
Abstract
Weight-bearing exercise is a well-accepted physiotherapy to prevent osteoporosis for stroke patients. But the immobility of stroke patients limits the types and intensity of conventional interventions. Recent advances in robot-assisted therapeutic device provide an innovative way which could potentially overcome the above-mentioned limitations. However, the effects of robot-assisted physiotherapy on osteoporosis prevention have not been fully understood. The purpose of the present study is to develop an innovative theoretical framework to investigate the effects of static robot-assisted walking exercise on bone health. Through conducting a series of studies using a robot, force insoles and CT-image-based computational modeling, our results show that robot-assisted walking can significantly reduce the osteoporosis risk for stroke patients. However, the vertical peak ground reaction forces generated from static robot walking is generally lower than that from treadmill walking due to the fact that there are no heel strike and push-off effects in static robotic walking.
Keywords
Introduction
With the increase of life expectancy, stroke becomes a major cause of mortality and long-term disability. Studies have shown that stroke would be the second leading cause of death and could affect about two million people each year in China. 1 More than half of the stroke survivors are aged over 75 years. 2 Development of osteoporosis after stroke is rapid and pronounced because of significant bone loss in paretic or paralyzed limbs. 3 Most of the complications after stroke, such as immobility, 4 gait impairment, 5 reduced muscle strength, 6 and low cardiorespiratory fitness, 7 are well-recognized risk factors of osteoporosis. Previous studies indicates that the loss of bone mineral density (BMD) can be up to 12% in the proximal femur and 3% in lean mass of the paretic leg,3,8 resulting a four-fold increase in the risk of osteoporotic fractures within the first post-stroke year.9–12 Clearly, enhancing bone formation is of crucial importance during early stroke rehabilitation.
Mechanical loading on bone generated by ground reaction force (GRF) and muscle contractions can help to maintain bone mass and strength.13,14 Traditional gait rehabilitation programs including manual therapy and body weight-supported treadmill training have been proven to be beneficial for maintaining or improving bone strength, geometry, and gait function of stroke patients to some extent.4,15–19 Complications, such as spasticity, muscle weakness, and impaired balance, after stroke could reduce the mobility of patients significantly.4–7 Consequently, stroke survivors can only participate in limited physical exercises. In addition, it is worthwhile to note that conventional training programs still follow the “Let’s try and see” strategy, and the end-point is difficult to anticipate.20,21 The “one-to-one” supervision with low effectiveness/costs ratio is also limited by the fitness of therapists. 22
In recent years, robot-driven therapeutic devices are proposed to overcome the aforementioned limitations. Such innovative devices which employ robotic actuators/motors rather than therapists to assist patients with pre-defined therapy programs have drawn increasing attention in neuro-rehabilitation. 23 One notable advantage of robot-driven therapy over conventional therapy is that it can accurately and objectively measure patient’s joint kinetic and kinematic outcomes, and gait patterns. 24 In addition, its endurance will not be affected by repetitive tasks, and therefore human error can be avoided. 25 Nowadays, applications of robot-assisted therapy in neuro-rehabilitation mainly focus on gait recovery of stroke patients.26–31 Little is known about the effectiveness of the robot-driven therapeutic devices in preventing osteoporosis from happening during the early stage of stroke.
Weight-bearing measurement is essential during physical activities of stroke survivors. 32 Ambulatory devices, such as pressure/force insole, have been used extensively in determining the GRF for both clinical and research purpose.33–35 Integration of robots with ambulatory devices in neuro-rehabilitation may lead to better outcomes in prevention of osteoporosis. 36 However, relevant research in determining the relationship between weight-bearing exercises conducted using robot-assisted devices and their induced biomechanical stimuli on bone is limited. Consequently, successful design of training programs much depends on clinician’s experience rather than understanding the underlying relationship.
Therefore, the first objective of this paper is to investigate the feasibility of robot-assisted devices in maintaining bone formation and preventing development of osteoporosis. Secondly, we aim to develop a theoretical framework which can quantify the effects of weight-bearing exercises performed using robot-assisted devices on the biomechanical microenvironment of bone by conducting a series of gait exercises in conjunction with computational modeling. The findings of this research could potentially allow clinicians to accurately predict the treatment outcomes, and hence prescribe effective gait training programs.
Methodology
Figure 1 shows the methodology and approach used in this study. The peak ground reaction force (PGRF) of various gait exercises on treadmill and robot was quantified by ambulatory device. The raw computed tomography (CT) data of participated subjects were used to reconstruct the three-dimensional (3D) tibia model. Both the PGRF and the tibia model were used as input to predict the bone health by developing a computational model based on our previous studies.20,37–40
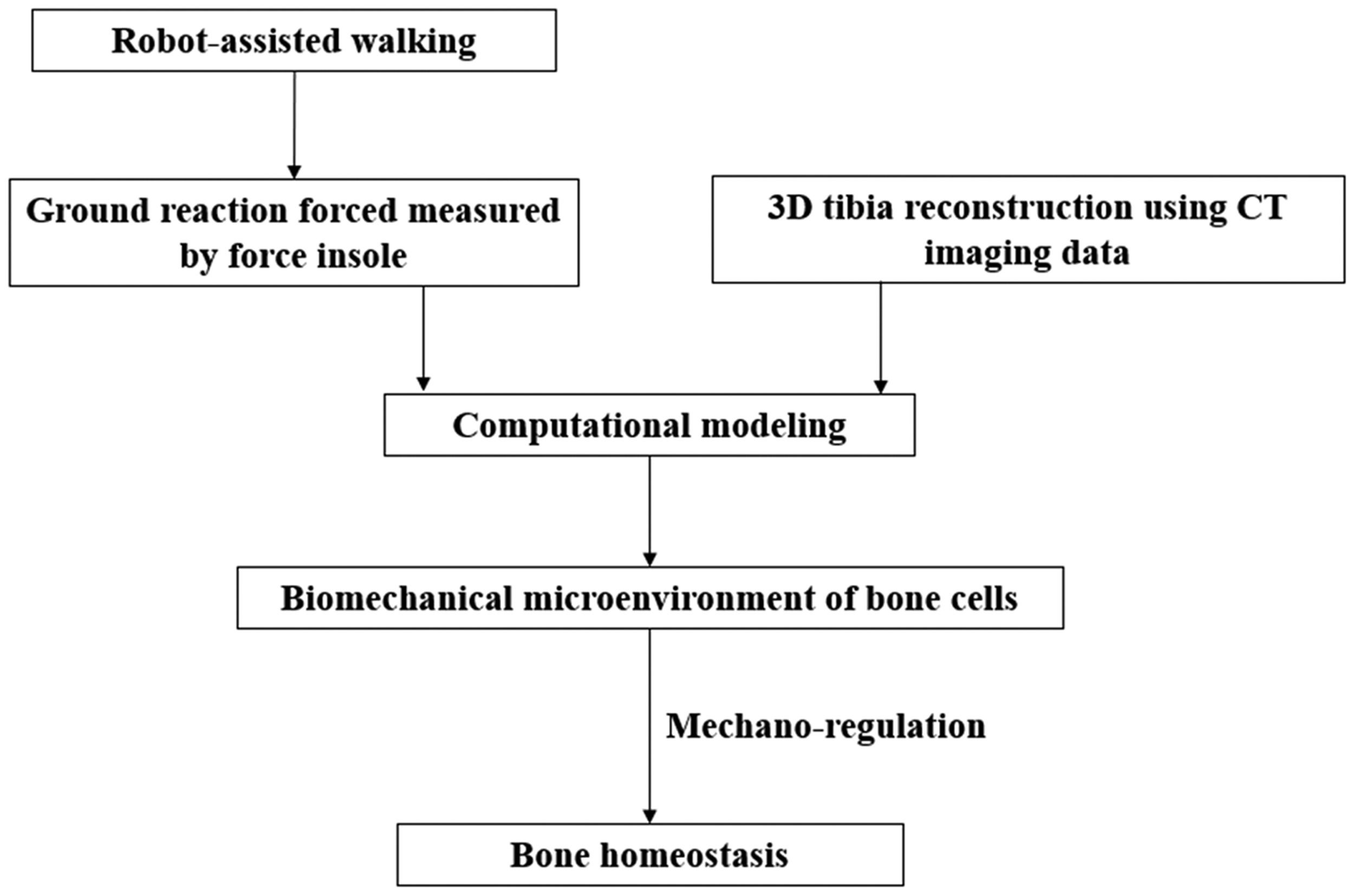
The schematic diagram showing the methodology used in this study.
Gait training on treadmill and robot
Five healthy volunteers (three females and two males, mean age ± SD = 21.2 ± 0.84 yr, BMI ± SD = 22.0 ± 2.12 kg/m2) were recruited from the Second People’s Hospital of Shenzhen, China. All participants were given written informed consent, and ethics approval was granted by the hospital committee (code: 20180515008).
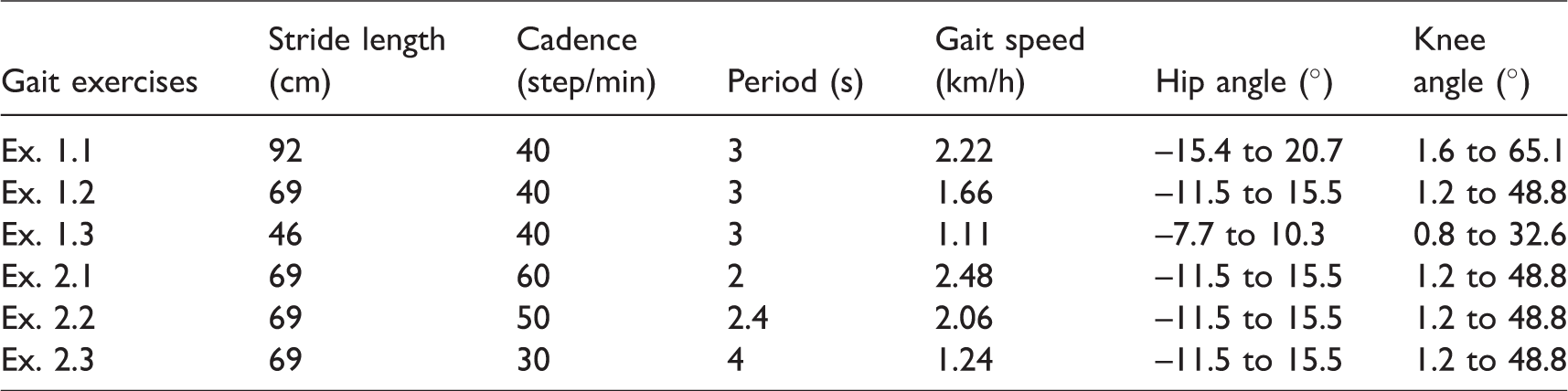
A series of weight-bearing activities under normal walking speed (i.e. walking speed = 1–6 km/h) 41 was conducted on treadmill (SportsArt Fitness T652M, Mukilteo, WA, USA). Each walking test was set to be 1 min (Figure 2(a)). Before the testing, all subjects were required to conduct multiple trials on treadmill until their stride length and cadence are consistent for each given speed according to video record. After the testing on treadmill, all participants were required to perform gait exercises on a static robot (Flexbot, Jinho Robot, China). This robot-assisted gait trainer has four actuators located at left and right hip and knee joints. Both legs of a subject were attached to the robot by using two hip braces, two knee braces, and two ankle braces (Figure 2(b)). Stride length and cadence are adjustable in software installed in a high-performance computer for parametric study. The gait period is dependent on the cadence, whereas both hip and knee angles rely on the stride length. The gait speed is automatically calculated by the system provided the stride length and cadence values are given. In this study, the gait parameter values of all exercises inside the robot are listed in Table 1. The gait training time was set to be the same as on treadmill (i.e. 1 min).

Clinical and numerical experiments conducted in this project: (a) walking tests on treadmill; (b) gait training on robot; (c) data acquisition system; (d) 3D reconstruction of tibia.
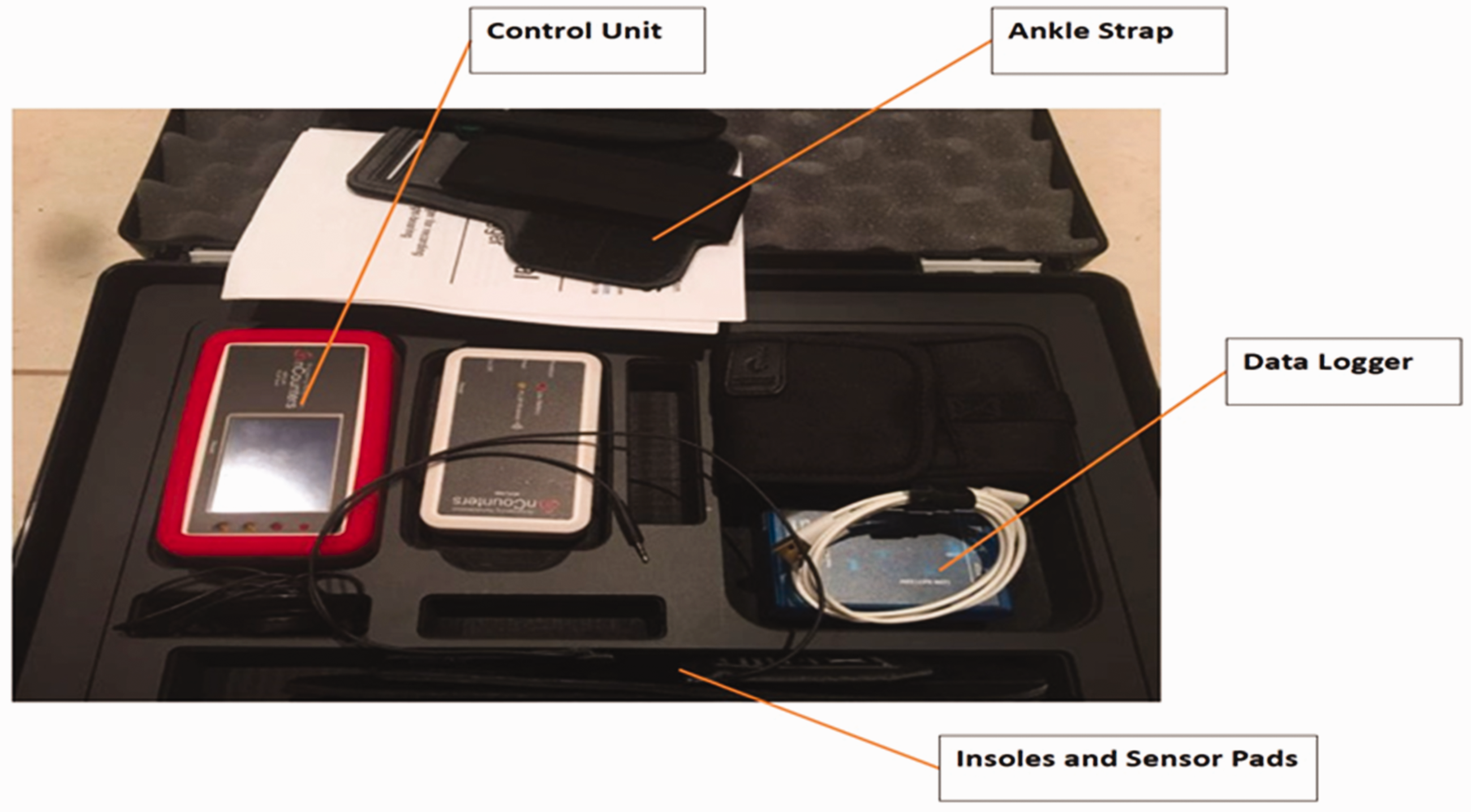
The force insoles with the data logger (nCounters, Melbourne, Australia) used in the experimental measurements.
Values of gait parameters in the parametric study.
Measurement of vertical GRF
The vertical GRFs were measured by force insoles (nCounters, Melbourne, Australia) in which two force sensors were attached to forefoot and heel, respectively. A data logger was connected to the insoles and placed above subject’s right ankle (Figures 2(c) and 3). The sampling rate was 100 Hz. Fast Fourier transform technique has been used to filter away background noises. Data from the insole were recorded by the data logger and displayed on computer screen. A customized Excel program was used to graph the GRF–time history curves. The total vertical GRF is calculated based on the so-called “One-Plate” method which assumes the total GRF is the sum of loading acting on the back limb and the front limb, and is widely applied to investigate GRF during healthy and clinical gait.
42
In the present study, only the vertical peak GRFs expressed in terms of body weight (BW) are used as inputs for predicting the bone homeostasis under different physiological loading conditions. One minute was given to each participant to practice walking with insole and also to condition the sensors before testing

CT scan and 3D reconstruction of tibia
The right tibia of the participants was subjected to a Siemens Somatom Definition AS 128 slices CT scanner (Siemens Healthcare Gmbh, Germany). The slice size was 512 × 512 pixels and slice thickness was 1 mm. The original CT images in Dicom format were imported to Mimics (Materialise, Leuven, Belgium) for 3D reconstruction which included main procedures such as segmentation, region growing, edit mark, Boolean operation, etc. (Figure 2(d)). Both surface and volume mesh were created in 3-matic (Materialise, Leuven, Belgium) for computational modeling.
Computational modeling
A computational model was developed in this study to investigate the influence of robot-assisted gait exercise on lower extremity bones health. The mechanoregulation theory by Prendergast et al. was adopted to simulate the influence of insufficient loading on bone resorption and osteoporosis.
43
This theory was originally developed to simulate cell differentiation during bone healing and later was extended to model bone resorption. The theory suggests that cell differentiation in bone is governed by two mechanical stimuli: octahedral shear strain of the tissue (γ) and interstitial fluid flow (ν) defines the so-called mechanical stimuli index (
We have recently developed a computational model for bone fracture healing using the mechanoregulation theory of Prendergast et al.20,37–40 Using the theory of porous media, the model computes the octahedral shear strain of the tissue 

By writing the continuity equation for solid phase, we can find the relationship between solid phase velocity and deformation as follows

The conservation of momentum equation with the absence of inertial term and body forces for the media can be expressed as

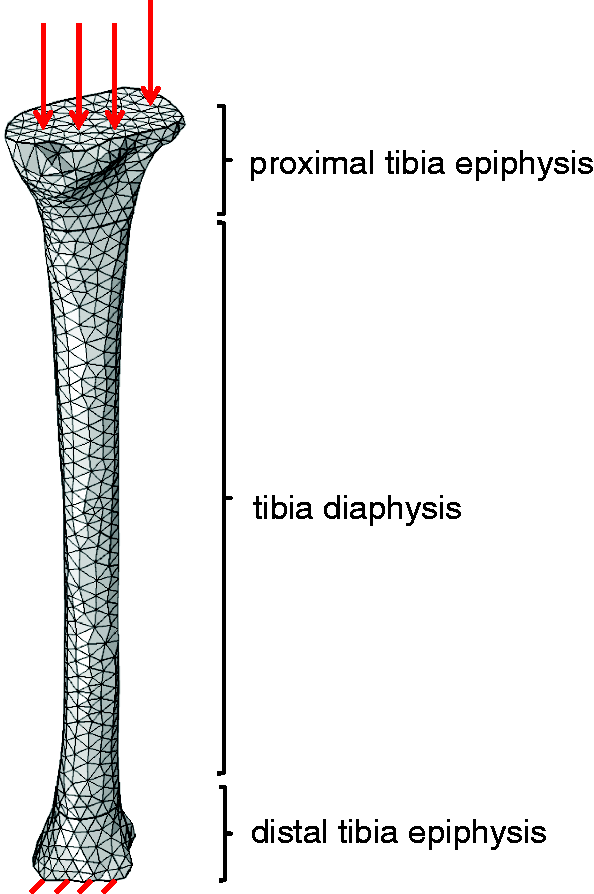
Finite element model of tibia and the boundary conditions used in this study.
Material properties of tissues used in this study.50

Results
Walking tests on treadmill
Figure 5(a) to (e) presents the anterior–posterior vertical GRF–time histories of all five participated subjects who conducted a series of walking exercises on the treadmill. All of the vertical GRF–time curves exhibited the classic patterns of walking with double peaked configuration. For walking speed up to 6 km/h, the first peak occurred between 18% and 28% of the total stance time, while the second peak occurred between 70% and 82% of the total stance time. The relationship between the vertical PGRF and gait speed is presented in Figure 6 which reveals a strong correlation with coefficient of determination (R2) = 0.97. The obtained linear regression equation for vertical PGRF and gait speed is

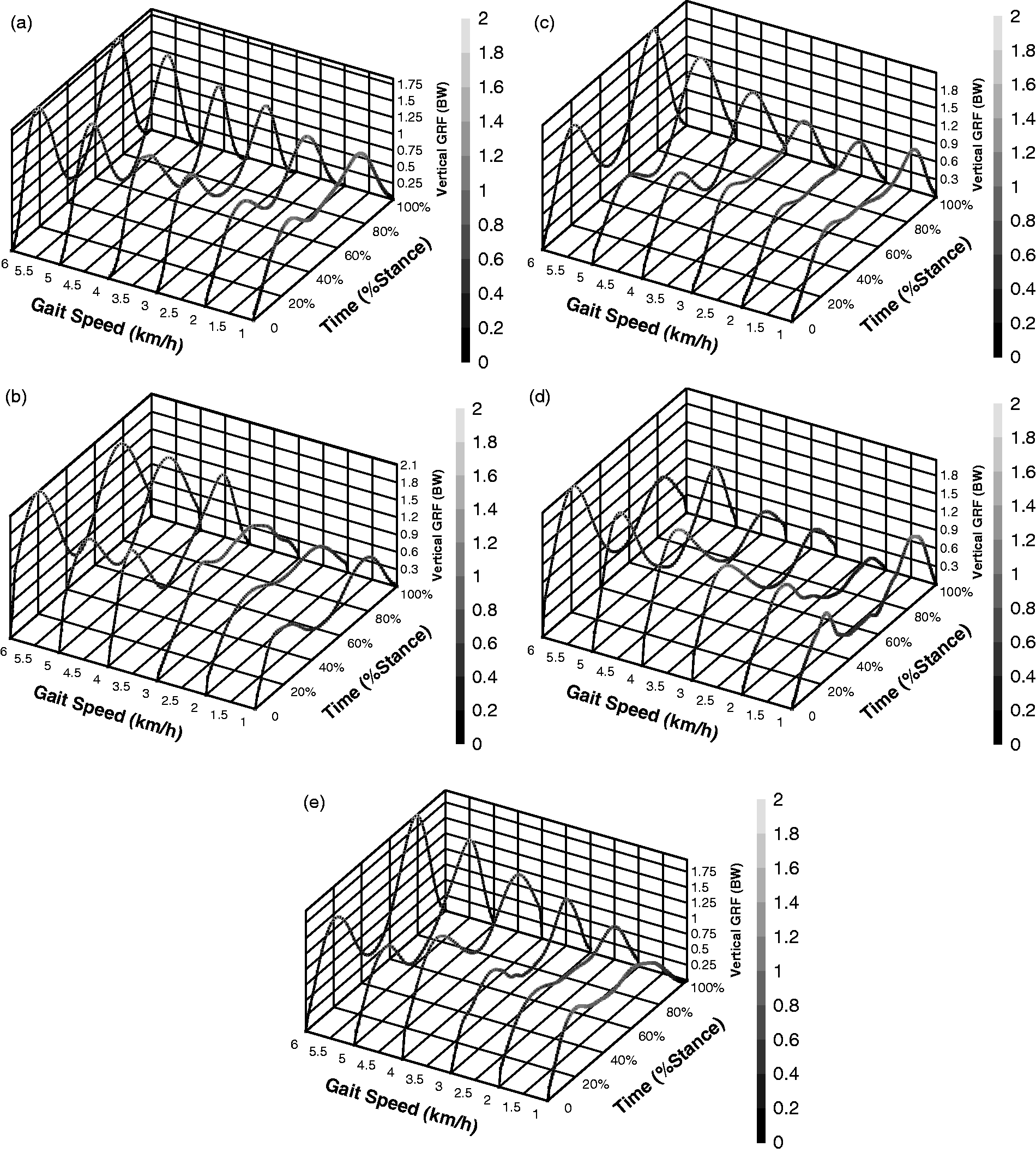
Vertical GRF–time histories of (a) subject 1; (b) subject 2; (c) subject 3; (d) subject 4; and (e) subject 5 for a series of walking tests on the treadmill.
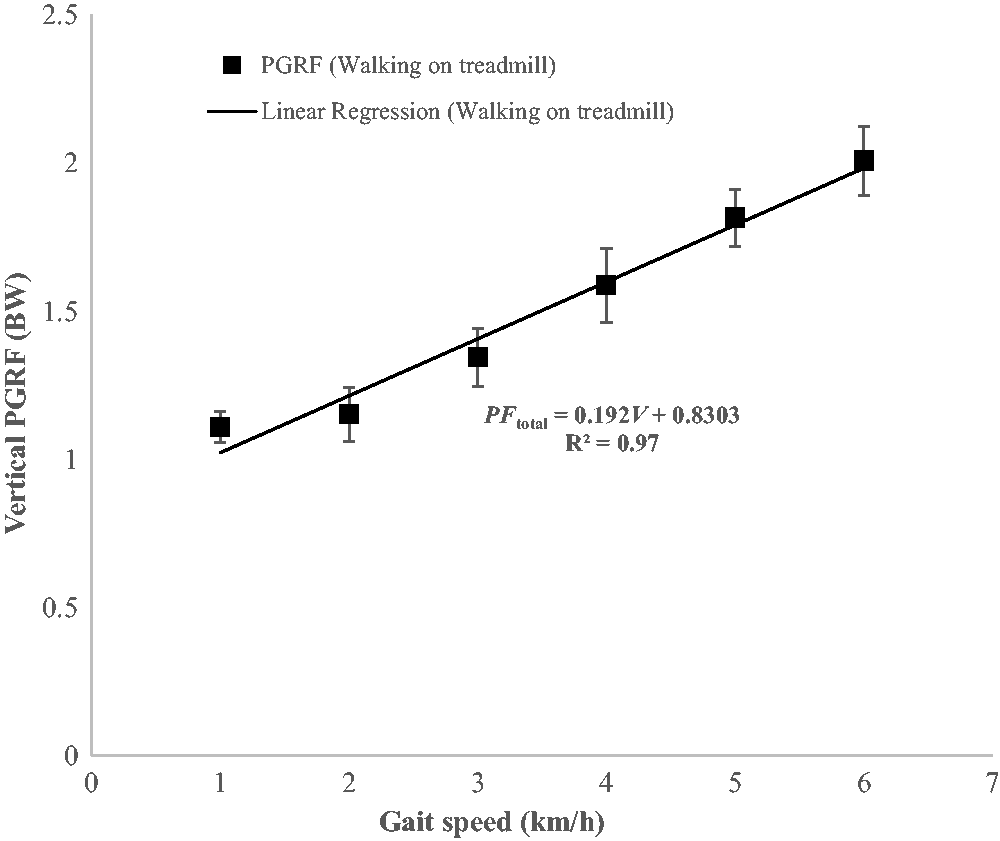
The relationship between vertical PGRF (PFtotal, in terms of BW) and gait speed (V, in terms of km/h) for walking on the treadmill.
Gait exercises on robot
Figure 7(a) to (e) presents the anterior–posterior vertical GRF–time histories of all five participated subjects who performed a series of walking exercises on a robot-assisted gait trainer. It can be seen from Figure 7 that most of the GRF–time histories associated with gait speed smaller than 2.2 km/h only exhibited single peak value which located at about 41%–50% of the total stance time. When the cadence was kept at 40 step/min, the vertical PGRF associated with different stride lengths had a strong positive relationship with the gait speed. On the other hand, the PGRF associated with constant stride length (i.e. 69 cm) and various cadence values yielded a positive correlation with the gait speed (Figure 8). The linear regression equations for vertical PGRF versus gait speed are shown in equations (8a) and (8b) for cadence = 40 step/min, stride length = 46 cm–92 cm and stride length = 69 cm, cadence = 30–60 step/min, respectively


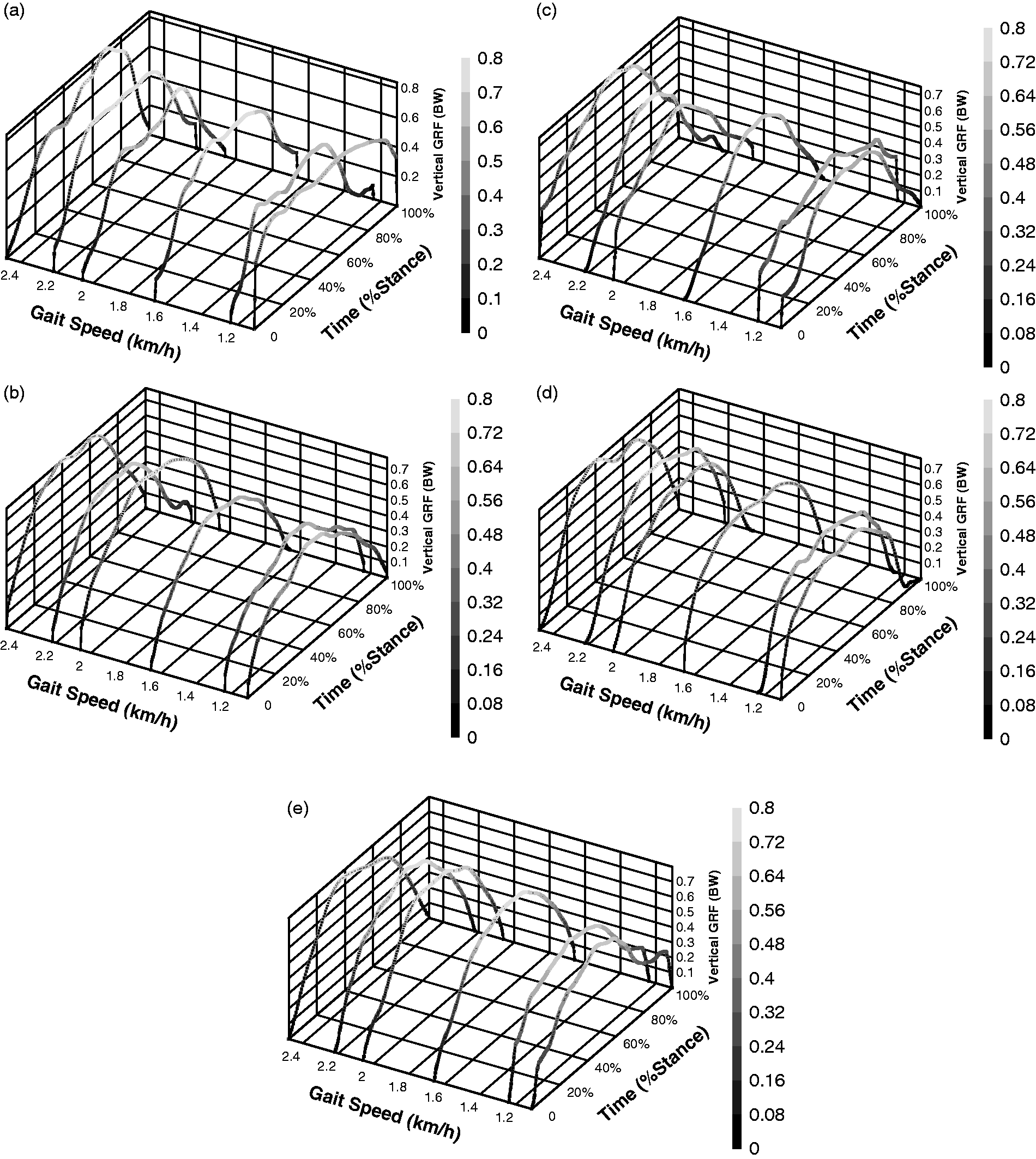
Vertical GRF–time histories of (a) subject 1; (b) subject 2; (c) subject 3; (d) subject 4; and (e) subject 5 for a series of walking tests on robot.
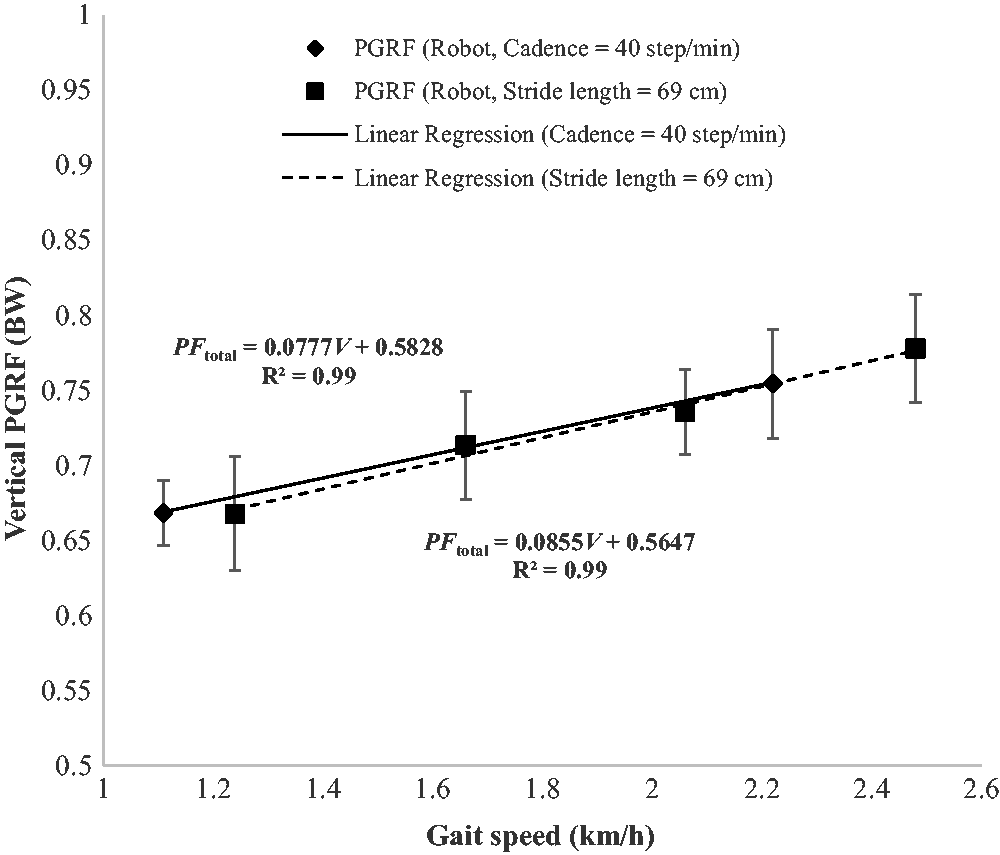
The relationship between vertical PGRF (PFtotal, in terms of BW) and gait speed (V, in terms of km/h) for walking on robot. Solid line: cadence = 40 step/min, stride length = 46 cm–92 cm; dash line: stride length = 69 cm, cadence = 30–60 step/min.
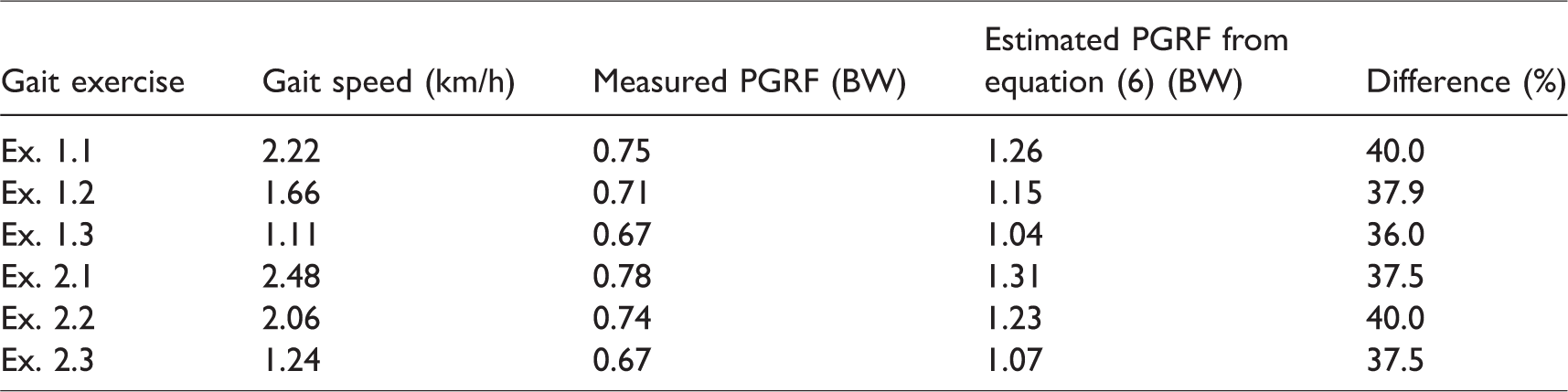
Comparison between the predicted and measured PGRF on robot
By substituting the speed of gait on robot into equation (6), the calculated PGRFs were 36%–40% higher than direct measurements from force insole as indicated in Table 3.
Comparison between the predicted and measured PGRF on robot.
Computational simulation results
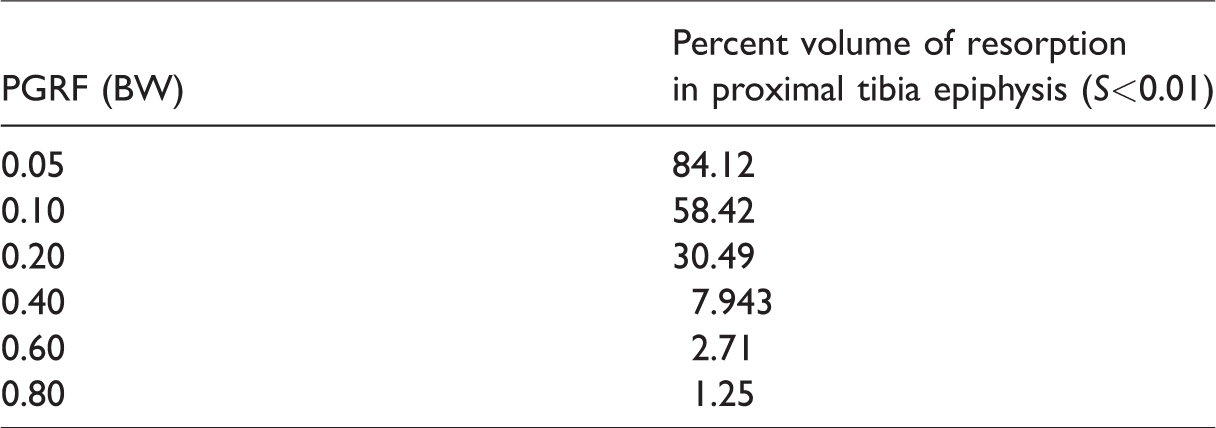
A computational model was developed in this study to investigate the influence of robot-assisted gait loading on lower extremities bone health. Figure 9 illustrates the computational model prediction of bone resorption area for proximal tibia epiphysis (at sagittal section) under different magnitudes of PGRF. The cancellous bone area with insufficient mechanical stimuli (S ≤ 0.01) was considered to undergo bone resorption. As illustrated in Figure 9, the model predicts a large area of bone resorption for sagittal section of proximal tibia epiphysis under small load-bearing conditions (PGRF < 0.2BW). Table 4 shows the computational model prediction of resorption volume in proximal tibia epiphysis under different levels of PGRF.
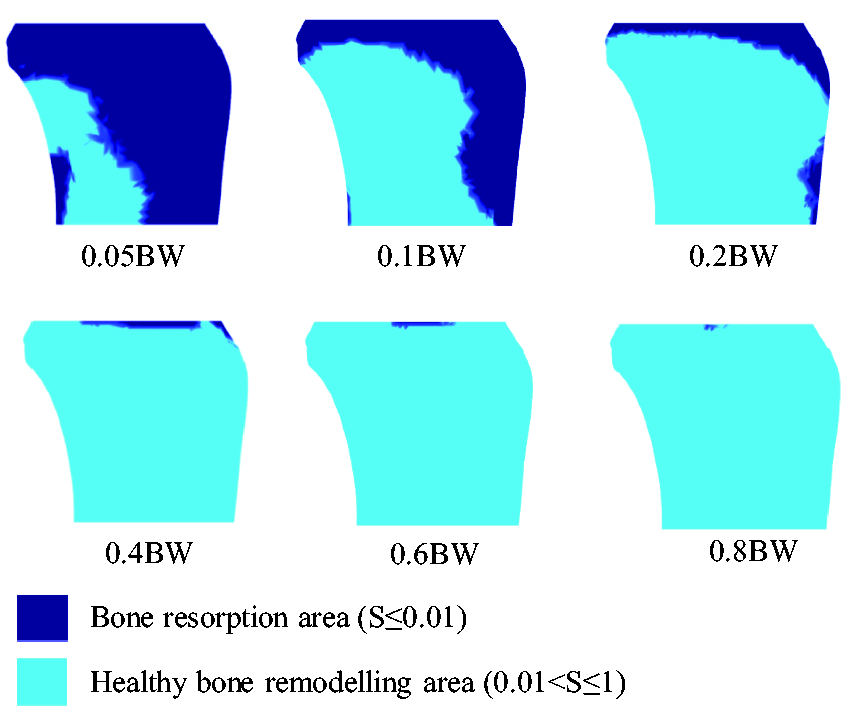
Computational model prediction of bone resorption area for proximal tibia epiphysis (sagittal section) under different magnitudes of PGRF.
Computational model prediction of resorption volume in proximal tibia epiphysis under different levels of PGRF.
Discussion
Weight-bearing exercise is considered to be an effective treatment method for enhancing bone strength and preventing osteoporosis and fragility fractures in neuro-rehabilitation.51,52 Jorgensen et al. demonstrated that stroke patients who started to walk within one-week and two-month post-stroke showed 3% and 8% losses of BMD in femoral neck of the paretic limb, respectively. On the other hand, stroke survivors with immobility for one year experienced a significant reduction in BMD of 13%. 4 Pang and Lau showed that treadmill training for six months could significantly improve the cortical thickness of stroke patients, walking endurance, and muscle strength in the paretic legs. 17 Conventional training programs have several limitations in neuro-rehabilitation. 25 The robot-assisted therapeutic therapy is developed to overcome these limitations. 22 However, very few studies investigate the feasibility of robot-assisted gait training in osteoporosis prevention for stroke survivors.
In this study, we employed both conventional treadmill therapy and robot-assisted gait therapy to quantify the effects of weight-bearing exercises in the biomechanical environment of bone. The PGRFs generated by weight-bearing activities on treadmill was determined by force insole for a wide range of normal walking speed (i.e. 1 km/h–6 km/h). The measured vertical PGRFs are slightly higher than those reported in Keller et al. 53 and Chiu and Wang 54 who investigated the vertical PGRFs of weight-bearing exercises overground. It is demonstrated that normal gait for walking features double-peaked pattern (in GRF–time histories). The first peak generally occurs when the whole foot is in contact with the ground between 18% and 28% of the total stance time, whereas the second peak takes place during push-off phase between 70% and 82% of the total stance time. Our results show remarkable agreement with the published results.53,55 The vertical PGRF increases with the increase of walking speed in linear manner up to 6 km/h (R2 = 0.97), which is in good agreement with the reported results.53,56 A linear regression equation (i.e. equation (6)) is proposed in this study for estimating the vertical PGRF for normal walking speed.
On the other hand, the GRF–time histories for robot-assisted walking only exhibit a single-peaked value located at approximately 41%–50% of the total stance time for walking speed up to 2.2 km/h. Such gait pattern is similar to forefoot strike pattern, meaning no significant impact transient is observed in the GRF–time history curve. 57 The magnitudes of the PGRF generated by weight-bearing activities on robot are in the range of 0.67BW–0.78BW which is significantly lower than those measured on the treadmill. As the subjects are guided by the robot to walk in a fixed place, it is required that their feet is placed and braced on the footplates of the robot. The continuing contact between the feet and footplates diminishes the heel strike and push-off effects on walking, leading to no significant impact transient in the experiment. Another explanation of the reduced PGRF is that the interaction forces and torques between human and robot might impose false loading. 22 For the parametric study conducted on robot, both cadence and strike length affect the gait speed, which ultimately change the vertical PGRF. As indicated in Figure 8, the solid line represents the relationship between vertical PGRF and gait speed for cadence = 40 step/min, stride length = 46 cm–92 cm, while the dash line represents the relationship between vertical PGRF and gait speed for stride length = 69 cm, cadence = 30–60 step/min. Interestingly, the lines are nearly overlapping with each other, revealing gait speed is the main factor which affects the vertical PGRF.
Healthy bone remodeling process requires a balance between bone resorption by osteoclasts and bone formation by osteoblasts. 58 Exceeding bone resorption over bone formation causes an imbalance in skeletal turnover, leading to the development of osteoporosis. 59 Weight-bearing exercise is believed to be a low-cost and effective anti-osteoporosis therapy method that promotes osteoblast function. 60 It is well known that the biological actions of osteoblast and osteoclast exhibit a threshold behavior which depends on the intensity of mechanical stimulation. The mechnoregulation theory proposed by Prendergast et al. 43 was adopted herein to investigate whether the gait exercises conducted on static robot will generate sufficient loading for osteoblast activity based on our well-established computational model. Different magnitudes of vertical PGRF expressed in terms of BW are used in computational simulation. As indicated in Table 4 and Figure 9, 0.6BW and 0.8BW are associated with 2.71% and 1.25% bone resorption volume in proximal tibia epiphysis, respectively. Considering the loading generated by gait training on robot ranges from 0.67BW to 0.78BW, the computational model results suggest that the robot-assisted gait loading can significantly reduce the risk of bone resorption and osteoporosis for patients with limited mobility.
The purpose of this study, in fact, is to develop a theoretical framework which can quantify the effects of weight-bearing exercises performed using robot-assisted devices on the mechanical microenvironment of bone, ultimately the bone homeostasis. Preliminary studies involving five volunteers were carried out to assess the workability of the developed framework. A series of clinical studies involving a large number of participants should be carried out to validate the model predictions. There are some other limitations of this study. Firstly, the gender effects on the GRF are not investigated. Secondly, the robot employed herein is static robot which constrains the subjects to exercise in a fixed place. A dynamic exoskeleton system, allowing participants to move around the environment, could potentially generate gait patterns that are similar to normal gait. Last but not least, a computational proximal femur model should be developed for investigating osteoporotic problems in our future studies.
Conclusion
The application of robot-assisted therapy in neuro-rehabilitation has drawn increasing attention to clinicians and researchers. The investigation of the effects of weight-bearing exercise on bone health requires accurate measurement of GRF. In this study, force insole and static robot were employed to study the effects of robot-assisted gait therapy in the biomechanical environment of bone required for the prevention of osteoporosis by conducting a series of walking exercises. A computational model was developed to analyze the percent volume of bone resorption in proximal tibia epiphysis under different intensity of weight bearing. The computational results suggest that static robot can be used to reduce the risk of bone resorption, and hence prevent development of osteoporosis for motor impaired patients.
Footnotes
Acknowledgments
We are grateful to the Radiology Department, The First Affiliated Hospital of Shenzhen University, for their technical support on tibial CT scan.
Authors’ contributions
Conceptualization, Shanshan Guo and Yulong Wang; methodology, Guo Shanshan, Yulong Wang and Yi Yang; GRF measurement on treadmill and robot, Kun Wang and Jianjun Long; CT scan, Zhiyong Huang and Xing Lv; 3D reconstruction, Saeed Miramini; data Analysis, Kun Wang and Lihai Zhang; resources, Zhiyong Huang and Yulong Wang; writing-original draft preparation, Shanshan Guo and Yi Yang; writing-review and editing, Lihai Zhang and Yulong Wang; visualization, Jianjun Long and Saeed Miramini; supervision, Yulong Wang; project Administration, Shanshan Guo; funding acquisition, Yulong Wang.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Rehabilitation Center, The First Affiliated Hospital of Shenzhen University. The funding was obtained from LiJian’an’s team of academicians, Shenzhen Sanming Project (code: SZSM201512011).