
Abstract
The standard process for starting anamnesis in the follow-up cancer consultation is for the doctor to ask a ‘How are you?’ question. This question gives the patient the opportunity to give a gloss of their general condition and offer the first topic of discussion. Findings in earlier analyses of US and UK data in a broad array of medical contexts show that the question is ambiguous and hence patients may interpret it as social rather than medical. A discourse analysis of a corpus of 28 video-taped consultations shows that the ‘How are you?’ question in the context of Dutch follow-up cancer consultations is consistently interpreted by both doctor and patients as a holistic medical question, making relevant a – frequently complex and nuanced – medically oriented response. We suggest that this difference may have to do with the interactional norms of hospital visits in the Netherlands, and with the specific contextual parameters of return visits, more specifically with follow-up cancer consultations, which affect the way the HAY question is placed, intended and understood.
Keywords
Prologue
This article is the result of a serendipitous finding in a research project on the interactional effects of the introduction of discussion tools in follow-up consultations in a major cancer centre in The Netherlands. When we began transcribing the data we had collected for this project, we noticed that they all but one opened in the same way: with a ‘How are you?’ question, the canonical opening of medical consultations that has been widely researched. What was striking, though, is that, at first sight, it seemed to us that all these questions were answered as requests for medical information. This outcome would not be in line with earlier research on ‘How are you?’ questions, which hinges on the ambiguity of the question. We therefore decided to see if we could validate our intuitive, pre-theoretical ideas about the data through a detailed investigation of the global and local interactional parameters of the encounter. A new research question had emerged (c.f. Edelsky, 1981) and this question is the departure point of this study.
Introduction
The Opening of medical consultations is generally achieved by (a variation on) the question ‘How are you?’ (see for example, Coupland et al., 1994; Frankel, 1995; Heritage and Robinson, 2006; Rogers and Todd, 2010). Coupland et al. (1994) for instance, found that 94% of the consultations they recorded in a geriatric outpatient clinic opened with this question. In the institutional, medical setting of the doctor-patient consultation the ‘How are you?’ question then may be seen to function as a verbal contextualisation cue (Erickson and Schultz, 1981; c.f. ‘bracketing’ device, Goffman, 1976) that physicians employ to signal and effectuate the transition from informal chit-chat towards the formal context of the consultation proper.
In non-institutional settings, ‘How are you?’ questions tend to fulfil a phatic, almost ritual function, intended to achieve bonding, rather than that they are genuine inquiries into the other’s state of health, as can be observed in for example, informal conversations in the United States (see for example, Coupland et al., 1992; Sacks, 1975). In his analysis of this type of question in informal social contexts, Sacks (1975) calls the question a ‘greeting substitute’, because it can both follow and replace an ‘ordinary’ greeting sequence. And like greetings, ‘ritual’ ‘How are you?’ usually appears in a reciprocal exchange sequence: as the first pair part of an adjacency pair that makes a second pair part sequentially relevant (Schegloff, 1986).
Informal, phatic ‘How are you?’ questions and their institutional (hoc loco medical) counterparts seem to be different moves, fulfilling different interactional functions. Openings of institutional events must be negotiated by the participants to ensure mutual orientation to the task-at-hand, and transitions from informal to institutional settings do not always proceed without a hitch. Ambiguity may arise with the question at the very beginning of medical consultations as to ‘where we are’ in the interaction (c.f. Erickson and Shultz, 1981). The context may be interpreted by one (or some) of the participants as ‘still social’ and the question as a form of/invitation for (more) phatic communication, while others may interpret the context as ‘now institutional’. This potential for hybridity as to the function of the question has been widely reported for Anglo-Saxon medical contexts, showing that, since the boundary between the social and the medical context at the start of the medical consultation is fuzzy and permeable, the opening question is sometimes being interpreted and answered as social, and sometimes as medical (e.g. Coupland et al., 1992, 1994; Frankel, 1984; Heritage and Robinson, 2006). As mentioned in the Prologue, these findings contradicted our intuitions about the data we collected for this study and has triggered the investigation that follows.
Data and method
The data for our research project on the interactional effects of the implementation of a discussion tool in follow-up cancer consultations were collected at the outpatient clinic of the head and neck cancer department of a specialised cancer hospital in the Netherlands. 1 One of the rooms at the outpatient clinic was equipped with a small, unobtrusively placed camera and microphone to record the consultations (see Figure 1).
The position of the camera in the consultation room.
The original dataset consisted of video recordings of 67 consultations with four different physicians, of which 21 recordings could not be used because of technical and/or language problems, or because the patients were involved in another Quality of Life study. This left 46 usable recordings. These were viewed to select the recordings that fit the focus of this study, that is, doctor-patient interaction in the routine follow-up cancer consultation. This meant the patients had to have finished treatment for a malignancy, and they had to have come in for their routine, scheduled follow-up consultation. Patients who did not meet these criteria were excluded from the study. This left a total of 28 routine follow-up consultations for analysis, with 18 (64%) male, and 10 (36%) female patients. A detailed transcription, including relevant prosodic, paralinguistic and nonverbal moves, was made of the videotapes of the consultations for analysis.
All but one consultation in our dataset opened with a ‘How are you?’ question. Patient responses varied, as can be seen in Table 1. This table differentiates between responses that orient towards wellness and those that do not; responses that include a complaint/distress, and those that do not; responses that were prefaced by delay (in the form of filled and unfilled pauses, see below) and those that were not; and combinations of these features.
Types of responses to the ‘How are you?’ question in standard follow-up cancer consultations.
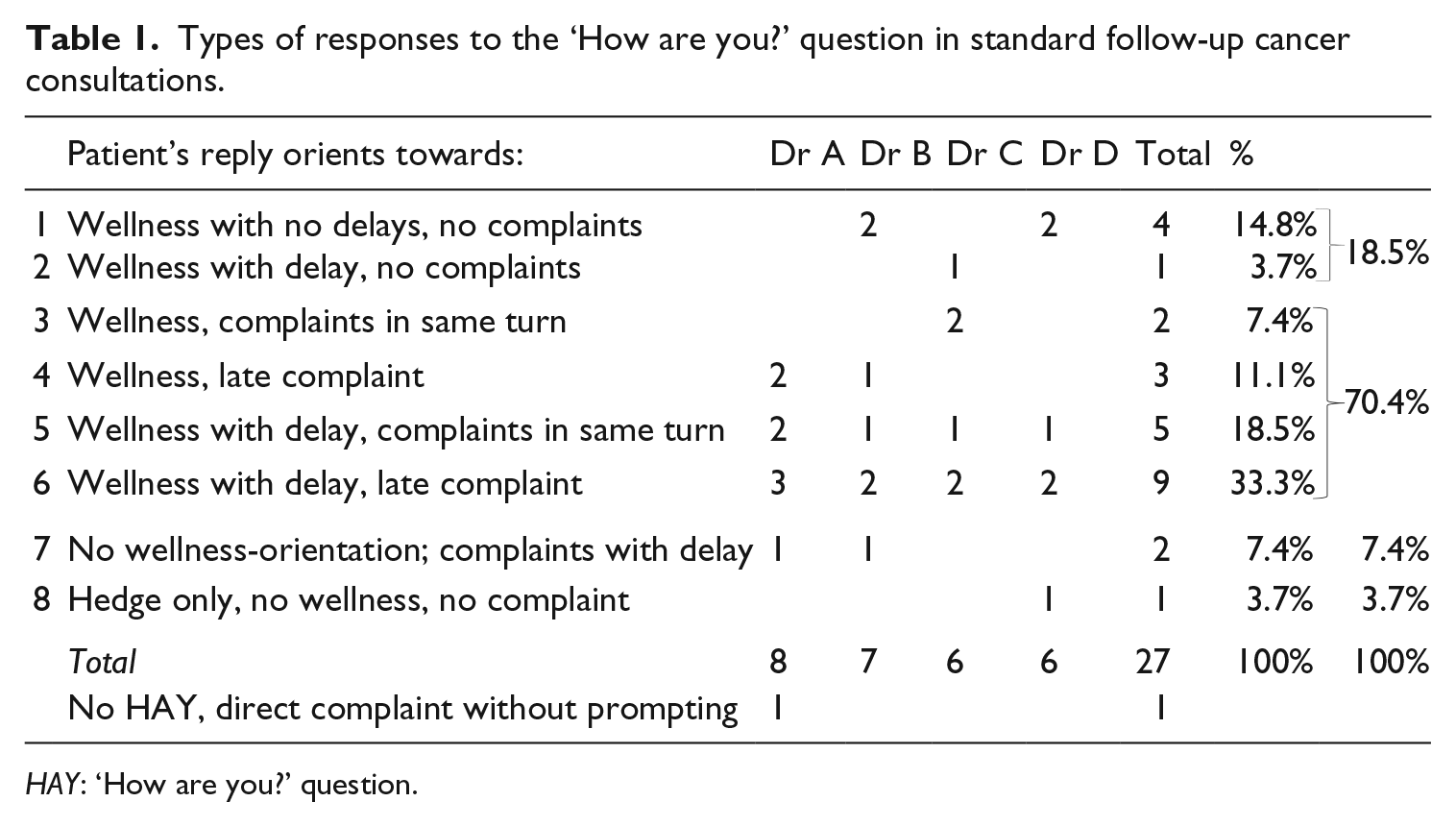
HAY: ‘How are you?’ question.
In our data, only two patients immediately respond with a negative response to the question (category 7 in Table 1), directly formulating distress or a complaint. Five patients responded with an unequivocal orientation to wellness, with no complaints surfacing in the rest of the consultation (categories 1 and 2). In the discussions of whether ‘How are you?’ questions and their responses can be seen as social/phatic or interactional/medical, earlier research has judged unequivocally positive and negative appraisals ‘to be more readily interpreted in a medical frame’ (Coupland et al., 1992: 221), and as non-phatic. In the current data, these patients’ initial gloss of wellness or distress, indeed, matches the information they give in the rest of the consultation, so there seems to be little reason to problematise these assessments.
In the majority of the cases, however, positive first glosses are combined with complaints: patients respond with an initial orientation towards wellness and then either immediately, in the same turn, or later in the consultation, voice a complaint (categories 3, 4, 5 and 6). This pattern mirrors the findings of Coupland et al. (1992, 1994), Frankel (1995) and Heritage and Robinson (2006), who observed that patients, immediately after claiming they are fine, frequently present problems, for example, with troublesome symptoms, or side-effects and after-effects of the treatment they received. This prompted their position that in wellness-oriented replies to ‘How are you?’ questions that are followed by complaints, the first-half of the response must be seen as oriented towards the social context rather than the medical one (e.g. Rogers and Todd, 2010), or at least as ambiguous between the two (Coupland et al. 1992, 1994). The patients in our data, however, consistently orient to the medical context in their response to the question, which led us to the research question for this article: can we pinpoint dimensions of the global, institutional and local, interactional parameters of the consultations in our data that account for the difference between our observations and earlier research?
To find an answer to this question, we will zoom in on relations between the interpretation of the ‘How are you?’ question in our data and interactional and contextual features of the particular speech event they derive from:
The interpretation of the question relative to the socio-cultural and institutional characteristics of the follow-up cancer consultation in the Dutch context (1); 2
The interpretation of the question relative to the context of the ‘return visit’ (2);
The response to the question relative to the intrinsic complexity of the question in the follow-up cancer consultation(3).
The interpretation of ‘How are you?’ relative to the socio-cultural and institutional parameters of the encounter
The influence of culture, ethnicity and concomitant discourse patterns in medical encounters has often been researched, for example, in an effort to identify barriers to establishing effective doctor–patient relationships (e.g. Schouten and Meeuwesen, 2006), but we are not aware of any studies that offer an analysis of the socio-cultural and institutional dimensions of the organisation of the encounter itself as instrumental in the discursive construction of the opening of the speech event ‘medical consultation’. We propose, however, that such an analysis could be helpful in answering our research question. Below, we will explore how routine procedures in the opening of the event may influence the interpretation of the ‘How are you?’ question.
Robinson (2013) describes four tasks that must be accomplished in order to establish a medical context: greeting, establishing identities, checking records and embodying readiness. If the ‘How are you?’ question is asked before these tasks have been completed, Robinson argues, the boundary between the social and the medical is not clear (c.f. Coupland et al., 1992, 1994; Frankel, 1984; Heritage and Robinson, 2006), that is, the medical context has not yet been fully established and this increases chances for a social interpretation of the question. Tasks 1, 2 and 4 from Robinson’s list are enacted as contextualisation cues (Gumperz, 1992), interactional tools by which the interactants co-construct ‘that something new is happening’ (Erickson and Shultz, 1981: 150). Contextualisation cues signal context changes and concomitant changes of ‘footing’ (participant alignment, for example, speaker and hearer rights and obligations; c.f. Goffman, 1979) and include changes in voice tone, pitch, and other features of speech prosody; changes in linguistic code, style, and topic; changes in the tempo and rhythmic organization of speech and body motion; changes in gaze direction and facial expression; [and] changes in number of speakers and listeners. (Erickson and Shultz, 1981: 148–149)
Major transitions in situational contexts, such as the transition from an informal conversational setting to a formal institutional one, are usually marked by a great redundancy of contextualisation cues, clusters of them being used in tandem to mark, and thereby facilitate, the transition.
When in the Netherlands patients come in to see a physician, they meet in the waiting room. The doctor walks over from the consultation room and calls out the patient’s name. Both parties shake hands, exchange greetings and – chatting on the way – together they go back to the consultation room. This practice differs from the standard procedure in most Anglo-Saxon contexts. Here participants typically meet in the consultation room where either doctor or patient is already seated.
Since doctors routinely have a look at patients’ medical records before they go and meet them, we may determine that in our data the first three of Robinson’s tasks – greeting, establishing identity, checking records – have already been accomplished when doctor and patient enter the consultation room. Task 4 – embodying readiness – is then performed through a cluster of, in some cases individually different, contextualisation cues. Typically, doctor and patient sit down on either side of the doctor’s desk. Dr A, Dr B and Dr C look at the screen while the patient sits down, conveying what Robinson (1998: 109) calls ‘the doctor doing bureaucracy’, and thus establishing a clear medical context. They then turn to the patient and, making eye contact, ask Hoe gaat het? (‘How are you doing?’).
3
They often add a temporal focus to the question on the time between the last and the current visit, (e.g. intussen or in de tussentijd = ‘in the meantime’) (c.f. Coupland et al., 1994), referencing the context of the return visit (see section
In these data, the physician interacts with a patient who went through excision and radiotherapy of a carcinoma on the tonsil 11 months before the consultation.
Data 1
[Participants have met in the waiting room, have exchanged greetings and have entered the consultation room]
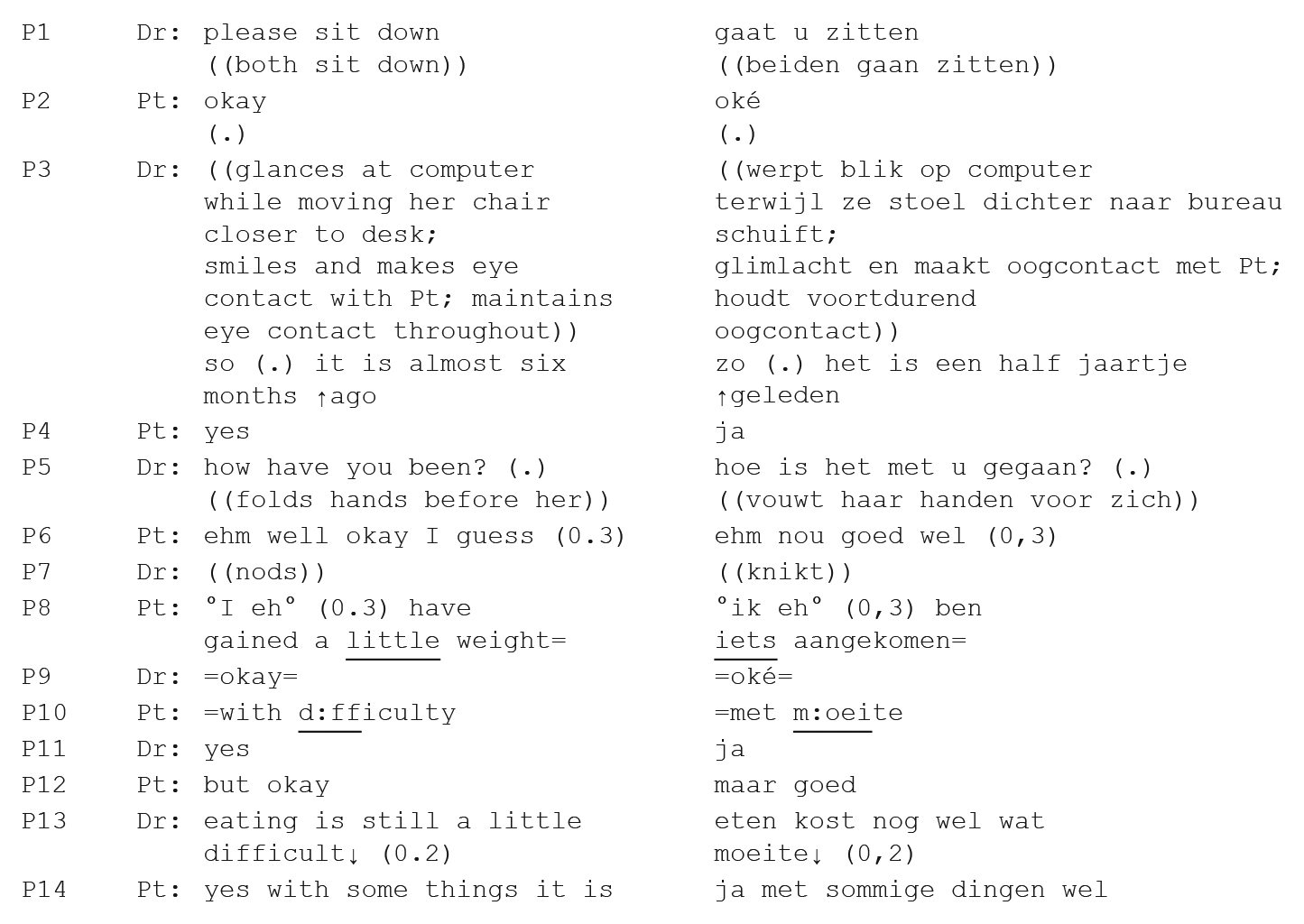
In this data, the doctor uses a cluster of contextualisation cues to mark the transition to a medical context: she glances at the screen, she establishes eye contact with patient, she uses the discourse marker zo (‘so’), which according to Bolden (2009: 974) ‘demonstrates that speakers [. . .] indicate the status of the upcoming action as “emerging from incipiency” rather than being contingent on the immediately preceding talk’. She also explicitly refers to the time that has gone by since patient’s last visit het is een half jaartje geleden (‘it is been almost six months’), which highlights their shared history of medical encounters. Only then, after patient has accepted the timeframe with ja (‘yes’), does she ask the ‘How are you?’ question – with a time-lapse marker in the tense form: hoe is het met u gegaan (lit: ‘how has it gone with you’, gloss: ‘how have you been’). Patient responds to the question with an overall self-assessment goed (‘okay’), which, because of the delay ehm nou (‘uhm well’) and the hedge wel (‘I guess’), cannot be marked as unequivocally straightforward. Patient then elaborates by saying he has gained weight – a positive signal in the medical sense in head-and-neck cancer patients. The choice of weight gain as a topic here indeed shows that patient’s initial gloss should be interpreted as a medical orientation to the ‘How are you?’ question. As patient himself adds (P10, P14): the weight gain was not easy (eating is still difficult), due to after-effects of the treatment.
Data 1 shows how the doctor uses a wide range of multimodal cues to mark the transition to the medical context. As a result, the ‘How are you?’ question, constituting the transition to the anamnesis (i.e. the business-at-hand of the consultation), is solidly embedded in the medical context. Patient’s response consists of a hedged positive gloss followed by a next-turn elaboration that clearly shows a medical orientation.
To summarise, the medical interpretation of the ‘How are you?’ question in our dataset is supported by the density of multimodal contextualisation cues that routinely accomplish three out of four of the tasks that Robinson (2013) sets out for the creation of a medical context before the question is asked. This makes the boundary between the social and medical context in our dataset much less fuzzy and permeable than in comparable, Anglo-Saxon, contexts as reported on in earlier research.
The interpretation of ‘How are you?’ relative to the context of the ‘return visit’
The follow-up cancer consultation is by definition a return visit (c.f. Gafaranga and Britten, 2005; Heath, 1981; Robinson, 2006). This feature of the encounter has an impact on for example, what questions are relevant and how they are formulated. As illustrated in Data 1, the ‘How are you?’ questions in our data are often accompanied by a time marker which stresses the ‘return’ aspect of the visit. In our dataset, doctors referred to this aspect in 19 out of 28 consultations. In six cases, patients also refer to the return-visit context in their answers. These time markers steer the discourse to information on how the patient has been since their last visit to the doctor, through references to relevant time periods by means of phrases like de laatste tijd (‘lately’) and in de tussentijd (‘in the meantime’). In this way, doctors and patients discursively co-construct the medical context, as is illustrated in Data 2.
The patient in Data 2 had a laser excision of a melanoma on the head 3 months before followed by two operations, including excision of the lymph nodes in the neck a month later.
Data 2
[Participants have met in the waiting room, have exchanged greetings and are entering the consultation room]
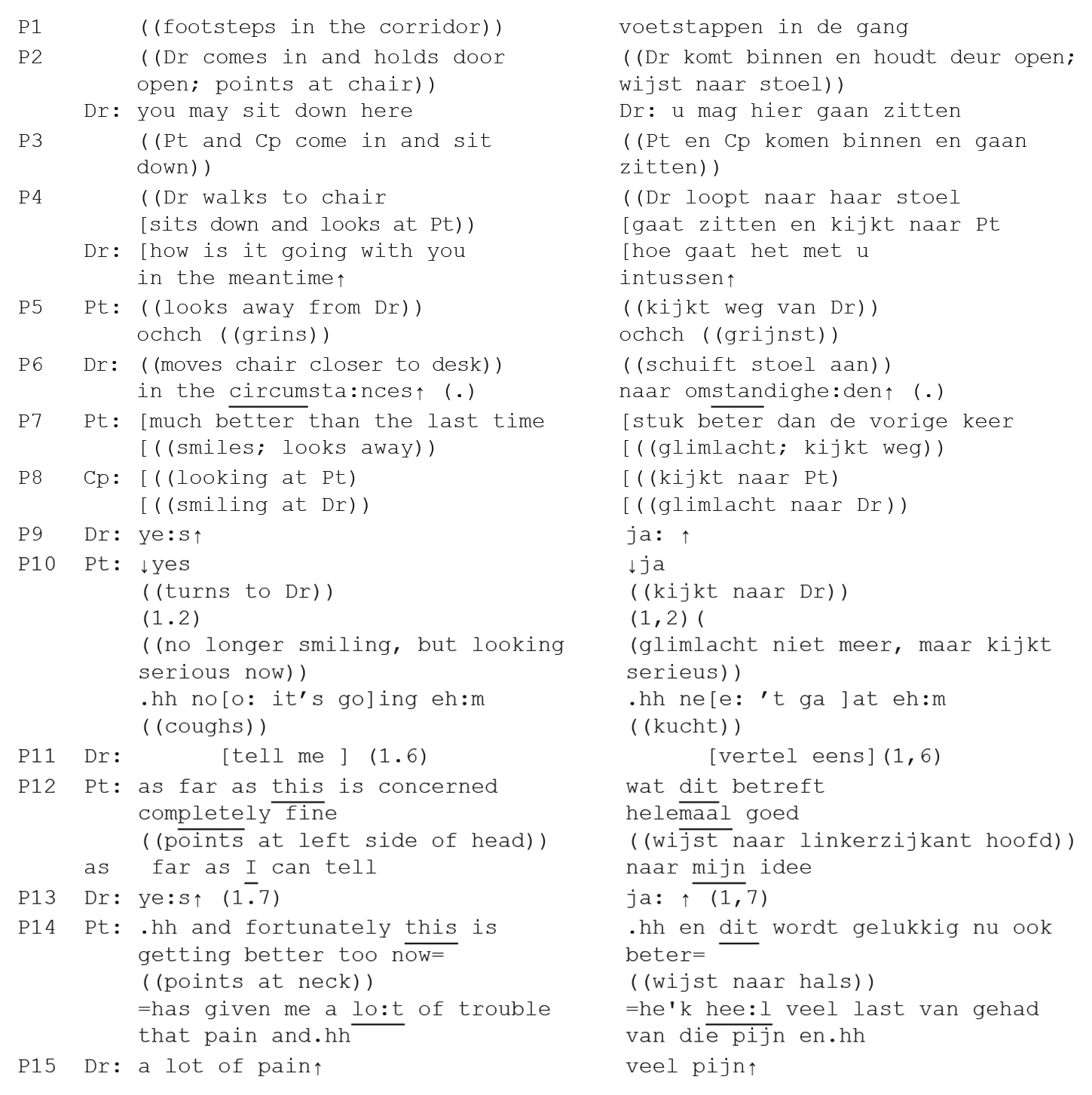
In Data 2, the physician references the context of the return visit with the phrase intussen (‘in the meantime’), which she attaches to her question hoe gaat het met u (‘how is it going with you’). Patient first responds with a vocal hedged delay, ochch. At the same time he grins at the doctor, but he also looks away, apparently not committing himself to a clear response. The doctor interprets patient’s reaction as a trouble premonitor (Jefferson, 1980, 1988) and qualifies her original question, making it more specific by referring to the circumstances (P6: omstandigheden) of the patient, who has only recently undergone an operation to remove a melanoma on his skull. Patient mirrors the doctor’s orientation to the return aspect of the encounter with a temporal reference of his own, to the last time he saw doctor: stuk beter dan de vorige keer (‘much better than the last time’), before continuing with more details of his medical condition (P10–14).
To summarise, the references by both participants to the time aspect of the return visit and relevant medical circumstances, plus patient’s layered response show that from the very start patient oriented towards the medical context of the encounter.
The response to ‘How are you?’ relative to the intrinsic complexity of the question for cancer patients
Just as in earlier research on the subject, patients in our data tend to begin their answers to doctors’ ‘How are you?’ openings with a holistic positive gloss, even if they disclose various complaints and troubles in same or following turns. The presence of the positive gloss is often interpreted as evidence for the reply to be (partly) social/phatic rather than medical and/or as evidence for the idea that the troubles resistance which is reported to be typical of ordinary interaction is spilling over into the medical consultation (Coupland et al., 1992; Coupland et al., 1994; Heritage and Robinson, 2006; Rogers and Todd, 2010). It is not seen as truthful and informative, but as a social gambit, which is (later) followed by the ‘real’ answer: the complaint. As observed earlier, this is argued to be the result of the ambiguity of the status of the ‘How are you?’ question, with the patient interpreting the question as a social inquiry (Coupland et al., 1994; Rogers and Todd, 2010).
We propose that in the context of the follow-up cancer consultation the combination of a positive gloss followed by a complaint may have a different cause altogether: for cancer patients, formulating an answer to a ‘How are you?’ question may not be completely straightforward (similarly to for example, geriatric patients; see Coupland et al., 1992), for various reasons.
First, it is not always easy to determine what exactly the question refers to: does it point to the patient as defined by their disease – so restricted to the area affected by and treated for the malignancy? Does it refer to the after-effects of the treatment, to the patient’s psychosocial situation, or is it meant holistically – referring to both the patient’s biomedical and psychosocial condition?
Moreover, just as in ordinary conversations, patients need to decide whether the hearer – in this case the doctor – is, at this point in time, the person they wish to share this information with, and whether the hearer is willing and able to deal with their response (Sacks, 1975). So patients need to decide which particular aspect of their physical/mental/emotional condition – whether good or bad – they wish or need to share with this particular physician at this particular moment in this particular consultation: are troubles that have been discussed and treated on earlier occasions still or again relevant? Do they want to share psychosocial problems with their oncologist, or would they prefer to discuss them with their GP, their loved ones, or another professional? Is the small side-effect worth mentioning, or will they simply cope?
And finally, answering a ‘How are you?’ question in a follow-up cancer consultation is always related to the context of (recently) having been treated for cancer, which conjures up all sorts of difficulties in terms of how to formulate the answer: how is the patient doing compared to what? Compared to how patients felt before they had cancer, after diagnosis, directly after treatment, at the last follow-up consultation? So the question would need to be interpreted in relation to time and circumstances. Doctors generally acknowledge this patient conundrum, as is illustrated in Data 2 earlier, where the doctor makes specific reference to the omstandigheden (‘circumstances’), that is, the fact that the patient has very recently been operated on to remove a melanoma, to pinpoint the scope of the question. Patient, then, interprets the question and explicitly formulates his answer as compared to his condition at the last visit to Doctor: de vorige keer (‘the last time’).
But these omstandigheden (‘circumstances’) can also be interpreted more broadly, to include the wider social and biomedical circumstances of patients. Coupland et al. (1992) report that the elderly people who were interviewed in their study, when asked how they were, responded in relation to their circumstances: being very old, they suffered from the complaints elderly people tend to suffer from, which both they themselves and the interviewers were well aware of. So a positive response would be given, taking into account the baseline of ‘positive’ that can be held to apply to the very old (c.f. Bredmar and Linell, 1999). Cancer patients in follow-up consultations might make similar judgements when answering ‘How are you?’ questions: a positive reply might take into account the baseline of ‘positive’ that is relevant and to be expected in the circumstances of recovering from cancer.
Thus, when patients give seemingly contradictory answers to the ‘How are you?’ question, they may be conveying exactly what they mean and feel – that is, on the whole they are/feel OK, but/and they suffer from one or more complaints (c.f. Heath, 1981). This might simply be because there is no unequivocal answer to be given: under the circumstances they may generally be doing relatively OK, but there may (still) be specific issues (e.g. after-effects, problems with medication, anxiety) that distress them, as is illustrated in Data 3.
The patient in this data had an excision and radiotherapy of a tumour in the supraglottis 3 years and 6 months ago.
Data 3
[Participants have met in the waiting room, have exchanged greetings and are entering the consultation room]
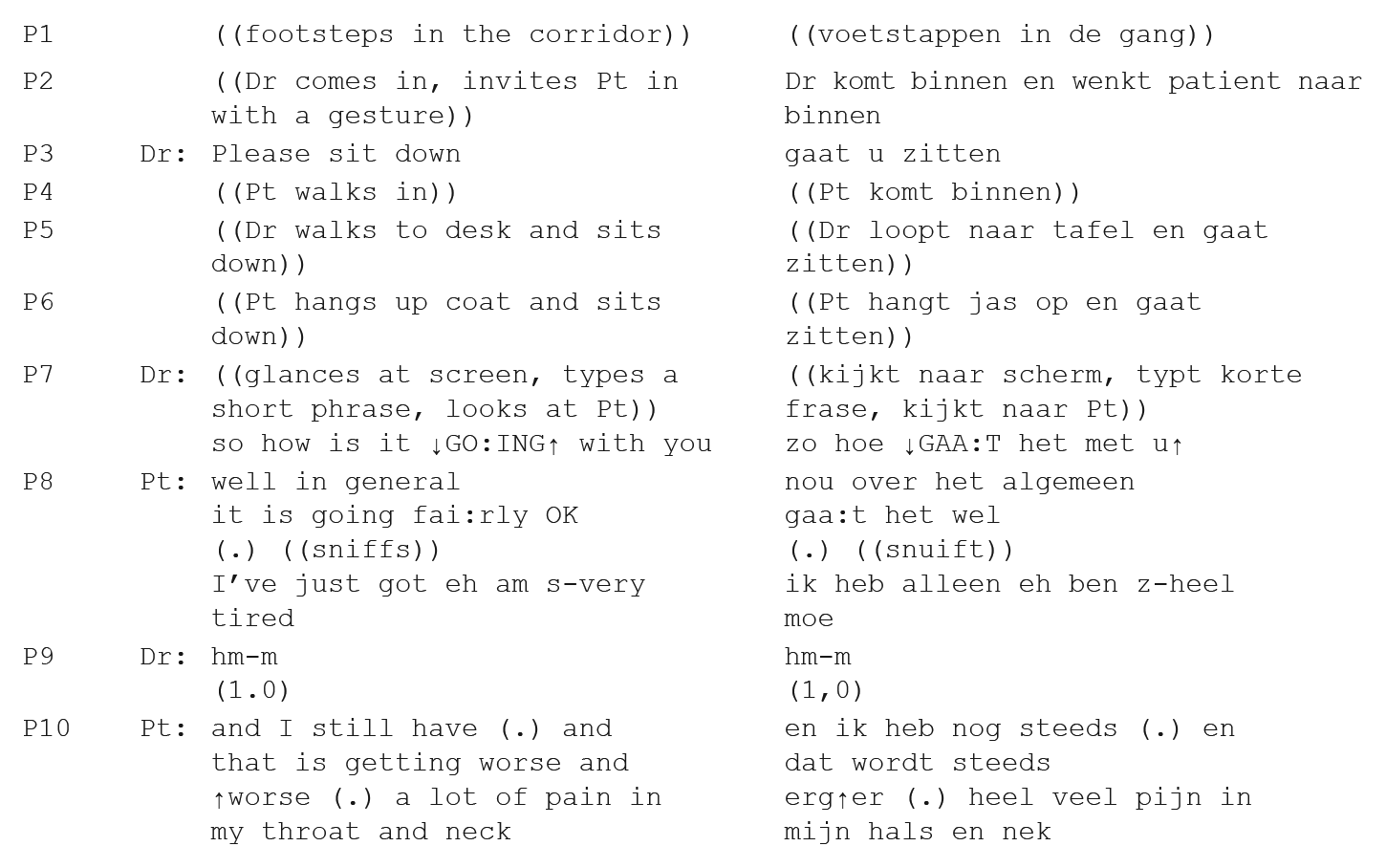
When doctor and patient have seated themselves at either side of doctor’s desk, embodying readiness, the physician opens with the discourse marker zo (‘so’) as a cue to indicate a shift to the next topic (Bolden, 2009; Raymond, 2004), before asking hoe GAA:T het met u (‘how is it GO: ING with you’), with strong emphasis on the main verb. Patient delays his answer with nou (‘well’) – a complexity marker, signalling that the answer may not be equivocal or simple to give (Mazeland, 2016) – and formulates a layered answer, giving a moderately positive gloss (over het algemeen gaa:t het wel – ‘in general things are fairly OK’) of his general condition. This references a holistic overall assessment of his condition, indicating that – within the frame of normality of having been treated for cancer (c.f. Bredmar and Linell, 1999) – he is doing reasonably well. Then, preceded by delay in the form of a short pause and a sniff, patient limits the scope of the positive gloss with ik heb alleen (‘I’ve just got’), delay (eh), and a first complaint, ben alleen z-heel moe (‘only [I] am s-very tired’), thus creating an exception to his expression of general relative wellness. Doctor responds with a continuer (hm-m), inviting patient to elaborate, and patient then adds another complaint. By constructing this complex response – combining a positive gloss followed by specific complaints – patient negotiates the complex force of the question in relation to his situation, which can only be done justice to by means of this seeming contradiction.
Additional evidence for our position that the patients in our dataset orient towards the complexity of answering their doctors’ ‘How are you?’ questions is reflected in the fact that most wellness-oriented patient responses begin with a form of delay (15/24), consisting of unfilled pauses and pauses filled by for example, u: hh and nou (‘well’) (c.f. Data 1 and Data 2). This is even more salient for responses that are later followed by a complaint (14 delayed responses out of a total of 19 wellness-oriented responses that are followed by a complaint).
Delay has been argued to preface dispreferred responses (see for example, Brown and Levinson, 1987; Jefferson, 1980), to delay or resist trouble (Heritage, 1998; Jefferson, 1980), or to mitigate a face-threatening act (Brown and Levinson, 1987). However, various studies into discourse markers have also shown that delay before a reply may be related to the fact that the question may not be one-dimensional, may therefore be difficult to answer and that formulating a response requires some thought (e.g. Button and Casey, 1984; Coupland et al., 1994; Mazeland, 2016). Taking this into consideration, it is likely that the difficult choices patients need to make in formulating the answer to their doctor’s ‘How are you?’ question are reflected in the heavy use of delay; it shows that the answers require some thought, are ‘searched for’ (Button and Casey, 1984: 177) and may be complicated (c.f. Mazeland, 2016). So, far from being phatic, automatic, social responses, the responses in our data seem to be well-considered, complex and institutionally oriented.
Summary and discussion
Contrary to findings in much previous research on the ‘How are you?’ question in medical contexts that report confusion about the social or medical interpretation of the question (see for example, Coupland et al., 1994; Frankel, 1984; Rogers and Todd, 2010), we conclude that the ‘How are you?’ question opening the consultations in our study was interpreted as a medical inquiry in all instances. Patients constructed the question as a first concern elicitor that makes a response relevant that refers to the medical condition of the patient (c.f. also Gafaranga and Britten, 2005; Heath, 1981).
We identified a number of dimensions of the global and local contextual parameters of the specific encounter that may account for our findings. First of all, the wider socio-cultural context might influence the interpretation of the question. Dutch routine procedures create affordances for three of the four tasks that establish the medical context (greeting, establishing identity and checking records; Robinson, 2013) to be completed before doctor and patient enter the consultation room. The fourth task, embodying readiness is realised by means of a wide range of other contextualisation cues that the physicians use to effectuate and facilitate the transition from social to medical context, such as discourse markers, gaze and reading patients’ files (c.f. e.g. Coupland et al., 1994; Heath, 1981; Robinson, 2013), which afford a medical interpretation of ‘How are you?’ questions (Heritage and Robinson, 2006; Robinson, 2013).
Also, much of the earlier research does not seem to differentiate between different types of consultations in their analysis of ‘How are you?’ openings (e.g. Coupland et al., 1994; Frankel, 1995; Rogers and Todd, 2010). We argue, however, that such differentiation is relevant to the interpretation of the question (see also Gafaranga and Britten, 2005; Heath, 1981). The fact that the follow-up cancer consultation is by definition a return visit is consequential for the interpretation of the question. Doctors topicalised this feature of the consultations in the data by the use of a temporal addendum, such as ‘since your last visit’. Also, since – in contrast to for example, acute GP consultations – in return visits, doctor is familiar with the complaints that have brought the patient to the consultation room, patients tend to interpret ‘How are you?’ questions as designed to refer to this knowledge and as soliciting a medical reply that is relevant to patient’s illness (Heath, 1981). Heath (1981) and Gafaranga and Britten (2005) analyse ‘How are you?’ as a typical way to elicit medical information from patients in return consultations.
Finally, we argue that research into the interpretation of ‘How are you?’ questions should include an analysis of the nature of the patient group that the data focus on. For cancer patients (and also for other groups of patients, such as for example, those with chronic conditions, or geriatric patients, c.f. Coupland et al., 1992) ‘How are you?’ is a complex question to respond to. This complexity shows in the pervasive and sometimes heavy use of delay at the start of response turns and in the often seeming contradiction between a positive first gloss and the expression of complaints either in same turn or later in the consultation.
Conclusion
We propose that in order to understand what happens in the openings of medical consultations and to account for differences in patient interpretation of the ‘How are you?’ question, we have to adopt a context-sensitive approach and move beyond analysis of the question-response adjacency pair. We need to both:
Zoom out and scrutinise global, institutional contextual parameters of the speech event, taking into account the importance of the inclusion of multimodal data;
Zoom in to the local interactional parameters of the speech event as they surface in the formulation of the question and the (possibly) inherent complexity of the answer for the particular patient group under investigation.
Footnotes
Appendix 1
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.