
Abstract
In this paper, we analysed Dutch and British radio phone-in conversations on ADHD and vaccination between radio hosts and callers, focusing on how interactants dispute the authority of both scientific and experiential claims to expertise. We found that interactants never challenged the authority of science and experience as such, but resisted their normative relevance. When callers offered expertise in the form of personal experience, hosts challenged its relevance for the overhearing audience by treating the experience as mere belief. When callers offered expertise in the form of scientific knowledge, hosts carefully patrolled the boundaries of ‘real’ science and who may speak for it. We discuss how our findings can explain the frequent contestation of factual sources in semi-public exchanges and offer a new perspective on the supposed diminished authority of scientific knowledge.
Keywords
Introduction
The perceived lack of respect for truth in general, and certified or scientific expertise in particular, has become an important topic of debate in recent years (Kakutani, 2018; Nichols, 2017; Nurse, 2011). Within the context of an alleged ‘post-truth society’ (Harsin, 2018), it is often claimed that the authority or perceived credibility of personal experience has grown at the expense of trust in certified expertise (Nelson et al., 2023). Certain narratives seem to be able ‘to inoculate themselves against criticism, precisely by emerging as the voice of authentic experience, an experience that cannot be denied, without violating the integrity of the narrator’ (Gabriel, 2004: 177). Such an ‘i-pistemology’ (van Zoonen, 2012) could challenge the authority of certified expert knowledge (Breeze, 2021; Popay and Williams, 2006: 123; cf. Collins and Evans, 2002). Other authors, however, point to a more complex interaction of knowledge claims. For instance, drawing on interviews with mothers who refused one or more vaccines, Carrion (2018) observes that these individuals, often perceived as ‘anti-scientific’, draw on an ideal of science while criticising existing research for failing to meet its standards (cf. Versteeg, 2018). This raises the question of what interactants actually do when claiming authoritative knowledge based on either personal experience or scientific, certified expertise.
Given the complexity of contemporary society, reliance on the certified expertise of others is unavoidable for any given individual (Moore, 2021; Warren, 1996). At the same time, and perhaps because of this tremendous importance of expertise, struggles about what constitutes credible expertise keep erupting. These struggles are not equally divided over scientific fields, or, as Shapin puts this eloquently: whereas ‘particle physics is hard to understand and often counter-commonsensical, this is not a problem for the laity’, because it ‘is not an expert practice that they care much about, and they simply let the experts “get on with it”’ (Shapin, 2007: 174). But it becomes a different matter when claims of expertise touch on topics pertinent to everyday life, such as diet, child rearing, climate change, vaccination, or corona policy measures (e.g. Prettner et al., 2023; van Burgsteden and te Molder, 2021; Veen et al., 2012).
Within the social sciences, it has long been established that whether one is recognised as an expert and treated as such by others, is never a given. Expertise has been described as an entitlement to speak (Myers, 2004: 177), a claim that interactants will evaluate moment-by-moment. Within the field of conversation analysis specifically, researchers have shown that participants actively manage and display their knowledge relative to others, defining and policing their own epistemic boundaries (e.g. Bolden, 2013; Heritage, 2011, 2012; Raymond and Heritage, 2006). Researchers have thereby argued that the ‘epistemic domain is morally ordered’ (Stivers et al., 2011: 3): People can and do hold each other accountable for properly fulfilling their obligations and asserting their rights to knowledge.
In a similar vein, conversation analysts have shown that the experiential domain is morally ordered: people in interaction locate personal experience firmly within the epistemic domain of the speaker who owns it (Heritage, 2011; Pomerantz, 1980; Sacks, 1984). Since interactants can claim the primary rights to their own thoughts and experience, recipients will need to avoid the twin risks of appearing either disengaged from the affairs of the other, or appearing over-involved with, and even appropriating such experience (Raymond and Heritage, 2006: 701). For instance, when speakers display empathy, they need to show proof of their understanding of the other’s experience (avoid appearing disengaged), while being careful that this proof does not overshadow the story of the other’s experience (avoid appropriation; Heritage, 2011). Yet, starting from the field of science communication, the question remains whether experience is indeed impossible to challenge and whether certified expertise is perhaps easier to dispute, as the abovementioned observations by Gabriel (2004) suggest.
To answer that question, we have used conversation analysis (CA), an empirical approach to examining social interaction. CA research on how people deal with claims of certified or experiential expertise offers an alternative approach to established methods of examining expertise (e.g. interviews or surveys) by examining what people do when making claims of expertise in everyday talk. For this purpose, we have compared conversations from a corpus of radio phone-ins. The radio phone-in is an ‘extreme case’: its format is biased towards personal experience, as this is what callers are invited to contribute (Hutchby, 2001). Within this format, the description of expertise as an entitlement to speak (Myers, 2004) holds literally true: participants must demonstrate the relevance of their contribution to be allowed airtime. Claiming personal experience or certified, scientific expertise are two ways to achieve this. In the current study, we focus on the interactional positioning and evaluation of personal experience relative to that of claims to scientific expertise.
The radio phone-in as ‘extreme case’
The radio phone-in is a specific, highly regulated context, making it interesting as an ‘extreme case’ to learn more about how interactants evaluate claims based on scientific expertise or personal experience. Most importantly, the format of the phone-in elicits callers’ experiences, but the hosts are typically in pursuit of controversy (Hutchby, 1992). As such, they challenge experiences that are not theirs and make claims to science that they are often unable – and not necessarily willing – to judge.
Callers contribute to a radio phone-in by offering their first-hand knowledge or non-polished opinion (e.g. Fitzgerald and Housley, 2002; Hutchby, 2001; Thornborrow, 2001b). A radio phone-in provides ‘one of very few regular environments in which ordinary members of the public are given the opportunity to speak on issues and events in their own voices’ (Hutchby, 2001: 481). Radio phone-in hosts frequently position themselves as the representative of the overhearing audience. At the same time, the radio phone-in provides an environment in which nobody ever changes their mind (Myers, 2004: 195). In this respect, they present a microcosm of societal controversies, in which people rarely show that they have changed their initially displayed opinion (e.g. Nyhan et al., 2014).
The offering of experience constitutes a regular first turn in a radio phone-in. Callers are highly aware of the need to gain airtime and will therefore actively work to present themselves as ‘authentic’, ‘relevant’, and ‘in-depth’ (Fitzgerald and Housley, 2002; Hutchby, 2001; Thornborrow, 2001a). For instance, in one of the radio phone-ins analysed in this paper, a caller validates his call by saying that he is not a scientist but has an ordinary technical education. This introduction contrasts the identity he draws on with those of the invited experts who were speaking earlier. Presenting himself as ‘not a scientist’, this caller strengthens his right to speak as one of the ‘ordinary people’, in other words, as the voice of common sense. Hutchby (2001) has shown that this is not without danger, suggesting that ‘the limits of the caller’s witnessing can be interactionally managed’ (Hutchby, 2001: 492; italics in original).
Our analysis compares how recipients evaluate personal experience versus scientific expertise. We show that, whereas radio phone-in hosts typically respect the caller’s epistemic primacy regarding their own experience, they can resist the relevance of this experience. By singling out the caller as a naive individual and treating the experience as mere belief, they demonstrate their own epistemic vigilance (Sperber et al., 2010). In contrast, when a caller offers a claim based on the language of scientific expertise, this is not treated as belief or merely an opinion. Rather than challenging the relevance of scientific expertise as such, the host questions the speaker’s right to act as its spokesperson. Both caller and host thus protect the status of science by carefully policing both the entitlement to speak for it, and the ensuing responsibilities.
Data and method
Data selection
To pursue these questions in an exploratory way, we analyse one Dutch and two British broadcasts (total duration: 107 minutes), focusing on the flu shot and ADHD, respectively. The excerpts have been broadcast by Dutch national radio (Radio 1), the London-based LBC 97.3 and BBC5. Although the flu shot and ADHD are distinctly different health topics, they are both the subject of heated societal controversy and, in the analysed excerpts, both topics are framed in such a way as to invite the listeners to judge their ‘realness’. The listeners in the Dutch radio phone-in can have their say about whether the flu shot is beneficial after host Joost Eerdmans has interviewed an invited General Practitioner who does not think so. The host’s statement to which listeners can react is that ‘the flu shot only helps the pharmaceutical industry’. The British host James O’Brien starts his LBC 97.3 broadcast with the statement, based on a book written by a former NHS psychotherapist, that ‘millions of us, including children, are wrongly labelled with psychiatric problems’ and suggests that ‘a lot of children in this country who have been diagnosed with attention deficit hyperactivity disorder do not have a medical condition whatsoever’. Again, listeners are invited to confirm or – more likely – contradict the expertise of certified health professionals. Finally, in a reversal of events, the BBC Broadcast first features a guest discussing the ADHD she and her son experience, followed by an expert offering his opinion on whether ADHD is a medical condition. All broadcasts in the dataset are contentious, with hosts defending a specific storyline and challenging callers who disagree, rather than remaining neutral.
Analytic procedure
The radio phone-ins were initially transcribed verbatim. Selected fragments were then transcribed in more detail using Jefferson’s (2004) system. The original audio material can be found online 1 or requested from the authors. The analysis followed CA’s guiding principle that participants use the turn-by-turn development of conversations to understand the social actions being accomplished (e.g. accusing, complimenting, questioning). These publicly displayed and continuously updated understandings of what is being said and done are an important ‘proof procedure’ for the analyst: Every turn in a conversation demonstrates the speaker’s understanding of the prior turn, making this understanding available for analysis (Sacks et al., 1974). The analysis remains agnostic regarding the truthfulness of what participants claim to know or to have personally experienced. Instead, it focuses on what participants achieve in the interaction by claiming particular knowledge.
While listening to the phone-ins, explicit disputes between hosts and callers concerning what counts as relevant and/or valid knowledge drew our attention. The recordings and transcripts were examined to look for situations where callers disagreed with the host, offering claims to either scientific or experiential knowledge. We took an iterative analytical approach, conducting multiple rounds of analysis to examine individual instances while also considering their shared characteristics.
For this paper, Dutch data have been translated into English by adhering as closely as possible to the original wording, while ensuring that readers can follow the analysis as it was conducted by the authors based on the Dutch text. The original Dutch data are available from the authors upon request.
Analytic results
In what follows, we will show how interactants negotiate the value of personal experience (4.1) and scientific expertise (4.2). The excerpts presented in paragraph 4.1 show how the host challenges what has been offered as personal experience, without trespassing on the epistemic domain of the caller. Rather than disputing the experience as such, the host treats it as mere belief, hence not relevant to the overhearing audience. The excerpts presented in paragraph 4.2 show how both callers and host carefully patrol the borders of what constitutes ‘real’ scientific expertise and who is allowed to speak for it.
Resisting the prescriptive relevance of experience: Treating it as belief
The following excerpt, a fragment from a Dutch radio phone-in about the flu shot, serves as a first and comparatively simple example of (a) how callers try to build a strong claim on based of personal experience and (b) how the relevance thereof can nevertheless be disputed by the host.
We join the participants when the host mentions ‘extensive research of a leading journal’ (lines 1–2), which, according to the host, shows that the flu shot will prevent people from getting the flu is ‘real nonsense’ (line 5). The host refers to his own position by indicating that ‘that’s what he will stick to’ (line 7). By introducing the next caller as someone who disagrees with him (line 8), the host not only establishes a tone of conflict for the upcoming conversation but also implicitly portrays the caller’s stance as irrational, as it dismisses the purportedly thorough research from the leading journal. The caller begins the conversation by stating that he started getting the flu shot after turning 65 and has not had the flu since then (omitted from transcript). He then emphasises his willingness to pay for the flu shot himself if it were not reimbursed and highlights how he has personally benefited from it (lines 19–22):
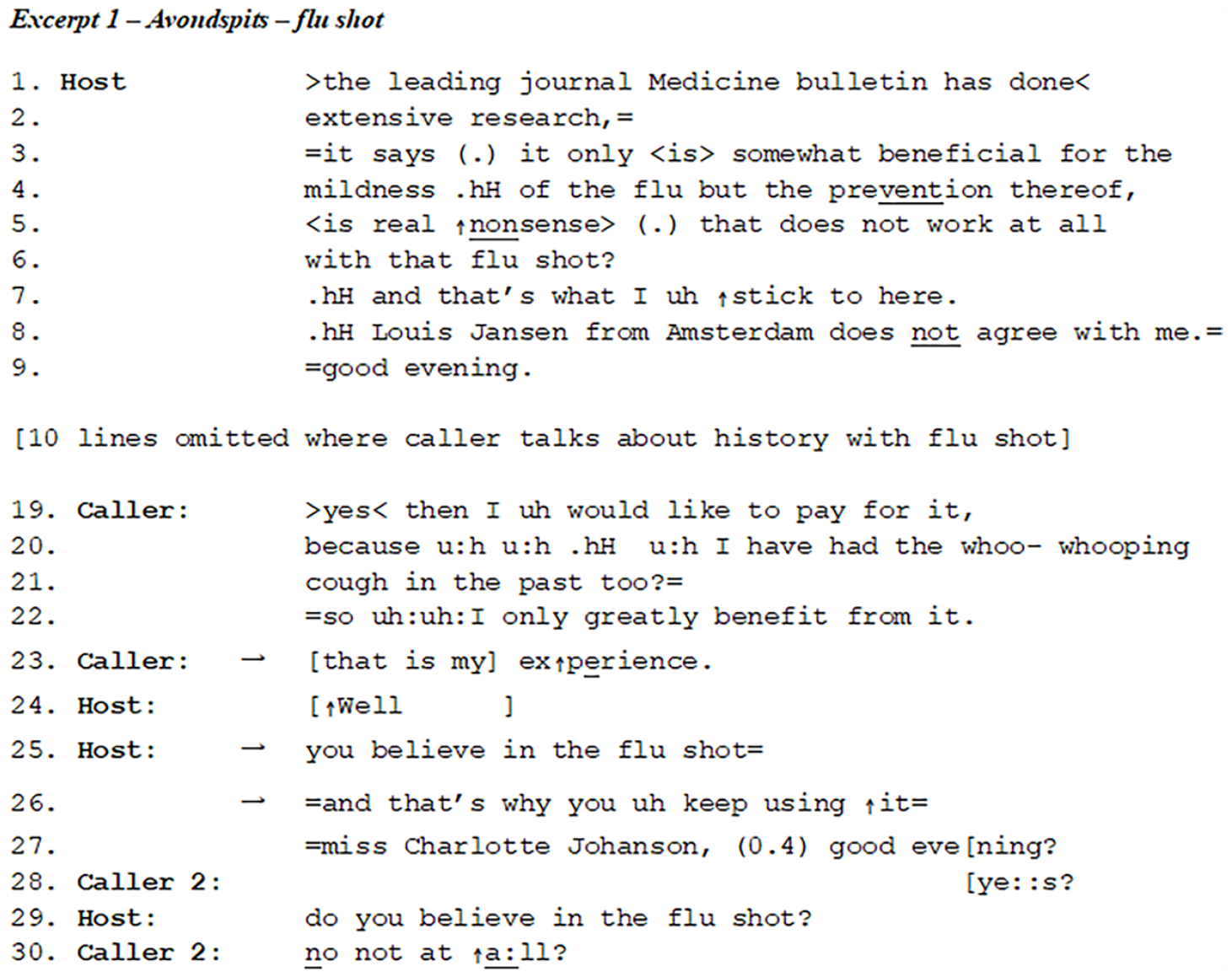
The caller uses ‘so’-prefacing (line 22) in producing the upshot of his talk, marking this as the final unit in his turn (Raymond, 2004), which is reinforced by the turn-final intonation. The host also treats it as such by starting to formulate what has been said, using the preface ‘well’ (line 24). This is a known ‘alert that the turn it prefaces will privilege its speaker’s perspectives, interests or project relative to the expectations for action established in the prior turn or sequence’ (Heritage, 2015: 88). While marking his turn as complete in line 22, the caller adds, in overlap with the host, that the beneficial workings of the flu shot are his ‘exp
Generally, within phone-ins, one of the host’s category entitlements is to conclusively formulate the opinion of the caller before proceeding to the next topic (Fitzgerald and Housley, 2002), a right that reflects the asymmetrical organisation of phone-ins (Edwards, 1997: 127). This is also what we see happening in Excerpt 1. The host uses his final formulation to dismiss the caller’s experience as merely a consequence of his belief in the flu shot (lines 25–26). In this way, he avoids disputing the experience itself, but he does cast doubt on the caller’s credibility as an observer of this experience, singling him out as an irrational individual, a believer. Treating the caller as a believer allows the host to resist the prescriptive implications of the caller’s positive experience with the flu shot, and thus to remain in control of the overarching narrative of the show. The next caller’s defensive extreme case formulation ‘
The next excerpt, again discussing the flu shot, provides another instance where the host dismisses the relevance of a caller’s offered experience. Again, it is not the experience itself that is directly contested. Instead, much like in the previous segment, the host questions the caller’s credibility as a reliable observer of her own experience – thereby undermining the relevance of her account for the listening audience. The excerpt starts with the caller describing her personal experience. The caller’s extreme case formulation (‘I have n
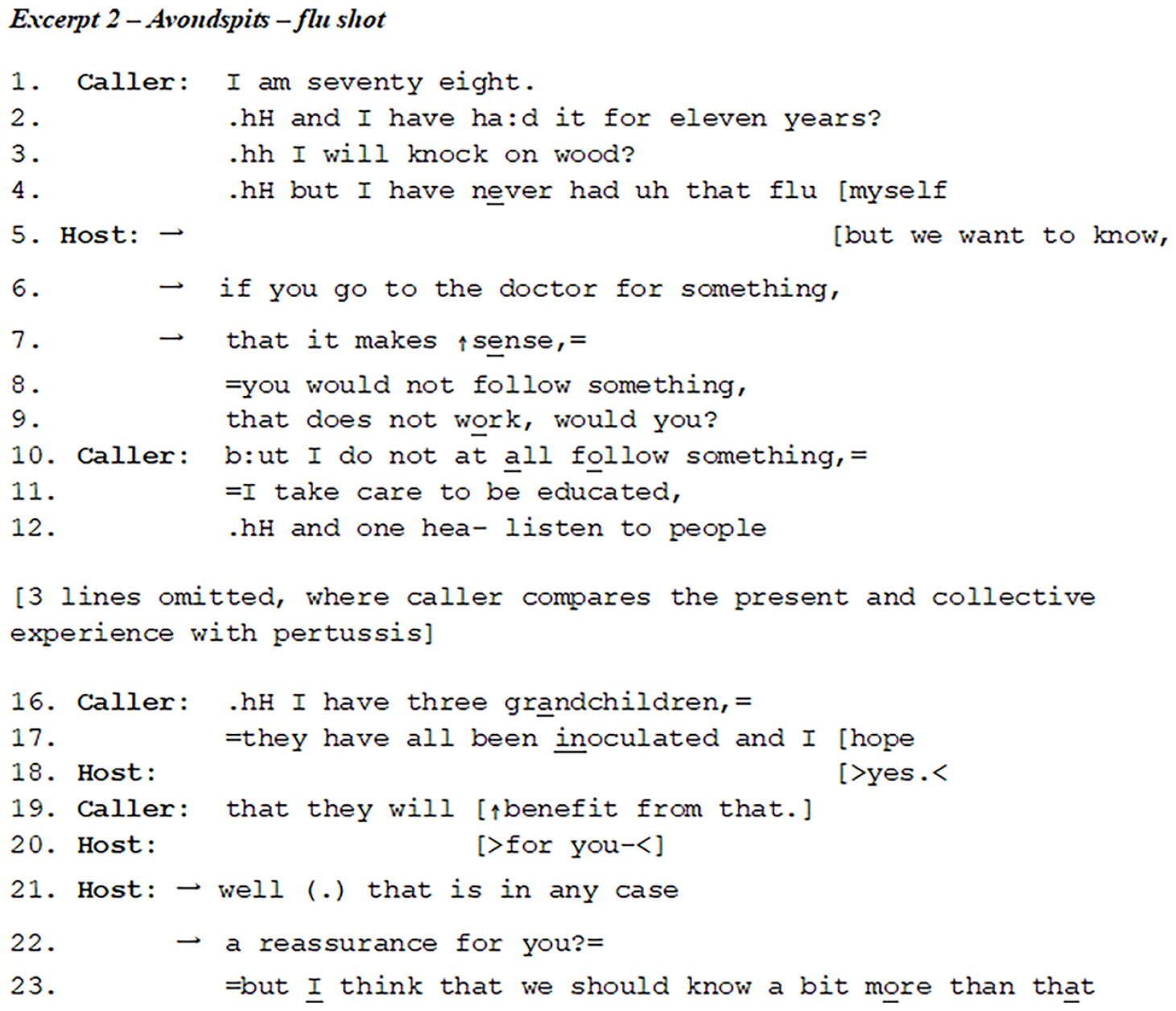
It would be challenging for the host to dispute matters that clearly fall within the caller’s realm of personal knowledge. However, in his next turn, he subtly shifts the conversation from the effectiveness of the flu shot to the caller’s naivety. Note how he invokes the overhearing audience as generalised ‘we’ (line 5), suggesting a common sense shared by rational citizens/consumers while characterising this caller as someone who visits the doctor for ‘something’ (i.e. the flu shot) which ‘does not make sense’ (lines 6–7). The host’s statement, ‘you would not follow something that does not work’, employs a generalised personal pronoun that does not necessarily address the caller (in Dutch: je, rather than jij or u, comparable to the English gender-neutral, indefinite pronoun one). As in the first fragment, the caller is positioned as a naive individual, reinforced by the characterisation of the caller as someone who ‘merely follows’ (lines 8–9). This becomes even more clear in the next part of the conversation. While the host used a generalised personal pronoun, the caller treats his claim as a personal challenge (‘but I do not at
Now that the host has held the caller accountable for uncritically trusting, she defends herself by mentioning that she ‘takes care to educate herself’ (line 11). She continues with ‘and one hea-’ (line 12), which appears to point to ‘one hears’, but the caller substitutes this with the more proactive verb ‘listens’, demonstrating an active process of selecting advice. She proceeds to share her personal experience regarding her grandchildren (lines 16–17) and concludes with a cautious expression: ‘I hope that they will benefit’ (lines 17, 19), which makes relevant a response like ‘I hope so too’. However, the host does not respond in this manner. Instead, he presents his final statement (lines 21–23), reinforcing his earlier position (lines 5–9), which categorically divides ‘you’ (easily reassured) from ‘I’ (seeking genuinely reliable numbers). Even more explicitly than in Excerpt 1, the host particularises the relevance of the caller’s experience by singling her out as a naive, trusting individual. The caller is portrayed as gullible, thereby undermining the relevance of her shared experience for the audience.
The final excerpt in this section differs slightly from the previous ones, as one of the guests is present on location with the host, while the expert who calls in has been invited by the programme. The topic of this conversation is ADHD. Like the previous phone-ins, this conversation is oriented towards conflict. The host begins by reading out several listeners’ reactions, suggesting that ADHD is perceived as an invented excuse by irresponsible parents (omitted from transcript). This has been strongly resisted by the invited guest, who has previously shared her own challenging experiences with her son, who, like herself, has been diagnosed with the disorder (omitted). Next, the host starts to question the guest about her own symptoms:

The host posits that the guest believes that she herself has ADHD (line 2). The mother corrects this in her reply, preempting an implicit challenge: she doesn’t believe she has it, she knows she has it (lines 3–4). The answer implies that she has been officially diagnosed with attention deficit hyperactivity disorder. The mother positions herself as someone who knows, rather than someone who merely believes, thus establishing her authority on this topic. In reaction, the host first provides a listening token (line 5), which prompts the caller to provide evidence for her claim (lines 6–10). Next, the host asks her to specify this (line 11). Evidently, the guest is in a position where she needs to account for ‘how she knows’ (cf. Pomerantz, 1984) as she starts explaining some of her own behaviour, implying that this deviates from what is ‘normal’ (lines 12–21). Next, she pre-empts a challenge by mentioning ‘what people say’, and her own answer to that (lines 22–26).
Instead of reacting directly to the experience offered by her guest, the host introduces the – hitherto silently listening – expert to the programme and asks him whether this is a medical condition (line 27). In this way, the mother’s experiences are not treated as relevant for the here-and-now; instead, the host indicates to prefer a certified, medical explanation. Given that the guest has built an account designed to distinguish between her own symptoms and ordinary problems (lines 12–26), the host’s question is potentially damaging. It is perhaps for that reason that the expert – a clinical psychologist and author – avoids the terms of the host’s yes/no-question (Raymond, 2003), issuing a general statement rather than directly categorising the guest’s individual experience. Instead of using the lay category ‘medical condition’, he uses the more exclusive expert category of the ‘genetically caused brain disorder’ (lines 29–32). The absence of such a disorder once again opens the door to blaming the mother for her son’s condition (Versteeg, 2018). Whereas host and expert do not dispute the content of the caller’s experience, the host has given the expert the right to determine whether this is evidence of a bona fide medical condition (line 27). The expert’s response does not address the guest’s experiential evidence at all, thereby implicitly undermining its relevance in proving the authenticity of the condition.
In sum, this section has shown how the relevance of personal experience can be disputed by formulating it as mere belief. Furthermore, the excerpts illustrated that being positioned as (simply) ‘trusting’ is an interactional problem for receivers, because it can be easily equated with being irrational, gullible, or naive.
Resisting the prescriptive relevance of scientific claims: Probing the right to speak for scientific expertise
In the following part of our analysis, we show that contrary to what might be expected in the alleged ‘post-truth era’, interactants do not treat claims cast in the language of scientific expertise as belief or ‘merely an opinion’. Instead, both callers and hosts carefully delineate which kind of scientific expertise can be claimed by whom. Rather than contesting the relevance or the authority of scientific expertise itself, they dispute who is allowed to speak for it.
We present three examples in which scientific or certified expertise is employed as a trump card. The host probes the knowledge claims put forward by callers to varying degrees, depending on whether the caller positions themselves as a layperson (Excerpt 4) or as an expert (Excerpts 5, 6). In the first excerpt, the caller herself emphasises the epistemic authority of certified experts. In the two latter excerpts, the host challenges the caller’s entitlement to claim a type of knowledge that would be the prerogative of certified experts. In the prior section, we have seen that experience can be particularised and made irrelevant to the overhearing audience. In contrast, we will show in the following excerpts that the relevance of scientific or certified knowledge is not challenged. Instead, the interaction focuses on who is allowed to speak for ‘true’ science.
The first excerpt is a conversation between a host and a caller. Before the excerpt, the caller has indicated that her son has been diagnosed with ADHD, about which she has expressed her doubts (omitted from transcript). The excerpt demonstrates how the caller, even when disagreeing with medical professionals’ diagnoses, persistently positions herself as a layperson, thereby upholding the authority of certified experts. The excerpt begins with the host reflecting on how the ADHD debate seems centred on labelling (lines 1–2), noting that individuals such as the caller may believe their child is not ill (lines 4–6), contrasting with the perspective of ‘the medical establishment’ (line 9). The host makes this juxtaposition explicit in sceptical terms: describing certified experts as the ‘medical establishment’ (line 9) is a mark of respect, while implying room for criticism of this established position. Yet in the caller’s next turn (10–14), we see her struggling to account for her disagreement with the medical establishment, rather than questioning the salience of this established knowledge. She mentions other diagnoses for her son that she has dismissed (omitted), after which she describes her son in casual terms as a ‘bad case of boy’ (lines 36–37), eliciting the host’s laughter in response. However, using a conditional ‘would’-formulation (line 39), the caller emphasises the personal and tentative nature of her description, positioning herself not as the expert on this matter:

In response, the host once more contrasts the caller’s description with the expert opinion (lines 40–41). Nevertheless, the caller acknowledges the possibility for both the expert opinion and her own description to coexist: the experts may have their reasons to classify this behaviour as a psychiatric illness (line 42–43), and she reiterates her position as a non-expert (line 44). Before reiterating her claim that it is ‘more of a boys’ thing’ (line 47) – again in tentative, particularised terms, using the epistemic downgrader ‘it seems to me’ – she emphasises that she ‘does not know her facts at all’ (line 44). Focusing on doctor-patient interactions, Lindström and Karlsson (2016) show that patients use ‘I don’t know’ responses as epistemic disclaimers to not appear more knowledgeable than a doctor or to not take initiatives that are traditionally reserved for medical professionals, such as suggesting a diagnosis or treatment. The ‘I don’t know’-prefaced turn by the caller in Excerpt 4 seems to be used for similar purposes: she demarcates the boundaries of her own knowledge, indicating that making such claims is the prerogative of experts. Thus, even when disagreeing with the experts’ opinion, the caller carefully claims only the knowledge appropriate to a layperson. The host has attempted to create a conflict between the mother’s characterisation of her son’s condition (‘a bad case of boy’) and how certified experts describe it (ADHD as a psychiatric illness, line 41). However, his attempts to provoke conflict failed because the caller consistently positioned herself as a layperson, thereby protecting the authority of certified experts, and consequently, affirming the legitimacy of her son’s diagnosis.
In contrast to the previous excerpt, the caller (a mother who claims her son has ADHD, lines 3–5) in the next fragment begins by positioning herself as an expert, invoking the ‘language of science’. In this programme, a psychotherapist’s assertion that many ADHD diagnoses are unjustified served as the starting point, inviting callers to discuss the topic. We will observe how the host responds to the mother’s knowledge claims and how he emphasises medical professionals as the authorities on the subject.
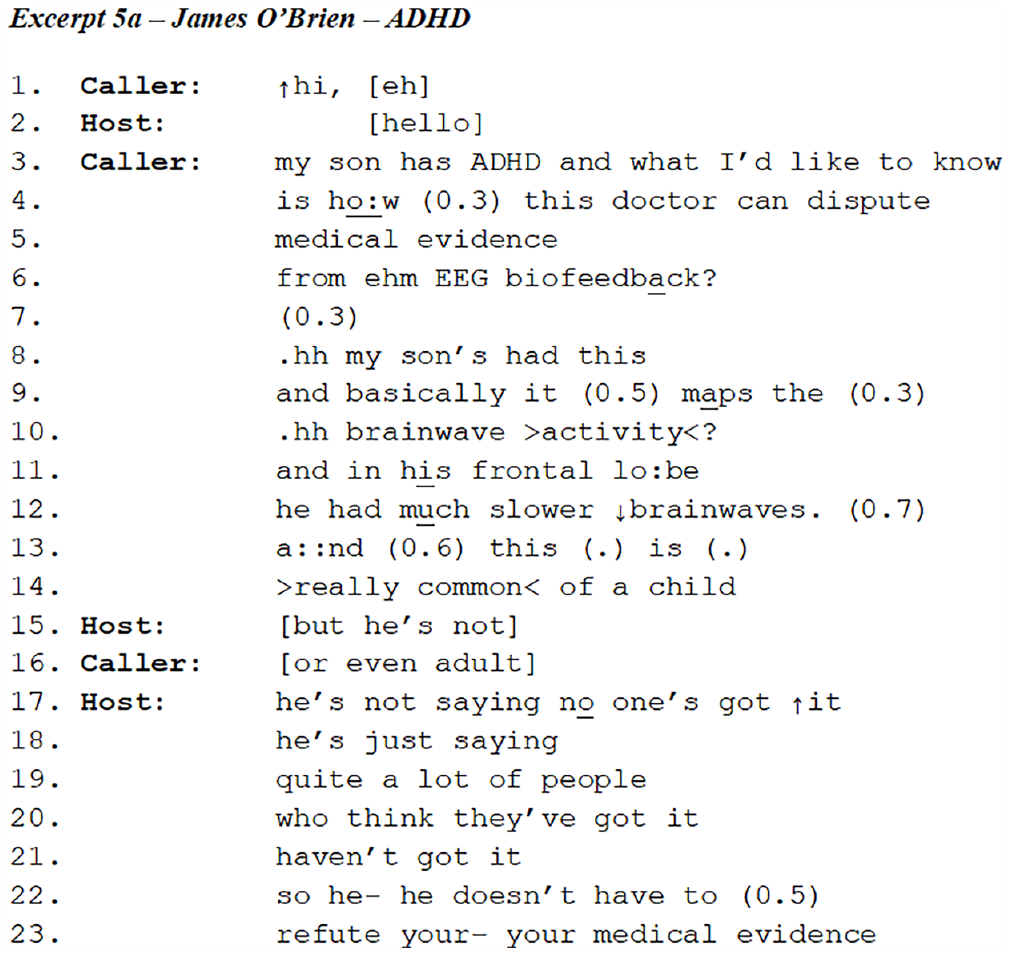
From line 3 onwards, the caller adopts an expert footing, explaining the workings of EEG biofeedback and contrasting the position of ‘this doctor’ (the psychotherapist) with the body of medical evidence. In his response, the host upholds the psychotherapist’s expert status by specifying the general ‘medical evidence’ mentioned by the caller (line 5) to ‘your- your medical evidence’ (line 23).
At this stage, the host and caller still uphold the truth value of both the ‘medical evidence from ehm EEG biofeedback’ (lines 5–6) and the expert authority of the psychotherapist disputing the realness of ‘quite a lot of’ ADHD diagnoses (lines 17–23). Probably unsure about the caller’s credentials, the host does not yet challenge her claims to scientific expertise, but this changes during the conversation, as we will see below.
In the interaction following lines 22–23 (here omitted for reasons of space), the caller first apologises for having misunderstood. The conversation then shifts to the possibility of identifying ADHD through EEG biofeedback, which the caller claims is possible. While ostensibly accepting the truth value of the caller’s claim, the host wonders why, if ADHD is so simple to identify, this test is not taken by everyone. This seemingly innocent question casts doubt on the plausibility of the caller’s statement, especially when the caller adds that the test is not widely available on the NHS. The following interaction ensues:
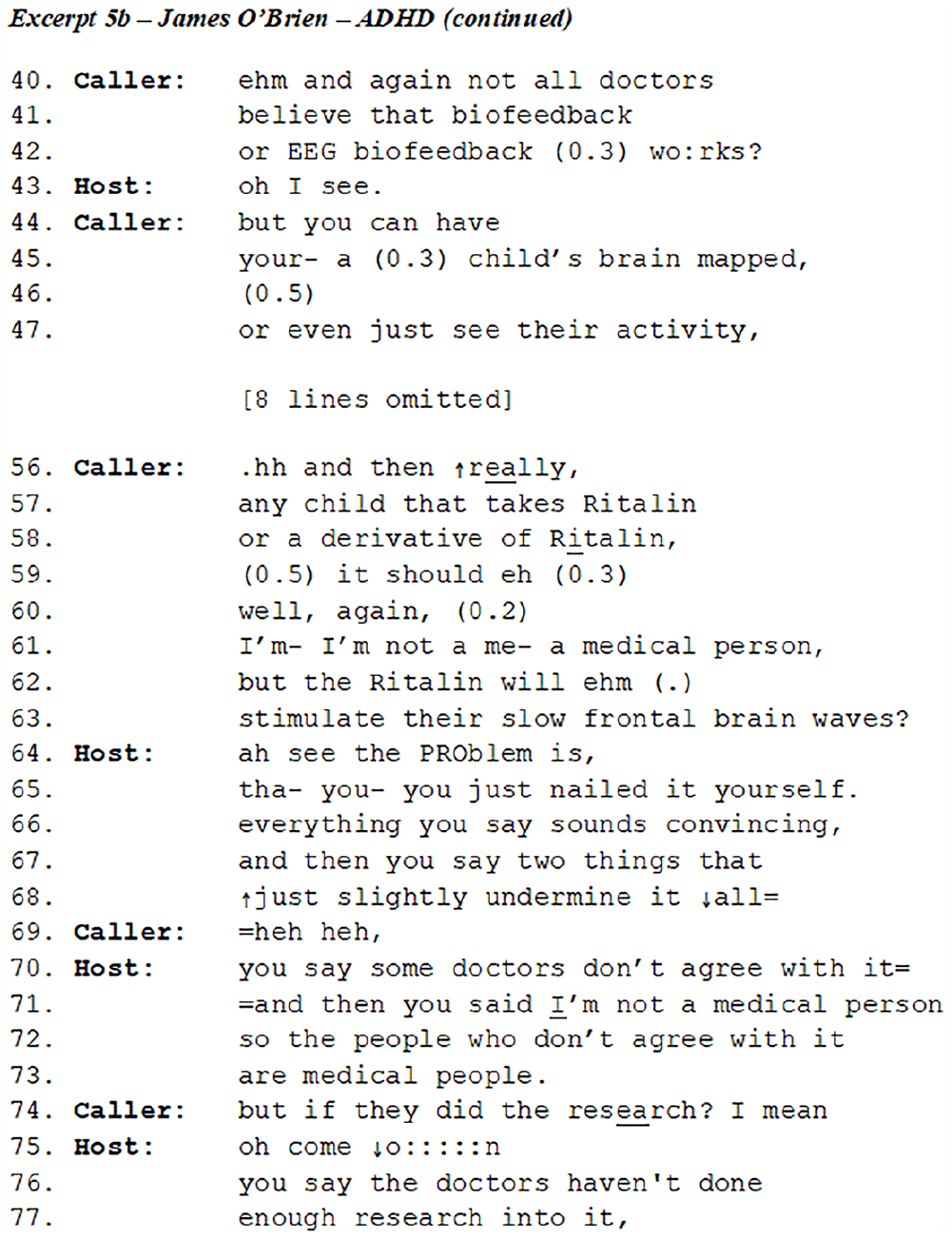
In her first utterances (40–42), the caller treats the effectiveness of biofeedback no longer as a matter of medical evidence but as the subject of belief. She thus positions the alleged minority of doctors who do not subscribe to the effectiveness of neurofeedback as (non-)believers, rather than dissenting experts. Rather than inquiring why some doctors do not believe in neurofeedback or otherwise reacting to the content of the claim, the host merely acknowledges the caller’s claim as received information (line 43). This response conveys disinterestedness or scepticism about the caller’s claims (cf. an Burgsteden and te Molder, 2021). Her assertions about Ritalin (lines 56–58) claim epistemic authority regarding this topic, before faltering (line 59) and providing the disclaimer that ‘I’m not a medical person’ (line 61). In response, the host merely points out the discrepancy between the caller’s ‘convincing’ argument and her lack of category entitlements to make this argument, because she is ‘not a medical person’. In her response to the host’s rather damaging statement, the caller refers to another scientific symbol, suggesting that the doctors did not do the necessary research (line 74). The host reacts by treating her claim as ridiculous (line 75). Consequently, the caller’s claim to epistemic authority has been thoroughly discredited and she herself is no longer treated as a credible spokesperson. In sum, throughout the interaction, both the host and caller have protected the authority of ‘medical evidence’ and ‘the doctors’ – while defending a position that some doctors may not agree with.
The caller in the next fragment also positions herself as an expert, when recommending the use of elderberry extract instead of taking the flu shot (lines 1–7). In this case, however, there is a certified expert – a general practitioner – present in the studio. The host starts to address him in line 8:
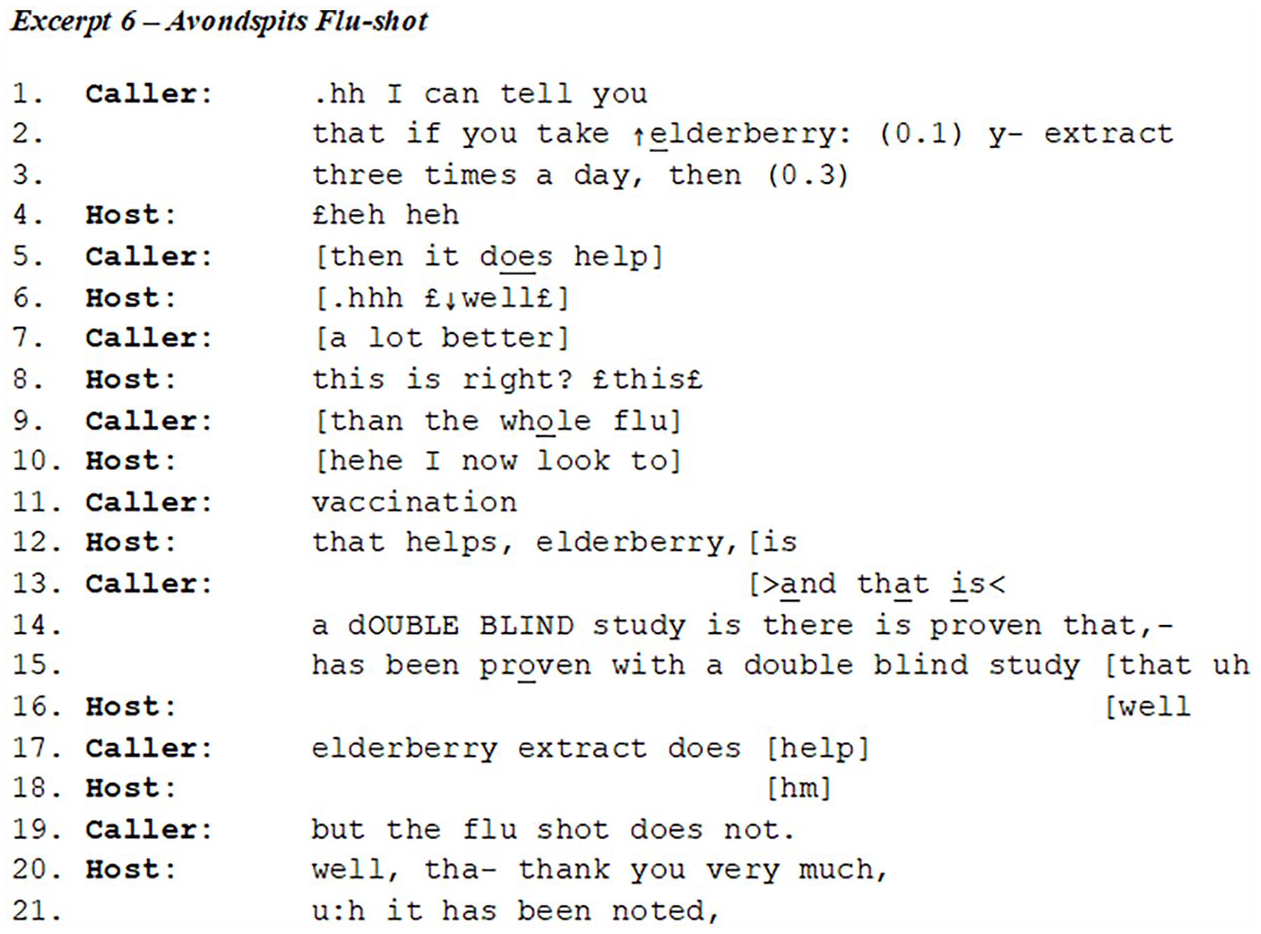
The caller adopts an expert footing by using a conditional ‘if . . . then . . .’ statement, a recipe-type formulation (cf. Matoesian, 1999; Sneijder and te Molder, 2005). The host starts to laugh. The laughter’s sequential positioning, immediately following the caller’s turn, identifies this turn as the laugh source (Jefferson, 1979) – the element of talk triggering the laughter (Glenn, 2003). The host’s laughter is not presented as ‘laughing with’, but rather as ‘laughing at’ the caller (Glenn, 1995). Through his laughter, then, the host shows his doubts regarding either the caller’s remedy or her right to provide people with this advice. In lines 5–11, the host and caller struggle for the floor. The host unsuccessfully attempts to interrupt the caller at the transition relevant points, questioning her right to provide advice by directing a question to the general practitioner who is his studio guest (lines 8, 10 and 12). Throughout this struggle, the host tries to grant the GP the epistemic right to either confirm or conclusively deny the value of the caller’s suggestion. But the GP is silent, and the caller refuses to be overruled, instead referring to the scientific basis of her claim and repeatedly pointing out that this has been ‘proven’ in a ‘double blind study’.
Now that the privileged epistemic status of the expert has been made relevant by the host, the caller claims objective access to a scientific study that has proven her argument. By drawing on a superior kind of scientific knowledge (a double-blind study, rather than a single expert’s voice) the caller ups the ante. When the GP stays silent, the host retreats and confines himself to a doubtful interjection (‘hm’, line 18). Only when the caller offers ‘so the flu shot does not’, providing the upshot of her claims (Raymond, 2004), does the host respond with ‘it has been noted’. This response allows him to proceed to the next conversation without evaluating the truth value of this caller’s prescriptive claim. It acknowledges the caller’s prescription in a tokenistic way rather than engaging with its content. Because the GP – the host’s certified expert – did not intervene, the truth value of the double-blind study is neither confirmed nor undermined in decisively.
Conclusion and discussion
In this paper, we discussed the evaluation and treatment of different knowledge sources offered by callers in the context of the radio phone-in. We were specifically interested in whether there would be a difference in the way hosts resist the relevance of offered personal experience as compared to the relevance of claims based on certified knowledge.
We found that that personal experience and certified knowledge are treated by the speakers as incontrovertible sources in themselves, but that their relevance to the overhearing audience can nevertheless be disputed. This, however, happens in strikingly different ways. The host cannot challenge the caller’s experience as such, but he can particularise its relevance by treating the caller as naive for blindly trusting his or her own experience. The host then acts as the spokesperson for the more rational overhearing audience, singling out the caller as a gullible individual. This practice restricts the pertinence of the caller’s experience to the caller himself, resisting its relevance for the overhearing audience.
In contrast, when the host disputes evidence that is presented as certified or scientific, he does not challenge the relevance of science. Instead, he challenges the right of the caller to act as science’s spokesperson. Both host and caller treat science as a superior knowledge source, to be employed as a trump card in the interaction. Whereas callers may claim knowledge by using a scientific vocabulary (‘proven by a double blind study’), they are also careful to admit their own, non-expert status (‘I’m not a medical person’) – sometimes, as in Excerpt 5, during the same conversation. Paradoxically, while disputing each other’s claims, the host and the caller thus cooperate in upholding the authority of scientific or expert knowledge.
The radio phone-in is a specific, highly regulated environment, in which the host enjoys far-reaching privileges. Whereas one should be careful in generalising the findings of this study to other contexts, we argue that the way in which experience and science are treated in radio phone-ins enlightens us about broader societal norms.
First, our results suggest a possible explanation for the frequent contestation of factual sources in semi-public exchanges (van Zoonen et al., 2007). Speakers provide knowledge sources not merely to support or to limit a claim (Pomerantz, 1984), but also to prove their ‘epistemic vigilance’ (Sperber et al., 2010). Being treated as a gullible person or believer is an interactional problem, as illustrated by Excerpts 1–3 in this article. Referring to scientific knowledge helps speakers to demonstrate that they are not inclined to easy beliefs or vulnerable to being duped. This results in the somewhat paradoxical situation that science is employed to show one’s own critical attitude. Providing sources of knowledge becomes part of interactants’ ongoing attempt to index the relationship between them – even in a context where this relationship is highly regulated and predefined as asymmetrical.
Second, our results shed a different light on the allegedly diminished authority of scientific knowledge. If the truthfulness of facts did not matter, people would not need to contest them so vehemently, both within interactional environments designed to elicit controversy and outside them (Versteeg, 2018; van Zoonen et al., 2007). Given how interactants employ scientific knowledge sources as a trump card and collaboratively police who should be allowed to speak for science, we argue that science is treated as a highly authoritative source of knowledge, even in the seemingly anti-scientific environment of the radio phone-in (cf. Bolden, 2013; European Commission, 2010, 2014; Kerr et al., 2007; Martin et al., 2019).
When interactants try to prove a point, they will often do this by emphasising the merits of one particular knowledge source as compared to others. For instance, as Pollner (1987: 8) argues: ‘when the virtuosity of science’s systematical nature is displayed, it is displayed in contrast to the more or less chaotic character of common-sense knowledge’. In the cases analysed here, experience often provided the entry ticket for callers, whereas science was clearly employed as a trump card to win the argument. This finding reflects the set-up of the radio phone-in and does not mean that one knowledge source always outranks the other. However, combined with the reluctance shown by interactants to challenge the relevance of certified expertise, it does suggest that science – or at least a ‘scientific repertoire’ – carries considerable authority.
Further research should therefore not limit itself to the question as to whether either personal experience or certified or scientific expertise is the more authoritative knowledge source. Rather, we should inquire how interactants selectively employ knowledge sources. Knowledge, as we hope to have shown, is used not merely to win an argument, but as part of interactants’ ongoing endeavour to establish their credibility as critical, and for that reason, trustworthy speakers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.