
Abstract
Noise pollution in hospitals has increased over the last few years to a level that can threaten the health and productivity of staff and patient safety. There are many control measures to reduce hospital noise. However, there is still no consensus on the best measures. This study aims to prioritize the control measures for reducing hospital noise. The work is divided into three phases. The first phase identifies and categorizes noise sources in hospitals through a review of the state-of-the art literature using Scopus®, ProQuest, PubMed, Google Scholar, Embase,™ and Web of Science™. The second phase identifies possible strategies for reduction of hospital noise and the best criteria for their adoption using findings from the literature review and interviews with corresponding experts. The third phase uses Fuzzy Analytic Hierarchy Process (FAHP) method and the Technique for Order of Preference by Similarity to Ideal Solution (fuzzy TOPSIS) method to weigh the criteria and to prioritize the control measures. Based on the results, hospital noise sources were classified into four groups: outdoor noise sources (29.7%), noise produced by domestic facilities (20.8%), indoor noise from human activities (27.5%), and noise produced by diagnostic and treatment equipment (22%). The study further arrives at a set of 9 criteria and 22 alternatives ranked using FAHP and fuzzy TOPSIS. The criteria’s weights were determined using the FAHP method, with feasibility (0.175), effectiveness (0.143), and interference with staff activities (0.140) being the most important criteria. It was found that engineering controls such as substitution of noisy equipment (rank = 1), using acoustic enclosures (rank = 2), using double-glazed windows (rank = 2), and soundproofing walls, doors, and windows (rank = 3) have priority for reducing hospital noise.
Introduction
The importance of hospital noise has been noticed in the last few decades. However, little research has been done to identify and reduce hospital noise. Noise pollution is significant due to its adverse psychological and physiological health effects such as reduced speech intelligibility, cancer, annoyance, disturbed sleep, hypertension ischemic heart disease, disturbed communication, reduced job satisfaction and leading to reduced productivity, anxiety leading to increased medical errors, and impaired performance.1–7 In addition to being exposed to acoustic energy, factors such as peak levels, changes over time, changes in amplitude, sudden impulses, and the distribution of frequencies significantly influence annoyance and perception of exposed people.8–12 Moreover, Diana et al. 13 have studied the impact of hospital noise on patients' speech intelligibility and recall. They have reported that hospital noise has a significant effect on both measures. It has also been reported that noise reduces patients’ well-being and their recovery and healing.14,15 Noise exposure prevention is important to avoid levels that will lead to complaints. 16
Therefore, the Environmental Protection Agency (EPA) and World Health Organization (WHO) have established exposure limits for noise in hospital environments in terms of daytime or night-time. The EPA has recommended that noise levels in the indoor environment of hospitals should not exceed 45 dB in the daytime and 35 dB in the night-time, while the WHO recommends that noise levels should not exceed 35 dB in the daytime and 30 dB in the night-time, and that peak noise levels at night should not exceed 40 dB(A). 17 Andrade et al. 18 in a recent systematic review on noise in the hospital have reported that equivalent continuous sound levels in hospital environments in the daytime were 37 to 88.6 dB(A) and in the night-time were 38.7 to 68.8 dB(A). Despite the highlighted importance of hospital noise and its adverse effects on staff and patients, its average levels are increasing annually.
Different sources are reported causing hospital noise pollution. Most common indoor sources of noise pollution are documented as human activities, communications among staff and patients, and healthcare activities.19,20 Moreover, outdoor noise sources such as traffic noise can expose staff and patients to adverse noise levels. 21 Generally, there are three methods for monitoring and controlling noise: control at the source, in the path of sound propagation between the source and receiver, and at the receiver.22,23 Due to the existence of various indoor and outdoor sources of noise, different noise control strategies are adopted for reduction of noise level exposure of healthcare staff and patients. Previous studies adopted methods such as implementation of quiet time protocol, education program, and use of soundproof materials.24–26 Due to the complexity of hospital noise, adopting a single method for noise abatement has not been recommended. Konkani et al. 15 have stated that behavior changes were not effective for noise control while in another study Konkani and Oakley 16 have confirmed that staff education is one of the effective interventions for reducing noise. MacLeod et al. 27 have used fiberglass absorbing panels on the ceiling and walls of the hospital for reducing noise. Their results have shown that absorbing panels had a dramatic effect and led to 5 dB(A) noise reduction. 27 Kol et al. 28 have reported that interventions including device overhaul and repair, physical space arrangement, and staff education were effective approaches for reduction of noise in the intensive care units, and this has led to about 12 dB(A) noise reduction.
Although there are many noise reduction strategies, the applicability and effectiveness of these strategies are somewhat controversial. In the case of hospital equipment, controlling noise at the source probably is not a feasible strategy for reasons including financial, and interference with work and equipment performance. On the other hand, staff and patients resist wearing ear protection devices because these devices disturb users and interfere with their work and communication. Considering such issues, adopting the best effective and applicable strategy for noise control in hospitals is a challenging issue. MCDM techniques assist to adopt contradictory questions, selecting the best solution based on the appropriate criteria, and merge various attitudes and views with each other. 29 In other words, these techniques by applying computational methods are used to reach an optimum way to solve a problem that cannot be solved by individual experiences. This technique incorporates several criteria to choose the best alternatives. 30 MCDM methods incorporated with fuzzy theory comprising fuzzy analytic hierarchy process (FAHP) and fuzzy TOPSIS (the technique for order of preference by similarity to ideal solution) are used to weigh the criteria and to prioritize the alternatives.31,32 With fuzzy methods, the ambiguity in subjective and wrong judgments of experts are eliminated.33,34 Accordingly, reliance on multi-criteria decision-making methods (MCDMs) and fuzzy theory could result in adoption of the best sound control methods. 35 Therefore, by relying on these methods, this study aims to prioritize the control measures for reducing hospital noise. The present study can be helpful in theory and practice and can make a connection between theory and practice. Accordingly, managers and engineers can use the obtained results to choose the most appropriate method to reduce noise in different departments of the hospital. Subsequently, the selection of the best noise reduction method and lowering hospital noise level can help staff to perform their work more optimally. 36
Method
This case study was conducted during 2021 in Imam Reza hospital in Tehran, Iran. The hospital is affiliated to Aja University of Medical Sciences and is located next to Chamran highway in Tehran, Iran. Units including intensive care unit (ICU), cardiac care unit (CCU), emergency ward, general internal medicine ward, postoperative care department, blood transfusion department, and operation room are operationally active in this hospital. This research was carried out in three phases. The flow diagram of the steps of study is presented in Figure 1. Flowchart of steps of the study.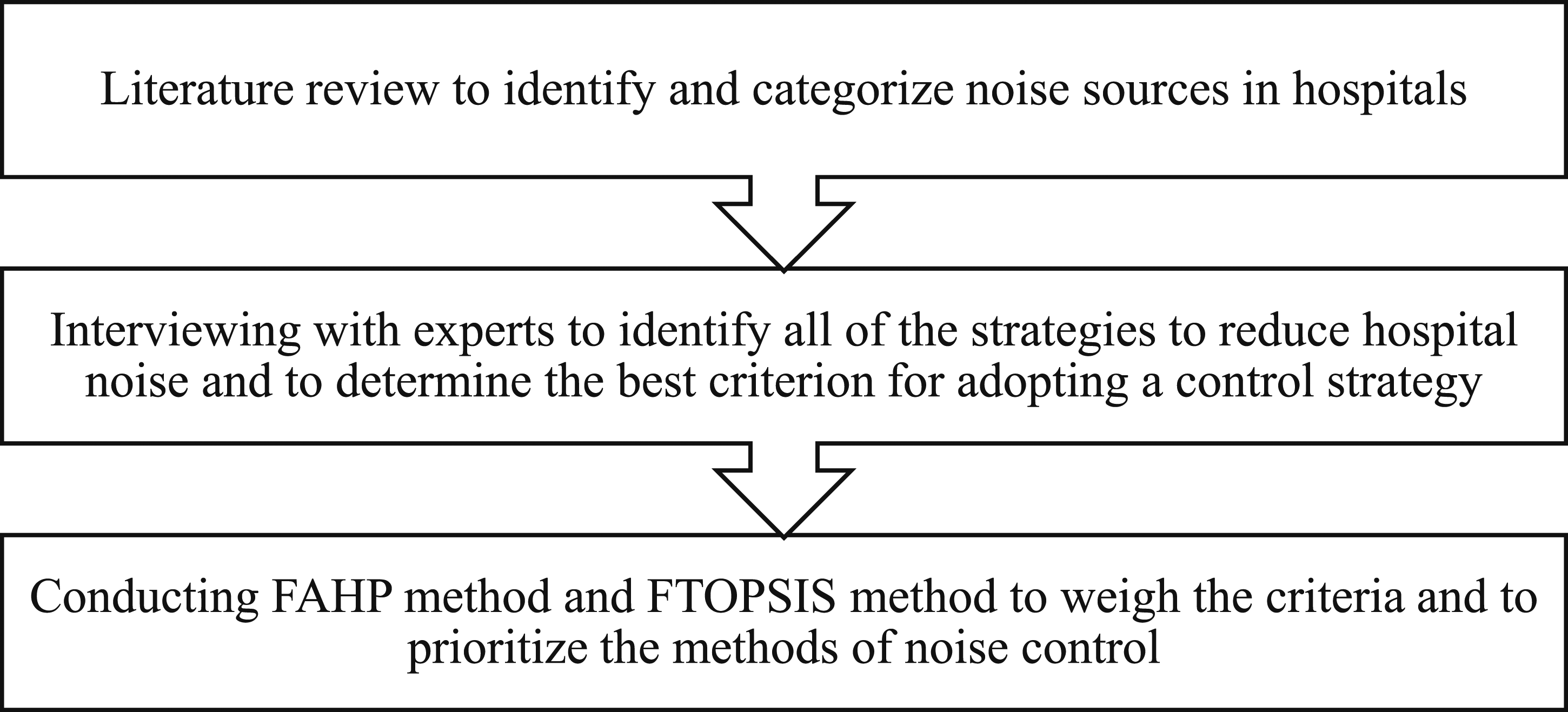
In the first phase, to identify and categorize noise sources in hospitals, a literature review was carried out using Scopus®, ProQuest, PubMed, Google Scholar, Embase,™ and Web of Science™. The identified sources were classified into four groups, namely, 1) outdoor noise sources (include traffic noise; noise produced by generators, compressors, and massive equipment; the screams of people outside the hospital; the noisy industries around the hospital; and the noise of construction operations), 2) noise produced by domestic facilities (such as telephones, air conditioners, speakers, pagers, lamps and lights, radio and television, elevators, keyboards, and printers), 3) indoor noise from human activities (such as nurses and patients talking, opening and closing doors, cleaning work, and moving beds and wheelchair), and 4) noise produced by diagnostic and treatment equipment (such as monitors, ventilators, imaging devices, and operating room equipment). These sources were presented to the staff in the hospital, and they were requested to choose the most common noise sources in their workplace. They were allowed to select one or several sources. The results were presented to an expert panel to better understand the current situation of hospital noise pollution from the perspective of staff.
In the second phase, along with a literature review, several interviews were conducted with experts in the field of noise control engineering, health education and promotion, occupational health, and health, safety, and environment management to identify the probable strategies to reduce hospital noise and further to determine the best criterion for adopting a control strategy. The expert panel comprised 20 experienced academic experts from different fields of study, including noise control engineering (4 experts), health education and promotion (4 experts), health, safety, and environment management (4 experts), and occupational health (8 experts). Noise control methods were divided into three categories, namely: 1) engineering controls, 2) administrative controls, and 3) personal protective equipment (PPE).
In the third phase, the FAHP method and fuzzy TOPSIS method were used to weigh the criteria and to prioritize the methods of noise control in hospitals.31,32 With these methods, the relative importance of each solution can be determined and ambiguity of experts' opinions is eliminated.33,34 A questionnaire comprising identified criteria was developed for conducting FAHP. To weigh the importance of each criterion, the questionnaire was emailed to each expert. Experts were asked to compare the relative importance of each criterion in the pairwise comparison. They were asked to determine the relative importance of each criterion from “equally preferred” to “absolutely preferred” on a five-point linguistic scale (Table 1). Criteria were compared in pairs and in all possible sequences to determine which criterion was more important. The Chang’s technique was used for performing FAHP. The steps of this method are as follows: (1) Define the hierarchical diagram. (2) Specify triangular fuzzy numbers (TFNs) and linguistic terms. TFNs and their corresponding linguistic terms for FAHP and fuzzy TOPSIS.
38
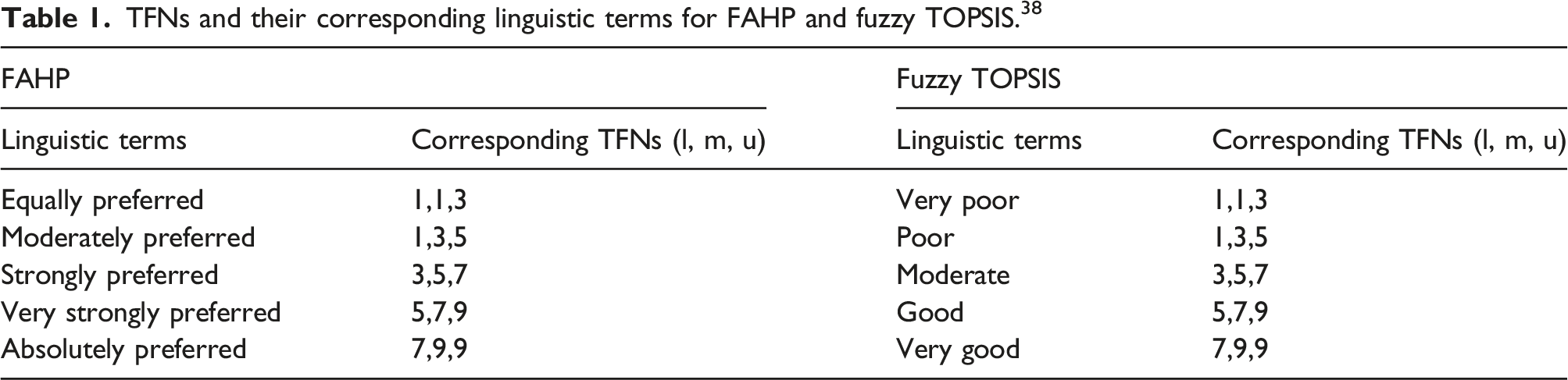
A TFN is defined as 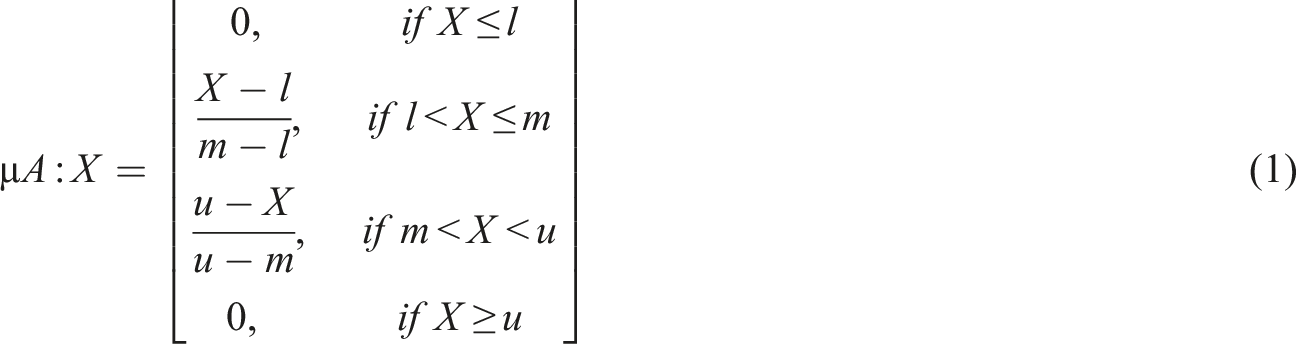
To determine the membership function, a five-point scale TFN was used (Table 1). (3) The pairwise comparison matrix (PCM) was created as follows: (4)


(5) Determining the extent of 


The extent of two fuzzy sets 

The extent of possibility of a TFN relative to k TFNs was determined as follows: (6) Specifying the weight of criteria as follows: (7) Calculating the un-normalized and normalized weights using the following equations: (8) All the experts’ responses were aggregated using the following equation: (9) Finally, aggregated opinions were defuzzied using the following equation:







Finally, to prove the consistency of the results, the consistency index (CI) was calculated. It is recommended that CI should be less than 0.1. 37 To conduct FAHP, the Expert Choice® software was applied.
The results obtained from FAHP were used as inputs to the fuzzy TOPSIS. This method uses a realistic modeling and compensatory approach for choosing alternative solutions depending on hard cutoffs. The method is applied to appraise multiple alternatives based on the considered criteria. To perform fuzzy TOPSIS, the experts were asked to choose a linguistic term from “very poor” to “very good” on a five-point linguistic scale for each alternative solution based on each criterion (Table 1). The steps to perform fuzzy TOPSIS are as follows: (i) Specification of the weighting of appraisal criteria (using FAHP). (ii) Determination of comparison matrix with m solutions and n criteria and specification of linguistic terms and corresponding fuzzy numbers. (iii) Specification of fuzzy positive ideal solution (FPIS) and fuzzy negative ideal solution (FNIS) as follows: (iv) Determination of the distance of each alternative from (v) Determination of the closeness coefficient index (CCI) to specify the ranking order of all alternatives. The alternative with the highest CCI is the most favorable solution. CCI is calculated using the following equation: (10) Finally, aggregated opinions were defuzzied using the following equation:







To conduct FTOPSIS, the formulated Microsoft Excel worksheet was applied.
Results
Prevalence of noise sources in the hospital based on the nurses' perspective.

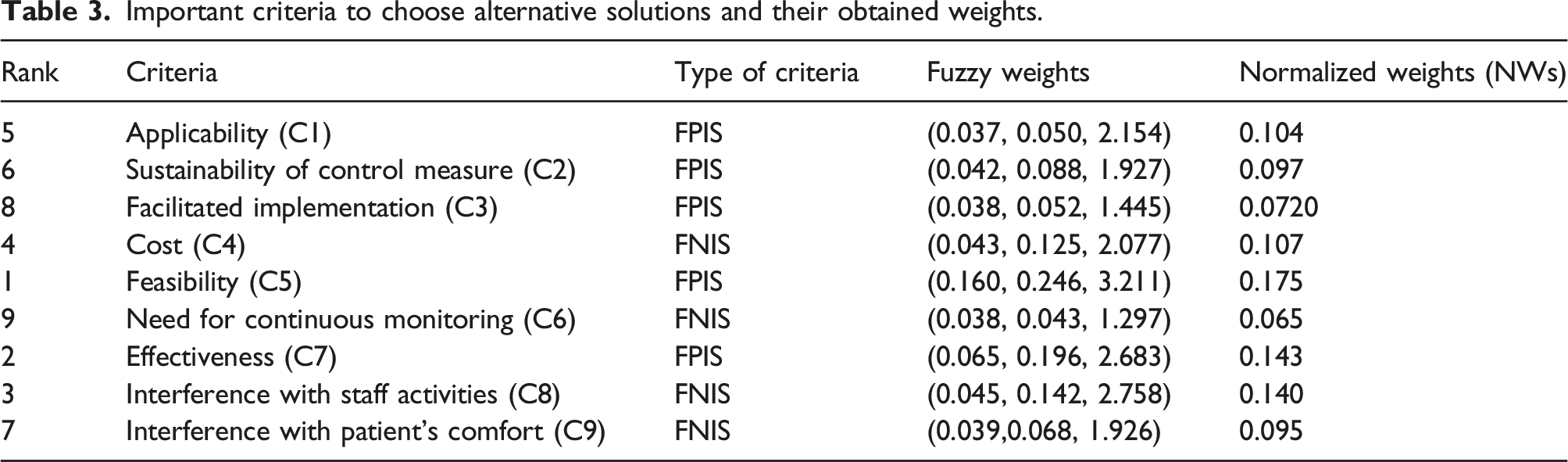
In the second phase, along with a literature review, several interviews were conducted with experts to identify all the probable strategies to reduce hospital noise and also to identify and to weigh the criterion for choosing the best control measures. Interviews were conducted with four experienced academic experts. Finally, nine criteria, namely, applicability (C1), sustainability of control measure (C2), facilitated implementation (C3), cost (C4), feasibility (C5), need for continuous monitoring (C6), effectiveness (C7), interference with staff activities (C8), and interference with patient’s comfort (C9), were considered to be the best control measures of hospital noise. Moreover, substitution of noisy equipment (A1), proper placement of equipment (A2), using acoustic enclosures (A3), routine repair and maintenance (A4), using smart and visual alarms instead of noisy alarms (A5), active control (A6), replacement of faulty devices and bulbs (A7), using double-glazed windows (A8), using partial mobile barriers (A9), soundproofing walls, doors, and windows (A10), installing absorptive material on floors, walls, and ceilings (A11), implementation of quiet time protocol (A12), reducing the number of patients in each room (A13), installing warning signs (A14), silencing the mobiles and telephones (A15), wearing headset and handsfree while watching TV or listening to the radio (A16), providing personal visual or vibrating pager (A17), assigning meeting room (A18), wearing noiseless clothes and shoes (A19), cleaning schedule during non-sleeping hours (A20), providing earmuff for patients and staff (A21), and providing earplug for patients and staff (A22) were selected as alternative solutions to reduce hospital noise. These methods are classified into three categories, namely, engineering controls, administrative controls, and PPE.
To weigh the relative importance of these categories, FAHP method was used, and a prepared questionnaire was submitted to 20 experts. Based in the 14 responses received from the experts (participation rate = 70%), engineering controls with normalized weight of 0.421 were determined as the most important methods to reduce hospital noise. Moreover, administrative controls and PPE were placed in the next level. The weights of administrative controls and PPE were 0.388 and 0.191, respectively.
As mentioned above, in this study 9 criteria and 22 alternatives were determined that must be ranked by fuzzy TOPSIS method. Therefore, a matrix with 22 rows and 9 columns was constructed, which is presented as a schematic diagram in Figure 2. Schematic diagram of the constructed matrix.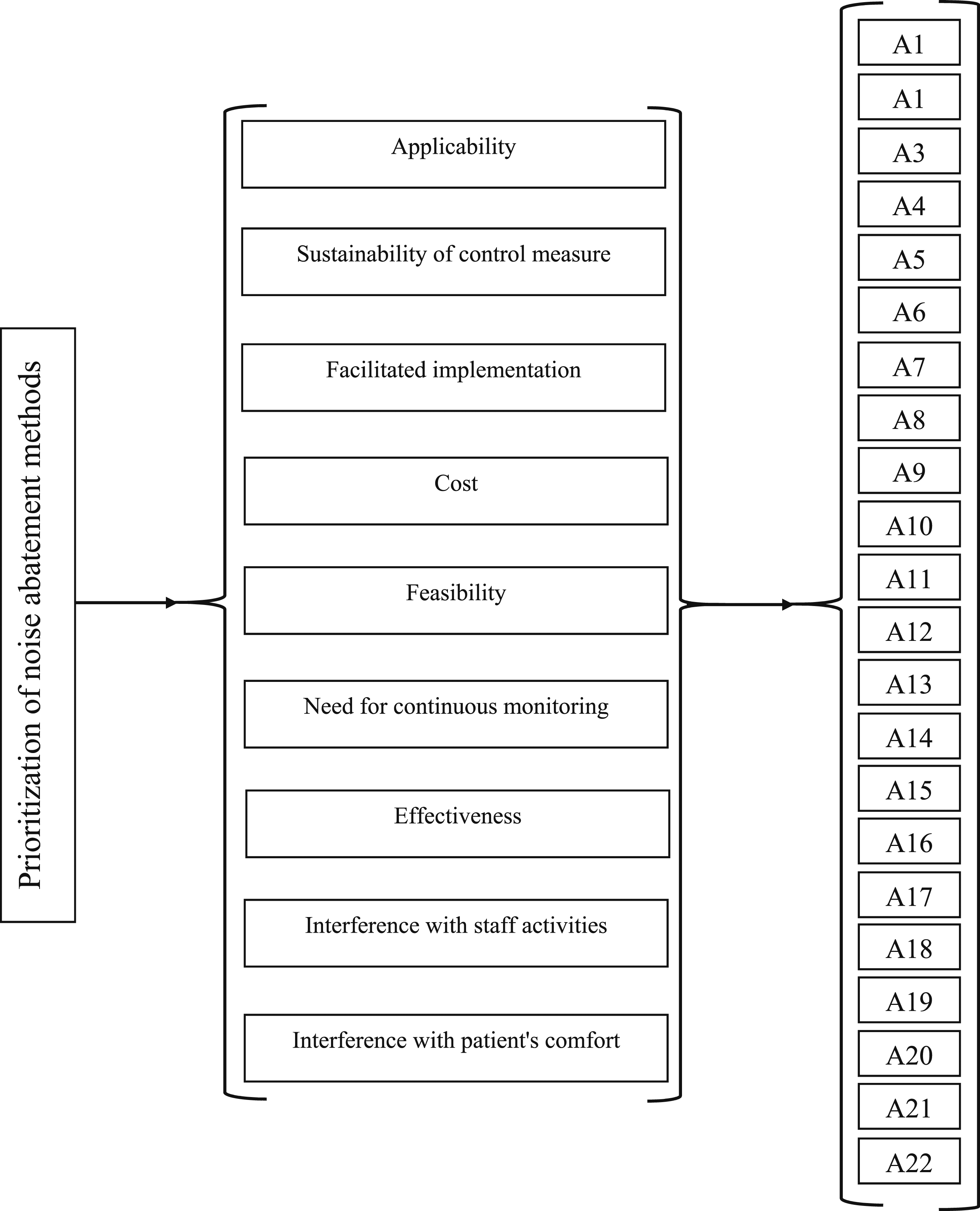
Important criteria to choose alternative solutions and their obtained weights.
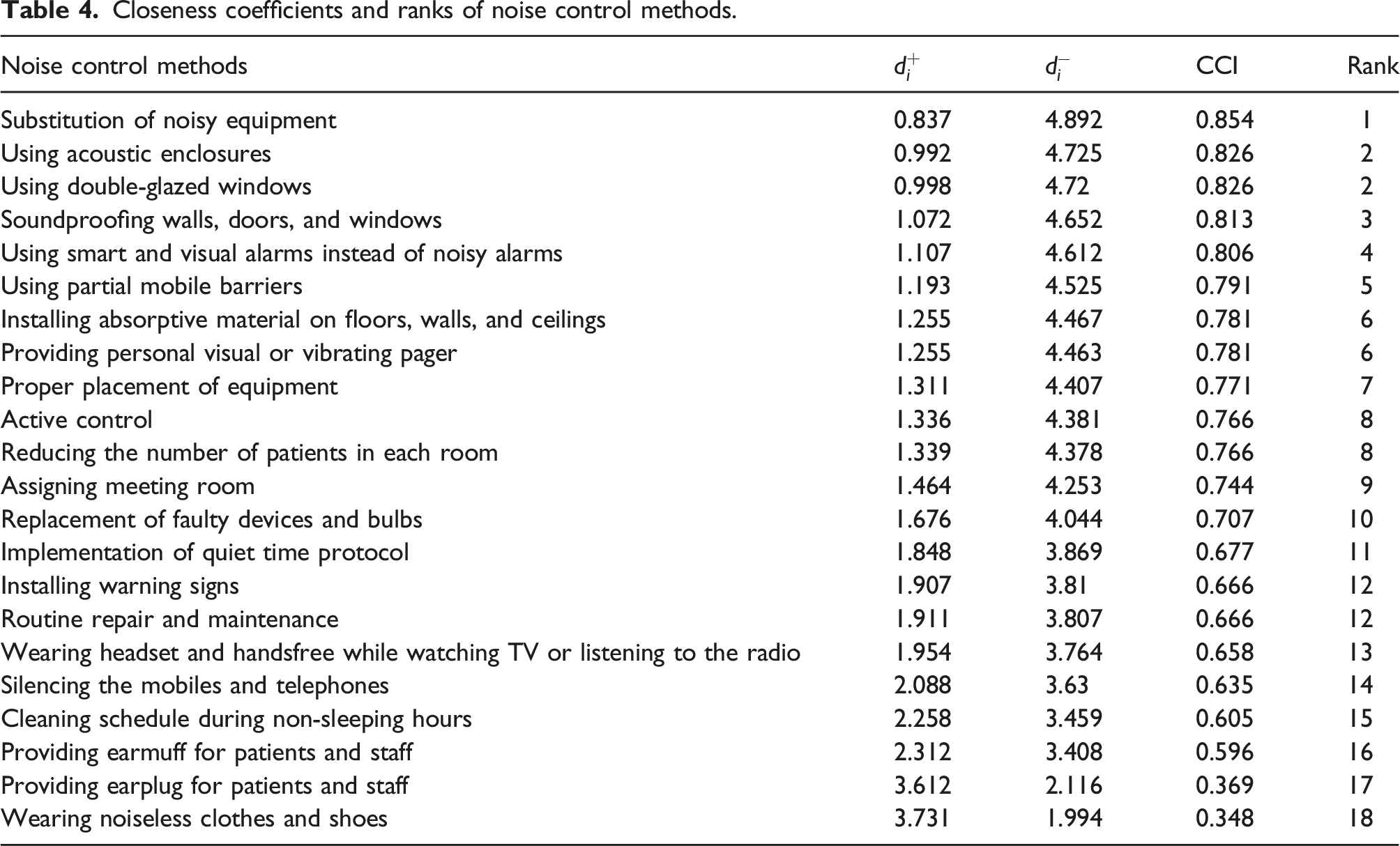
Closeness coefficients and ranks of noise control methods.
As reported earlier, the results of FAHP showed that experts determined engineering controls as the high-priority method. Moreover, administrative controls and PPE were placed in the next levels, respectively. Therefrom, it is confirmed that engineering control methods are in higher priority than administrative control measures, and administrative control measures are in higher priority than PPE.
Discussion
In this study, based on the prevalence of hospital noise pollutions, the best control strategies are prioritized. Considering the special condition of the hospital, the routine control measure may not be efficient for reduction of noise. Therefore, identifying and adopting a proper strategy is very essential for both hospital administrative and noise control specialists. Although there are various criteria to adopt as noise control measures, the weight and importance of these criteria are different. Based on the results of this study, feasibility, effectiveness, and interference with staff activities were the most important criteria. It is not unexpected that the hospital manager tends to perform strategies that are feasible, cost-effective, and non-restricting on staff performance. Further important criteria in terms of their importance are presented in Table 3. Using these criteria, the priority of noise control in the hospital environment can be determined.
The results presented in Table 4 show that the substitution of noisy equipment was the first method of interest of noise control in the hospital. This method is referred to as “control at source” and is the most effective strategy to reduce the noise at the source. 22 Criteria such as feasibility, effectiveness, substitution of noisy equipment, non-interference in the treatment process, and patient comfort and applicability can justify adopting this method as the first priority. Along with all benefits, financial issue and lack of noiseless equipment for a specific work such as MRI limit the adoption of this method. Following this method, the results showed that the installation of acoustic enclosures is the most popular and effective recommended method. An acoustic enclosure covers the noise sources fully, and its inner sides are lined with sound-absorbing material. This method can lead to a noise reduction of up to 20 dB. 39 To adopt acoustic enclosures, issues such as sufficient space, performance of machine, accessibility for operator or patients, heat transfer features, and dimensions and geometry must be considered. 40 In a hospital environment, this method is only effective for controlling the noise produced by hospitals' equipment and has no effectiveness for reducing the outdoor noise such as traffic noise pollution. Using double-glazed windows had equal priority to acoustic enclosure, and it was ranked as the second recommended method. These windows as a type of sound insulator are used to control transmission of outdoor noise to the hospital or to diminish noise transmission from noisy departments into others. The acoustic performance of double-glazed windows is dependent on the glass thickness and air space between glass layers, and it can effectively reduce noise pollution. This type of control should be implemented during the construction phase of the hospital building. Antonio et al. 41 have shown that double windows with discrete frames can perform similar to the double-glazed window, and they can be useful where improved acoustic insulation is required. Therefore, in the hospitals that double-glazed windows have not been mounted, to avoid the high cost of installing double-glazed windows, windows with discrete frames can be effective.
Based on experts' opinions, soundproofing the walls, doors, and windows (Rank = 3) was the next priority to reduce the noise levels in the hospital. Luwen et al. 42 have shown that concurrent use of soundproof metal doors and shutters can provide a noise reduction of 6 dB(A). Although modification of walls may be difficult, noise transmitted through doors and windows can easily be blocked by feeding the door with absorptive foam or sealing the windows or doors. Moreover, in the hospital environments where noise insulation is required, the partial mobile barriers can be a proper solution. In this study, using partial mobile barriers was ranked as the fifth priority. The acoustic performance of partial mobile barriers is based on their compositions, shapes, materials, and geometry. 43 Considering that the transparent barriers than opaque barriers are more efficient and convenient, in the hospital environments they can be used in places where there are no fixed barriers.43,44 Similar to partial barriers, acoustic curtains are suitable and effective materials that can be used to block the noise. 45 These curtains are easily installed, cost-benefit, and acoustically effective.
Many medical devices and electronic devices produce high levels of noise as alarms, and these are considered as one of the most prevalent sources of noise pollution in hospitals. 46 In this study, “using smart and visual alarms instead of noisy alarms” was introduced to the experts as a strategy to reduce noise pollution, and they ranked it as the fourth priority. In the study by Konkani et al., 47 it has been suggested that alarms should be managed as using “smart alarms,” “developing some protocols to improve alarm performance,” “auditory alarms with distinct features,” and “third-party alarm notification systems.” Although, visual alarms may solve noise issues, they may introduce issues such as sleep disturbance. Using a personal visual or vibrating pager, which is ranked as the fifth priority, is also recommended as an effective administrative control. 48 Generally, designing ergonomic alarms and pagers as noise control engineering at the source can resolve a large share of the noise problem. Additionally, simultaneous educational intervention to manage alarm can supplement the noise reduction process.
Installing absorptive material on floors, walls, and ceilings is one of the most common methods to reduce hospital noise and in this study, it was ranked as the sixth priority. Results of a previous study showed that pasting of fiberglass panels on the ceiling and walls has reduced hospital noise effectively by 5 dB(A). 27 Another study has shown that replacing ceiling tiles with noise-absorbing tiles has led to better sleep and reduced stress in patients and has increased quality of care. 49 To use absorptive material, some considerations should be noted. Barnhill et al. 50 have stated that in the hospital environments, especially in the ICU, conventional noise-absorbing materials are not recommended because these materials may facilitate microorganism growth or produce a high level of dust.
Proper placement of equipment was ranked as the seventh method. The goal of this method is to increase the distance between noise source and receiver or separate them. In the study conducted by Wang et al., 51 in a new ICU ward a dedicated service corridor was constructed. In this way, ICU staff was separated from noise sources by a service corridor. The results indicated that the addition of a dedicated service corridor is associated with less perceived noise level and also quieter ICU and in turn, it led to increased satisfaction and reduced noise. In this study, staff reported that outdoor noise including noise produced by generators, compressors, or other massive equipment around the hospital was the most prevalent source of the noise. Therefore, proper placement of indoor and outdoor equipment may have a dramatic effect on noise reduction.
Active control is identified as the eighth priority. Noise cancellation is an effective method to control noise in the low- and mid-frequencies below 1000 Hz and can be used to reduce hospital noise in these spectra. 52 This method uses low-frequency noise and operates on the principle of destructive interference between unwanted noise pollution and under-control generated noise. 53 Hutchinson et al. 54 used this method to reduce ICU noise due to alarms. Their results indicated that ICU noise was attenuated by 14.4 dB at the alarm tone’s frequency. In a related noise control study, Niklas 55 suggested that the noise-masking system is an efficient method in covering unwanted sound. It has been noted that with this method, the perception of unwanted sound can be disrupted and people will hear the masker as the dominant noise. 56
In this study several administrative controls such as reducing the number of patients in each room, assigning meeting room, implementation of quiet time protocol, installing warning signs, and routine repair and maintenance were ranked as 8th, 9th, 11th, 12th, and 13th priorities, respectively. Many studies have been conducted to investigate the effectiveness of these methods and results are controversial.57–59 Konkani et al. 59 have stated that although educational intervention and behavioral modification can reduce noise, it is not recommended to rely only on this intervention to control excessive noise. In another research, McGough et al. 60 have reported that quiet time bundle implementation has not reduced noise pollution in hospital significantly; however it can be implemented to improve patient and nurse perceptions of noise. In a comprehensive study, Chawla et al. 61 have attempted to reduce noise using administrative control measures on equipment, education and behavioral, and environmental modifications. They have shown that multipronged interventions have resulted in considerable noise attenuation. Kol et al. 28 have also exploited interventions such as staff education, device overhaul and repair, and physical space arrangement to reduce noise in an ICU ward. The results of their study have shown a 10 dB(A) reduction after the implementation of the interventions.
Based on the opinions of experts, PPE was determined as the last recommended measure. Moreover, the results in Table 4 show that providing earmuff for patients and staff, providing earplug for patients and staff, and wearing noiseless clothes and shoes were ranked as sixteenth, seventeenth, and eighteenth priorities, respectively, to reduce hospital noise. It is proven that PPE such as ear buds and earmuffs can reduce noise effectively up to 45 dB when used simultaneously. 62 Consistent with the current results, Gallacher et al. 63 used headphones to reduce patient’s noise exposure. Their results confirmed that headphone with active noise control has resulted in 6.8 dB reduction in patients' noise exposure. It has further been shown that earplug can reduce noise perception and in turn increase sleep quality and satisfaction. 64 Despite the effectiveness of this device, patients and staff do not have inclination to wear them because it may interfere with comfort and their work, respectively. Wearing soft-soled shoes in hospital is recommended as one of the methods to reduce hospital noise pollution, but the effectiveness of this method has not been studied. 25 In recent studies, prescribing some vitamins and nutritional supplementary was recommended to protect individuals against hearing loss. 65 The researchers can consider this as one of probably effective administrative methods and pay attention to this area of research. Despite the advantages of this study, there are some limitations in the light of which the results to be treated. The study has been carried out during the COVID-19 pandemic, and this might have an influence on the prevalence of noise sources in hospitals and, therefore, the priority of control measures may be slightly different. Moreover, all the departments have been considered as the hospital environment, while there are significant differences between departments especially in the prevalence of noise sources. Therefore, depending on dominant noise sources in each department, the prioritizations from department to department may vary.
Conclusion
In the hospital setting, standard noise control measures may not always work effectively due to unique challenges. Therefore, it is crucial for hospital administrators and noise control specialists to identify and implement appropriate strategies. This study utilized multi-criteria decision-making methods (MCDMs) like AHP and TOPSIS, along with fuzzy methods, to assess the importance of each solution based on expert opinions.33,34 The research revealed the varying significance of criteria for noise control measures, with feasibility, effectiveness, and interference with staff activities being key factors. The primary noise control method identified was substituting noisy equipment, followed by installing acoustic enclosures and double-glazed windows. Soundproofing walls, doors, and windows were also prioritized, emphasizing the need to address noise sources within hospitals. Administrative controls like reducing patient occupancy and implementing quiet time protocols were suggested, along with the use of earmuffs and earplugs as supplementary measures. This study offers valuable insights for enhancing noise management in hospitals by considering a variety of strategies comprehensively.
Supplemental Material
Supplemental Material - Prioritization of noise abatement methods for controlling hospital noise pollution
Supplemental Material for Prioritization of noise abatement methods for controlling hospital noise pollution by Milad Abbasi, Mohammad Osman Tokhi, Nazila Eyvazzadeh, Mohsen Falahati, and Mojtaba Zokaei in Journal of Low Frequency Noise, Vibration and Active Control.
Footnotes
Acknowledgments
The authors appreciate all experts and workers participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.