evokes whole food instead of processed. It also invokes the image of the all-natural hippy. With the exception of eschewing vaccines, which is sometimes also associated with a hippy or alternative lifestyle, the hippy or crunchy mother, embracing holistic health, is an idealised model of mothering. Framing it in slightly different terms, Gwen, the breastfeeding mother of a seven-week-old baby, confirms that immersion in an earth mother, or ‘women's empowerment’, framework makes a woman more likely to breastfeed: ‘Perhaps … if you sort of prescribe to … this approach that tries to make birthing more of a woman's empowerment [thing] then yeah, if you’re sort of in that world, then I think that breastfeeding is the more natural option’.
It is worth noting that in trying to explain their reasons for breastfeeding, both Anne and Gwen refer to their social location – to ‘places’ or a ‘world’ where it is the norm, and therefore where it is expected of you, and you expect it of yourself. Indeed, if breastfeeding was not expected in the social stratum to which they belong, formula feeding would not be estranged because it would not be accompanied by a shameful feeling of failure to meet expectations. Racialised and classed expectations around idealised motherhood generally, and infant feeding specifically, are at play here. Women of all perceived races and social classes are affected by culturally dominant expectations around idealised motherhood. It is held up as a standard for all women. However, the ways in which it is marshalled against a particular group, and how members of that group respond to it, depend, among other things, on their race and class (Hill Collins, 2014; Newman and Henderson, 2014) and what is considered natural. For example, poor, racialised women have historically been expected to prioritise paid work over child-rearing, while white middle- and upper-class women have been expected to stay at home (Arendell, 1999: 4–5; Roberts, 1999: 15). Newman and Henderson note that even mothers who reject culturally dominant ideologies of idealised motherhood and who are from backgrounds that cannot sustain it respond to it as the dominant ideal (2014: 474). They do so by constructing ‘deviancy discourses’ (Arendell, 1999) about their mothering. Patricia Hill Collins describes a culturally specific alternative mothering discourse when she develops the concept of ‘othermothering’ as a practice with deep roots among working-class African-American women in the US: ‘women who “catch” legal husbands, who live in single-family homes, who can afford private school and music lessons for their children, are deemed better mothers than those who do not. In this context, those African-American women who continue community-based child care challenge one fundamental assumption underlying the capitalist system’ (2014: 182). To be sure, each economic class, racialised identity and sub-culture may have its own particular ideals to contend with (Hill Collins, for example, describes the problematic image of the ‘strong Black mother’). Since intensive motherhood ideology is typically connected to white, heterosexual and middle class ideals. (Arendell, 2000: 1201), it is unsurprising that self-surveillance, resulting from internalisation of the intensive motherhood ideal, is common among middle- and upper-class women (Henderson et al., 2010: 234). Therefore, just as not all workers under capitalism feel frustrated or outside themselves, formula feeding is not inherently estranging. One's social location, which predisposes one to either resist or absorb any particular discourse of good motherhood, determines whether or not one will experience estrangement.
To the white middle-class mothers in this study, nursing an infant seems so ‘all natural’ that a woman's ability or inability to approximate the image of mother with baby at her breast appears to play a significant role in a woman's pride/satisfaction in, or shame about, her mothering practice in the early months of a child's life. That is, because holistic, all-natural mothering is presented as ideal mothering, those mothers who best approximate the ideal appear to have the higher moral ground over mothers who provide formula to their children. By contrast, mothers who use formula feel outside of ideal mothering, and severed not only from the natural choice but from their social class – a fact which, as we shall see below, they find deeply disturbing and shameful. The word ‘poison’ was used by several of the mothers with reference to formula, even if they were defending it against that charge, as in ‘I mean, it's not poison!’. The negative moral weight of formula appears to feel far greater than the positive moral weight of breastmilk. 7 This bears out Knaak's observation that mothers she interviewed did not simply prefer breastmilk but viewed formula in a negative light, associating the former with good mothering and the latter with bad mothering (Knaak, 2010: 349). Indeed, the weight of formula is so ponderous that it appears to nearly cancel out the presence of breastmilk for mothers who mix-feed (formula and breastmilk) or who switched away from breastmilk to formula. I expand upon this dynamic by turning now to formula shame's role in mothers’ perceived estrangement from themselves and from their species-being.
Estrangement from self and from species-being: ‘I couldn’t do it’
Breastfeeding's ‘natural’ status, addressed above, and the injunction to breastfeed that women encounter in pregnancy and childrearing manuals, childbirth preparation classes, mother/baby clubs, online forums and in the obstetrical context, led each of the women who participated in this research to desire breastfeeding. They saw it as the best option, and what they should do. However, once their baby arrived, they encountered a number of barriers to breastfeeding which caused a great deal of internal conflict, as the new information and feelings that came with the reality of breastfeeding led them into conflict with their belief in breastfeeding or intention to breastfeed. The conflict between desire to breastfeed, or the preponderance of advice to breastfeed, and a woman's need to incorporate formula led in many cases to an initial mistrust of herself and her judgments. In this sense, like the estranged waged worker who feels outside herself at work, the happenstance formula-feeding mothers experienced self-doubt instead of confidence, and a lack of feeling expertise in their mothering. Instead of feeling fulfilled, they felt frustrated.
Jane shares an excellent example of this dynamic. Jane had a caesarean section and several health complications after birth, and a child who nursed with great difficulty and remained hungry. Jane was counselled by a lactation consultant to ‘top up’ with formula while her milk supply was being established, so that her baby would be satisfied. Jane was adamant that she should nurse her child. She cited the health benefits, primarily enhanced immunity from illness, that breastmilk provides. She had also prepared herself prior to giving birth by doing research on breastfeeding, and knew that challenges were likely to present themselves in the early weeks. Consequently, when she noticed that her baby struggled even getting her lip around the nipple of a bottle, she raised the possibility of lip tie with health professionals, who took no decisive action to address that possibility. She was repeatedly told that everything was ‘normal’ and she felt ignored by medical professionals. To add to this conflict between Jane's sense that her baby needed assistance in establishing successful breastfeeding and the lack of support she received, she had been admonished by a doctor at the hospital, and in front of several medical students, that she should not be using formula because for each ounce of formula baby received, the baby was missing one ounce of mother's milk: ‘I had a paediatrician come in and give me a lecture about it … She had about six students there with her and it was just me, and they were all staring at me. And I got a lecture … because I was giving her formula’. This was a shaming experience, as evidenced by Jane's keen awareness of being outnumbered, and of the students’ gaze upon her as she was reprimanded. Jane's assessment of the situation was that her baby might need a medical intervention for lip tie, which was not forthcoming. After over a week, her baby had not gained sufficient weight, and Jane switched to formula after twelve days. Reflecting afterwards, Jane feels that she knew, given all these factors, that breastfeeding was not working for her, although she would have liked help in making it work. However, the fraught status of formula as opposed to breastmilk caused her to doubt herself and even to ignore her own instincts: [My mom] was watching me ignore my own instincts. Like, I really was ignoring. ‘Cause I was listening to everyone say ‘everything is normal, this is all fine. You can’t top up with formula ‘cause if you top up with formula your milk won’t come in’. And I was adamant that I wanted to do it [breastfeed]. And to the point that I wasn’t recognising that [my baby] was really hungry … I was ignoring my instincts, my motherly instincts. It was bad. And my mom could see it.
Jane's knowledge that breast is best and her memory of the doctor's admonishment made the decision to incorporate formula appear as a failure that she was initially unwilling to consider. It is easy to see how the inability to make breastfeeding work successfully could appear as a personal failure to give her relationship with her baby everything it deserved. As previous work has shown, women's shame at failing to maintain relationships (here the breastfeeding relationship) stems in part from internalising the failure as their own and blaming themselves, rather than noting how conditions (sometimes inevitable), and other people's behaviours, played a role in inhibiting their efforts (Manion, 2003: 24). Shame intervened in Jane's work as a mother to make her feel outside herself, to doubt her knowledge and capacity to accurately assess the situation and to act accordingly.
The shame evoked by formula use not only causes the mothers to doubt themselves, to ignore their instincts and thus to feel outside of themselves in their work as mothers. It also estranges them from their perception of their species-being – in this case, as women and mothers. As noted above, the model mother is both capable of physically nourishing her infant from the breast and willing to do so. Moreover, she finds enjoyment and fulfilment in this labour of love. However, when mothers feel shame over their use of formula, they feel inadequate and hence exiled from the institution of motherhood. Any breastmilk is beneficial to a baby who is receiving it. And yet, mothers who mix-feed their children report having great difficulty thinking of themselves as breastfeeding mothers, despite the fact that their child has benefitted from breastmilk. They have somehow failed to earn the ‘badge of honour’ that belongs to exclusively breastfeeding women.
Sally is mother to an infant who was mix-fed until four months of age, at which point she switched to exclusive formula feeding. Like many other formula-feeding mothers, Sally undertook formidable efforts to make breastfeeding work. Due to a serious and long-lasting health complication after birth, Sally was unwell, required frequent medical attention and had low milk supply. Through these difficulties, and although she was ‘crying all the time’, Sally always made the commitment to breastfeed. However, the presence of formula as the processed, ‘unnatural’ choice led her to feel that her breastfeeding somehow did not count, and diminished her pride in her maternal labour and in her motherhood generally: ‘I would literally be breastfeeding and crying ‘cause I couldn’t breastfeed … I was looking at what I couldn’t do. ‘Cause I guess I figured like, you’re a woman, and you should be – your body's put together to be able to do these things. And I couldn’t do it’. Sally had a strong feeling of failure, even though each medical professional she encountered confirmed the need to supplement baby with formula. Even when engaged in the act of breastfeeding, her attention was captivated by the negative moral weight of the formula, which negated the presence of her own beneficial breastmilk. In her all-or-nothing framework, she had not fulfilled her role as a woman and mother. In addition to concerns about formula itself, Sally's comments also indicate an association between women's bodies and reproduction (I have breasts, therefore I should lactate and breastfeed successfully) that lead us back to the image of the all-natural breastfeeding mother, for whom breastfeeding comes naturally (emotionally and physically), and who does not need assistance or supplementation (adulteration). Sally's shame stems from her sense that she failed to meet the high expectations of exclusively breastfeeding a child, even knowing that she has faced exceptional circumstances and still provided a rather remarkable four months’ worth of her own milk. She has a deep internal conflict between her assessment of her situation, which accepts that her child required formula, and her notion that physically and morally, breastfeeding is what mothers do.
Sometimes conflicted feelings about a woman's motherhood role are more ambivalent. Penny, who had fairly positive feelings about formula, exclusively breastfed to four months, when she gradually switched to formula upon her return to waged work. For her, using formula was intended, and part of what she describes as an ‘equitable’ relationship with her partner. Since he stayed at home to care for their child, she wanted to help him upon her arrival home, rather than sitting down to breastfeed. Also, she did not particularly enjoy breastfeeding: ‘it wasn’t really a personal experience. It was more of a job’. Yet even for Penny, whose experience seemed to me notably empowered, she remembers sensing negative reactions from medical staff when she switched to formula, and that the pressure to conform to ideals of good motherhood did upset her. When her sister discussed her own love of breastfeeding, Penny found it difficult ‘because I wasn’t fitting in the stereotypical role’. This notion that breastfeeding is the only acceptable infant-feeding behaviour among mothers causes a rift between the woman and dominant notions of motherhood, and even womanhood – thus, her species-being. It also estranges her from other women, a subject to which I turn next.
Estrangement from others: ‘I was afraid to take out a bottle of formula’
Marx tells us that if people are estranged from themselves and their species-being, then they will inevitably be estranged from other individuals. When formula-feeding mothers feel shame, their sense of self is sufficiently disrupted to interfere with engagement with others. Mothers who participated in this research reported feeling ashamed in public, and unable to speak with their friends about infant feeding. They are aware that many people disapprove of formula, and therefore are unwilling to expose themselves to the potential criticism of that which is so important to them – their motherhood – should they pull out a bottle of formula in public. Shame therefore seems to be something that formula-feeding mothers in this research experience primarily when they leave their homes, among members of their social class. This speaks to judgment by others as the other side of shame. Kathleen, the sole member of her group of friends with children to use formula, who had previously understood herself as ‘crunchy’, describes this well: I felt a lot of shame initially about formula feeding. To the point where I would feel guilty taking out a bottle at playgroup cause everyone else was latching their babies. And I was like, okay well here's my [bottle] with [formula] in it and, you know, so that was initially very sad. And the first couple of times I went to buy formula was extremely difficult to the point where my husband bought it instead, for the first little while.
Charlotte provides context for the more explicit fear of judgment and consequent shame that she perceives. Remembering that her family physician and gynaecologist gave her many cues to breastfeed while never discussing formula, and ‘very, very judgy moms’ at her weekly mother-baby group, she notes that she was primed for a feeling of failure: When it didn’t work out – and I mean, we really tried our best – it felt like a failure. I felt like, yeah, I failed to do this. This was best for your baby. Right? And all these people told you that you should breastfeed and you failed at doing that. So now you feel guilty because you couldn’t do it and you couldn’t give your baby the best. And it takes a long time to get over that.
In Charlotte's case, she links this sense of failure, the difficulty of discussing the challenges of being a formula-feeding mother ‘in mixed company’ (i.e. in front of breastfeeding mothers) and the lack of support or services for formula-feeding mothers to her eventual diagnosis of post-partum depression. Elodie, a breastfeeding mother, confirms this separation between formula- and breastfeeding mothers, noting that infant feeding is something of a taboo in ‘mixed company’: ‘With friends who didn’t [breastfeed], I don’t bring it up. And they don’t talk about it. And I’ll be sitting there breastfeeding, talking to them, and we don’t discuss it … it's kind of sad’.
This separation from other mothers extends to health services for new mothers. Indeed, all formula-feeding mothers in this study noted that they felt excluded from support services due to their use of formula. This reportedly took the form of having no post-partum follow-up once they switched to formula, feeling unwelcome at the local baby weigh-in clinics, dubbed ‘breastfeeding support’ groups and difficulty acquiring required knowledge about formula (e.g. whether and when to use powder vs. liquid, how to sterilise equipment, how long formula can remain in the fridge before being discarded, etc). Elaine, for example, notes that she felt that once she stopped breastfeeding at two months, her file was closed, precluding any further help: ‘[my health care provider] told me that she was closing my file. Hers [the baby's] was open. But mine was closed’. Leah, who turned to formula after disliking breastfeeding, echoes this, noting her sense of confusion: ‘You don’t know where to go, like, you don’t know what you’re doing’. The blanket silence about formula, a good faith effort to promote breastfeeding where rates are among the lowest in Canada has the unintended consequence of isolating formula-feeding mothers, putting infants at risk and increasing mothers’ feelings of incompetence (and thus estrangement) because they do not have adequate information. When a nurse told Kathleen, who was doing everything she could think of to make breastfeeding work, ‘you can still try harder’, she recalls: ‘that will stay with me forever. I sat in the parking lot with my daughter in the back seat and I just cried and cried and cried and cried’.
Hopeful notes
It seems clear from speaking with formula-feeding mothers that being judged an inadequate mother by others is shame-inducing. However, the shame that accompanies the experience of formula feeding also grows out of a conflict between what the mothers themselves accept about the benefits of breastmilk, and the fact that they nonetheless ultimately ended up incorporating formula. They believe that mothers should breastfeed, but find themselves in circumstances where exclusive breastfeeding does not appear possible. This conflict causes a rupture between their internalised ideals of motherhood and the reality of their own, personalised style of mothering. That is to say that they also stand in judgment of themselves. I would like to briefly return to the idea of a parent's moral responsibility towards their child to do their best to provide necessities, and not to infringe on their rights, given their resources.
If breastmilk is the gold standard for infant nutrition and health, then use of formula looms as a potentially significant moral failing for mothers who use it. However, mothers seem to begin to overcome this feeling when they resolve their internal conflict. This seems to take both time and dialogue. Over the course of participating in an interview, each mother constructed a timeline and a narrative to understand why she did not breastfeed. The clarity and precision of these narratives suggest that women have put a lot of time into thinking about breastfeeding, and into understanding why it did not work for them and why formula became part of their infant-feeding strategy. In most cases, their reasons included significant lack of the necessary support that would have made their breastfeeding goal possible for them. In such cases, the process of constructing what Bartlett calls their ‘corporeography’, or ‘storying’ their experiences, allowed them to construct alternative accounts to the medicalised discourses they had received (Bartlett, 2005: 63). Several women told me after they had been interviewed that they found it helpful to tell their story. Developing their own corporeography aided women in accepting the sequence of events that led to incorporating formula. It was part of a process of overcoming their estrangement and challenging abstract notions of duty – or idealised mothering.
Finally, it is worth recalling Manion’s (2003: 21) description of shame as involving a painful, sudden awareness of the self as less good than hoped for and expected, precipitated by the identification by others (imaginary or real), or simply by the ashamed self, of a seemingly significant character shortcoming. Ashamed formula-feeding mothers were able to identify numerous sources of shaming. However, given the combative tone of much of the work on ‘mommy wars’ and the often-pejorative use of the term ‘lactivism’ to describe breastfeeding promotion, it is more than worthwhile noting that most breastfeeding mothers in this study conveyed support and solidarity with their formula-feeding peers. Breastfeeding mothers made positive statements about formula-feeding mothers, such as Elodie, who says: ‘If they choose not to [breastfeed], I think they should be supported’. Most breastfeeding mothers also, when asked what else my breastfeeding research should address, indicated that more research on the needs of formula-feeding mothers was desirable.
This article has offered an empathic and descriptive account of some struggles faced by formula-feeding mothers. This fills a gap in the literature on infant-feeding experiences, which focuses overwhelmingly on breastfeeding. It shows that the reproductive labour of breast- and formula-feeding mothers is often stigmatised and rendered invisible. However, the fact that breastfeeding is part of culturally dominant notions of good motherhood means that formula-feeding mothers, especially of the middle classes most likely to internalise this notion of motherhood, experience estrangement. Just like estranged workers under capitalism, who engage in a grotesque and unfulfilling ‘going through the motions’ of labour with little or no promise of fulfilment, so mothers under ideals of intensive motherhood reflect on their sometimes joyless pantomime of motherhood. Rather than being self-directed, creative and ‘fun’ (a word that did not appear in my interactions with these moms), the pressure to deliver the very best in every respect, in accordance with culturally dominant ideals of motherhood, distorted their experience. In her work on emotional labour and emotion management, Hochschild notes that feelings of failure in one's tasks, and feeling that they are not fulfilling, are a sign of a ‘broken care system’ (2013: 28). The many controlling images of motherhood, of which the sanctified breastfeeding mother is one, contributes to such a broken care system, leading to estrangement. Acknowledging and naming this broken system is a step towards inclusive programmes for mothers which do not stream mothers into ‘formula feeding’ and ‘breastfeeding’, and encouraging mothers to see themselves as collectively resisting controlling images of motherhood, rather than being sorted into antagonistic groups by them.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.