
Abstract
This study identifies the effect of six social correction methods on vaccine skeptics’ intention to take COVID-19 vaccine. In April–May 2021, we conducted a 3 (corrector on Twitter: ordinary person vs medical doctor vs nurse) × 2 (correction strategy: priming vs rebuttal) + 1 (control: misinformation only) between-subjects online experiment with 569 vaccine skeptics in the United States. Results show that exposure to priming-based corrections performed by a corrector, regardless of their expertise, is positively associated with intention to take COVID-19 vaccine if the information shared by the corrector is perceived to be trustworthy. This is evident among those with high or moderate vaccine skepticism. What is only evident among those with moderate vaccine skepticism is that exposure to corrections using priming (any corrector) or rebuttal (ordinary person or medical doctor) is positively associated with intention to take COVID-19 vaccine if the respondents perceived that the corrector was an expert.
Introduction
Vaccine hesitancy is the reluctance or refusal to receive vaccines despite their availability (Truong et al., 2022). In 2019, the World Health Organization (2019) identified vaccine hesitancy as one of the ten threats to global health. Two years later, vaccine hesitancy was recognized as a major contributor to COVID-19 deaths in the United States (Simmons-Duffin and Nakajima, 2022). One important factor associated with vaccine hesitancy is vaccine skepticism (Truong et al., 2022). Vaccine skepticism is characterized by suspicions about vaccine safety, effectiveness, and importance (Larson et al., 2016). Such suspicions can make people hesitate to take vaccination for themselves or others. For instance, vaccine skeptics are less likely to receive (Solís Arce et al., 2021) or allow their children to receive vaccines (Joslyn and Sylvester, 2019; Tan et al., 2022).
Although vaccine skepticism is not a new phenomenon (The College of Physicians of Philadelphia, 2022), it has become a much more significant threat with the spread of vaccine misinformation on social media. Research shows that vaccine misinformation is so prevalent on social media (Center for Countering Digital Hate, 2021; Stolle et al., 2020; Wang et al., 2019) that it is responsible for COVID-19 vaccine skepticism and hesitancy (Pierri et al., 2022). Considering that vaccine skepticism is fueled by the spread of vaccine misinformation on social media throughout the COVID-19 pandemic, the WHO (n.d.), the US Centers for Disease Control and Prevention (CDC) (n.d.), and the US Surgeon General (Murthy, 2021) have issued guidelines on addressing COVID-19 misinformation on social media.
One way to address vaccine misinformation on social media is for social media users—both experts and non-experts—to engage in social correction, which the abovementioned guidelines have emphasized. Research shows that exposure to social correction can reduce misinformation beliefs (Bode et al., 2020; Bode and Vraga, 2018; Walter and Murphy, 2018) and encourage others to perform corrections (Tully et al., 2020). Moreover, studies show that corrections from expert sources were more effective than those from non-expert sources in reducing misperceptions (Vraga et al., 2022; Vraga and Bode, 2017; Zhang et al., 2021).
Several publications (e.g. Arora et al., 2022; Bautista et al., 2021a, 2021b; Murthy, 2021, WHO, n.d.) have advocated for more health care professionals to correct health misinformation considering that these groups of professionals are the most trusted source of COVID-19 information (Malik et al., 2020). Currently, there is limited research on the impact of corrections made by health care professionals on health beliefs. Several studies have examined the impact of expert sources on misinformation beliefs (e.g. Vraga and Bode, 2017; Zhang et al., 2021). However, these studies have conceptualized expert sources as health organizations rather than health care professionals and did not involve a health-related outcome.
This study examines the effect of various social correction methods on vaccine skeptics’ intention to take COVID-19 vaccine to add knowledge about the effect of expert and non-expert information sources in correcting health misinformation. First, we draw on previous health misinformation research (e.g. Tully et al., 2020; Van der Meer and Jin, 2020; Vraga and Bode, 2017, 2018, 2021; Zhang et al., 2021) to identify how the six social correction methods (see Table 1), that differ on explicit expertise of the corrector (i.e. ordinary person vs medical doctor vs nurse) and correction strategy (i.e. priming vs rebuttal), affect intention to take COVID-19 vaccine. Second, we draw on source credibility theory (Hovland et al., 1953) to examine whether perceived trustworthiness and perceived expertise mediate the effect of social correction on intention to take COVID-19 vaccine. Finally, based on previous work (Tan et al., 2022; Zhang et al., 2021), we examine how vaccine skepticism moderates the mediating effect of perceived trustworthiness and perceived expertise on the effect of social correction on intention to take COVID-19 vaccine.
Description of simulated Twitter posts.
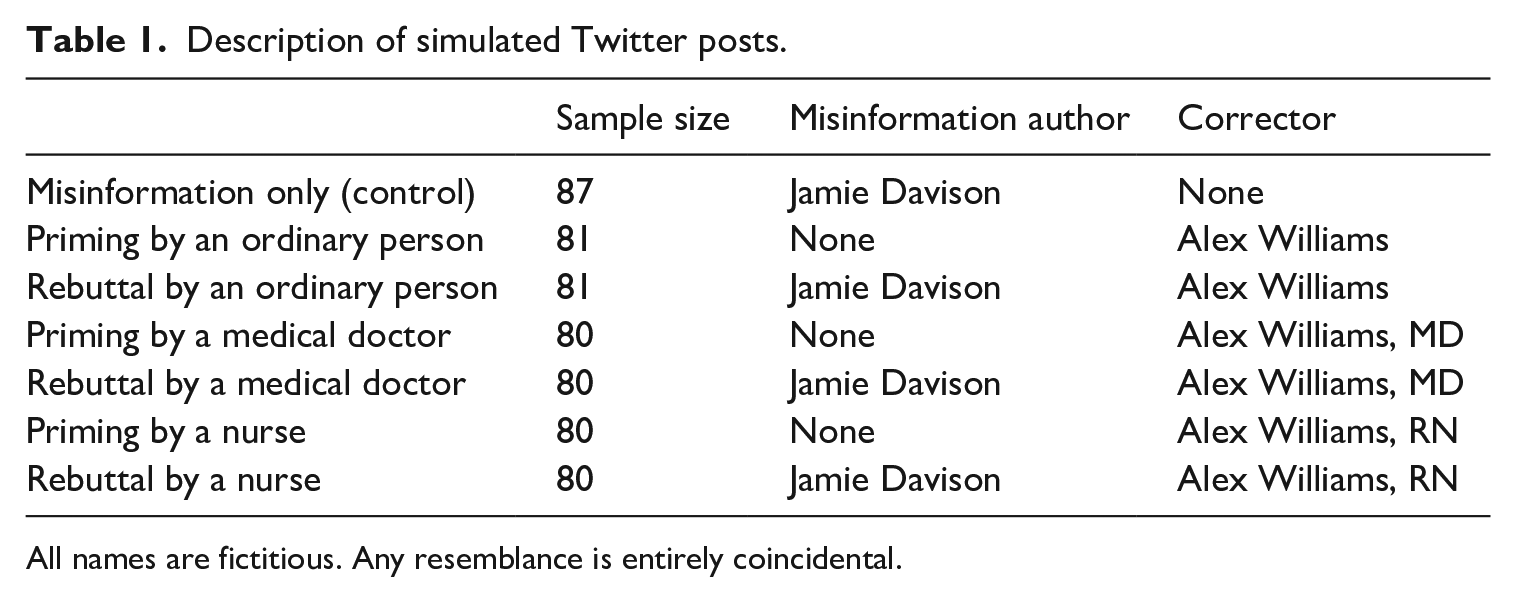
All names are fictitious. Any resemblance is entirely coincidental.
Literature review
Vaccine misinformation during the COVID-19 pandemic
Aside from being an infectious disease that has affected millions of people globally, the COVID-19 pandemic is also an infodemic wherein the overabundance of information on social media has fueled the spread of misinformation (Hao and Basu, 2020). Among the numerous COVID-19 misinformation spreading on social media, misinformation about COVID-19 vaccines is prevalent because of public skepticism on its fast development speed (less than a year) and the novelty of the technology (messenger RNA [mRNA]) involved in developing the vaccines (Hamel et al., 2021a). Scholars noted that the spread of vaccine misinformation throughout the COVID-19 pandemic is associated with greater vaccine skepticism and hesitancy (Pierri et al., 2022), which might have contributed to preventable COVID-19 deaths (Gisondi et al., 2022). Given the need to address vaccine misinformation on social media, this study examines the effect of six social correction methods aimed at correcting COVID-19 vaccine misinformation (see Table 1) on increasing vaccine skeptics’ intention to take the vaccine.
Social correction of health misinformation on social media
Social correction refers to the correction of misinformation by other people (Bode and Vraga, 2018; Kligler-Vilenchik, 2022; Vraga and Bode, 2018). Social correction of health misinformation on social media is at work when social media users, regardless of expertise, correct health misinformation on social media platforms. In the case of COVID-19 misinformation, both experts and non-experts are encouraged to correct misinformation. In fact, US Surgeon General Vivek H. Murthy (2021) encourages the general public and health care professionals to address health misinformation to build a healthier information environment by not only avoiding sharing health misinformation but also performing social correction of misinformation on social media.
There are several methods by which people can engage in social correction. In a meta-analysis conducted by Walter and Murphy (2018), people can either correct misinformation through priming (i.e. providing the correction as a forewarning and without the explicit presence of the misinformation) or rebuttals (i.e. providing a corrective reply to the misinformation post), with the latter being more effective than the former. Building upon Walter and Murphy’s (2018) work, Bautista et al. (2021a) added that priming and rebuttals on social media could be public (i.e. when the correction is publicly visible) or private (i.e. when the correction is not visible to everyone).
Although social correction is a viable method to curb the spread of health misinformation (Walter and Murphy, 2018; Walter et al., 2021), recent work suggests that few people actually correct misinformation (e.g. Bode and Vraga, 2021; Tandoc et al., 2020). Considering that correcting health misinformation should be a collective effort involving various stakeholders (Donovan et al., 2021; Murthy, 2021), scholars have urged health care professionals to be more proactive in correcting health misinformation, especially on social media (Gisondi et al., 2022; O’Connor and Murphy, 2020; Rubin, 2019). Fortunately, recent studies suggest that health care professionals are correcting health misinformation on social media. For instance, a 2020 survey among 377 US medical doctors and nurses found that at least 90% have corrected health misinformation on social media by using public priming or public rebuttal (Bautista et al., 2022a), and that they intend to do this, especially when their employers and colleagues support it (Bautista et al., 2022b). Research also shows that, despite intrapersonal (e.g. lack of time and self-efficacy), interpersonal (e.g. harassment and bullying), and organizational (e.g. lack of organizational support and social media training) barriers, health care professionals are motivated to correct health misinformation on social media to uphold their ethical obligations of doing good and preventing harm (Bautista et al., 2021b).
Most studies to date suggest that rebuttals made by health institutions (e.g. CDC and WHO), compared with non-health experts (operationalized as social peers, ordinary social media users, or news media), are likely to reduce misperceptions (Vraga and Bode, 2017), improve attitudes toward vaccines (Zhang et al., 2021), and successfully debunk misinformation (Van der Meer and Jin, 2020). However, research that compares the impact of corrections made by people—both health care professionals and ordinary people—using different correction strategies is limited. If we are to encourage both experts and non-experts to correct health misinformation on social media (Murthy, 2021; Vraga and Bode, 2020), there is a need to determine what correction strategy would work. This study intends to contribute to the literature by providing empirical evidence on whether correcting health misinformation on social media (either by priming or rebuttal), is a worthwhile effort for both health experts and non-experts. We propose the following research question:
RQ1: What is the effect of different social correction methods on vaccine skeptics’ intention to take COVID-19 vaccine?
The mediating role of perceived trustworthiness and perceived expertise
Source credibility theory posits that information consumers can be persuaded by a credible information source (Hovland et al., 1953). It conceptualizes credibility as the combination of the information consumers’ perceptions of the source’s trustworthiness (i.e. the information presented by the source can be relied on) and expertise (i.e. the information comes from a source that provides valid assertions). Accordingly, when information consumers deem an information source trustworthy and an expert, they are more likely to accept the information (Kareklas et al., 2015).
Research shows the role of perceived trustworthiness and perceived expertise on health-related issues. For example, parents are more likely to trust vaccine-safety information when it comes from their children’s doctor (Freed et al., 2011). Moreover, perceived trustworthiness of physicians is positively associated with the intention to take COVID-19 vaccine among Italian adults (Prati, 2020). Besides, health-conscious respondents reported a higher knowledge gain when exposed to nutrition label information that comes from a dietician (i.e. a credible source) rather than a celebrity or an ordinary person (Dong, 2015). Likewise, Phua (2016) found that diet and exercise self-efficacy can be predicted by the spokesperson’s competence (i.e. expertise) and trustworthiness. Finally, respondents exposed to misinformation correction from a high-trustworthy source had lower reliance on misinformation to answer questions about vaccination (Pluviano et al., 2020).
This study extends past research to understand how source credibility theory relates to people’s intention to take COVID-19 vaccine in the context of misinformation research. Both medical doctors and nurses play a crucial role in the dissemination of corrections about COVID-19 vaccine misinformation (Hamel et al., 2021b). US adults consider health care professionals (the majority of whom are medical doctors and nurses; Laughlin et al., 2021) the most trusted source of COVID-19 information (Malik et al., 2020). However, reports suggest that nurses are rarely considered a source of health information in mainstream media (Mason et al., 2018) despite having the highest ethical rating for more than two decades (Brenan, 2023). A recent review also noted that despite being equally important, nurses are perceived to be inferior or have lower social status and prestige than medical doctors (Rodríguez-Pérez et al., 2022). As a result, nurses’ invisibility in public discourse and perceived lack of social prestige can affect the public’s perception of nurses’ expertise and trustworthiness when it comes to addressing health issues, such as vaccine misinformation. Therefore, we further delineate the explicit expertise of the corrector by differentiating a medical doctor from a nurse as the corrector.
There is also limited research that examines perceived trustworthiness and perceived expertise as mediators. Previous works primarily treated these constructs as moderators (e.g. Pluviano et al., 2020) or used them as independent variables to determine their direct effects on health-related beliefs (e.g. Mai et al., 2021; Prati, 2020; Sui and Zhang, 2021). There is a need to treat these constructs as mediators in this study because exposure to information (whether it contains misinformation or corrections) cannot fully explain information consumers’ behavior since they also engage in information processing, such as ascertaining the credibility of the information (Jiang et al., 2021; Soffer, 2021; Vraga and Bode, 2018). This is supported by previous works wherein perceived trustworthiness (Naujoks and Benkenstein, 2020; Praxmarer, 2011; Schneider et al., 2021; Vraga and Bode, 2018; Willemsen et al., 2012) and perceived expertise (Naujoks and Benkenstein, 2020; Praxmarer, 2011; Willemsen et al., 2012)) were found to be statistically significant mediators. Following the source credibility theory, aside from the explicit expertise of the corrector, it is also important to consider information consumers’ perceptions of the information source’s trustworthiness and expertise because these can predict health-related outcomes (Kareklas et al., 2015), such as intention to take COVID-19 vaccine. Therefore, this study aims to determine whether perceived trustworthiness and perceived expertise mediate the effect of social correction methods on intention to take COVID-19 vaccine. We propose the following research question:
RQ2: Will perceived trustworthiness and perceived expertise mediate the effect of different social correction methods on vaccine skeptics’ intention to take COVID-19 vaccine?
The moderating role of vaccine skepticism
The Internet is an instrumental and accessible source of health information for people. However, it is plagued with poor-quality health information (Zhang et al., 2015). Social media platforms have become vaccine misinformation hubs due to the proliferation of vaccine skeptics that post anti-vaccine content (Wang et al., 2019). For instance, vaccine skeptic posts from the social media pages of Daily Wire (by Ben Shapiro) and Children’s Health Defense (founded by Robert F. Kennedy) have been shown to have more user engagement than reputable news organizations (Goldstein, 2022). Moreover, 65% of anti-vaccine content on Facebook and Twitter originates from notable vaccine skeptics known as the Disinformation Dozen (Center for Countering Digital Hate, 2021). With vaccine skepticism presenting as a major deterrent to the acceptance of vaccination as a public health intervention, there is a need to understand how vaccine skepticism influences efforts to correct vaccine misinformation on social media.
Research suggests that vaccine skepticism, as a concept, has been used in two ways. First, it was used as a predictor of health-related beliefs. For instance, vaccine skepticism has been found to have a negative association with attitude toward vaccines (e.g. Seddig et al., 2022) and intention to take vaccines (e.g. Honora et al., 2022; Kim et al., 2022). Second, it was used as a moderator. For instance, Zhang et al. (2021) examined whether the effect of various fact-checking labels on vaccine attitudes differed among those with high or low vaccine skepticism. Their results suggest that the level of vaccine skepticism did not influence such relationships. Another study by Tan et al. (2022) examined whether the relationship between confidence in the government’s handling of the COVID-19 pandemic and vaccination intent differed based on the level of vaccine skepticism (i.e. high or low). Contrary to Zhang et al. (2021), Tan et al. (2022) found that such a relationship is evident only among those with high vaccine skepticism.
In this study, we consider vaccine skepticism as a moderator to identify whether the effect of social correction methods (in consideration of the mediators mentioned earlier) on intention to take COVID-19 vaccine differs based on the level of vaccine skepticism. As emphasized by Horne et al. (2015), there is a need for studies that evaluate interventions that persuade vaccine skeptics to receive vaccines, especially those that target the high vaccine skepticism group. Although social correction might work in reducing health-related misperceptions (Walter and Murphy, 2018; Walter et al., 2021), some scholars argue that such interventions might not readily work for those with high vaccine skepticism as corrections might lead to a backfire effect (Ecker et al., 2022; Horne et al., 2015; Swire-Thompson et al., 2020; Ten Kate et al., 2021). Considering that vaccine skepticism is a potential moderator and several studies have used it as a moderator, this study examines whether vaccine skepticism moderates the mediating effect of perceived trustworthiness and perceived expertise on the effect of social correction methods on intention to take COVID-19 vaccine. We propose the following research question:
RQ3: Will the mediating effect of perceived trustworthiness and perceived expertise on the effect of social correction methods on intention to take COVID-19 vaccine differ based on vaccine skeptics’ level of vaccine skepticism?
Figure 1 shows the research model that reflects the research questions.
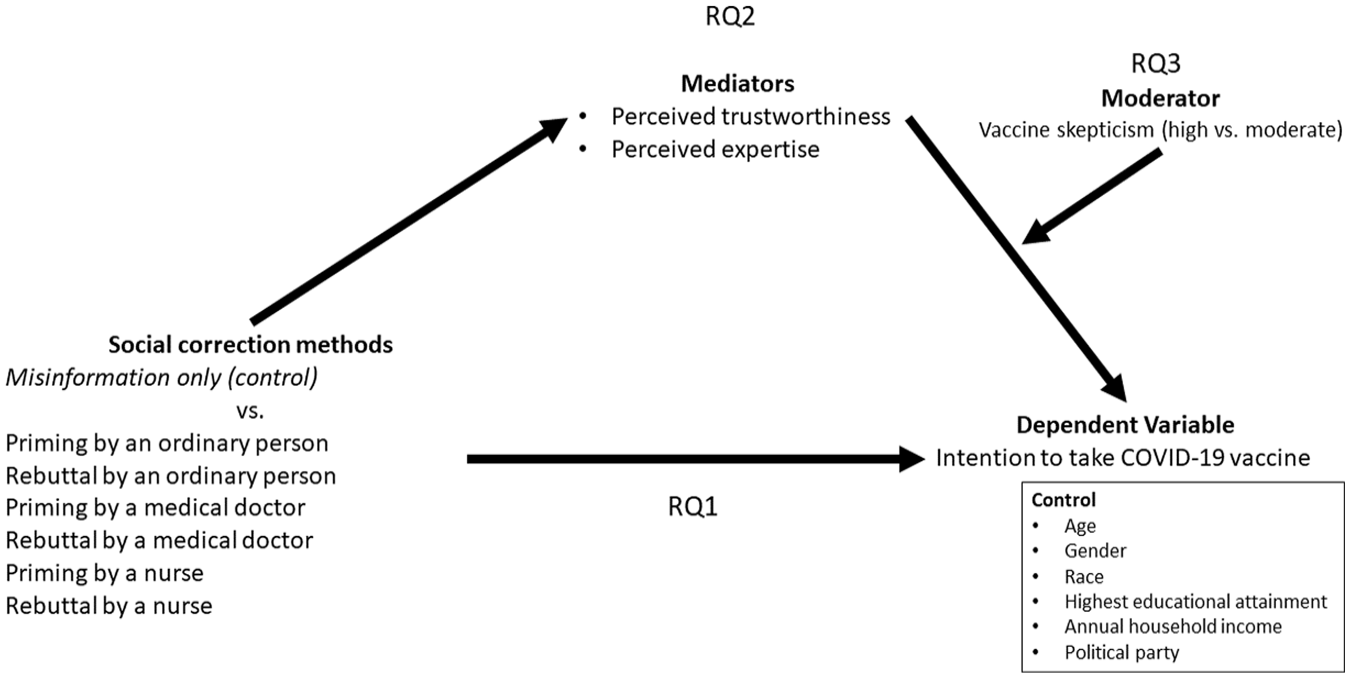
Research model.
Method
Design and data collection
After receiving approval from The University of Texas at Austin’s institutional review board (STUDY00000845), a Qualtrics online survey experiment was conducted in April–May 2021 by recruiting US adults through Amazon Mechanical Turk. Data collection was conducted around the time when all US adults became eligible to receive a COVID-19 vaccine (Hunnicutt, 2021). Although Amazon Mechanical Turk is not a platform used to recruit a nationally representative sample, relevant misinformation studies (e.g. Anspach and Carlson, 2020; Bode and Vraga, 2015; Lee et al., 2022) have recruited respondents from it since its respondent pool is more diverse than those of university students and it is a cost-effective means to test research models that are in the early stages of development.
Experiment flow
Figure 2 presents the flow of the experiment. First, potential respondents were asked to answer a series of screening questions (see Appendix 1). Eligible respondents are those who are US residents, aged ⩾ 18, vaccine skeptics (see the “Measurement” section for more details on identifying and classifying vaccine skeptics), Twitter users (frequently and always), non-health care workers (even their family members; vaccine acceptance is higher among health care workers and can influence family members to take it; Shekhar et al., 2021), and have not taken a COVID-19 vaccine. Eligible respondents provided consent to participate in the study. Then, they were asked for additional background information, such as gender, annual household income, race, highest educational attainment, and political party.
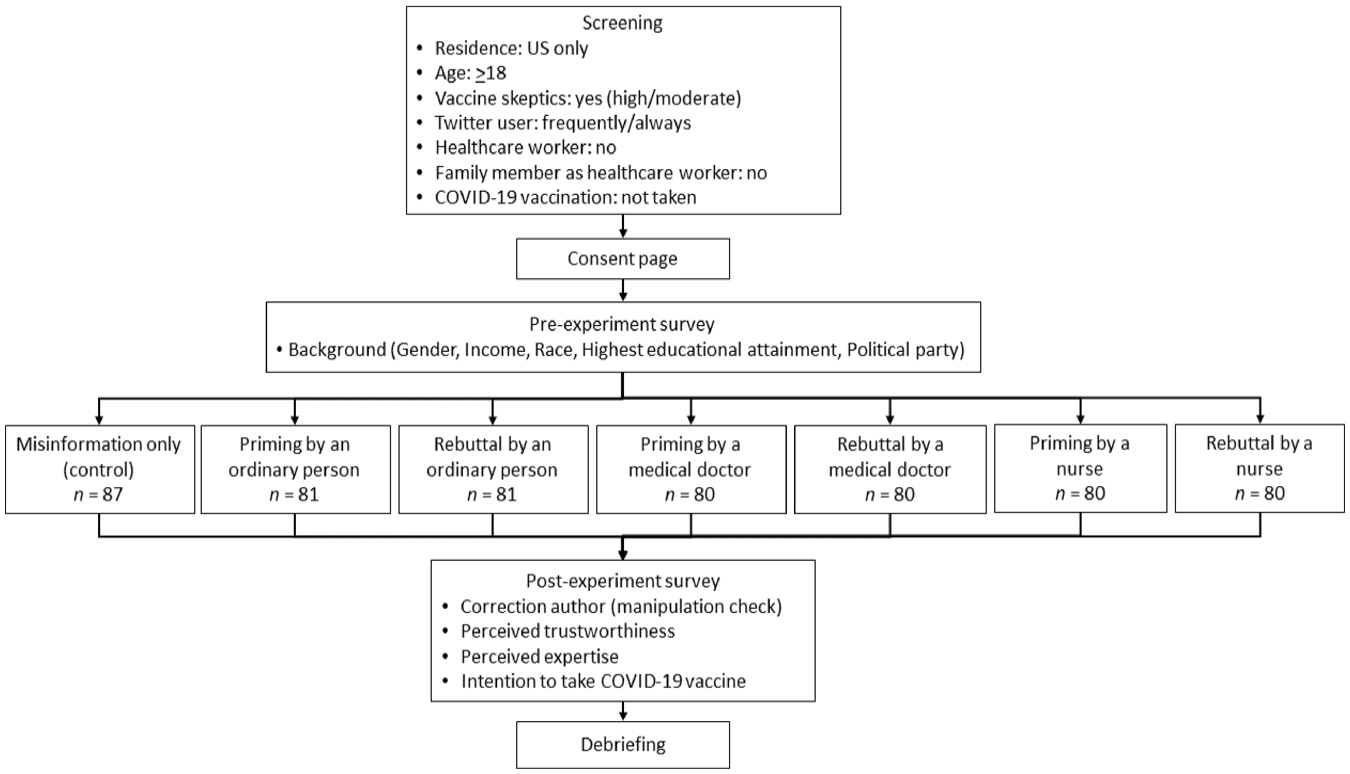
Experiment flow.
Following the background questionnaire, respondents were randomly assigned to read one of the seven simulated Twitter posts (one misinformation only group as the control and six social correction methods as the experimental groups). Table 1 shows a description of the simulated Twitter posts, while Appendix 1 shows the screenshots of the Twitter posts. We chose Twitter as the social media platform in this study because health care professionals tend to use Twitter to correct health misinformation on social media (Bautista et al., 2021a). The Twitter posts were manipulated based on the explicit expertise of the corrector (ordinary person vs medical doctor vs registered nurse) and correction strategy (priming vs rebuttal). The content of the Twitter posts focused on misinformation wherein COVID-19 mRNA vaccines (i.e. Pfizer and Moderna) change a person’s DNA. We selected this misinformation because it is one of the ten reported vaccine-related misinformation that has been fact-checked (McCarthy, 2021). A more important consideration is that the CDC (2021) provides a clear and concise correction to this misinformation on their website, which was instrumental in designing the simulated Twitter posts. The resulting Twitter post per social correction method conforms to the recommended practice of citing a highly credible information source (i.e. CDC) to support the correction (Ecker et al., 2022; Vraga and Bode, 2020). To reduce the effect of confounders, the names (i.e. Jamie and Alex) and profile pictures (i.e. nonhuman pictures) of the Twitter profiles were designed to be gender-neutral, and the number of retweets (i.e. 6) and likes (i.e. 10) were similar for all posts.
After exposure to the assigned stimulus, respondents answered a single multiple-choice question asking about the corrector’s name and/or designation as a manipulation check (Appendix 1). Passing the manipulation check means that the respondent could identify if the corrector on the Twitter post is an ordinary person, medical doctor, or nurse (those who failed the manipulation check were not excluded from the study; Aronow et al., 2019). The manipulation check item is followed by items measuring perceived trustworthiness, perceived expertise, and intention to take COVID-19 vaccine (see the “Measurement” section for more details). Finally, respondents were directed to a debriefing page that reminded them that vaccines do not alter their DNA and mRNA vaccines work with the body’s natural defenses to safely develop immunity to COVID-19.
Sample
A total of 3094 respondents answered the screening questions. Among the 577 respondents who were eligible to participate, we analyzed the data from 569 respondents who completed the survey. Following Aronow et al. (2019), data from the three respondents who failed the manipulation check were retained. The sample size per group ranged from 80 to 87 (see Table 1). The analytic sample size of 569 exceeded the estimated sample size of 341 based on G*Power (Faul et al., 2009; F tests = analysis of covariance [ANCOVA], effect size = .25 for medium, power = .95, numeratordf = 6, number of groups = 7, number of covariates = 11).
The respondents’ mean age was 36.35 years old (SD = 9.71), and they were mostly male (64%) and White (72%). Most had a bachelor’s degree (62%) and an annual household income of US$30,000–59,999 (46%). Most self-identified as democrat (53%) followed by republican (40%) and others (7%). Although the six experimental groups (85–93%) had more respondents with higher educational attainment (i.e. at least a bachelor’s degree) than those in the control group (misinformation only group; 73.6%; X2(24) = 39.12, p = .03), all groups were similar in terms of age, F(6, 562)= .38, p = .89; gender, X2(12) = 15.05, p = .24; race, X2(30) = 36.39, p = .20; annual household income, X2(18) = 16.98, p = .53; and political party identification, X2(12) = 10.15, p = .60.
Measurement
Appendix 1 provides a list of the items used in the study.
Perceived trustworthiness
Perceived trustworthiness (M = 5.17, SD = 1.37) was measured using five items adapted from the work of Vraga and Bode (2018). Respondents rated if the information presented to them by the misinformation author (control group) or corrector (experimental groups) is novel/new, useful, interesting, trustworthy, and credible on a 7-point Likert-type scale (1 = strongly disagree; 7 = strongly agree). The items had excellent reliability (McDonald’s Ω = .91).
Perceived expertise
Perceived expertise (M = 5.11, SD = 1.31) was measured using three items adapted from the work of Zhang et al. (2021). Respondents rated if the author of the Twitter post (misinformation author for control group and corrector for experimental groups) “is knowledgeable about vaccines,” “has a good track record of providing information about vaccines,” and “has expertise in vaccines” on a 7-point Likert-type scale (1 = strongly disagree; 7 = strongly agree). The items had good reliability (McDonald’s Ω = .89).
Vaccine skepticism
We used Zhang et al.’s (2021) method of identifying and classifying vaccine skeptics. As part of the screening questions, respondents were asked about their opinion on the statement, “The health risks of vaccines outweigh the benefits.” To mask the true purpose of the study, other statements were also included, for example, “Genetically modified (GMO) foods increase cancer risks” and “Climate change is a hoax made by the government for profits.” For all statements, respondents were asked to select “definitely true,” “probably true,” “probably false,” “definitely false,” or “unsure.” Those assigned to the high vaccine skepticism group (n = 351; 62%) answered “definitely true” and “probably true” while those assigned to the moderate vaccine skepticism group (n = 218; 38%) answered “probably false” and “unsure.” Those who answered “definitely false” were non-eligible for the study since they have low vaccine skepticism.
Intention to take COVID-19 vaccine
One item was used to assess respondents’ intention to take COVID-19 vaccine (i.e. I intend to take COVID-19 vaccine once it is available; M = 5.03, SD = 1.84). The item included the phrase “once it is available” because at the time of data collection (mid-April–early May 2021), there were still issues about the availability of vaccines in certain parts of the United States (Rattner, 2021). As such, we would not want to assume that it is something that is immediately available. A 7-point Likert-type scale was used to indicate their response (1 = strongly disagree; 7 = strongly agree).
Control variables
Respondents’ age, gender, race, highest educational attainment, annual household income, and political party were entered as control variables.
Data analysis
IBM SPSS Statistics 26 (hereafter SPSS) was used to manage and analyze the data. Exploratory data analyses consisted of descriptive statistics (mean, standard deviation, and percentage), chi-square, t-test, analysis of variance (ANOVA), and two-way ANCOVA. To test the model and answer the research questions, we used Model 14 of Hayes’ PROCESS Macro (version 4) plugin for SPSS (Hayes, 2021). In determining the effect of each social correction method, the misinformation only group was assigned as a reference group considering its role as the study’s control group and in consultation with previous experiments in correcting health misinformation (e.g. Mourali and Drake, 2022; Van der Meer and Jin, 2020’; Vraga and Bode, 2021). Unstandardized regression coefficients (B) were derived from 10,000 bootstrap samples. Results with p < .05 or a 95% confidence interval (95% CI) that did not cross zero were statistically significant.
Multicollinearity was not a concern since the values for tolerance (T > .20) and variance inflation factors (VIFs < 5) were within the normal range (Podsakoff et al., 2012) for the predictors of intention to take COVID-19 vaccine: perceived trustworthiness (T = .26, VIF = 3.81), perceived expertise (T = .26, VIF = 3.80), and vaccine skepticism (T = 1.00, VIF = 1.01).
Results
Table 2 provides descriptive results for the main variables of the study. ANOVA results indicate differences between study groups for perceived trustworthiness and perceived expertise. Tukey’s honestly significant difference (HSD) post hoc test reveals that those exposed to priming by an ordinary person, medical doctor, and nurse as well as rebuttal by an ordinary person and medical doctor had significantly higher perceived trustworthiness and perceived expertise as compared to those exposed to misinformation only (control group). On the other hand, no significant differences between groups were noted for intention to take COVID-19 vaccine and the proportion of those with high vaccine skepticism. Supplemental analysis shows that none of these constructs were significantly different when the control group was excluded from the analysis.
Descriptive results.
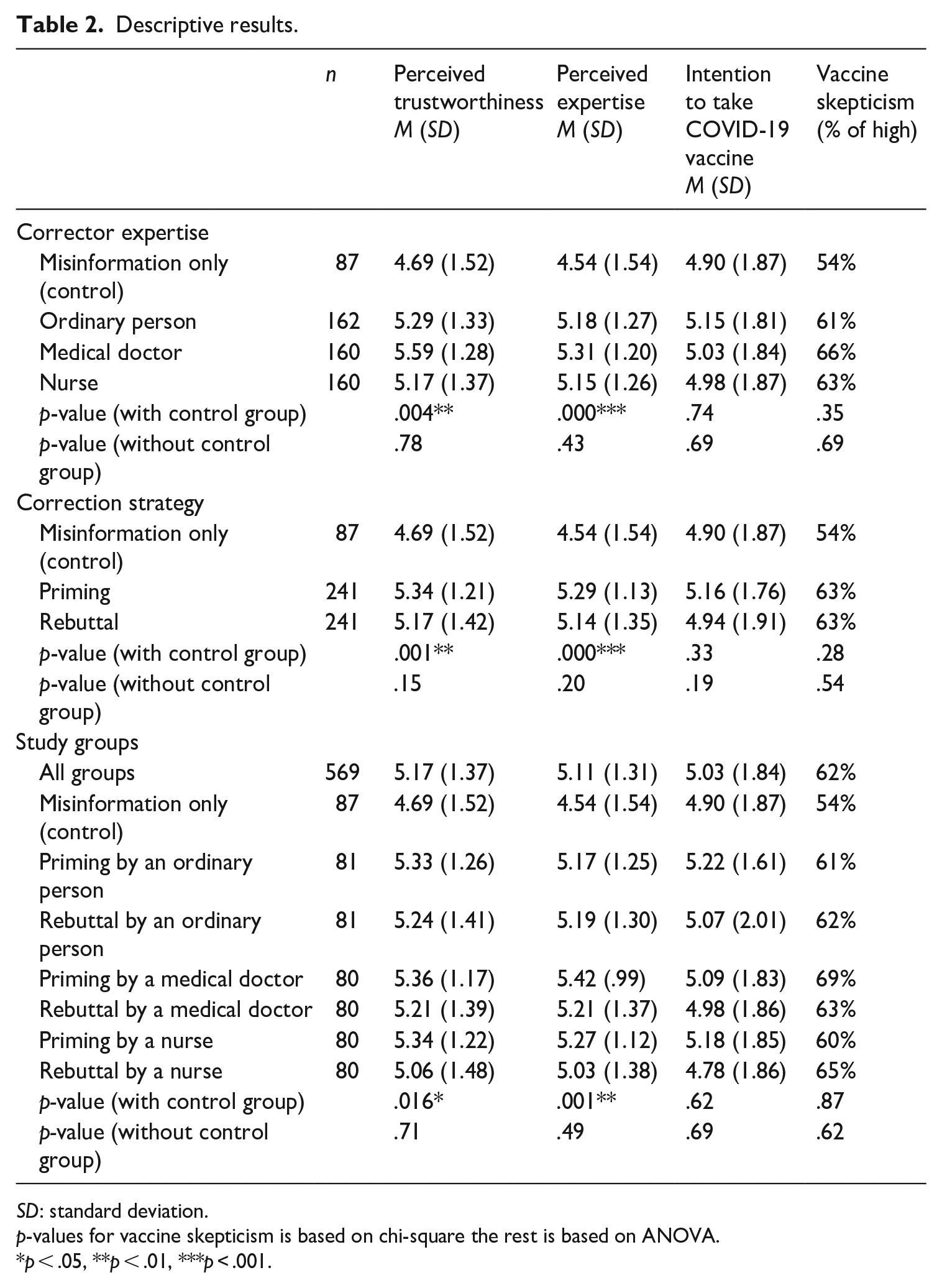
SD: standard deviation.
p-values for vaccine skepticism is based on chi-square the rest is based on ANOVA.
p < .05, **p < .01, ***p < .001.
Two-way ANCOVA was also performed to identify main and interaction effects of corrector expertise (i.e. ordinary person vs medical doctor vs nurse) and correction strategy (i.e. priming vs rebuttal) on intention to take COVID-19 vaccine. Perceived trustworthiness, F(1, 473) = 90.79, p = .000, η2 = .16; perceived expertise, F(1, 473) = 21.04, p = .000, η2 = .04; and vaccine skepticism, F(1, 473) = .02, p = .89, η2 = .00, were entered as covariates. Results show that corrector expertise, F(2, 473) = .86, p = .42, η2 = .00; correction strategy, F(1, 473) = .11, p = .75, η2 = .00; and their interaction, F(2, 473) = .29, p = .75, η2 = .00, had no effect on intention. Results are consistent even when the control group was included in the analysis.
Effect of social correction methods on intention to take COVID-19 vaccine
RQ1 asked about the effect of social correction methods on vaccine skeptics’ intention to take COVID-19 vaccine. As shown in Table 3, only priming by an ordinary person and nurse did not influence intention to take COVID-19 vaccine. Despite statistical significance, the other methods produced a negative effect, which means that exposure to rebuttal by an ordinary person (B = –.43, p = .04), medical doctor (B = –.51, p = .02), and nurse (B = –.45, p = .04), including priming by a medical doctor (B = –.50, p = .02), resulted in a lower intention to take COVID-19 vaccine.
Direct effect results.
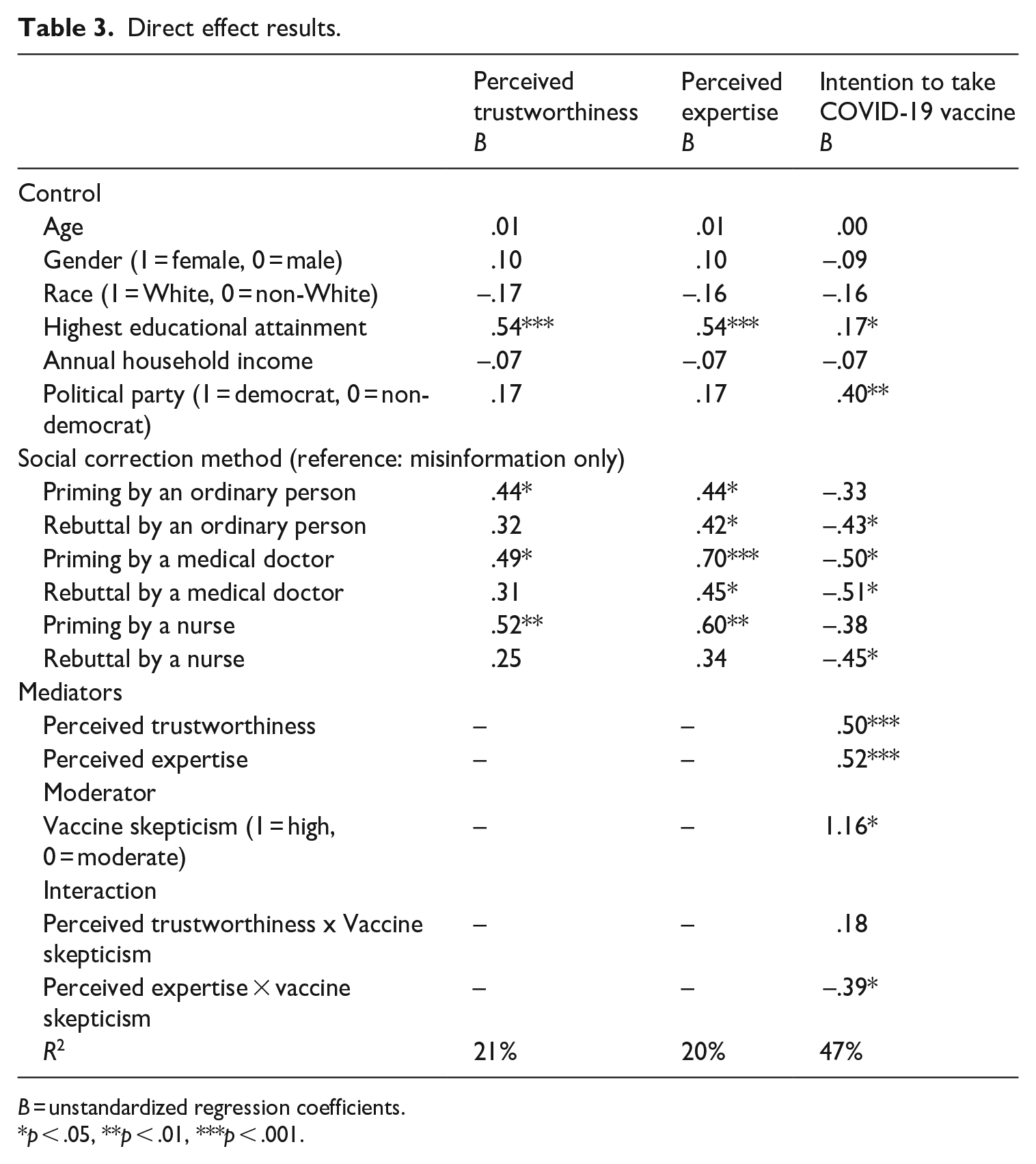
B = unstandardized regression coefficients.
p < .05, **p < .01, ***p < .001.
Mediation and moderation results
RQ2 asked whether perceived trustworthiness and perceived expertise mediate the effect of social correction methods on vaccine skeptics’ intention to take COVID-19 vaccine while RQ3 asked whether the mediation results will differ based on the level of vaccine skepticism. In general, Table 4 indicates the presence of mediation for most of the experimental groups (i.e., priming by an ordinary person, medical doctor, and nurse, including rebuttal by an ordinary person and medical doctor) since the mediating effect of perceived trustworthiness and perceived expertise reversed the non-significance (priming by an ordinary person) or negative direct effects of social correction methods (for priming by a medical doctor and nurse, including rebuttal by an ordinary person and medical doctor) on intention to take COVID-19 vaccine. We also found that the level of vaccine skepticism moderated the mediating effect of perceived expertise only.
Predicting intention to take COVID-19 vaccine
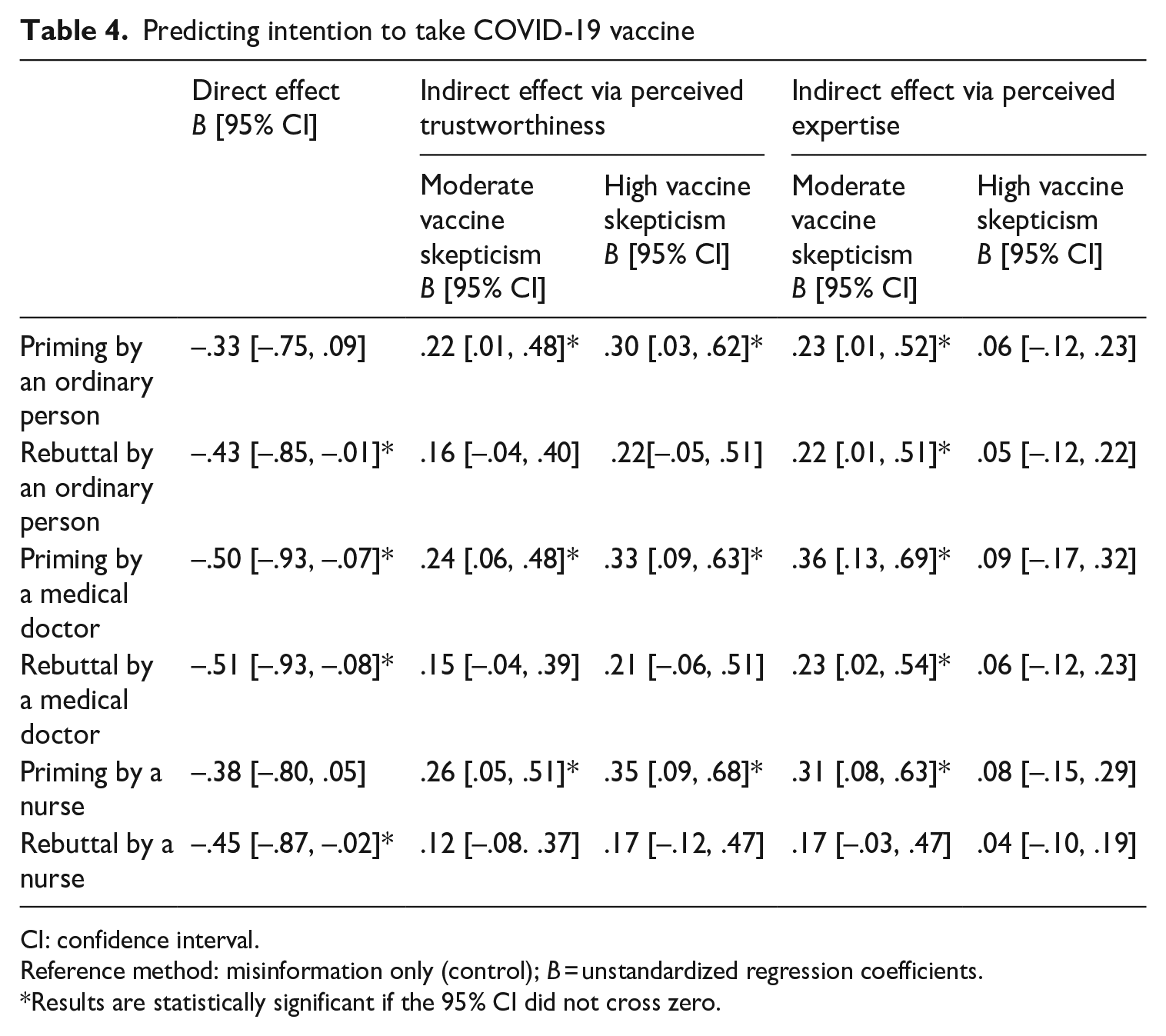
CI: confidence interval.
Reference method: misinformation only (control); B = unstandardized regression coefficients.
Results are statistically significant if the 95% CI did not cross zero.
As shown in Table 4, for both moderate and high vaccine skepticism groups, perceived trustworthiness was a significant positive mediator only for the effect of priming by an ordinary person (moderate vaccine skepticism: B = .22, 95% CI [.01, .48]; high vaccine skepticism: B = .30, 95% CI [.03, .62]), medical doctor (moderate vaccine skepticism: B = .24, 95% CI [.06, .48]; high vaccine skepticism: B = .33, 95% CI [.09, .63]), and nurse (moderate vaccine skepticism: B = .26, 95% CI [.05, .51]; high vaccine skepticism: B = .35, 95% CI [.09, .68]) on intention. This means that regardless of the level of vaccine skepticism and explicit expertise of the corrector, exposure to priming-based correction could lead to a higher intention to take COVID-19 vaccine if respondents perceived the corrector to be trustworthy.
Table 4 also shows that perceived expertise was a significant positive mediator for priming (moderate vaccine skepticism: B = .23, 95% CI [.01, .52]) and rebuttal (moderate vaccine skepticism: B = .22, 95% CI [.01, .51]) by an ordinary person, priming (moderate vaccine skepticism: B = .36, 95% CI [.13, .69]) and rebuttal by a medical doctor (moderate vaccine skepticism: B = .23, 95% CI [.02, .54]), and priming by a nurse (moderate vaccine skepticism: B = .31, 95% CI [.08, .63]). However, the mediation is only significant among the moderate vaccine skepticism group. This means that among those with moderate vaccine skepticism, exposure to corrections based on priming (by an ordinary person, medical doctor, or nurse) or rebuttal (by an ordinary person or medical doctor) led to a higher intention to take COVID-19 vaccine if the respondents perceived that the corrector was an expert.
Discussion
This study extends misinformation correction research by examining the effect of various social correction methods on vaccine skeptics’ intention to take the COVID-19 vaccine. It also provides insights into the role of perceived trustworthiness, perceived expertise, and vaccine skepticism when translating corrections into health-related beliefs. In general, the results show that social correction has a positive effect on COVID-19 vaccine intention. However, the effect is indirect and depends on the information consumer’s level of vaccine skepticism and their perceptions of the corrector’s trustworthiness and expertise. The following paragraphs discuss the key findings of the study.
It is interesting to note that a correction using rebuttal led to a lower intention to take COVID-19 vaccine regardless of the explicit expertise of the corrector. This finding reflects a backfire effect that is a concern when performing corrections (Ecker et al., 2022; Swire-Thompson et al., 2020). Although the backfire effect is usually observed when a correction leads to lingering or reinforcement of misperceptions (Pluviano et al., 2019; Vraga and Bode, 2017), this study suggests that it can also result in undesirable health perceptions (e.g. unwillingness to take a vaccine). Furthermore, a correction based on rebuttal is more likely to cause a backfire effect than priming, manifested by the findings that exposure to rebuttals from an ordinary person, medical doctor, or nurse resulted in a lower intention to take COVID-19 vaccine while only priming from a medical doctor resulted in it. A possible explanation for the backfire effect is that rebuttals may be misconstrued as an attack on one’s personal identity and worldview (Ecker et al., 2022; Lewandowsky et al., 2012).
The results partially support the source credibility theory (Hovland et al., 1953) because we found that perceived trustworthiness and perceived expertise only mediate the effects of certain social correction methods and vaccine skepticism only moderated the mediating effect of perceived expertise. The positive mediating effect of perceived trustworthiness made those exposed to priming-based corrections (regardless of explicit expertise) have a higher intention to take COVID-19 vaccine. This pattern can be observed for those with moderate and high vaccine skepticism. Second, although perceived expertise exerted a positive mediating effect on almost all social correction methods (except for rebuttal by a nurse), such effect can only translate to intention to take COVID-19 vaccine among those with moderate vaccine skepticism. In other words, priming-based corrections (rather than rebuttal-based corrections) seem to be effective in making both moderate and high vaccine skeptic groups more willing to take COVID-19 vaccine if the corrections came from a corrector with high perceived trustworthiness (i.e. someone who shares information that can be relied on). This result is apparent regardless of the explicit expertise of the corrector (i.e. ordinary person, medical doctor, or nurse).
Collectively, the findings are promising as they demonstrate priming as a more effective correction method to persuade both moderate and high vaccine skeptic groups to vaccinate. They also support previous work wherein corrections are more effective when correctors develop corrections that contain information from trustworthy sources (Pluviano et al., 2020; Vraga and Bode, 2017). Although Walter and Murphy’s (2018) meta-analysis suggests that rebuttals are more effective in correcting misinformation, our findings suggest that this may not be the case when considering interventions for those with different levels of vaccine skepticism. Although rebuttals seem to work for those with moderate vaccine skepticism, misinformation correction interventions should be designed to accommodate those with moderate or high vaccine skepticism. Moreover, since engaging in rebuttal may predispose someone to harassment (Arora et al., 2022; Bautista et al., 2021b), priming-based correction may be considered a better alternative.
Our findings are consistent with Pluviano et al.’s (2020) observation that source trustworthiness is more relevant than source expertise. Based on our results, respondents were more likely to evaluate the Twitter posts based on the trustworthiness of the shared information rather than the explicit expertise of the corrector. To illustrate, a medical doctor or nurse who shares health information from a questionable source is less likely to persuade others. On the other hand, an ordinary person that provides health information from reputable sources (e.g. drawn from CDC) is likely to persuade others. The results suggest that while health care professionals can leverage their expertise (Bautista et al., 2021a, 2021b) and the public’s trust (Malik et al., 2020) when correcting vaccine misinformation on social media, ordinary people can also contribute to addressing this problem by ensuring that the correction they share is supported by information from reputable sources (e.g. WHO and CDC).
Overall, the results indicate that exposure to priming-based social correction performed by an expert (i.e. health care professional) or non-expert (i.e. ordinary person) could increase vaccine skeptics’ intention to take COVID-19 vaccine if they perceived that the information shared by the corrector is trustworthy. This result is evident among those with a moderate or high level of vaccine skepticism. The findings provide insights into how priming-based social correction supported by trustworthy information sources can be an effective intervention to increase vaccine skeptics’ intention to vaccinate.
Theoretical and practical contributions
The study offers several theoretical and practical contributions. Theoretically, this study contributes insights into the applicability of source credibility theory (Hovland et al., 1953) to understand the mechanisms through which social corrections on social media translate to a desirable health outcome (i.e. increasing one’s intention to take COVID-19 vaccine). It also contributes to a better understanding by which perceived trustworthiness and perceived expertise could reverse the backfire effect of social correction methods on intention to take COVID-19 vaccine, as well as the pattern by which this occurs based on the level of vaccine skepticism.
The study also offers several practical contributions. First, the findings can guide public health planners in using social correction to persuade others to make optimal health decisions. Specifically, more people can be encouraged to engage in social corrections on social media by highlighting that priming (aside from rebuttal) can be useful regardless of one’s expertise as long as the information shared to support the correction comes from a reputable source. Second, the findings can guide health authorities when developing programs to encourage vaccine skeptics to go for vaccination. For example, interventions focusing on priming-based social corrections can be used when targeting respondents with different levels of vaccine skepticism.
Limitations and future research
Several limitations could serve as future research directions. First, the study is limited to the use of simulated Twitter posts. To enhance the study’s ecological validity, future research can identify actual Twitter posts that convey the social correction methods examined here and determine which methods influence health perceptions. Second, the study was limited to the Twitter platform. Since health misinformation is widespread on social media platforms other than Twitter (Vraga and Bode, 2018; Wang et al., 2019), future work can explore whether the findings are generalizable to other platforms.
Third, the results need to be interpreted with caution since the data did not come from a nationally representative pool of respondents. Future work can recruit respondents from survey panels that provide access to nationally representative samples. Fourth, the study was conducted among Western, educated, industrialized, rich, and democratic (WEIRD) respondents. Thus, the findings may differ in a study that uses non-WEIRD respondents (Muthukrishna et al., 2020). To further determine the generalizability of the findings, cross-country studies are needed.
Fifth, the study focused on a specific health misinformation topic (i.e. mRNA COVID-19 vaccines change a person’s DNA), and only one false story was presented. Future work can explore whether the results are consistent when multiple topics (e.g. Vraga and Bode, 2021) and false stories (Guay et al., 2022) are used. Finally, future work can add additional constructs or reconceptualize existing constructs to enhance the explainability of the model used in this study. For instance, researchers can consider how topic familiarity (i.e. measuring respondents’ familiarity with the false narrative that mRNA COVID-19 vaccines change a person’s DNA) mediates the effect of social correction methods on health-related intentions (Pennycook and Rand, 2020; Swire et al., 2017). Moreover, future work can explore the extent to which source trustworthiness and expertise serve as moderators (Pluviano et al., 2020).
Footnotes
Appendix 1
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Bautista is funded by the Bullard and Boyvey Fellowships awarded by the School of Information, The University of Texas at Austin.
Data availability statement
The data underlying this article will be shared on reasonable request to the corresponding author.