
Abstract
The article uses conversation analysis to investigate how patients and companions complain in palliative care interactions recorded in a UK palliative care setting, and how healthcare professionals (HCPs) respond. The patients’ and companions’ actions do not overtly state, and rather imply, complainable matters for which the co-present HCPs can be seen as responsible. This implicitness affords the HCPs opportunities to address the patients’ and companions’ conveyed concerns as problems in search of practical solutions – rather than grievances. We thus witness the somewhat paradoxical outcome that complaints mobilise remedial actions, but in the process, the one complaining is not treated as complaining after all. We propose that this is a way in which institutional realities pre-empt the overt articulation of nascent complaints. Our analyses show that this is very much the outcome of the interactional work collaboratively accomplished by patients, companions and HCPs. The interactions are in British English.
Keywords
Introduction
Healthcare professionals (HCPs) and academics have long recognised HCP-patient consultations as social and relational occasions (Balint, 1957; Donabedian, 2005; Heritage and Maynard, 2006). If the relationship becomes strained, both parties stand to lose: patients in terms of health outcomes (Stewart et al., 2000) and HCPs in terms of job satisfaction and potentially litigation (Humphrey et al., 2022). When patients or their representatives are unhappy this can manifest as complaining. By complaining, people draw attention to negative consequences of other parties’ actions, including mistreatment and disservice, and solicit recognition and remediation (Ahmed, 2021). The significance of these processes cannot be overstated for the domain of practice we investigate in this article: the delivery of palliative and end-of-life (EOL) care in face-to-face interaction. In the UK, our national context for this study, complaints about EOL care have increasingly been a focus of debate (Parliamentary and Health Service Ombudsman, 2015). Unsurprisingly, such discussions focus on formal complaints submitted by patients or their representatives. By contrast, the apparently more fleeting activity of complaining in co-present healthcare interactions, which may never eventuate in formally recorded grievances, has received no attention. It nevertheless constitutes an early opportunity for patients and companions to draw HCPs’ attention to ‘complainable matters’ (Drew and Holt, 1988; Schegloff, 2005) and for HCPs to undertake remedial actions before circumstances deteriorate (and perhaps before patients or companions seek the intervention of a third party (Emerson and Messinger, 1977)). We investigated cases in which patients with life-limiting conditions and their companions complain, and the ways in which HCPs respond in face-to-face interactions in a UK palliative care setting.
Complaining
Complaining can be understood as ‘express[ing] feelings of discontent about some state of affairs, for which responsibility can be attributed to “someone”’ (Heinemann and Traverso, 2009: 2381). As a social action, complaining invites recognition of, or even agreement with the complainer’s position and perspective (Couper-Kuhlen, 2012; Drew, 1998). However, complaint recipients in mundane interactions sometimes avoid doing so because of the consequences that supporting a complaint can entail (Holt, 2012; Mandelbaum, 1991/1992). In service interactions (see Pino (2022) for a review), endorsing a client’s complaint can be seen as siding with them against the target of the complaint, thus violating norms of professional neutrality and impartiality (Ruusuvuori and Lindfors, 2009). However, maintaining a neutral position towards a complaint can be equally problematic, especially in settings such as healthcare services, where professionals are also expected to demonstrate understanding of clients’ experiences and perspectives (Pino, 2022). We refer to this as a ‘distance-involvement dilemma’ (Raymond and Heritage’s, 2006: 701). Such dilemma is arguably exacerbated when a client complains about the actions of an addressed, co-present institutional representative rather than an absent party. In this context, endorsing a client’s complaint could be understood as an admission of responsibility, which institutional representatives may wish to avoid for various reasons (including avoiding providing materials that a client could leverage in the future, e.g. to seek compensation).
Previous research suggests that resources are available to navigate the distance-involvement dilemma when responding to complaints. In mundane interactions, recipients can produce responses that are somewhat equivocal – ‘mid-range’ between affiliation and disaffiliation (Holt, 2012) – thus avoiding the equally undesirable alternatives of supporting a complainer’s position and disagreeing with them. When a complainer’s turn does not state and rather implies a complainable matter and attendant attributions of responsibility, recipients can dis-attend the complaint aspects of that turn and respond to other aspects instead (Mandelbaum, 1991/1992). Particularly available in service interactions is the option to treat the client’s action as reporting a problem requiring a practical solution (Jefferson and Lee, 1992) rather than a grievance. Alshammari and Haugh (2024) showed that, in service interactions, reports of troubles implement requests for assistance and can thus be relevantly responded to by offering solutions. However, such reports can also be heard as doing more than seeking practical solutions, that is, they can be heard as attributions of wrongdoings, which make relevant more morally charged responses (including admitting to a wrongdoing and apologising). The relevance of such responses may increase when clients escalate their complaints – for example, by progressing from an implied to an explicit attribution of a wrongdoing.
Kevoe-Feldman (2018) documented that the call-takers of a customer service helpline worked to prevent implied complaints about delays in service provision from escalating (i.e. becoming explicit), for example by providing accounts for those delays. Other research has suggested that displaying some recognition of the complainer’s perspective may be key to preventing complaint escalation. By examining client complaints about absent parties in a bereavement support group, Pino (2022) proposed that such complaints embody a display of hurt (a characterisation of the negative impact an event had on the complainer) and a blaming (an attribution of responsibility to some absent party for causing that). The group facilitators had the option to recognise the impact of the reported events on the client (the hurt) whilst avoiding endorsing the attribution of responsibility (the blaming) also embodied in their complaint. Focusing on calls to a complaint phone line, Benwell et al. (2024) showed that displaying recognition of the caller’s perspective and treating it as reasonable (see also Ruusuvuori and Lindfors, 2009), was crucial to pre-empting complaint escalation and facilitating resolution of the complaint sequence. By contrast, withholding recognition was associated with complaint escalation.
In this article, we investigate cases within interactions in a UK palliative care setting where patients and companions complain about matters for which a co-present HCP can be treated as responsible, either personally or as part of a care team. To our knowledge, there has been no research on complaints about co-present (as opposed to absent) HCPs in healthcare interactions – a significant omission we redress here. We demonstrate that the HCPs deploy a combination of resources to navigate the distance-involvement dilemma when responding to patient/companion complaints: producing mid-range responses ostensibly designed to treat the patient’s/companion’s perspective as legitimate whilst avoiding endorsing it as complaint; and selectively attending to other aspects than the complaint aspects within the patient’s/companion’s actions – especially by addressing them as ‘problems to be solved’ (Jefferson and Lee, 1992). Use of these resources is made possible by the implicit manner in which the patients and companions raise complainable matters and attendant attributions of responsibility (Ruusuvuori and Lindfors, 2009). The HCPs’ responses work to maintain such implicitness, thus arguably preventing complaint escalation (Schegloff, 2005). What emerges in the end is not a full-blown complaint but rather a shared attempt to solve a problem. Our article advances understandings about complaining as an interactional activity by highlighting its paradoxical nature: raising a complainable matter and having it addressed may entail that the one raising it is not treated as complaining after all. We further argue that this is a way in which institutional realities, understood as the practical and emergent outcome of participants’ actions, pre-empt the overt articulation of nascent complaints.
Materials and methods
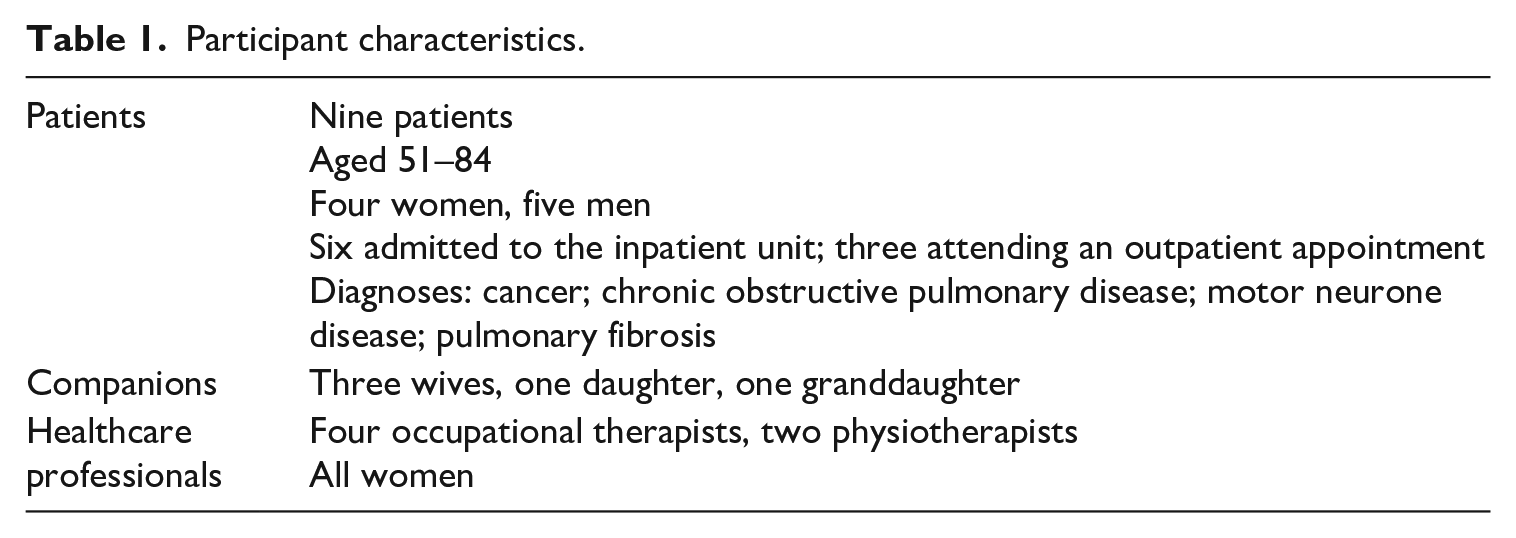
We used conversation analysis (CA; Sidnell and Stivers, 2013) to examine palliative care consultations recorded at a large UK hospice. Ethical approval was granted by UK NRES Committee Nottingham 2 (Ref: 17/EM/0037). Patients diagnosed with a life-limiting condition having an inpatient, outpatient or day therapy consultation with one or more physiotherapists and occupational therapists were invited to participate if they had capacity to consent, could speak and understand English, and were judged by their clinical team not to be in acute distress. Patients were engaged with hospice services primarily for assistance with managing difficult symptoms and for help planning their future care. These data, collected in 2017, comprise more than 35 hours of recordings of 48 consultations (39 video, 9 audio) involving 48 patients (21 being with a companion) and at least one of 8 therapists (3 physiotherapists, 5 occupational therapists). Everyone gave written consent for retention and analysis of the recordings, and for transcript publishing. All transcripts have been pseudonymised to maintain confidentiality.
CA is a well-established method for studying interaction in healthcare, and it has previously been applied to palliative care settings (Parry, 2024). CA involves examining naturally occurring, recorded interpersonal interactions, and analysing how participants accomplish social activities through interactional practices implemented through talk and visible conduct (e.g. gaze and gesture). Working inductively, we screened the corpus for actions that could be glossed as complaint implicative. Such instances were widespread. However, of 115 complaints, we only identified 11 instances wherein a patient or companion could be heard as treating a co-present HCP as responsible or co-responsible for the matter being complained about. We find this unsurprising and, indeed, a suggestive finding, supporting our conjecture that complaining about a co-present HCP is a highly sensitive activity. Although the small size of the collection grounding our analyses means that we may not have captured all the properties of patients’ and companions’ complaints and HCPs’ responses, it does not make our investigation less significant or less urgent, given the absence of research in this area.
The 11 complaints come from nine consultations (see Table 1 for participant characteristics). We used transcription methods that capture temporal and prosodic aspects of participants’ speech (Jefferson, 2004; see Appendix). We drew on our expert knowledge of the setting to articulate aspects of context and common ground, which we propose participants relied on to understand the complaints as co-implicating the HCPs’ responsibility. We nevertheless used CA validation procedures to support our claims by showing how the participants themselves observably oriented to these elements of responsibility (Schegloff and Sacks, 1973; Sidnell, 2013).
Participant characteristics.
Results
The patients’ and companions’ actions are unequivocally hearable as complaining. However, they do not state and rather imply the matter they are complaining about. The co-present HCPs can be understood as liable for those complainable matters, either solely or as part of the clinical team (see Marian et al., 2023), based on context and common ground. In one case where a complaint appears more explicit (extract 2a), additional and more pervasive complainable matters are implied. The HCPs respond in ways that recognise the patients’ and companions’ concerns and perspectives as legitimate but handle them as problems in search of a practical solution rather than grievances. We exemplify this with three cases that are representative of findings across our collection.
‘I don’t like the way you’re saying “I’ll see you tomorrow”’
Extract 1 is from an inpatient consultation between an 83-year-old woman with lung cancer, Carol, and two occupational therapists (OTs). The interaction takes place in Carol’s individual room. Carol has been receiving treatment in the hospice for several days. Before extract 1, she voiced her hope to be discharged today, to which one of the OTs responded that discharge has not been mentioned yet (presumably within the hospice multidisciplinary team, which is responsible for discharge; data not shown). After 25 minutes, in extract 1, one OT begins to arrange the next meeting, projecting the end of the interaction (lines 1–3). This invites a response from Carol, but a silence emerges (line 5).
The implied complainable matter
Carol’s response, ‘that is fine’ (line 6), accepts the OT’s proposal, but the emphasis on ‘is’ can be heard as projecting some unfinished business. After a silence, the participants re-enter in overlap. The OT produces ‘Alright’ (line 8) with falling intonation, audibly designed to close the matter. Carol, however, continues with a turn hearable as complaining: ‘But I don’t like the way you’re saying [. . .]’ (lines 9–10). This utterance is not designed to be understood literally as discontent with the OT’s speech, but rather as alluding to a different complainable matter. The OT’s response, ‘Because you want to go home’ (line 12) provides evidence that she understands Carol’s discontent to be about staying at the hospice for another night. Whilst this response recognises Carol’s conveyed perspective as reasonable (Benwell et al., 2024) and is thus hearably empathic (Ford et al., 2019), it foregrounds the positive outcome that Carol wants to achieve (going home) and maintains in the background the complainable matter (being kept at the hospice) and who is responsible for it. Carol validates the OT’s conveyed understanding with a repeat (line 13), confirming that she (Carol) has alluded to, rather than stated, the complainable matter (Schegloff, 1996).
The HCP produces a mid-range response
The complainable matter is one for which the clinical team, which the OT represents, can be seen as responsible based on context and common ground (they are responsible for planning discharge and, indeed, the present consultation is aimed at assessing Carol’s capacities for daily living and the kinds of support she might need when she goes home). Carol addresses matters of responsibility by expanding her response to the OT (lines 13–18) but offsets the possibility of being heard as blaming the clinical team by blaming her family instead (see Marian et al., 2023). She uses well-documented practices for complaining, including reported speech (lines 15–17 (Holt, 2000) ) and extreme case formulations (‘this is all I’m getting all the while from them’, lines 17–18 (Pomerantz, 1986) ). Despite this, the OT treats Carol’s complaint as pointing to the clinical team’s responsibility by providing a best interest account for extending her stay (lines 21 and 23). This implies the care team’s agency but stops short of articulating who exactly is responsible for Carol’s discharge. The conspicuous absence of a pronoun in subject position (lines 21 and 23) works to gloss over who wants to ‘get to the bottom of it’. It thus avoids detailing the circumstances of the complainable matter, which could amount to making explicit something that Carol has only implied (Drew and Walker, 2009). This arguably works to pre-empt escalation of a nascent complaint (i.e. making it overt; Kevoe-Feldman, 2018).
In these ways, the OT can be seen to achieve a delicate balance in her response. She recognises Carol’s conveyed dissatisfaction (line 12) but stops short of fully endorsing it, especially by avoiding addressing matters of responsibility (Pino, 2022; Ruusuvuori and Lindfors, 2009). The OT’s response is thus not straightforwardly affiliative or disaffiliative; it is, in this this sense, ‘mid-range’ (Holt, 2012).
The complainable matter is handled as a problem to be solved
The OT’s account (lines 21 and 23) alludes to the possibility of a quick resolution of the complainable matter; ‘just’ (line 21) suggests that Carol will not be held for longer than necessary. The OT thus maintains the practical, solution-oriented focus already implied by her earlier formulation of Carol’s perspective (line 12). This contrasts with other possible responses, such as an apology for extending Carol’s stay, which could amount to an admission of responsibility for a wrongdoing. Subsequently, the OT moves towards closing the matter with ‘Okay then’ (line 26) and treats the issue as a practical matter for which a ‘plan’ has been agreed on (lines 26 and 28).
To summarise, the OT balances recognising Carol’s dissatisfaction with avoiding commenting on the complainable matter and attendant attribution of responsibility. The opportunity to do so is afforded by how Carol herself designs the complaint (e.g. by only alluding to it, and then by deflecting responsibility to her family). A complainable matter (with its attendant attribution of responsibility) is thus collaboratively kept implicit and, concurrently, treated as a controllable problem rather than a major cause of dissatisfaction.
‘You want me to get my slippers out’
In extract 2, shown in two parts, the patient’s complaint is more explicit but still implies an additional, and more pervasive, complainable matter. We are at the start of an inpatient consultation between a 75-year-old woman with lung cancer and brain metastases, Jan, and the same occupational therapist (OT) as extract 1. The interaction opens with the OT entering Jan’s individual room and asking for permission to sit (extract 2a, lines 1–2).
The implied complainable matter
The complaint is constructed as a contrast: ‘well I don’t want me slippers on, but you want me to get my slippers out, go for a walk’ (extract 2a, lines 27–29). Responsibility is openly conveyed: ‘you want me to’ (line 28) attributes agency to the OT whilst displaying opposition to the anticipated project of going for a walk. Jan’s granular description (lines 27–29 and 32) depicts it as an imposition (Drew, 1998). By stressing three action verbs in a rhythmic pattern (‘↑get’, ‘↑go’ and ‘↑come’, lines 28–32), Jan renders the exercise as predictable and possibly tedious. Taken at face value, the problem appears to be that Jan anticipates being asked to do something that she does not want to do (especially through the pre-emptive and overdetermined (Drew, 1998) description of the OT’s intentions with ‘Where are you going to want me to go?’, lines 14–15). However, from the opening of the interaction there are also hints that she treats the OT as intruding on her. ‘Because I was sitting over there obviously’ (lines 8–9) implies that she has had to move to allow this consultation. She can thus be heard as alluding to the complainable matter that her routine is disrupted by the hospice staff, perhaps because of the unpredictability of her interactions with them – something she further alludes to later (extract 2b lines 46–47 and 49). This analysis is supported by our knowledge of ward interactions in healthcare settings. In a study of interactions between people living with dementia and hospital staff, Allwood et al. (2017: 224) noted that ward interactions are not initiated or sought by patients but rather ‘carried out in [their] best interest, and perhaps because of that, oriented to as an imposition on the patient’s time’. Our knowledge of the hospice suggests that the staff work to fit activities around the patients’ requirements and that they show sensitivity to their preferences and needs when doing so (like the OT does in extract 2a). Such considerations are nevertheless balanced with institutional requirements, including the need to complete assessments, and the availability of the HCPs. Orientation to this tension is evident in Jan’s anticipatory description of the OT’s agenda in extract 2a and in the negotiation seen in extract 2b.
The HCP produces a mid-range response
The OT responds with tokens of agreement (‘yeah’; extract 2a, lines 31 and 33), which can be heard as confirming that she wants Jan to walk, whilst not commenting on the complainability of the anticipated activity and Jan’s stated unwillingness to participate. This works to validate Jan’s anticipatory description of the OT’s agenda whilst avoiding uptake of its complaint elements. This appears designed to pre-empt escalation of a nascent complaint. The OT starts to offer an alternative arrangement (extract 2b, lines 34–35). The offer, which fully emerges in lines 41–43, constitutes a mid-range response between affiliation and disaffiliation, because it treats Jan’s display of opposition as serious enough to warrant a change of plans but stops short of treating it as a complaint (e.g. by apologising, which would concurrently admit responsibility for a wrongdoing).
The complainable matter is handled as a problem to be solved
The OT’s proposal of an alternative plan is framed as an offer, ‘do you want to’ (line 34 (Curl, 2006) ). She suspends this in favour of proffering a reason for the offer: that Jan has been experiencing back pain (lines 34–35). Jan confirms (line 36), adds that she has taken pain killers (line 36), and speculates about the time it should take for the medication to work (lines 38–40). Jan thus displays an understanding that the OT’s projected offer is to postpone the walk until her pain subsides. The OT proceeds to make such offer (lines 41 and 43), which Jan accepts (albeit conditionally, lines 44 and 46–47). The OT and Jan thus collaborate in handling the matter as a problem to be solved (Jefferson and Lee, 1992) rather than a cause for grievance – as temporary inability to engage in a planned activity, which is accommodated with a postponement. The reason for postponing (back pain) stands in contrast to possible alternatives, especially the alluded-to matter of being disrupted by the staff. The focus of the complaint is thereby ‘displaced’ (Edwards, 2005: 16) to a matter for which the staff cannot be seen as responsible. Compared with extract 1, in extract 2b the OT thus works more actively to fend off the implication of a wrongdoing on the staff’s part. Invoking the burden of pain displays attentiveness to Jan’s needs and is hearably empathic.
To summarise, the OT recognises Jan’s perspective (Benwell et al., 2024) but does not validate it as a complaint, thus working to keep a complainable matter and attendant attribution of responsibility unarticulated – with which Jan collaborates. Handling the complainable matter as a practical problem for which a plan is put in place further works towards sequence closure and arguably pre-empts escalation of a nascent complaint, which could otherwise progress towards a full-blown attribution of responsibility to the OT for disrupting Jan’s day. Jan eventually refers to another incident, which happened in the morning. Although this complaint more explicitly points to the timing of the HCPs’ interactions with her as a complainable matter (lines 49), it is not foregrounded and rather remains embedded within Jan’s request that the OT does not postpone the anticipated by activity for too long (lines 46–47; Ruusuvuori and Lindfors, 2009). Therefore, what becomes crystallised is not an overt complaint about HCPs, but a negotiation about the timing of a planned activity that should take place when Jan is most physically comfortable.
‘The palliative care was not there’
Our final example (extract 3, shown in three parts) again concerns the thorny issue of discharge home (see extract 1). It further demonstrates the patterns identified in the previous cases, with some differences. The complaint is produced by a companion and is more extended. Also, treating the clinical team as responsible for a possible wrongdoing is more implicit. Finally, the patient, rather than the HCP, is the first to move towards a possible solution.
Extract 3a starts 8 minutes into a 12-minute inpatient consultation involving a physiotherapist, a 61-year-old man with rectal cancer, Karl, and his companion (his wife), Susan. The interaction takes place in a consultation room used by the physiotherapists to assess physical abilities. Prior to extract 3a, Karl completed a physical exercise (walking up and down a set of steps twice) designed to assess how he might manage at home. It was demonstrably an effort, causing him to shake (data not shown). As he is assisted to sit in his wheelchair, the physiotherapist comments that Karl would only need to climb the stairs once a day at home because he has a toilet downstairs (extract 3a, lines 1–2 and 4–5). Then, for the first time, the physiotherapist asks Susan a question.
The implied complainable matter
The physiotherapist’s question is followed by silence (extract 3a, lines 9 and 11). She treats this as forecasting trouble by rephrasing ‘how did you feel that went’ (line 8) to the more problem-attentive (Stivers, 2007) ‘have you got any concerns about stairs’ (line 15). Susan responds by raising broader disquiet about Karl coming home (lines 17 and 19). This appears to treat the physiotherapist’s earlier comment that Karl would only need to climb the stairs once a day (lines 1–2 and 4–5) as implying that Karl is seen as fit to go home. ‘I have concerns’ (line 19) does not directly blame the physiotherapist or the hospice clinical team, but by later adding ‘I’m sorry to say’ (line 27) Susan manages the possibility of being heard as complaining about their actions. She then specifies her worry about managing Karl’s pain without professional support. Invoking previous experience with her father, she complains that ‘the palliative care was not there’ (line 28) and conveys that she anticipates facing the same problem now (‘And I don’t think I can deal with that’; line 32). We might describe Susan’s action as a ‘proxy complaint’: at the surface, she anticipates difficulties because of insufficient palliative care at home (a ‘safer’ complaint (Sacks, 1992) because this is something for which the hospice clinical team cannot be seen as responsible based on context and common ground). However, by raising this after the physiotherapist’s assessment of Karl’s mobility (lines 1–2 and 4–5), which referred to the layout of their house and can thus be heard as presuming that he will go home, Susan can be heard as alluding to the complainable matter that the hospice team might be planning to discharge Karl in unsafe conditions.
The physiotherapist asks whether the doctors have discussed home (extract 3b, lines 33–35). This question is hearable as a pre-recommendation (Barnes, 2018), working to establish whether a solution has been attempted before possibly suggesting it. This pre-recommendation shares some features of a mid-range response (treating Susan’s conveyed concern seriously whilst not validating it as a complaint) and opens a space for negotiation of a possible solution. However, it also allows Karl and Susan to raise another complainable matter – that the doctors have not addressed his discharge home. However, rather than escalating the complaint, Karl and Susan mitigate it with ‘not really’ (lines 36–38) and ‘yet’ (line 38). There is evidence that Karl treats the prospect of discharge as the complainable matter to which Carol has alluded: he reassures that ‘there’s no pressure being put on me [. . .]’ (lines 43–44). The physiotherapist confirms this (line 45) and expands with further reassurance (lines 49–50 and 52). In these ways, the participants collaboratively minimise the possibility that Susan’s conveyed concern is understood as a complaint about the clinical team (whilst showing orientation to this possibility; Schegloff, 2005). Karl then goes on to develop Susan’s concern about the availability of analgesia at home (lines 53–55, 57, 59 and 61–62), which gives Susan the opportunity to reiterate, ‘That’s what I mean . . . the palliative care is not there’ (lines 64 and 67).
The HCP produces a mid-range response
Karl is the first to imply a possible solution in extract 3c: a transfer to the ‘ward at Belton’ (a community hospital) as an alternative to home (lines 69–70 and 72). It is unclear if this has already been discussed with a HCP, but there are constraints on the physiotherapist who would not usually authorise such a transfer. She offers to relay what has been said to the doctors (line 80–81 and 85). This is a mid-range response between affiliation and disaffiliation – treating the concern as serious enough to warrant raising with the wider clinical team without agreeing that there is a problem.
The complainable matter is handled as a problem to be solved
Offering to feed back to the doctors (line 80–81 and 85) provides a pragmatic solution. The complainable matter – that the hospice can be understood as planning to discharge Karl without appropriate support in place – remains in the background whilst a practical facet of the situation is foregrounded instead: Susan cannot cope with supporting Karl at home, which should be addressed by the wider clinical team. Immediately after extract 3c, in data not shown, Susan voices concerns about the stairs. The physiotherapist explicitly acknowledges that things need to be safe. However, no other plan is suggested; she reiterates the proposal to feed back to the doctors. This being accepted by Karl, she returns him to the ward.
Discussion
The patients and companions do not overly state and rather allude to the nature of the matter they are complaining about and who might be responsible for it. When a complaint is more explicit (as in extract 2a), additional complainable matters and associated responsibilities can be inferred. The patients’ and companions’ caution is not surprising given that they are complaining to HCPs who are responsible for their care. This implicitness affords the HCPs the opportunity to respond in tactful ways, treating the patients’ and companions’ conveyed concerns seriously but concurrently avoiding recognising them as grievances. The HCPs do so through mid-range and pragmatic responses, which reflexively treat those concerns as practical problems requiring solutions. This is reminiscent of cases in ordinary interactions of ‘disattending, or not taking up, another’s apparent complaint’ (Mandelbaum, 1991/1992: 97) and of ‘working through [. . .] the “trouble” in a virtual complaint sequence – one in which both the complaint and the apology are preempted, neither being said by its appropriate sayer’ (Schegloff, 2005: 468).
The participants nevertheless treat the matters being complained about as ones for which the co-present HCPs can be seen as responsible. Evidence is to be found in how the patients and companions work to minimise that attribution of responsibility by deflecting it to other agents (extract 1, lines 13–18, and extract 3a, lines 27–28); and in how the HCPs displace the complainable matter to one for which they cannot be seen as liable (extract 2b, lines 34–35), allude to a swift resolution (extract 1, line 23), commit to actions that may lead to a resolution (extract 3c, lines 80–81), and importantly, reassure the patients that they have their best interest at heart (extract 1, line 23; extract 2b, lines 34–35; and extract 3b, lines 49–50 and 52). We thus witness a somewhat paradoxical outcome whereby nascent complaints mobilise commitments to remedial actions and reassurance, but in the process, the one complaining ends up being treated as not complaining after all. How can we interpret these findings?
In her book Complaint! Ahmed (2021) investigated oral accounts of staff and students who had complained about (or had been treated by others as having complained about) bullying and harassment in UK universities. Based on those accounts, Ahmed discussed the ‘institutional mechanics’ entailed in variously discouraging, stopping and instrumentalising complaints. Although we do not see the same dynamics in the cases we have examined, we find it important to explore points of contact. In a hypothetical natural history of troubles (Emerson and Messinger, 1977), complaining in co-present interaction may be ‘the stage at which sometimes vague perceptions of something being wrong are cast into the public domain, in an effort to mobilize help in remedying the trouble’ (Drew and Holt, 1988: 399). Our findings suggest that this initial stage is also where a nascent complaint can be deactivated (or where such deactivation can be attempted) by treating a complainable matter as a less damaging object – a practical problem in need of a solution. This is made possible by the ways in which the patients and companions design their complaints as allusive, pliable objects in the first place, and even actively minimise the possibility of being heard as complaining about the HCPs (extract 1, lines 13–18; extract 3b, lines 43–44). In this context, the promissory quality that characterises the HCPs’ proposed remedies (extract 1, line 21; extract 2b, line 48; extract 3c, lines 80–81) appears to work as a tacit invitation not to make these complaints overt, based on trust that the staff will satisfactorily address conveyed concerns and unmet needs. The ‘institutional mechanics’ (Ahmed, 2021) entailed in containing nascent complaints are thus very much the joint product of patients’, companions’ and HCPs’ actions.
Our findings further resonate with Ahmed’s (2021) observation that complaints regularly attract negative responses and evaluations. For instance, they can be treated as ‘rocking the boat’ (Ahmed, 2021: 76), that is, as upsetting the status quo of presumably harmonious relationships within an institution; and they can be experienced as ‘sticky’ (as something that ‘sticks to you’ (Ahmed, 2021: 117)). Along these lines, prior research on a different kind of complaining (complaining about absent parties) has suggested that participants treat it as a dispreferred action because it can attract negative inferences about the complainer themself (Edwards, 2005). To guard themselves against such outcomes, complainers may only allude to, rather than state, a critical view about an absent party, thus giving recipients the options to either take it up and perhaps develop it further (Drew and Walker, 2009) or to dis-attend it (Mandelbaum, 1991/1992). Similarly, the patients and companions in our study make their dissatisfaction available without precisely pinpointing its locus, leaving this as a matter for inference. This enables the HCPs to respond in ways that keep the alluded-to complainable matters implicit. The other side of the coin is, nevertheless, the possibility that the virtual quality of implied complainable matters endows them with a degree of strength. That is, projecting the possibility of complaining may be a way of getting others to engage in remedial actions (Alshammari and Haugh, 2024; Ruusuvuori and Lindfors, 2009). In all these ways, the patients, companions and HCPs engage in a ‘micro-politics of social action’ (Drew, 2022), walking the fine line between raising complainable matters and ‘rocking the boat’ (Ahmed, 2021), and undertaking remedial actions in ways that concurrently avoid fully ratifying (and perhaps consolidating) what is clearly treated as a problematic object: a complaint.
Footnotes
Appendix: Transcription conventions ( Jefferson,2004 )

| Convention | Meaning |
|---|---|
| 01 02 |
Line numbers for each transcript line |
| Pat: OT4: |
Abbreviated pseudonym of speaker |
| (unsure) | Parentheses enclose words and sounds that are not completely clear from the recording and represent the transcriber’s best attempt |
| ((note)) | Double parentheses contain transcriber’s notes |
| Ov[er]lapping Ta[lk] |
Square brackets enclose talk that speakers produce at the same time [ indicates beginning of overlap ] marks end of overlap |
| . | Full stop for falling intonation. |
| , | Comma for slightly rising intonation |
| ¿ | Inverted question mark for rising intonation that is more marked than a comma, but less than a question mark |
| ? | Question mark for markedly rising intonation |
| _ | Underscore for level intonation |
| = | Equals sign for ‘latching’ – rapid movement between two TCUs |
| Cut o- | Hyphen for a cut-off word or sound |
| hh | Indicates out breath. More ‘h’s mark a longer out breath |
| .hh | Dot before an ‘h’ for in breath. More ‘h’s signify a longer breath |
| Stre::tched | Colon for extension of a sound in the middle or at the end of a word. More colons indicate a longer sound |
| Em |
Underlining for words or syllables that are hearably emphasised |
| °quiet° | Degree signs for talk that is produced quietly. More degree signs indicate whispering |
| LOud | Capital letters for a word or part of a word for loud delivery |
| ↑Raised pitch | Up arrows for raised pitch at the start or middle of a word |
| >faster< | Words enclosed by outwards facing chevrons have been produced noticeably more quickly than other talk from a given speaker |
| <slowly> | Words enclosed by inwards facing chevrons have been produced noticeably more slowly than other talk from a given speaker |
| £smile£ | Pound sign for word or part of word that is hearably produced as speaker is smiling |
Acknowledgements
We would like to thank the staff, patients, and companions who consented to being recorded. We are grateful to Ruth Parry for her overarching work in establishing and leading the VERDIS project and building and supporting the team that made this article possible. We thank an anonymous reviewer for their detailed and helpful comments on an earlier version of this article, and the Editor of Discourse Studies for his support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Creation of the data set for this study and earlier analyses were funded by The Health Foundation [Grant IDs: AIMS 1273316, AIMS 1273743/GIFTS 7210], an independent charity committed to bringing about better health and social care for people in the UK, and by the National Institute for Health Research Academy Career Development Fellowship to Ruth Parry: ‘Enhancing staff-patient communication in palliative and end of life care’ (Grant ID CDF-2014-07-046). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.