
Abstract
Objectives
This study explores the governance intricacies in establishing a large-scale information infrastructure for integrated care within the National Health Service of England. By focusing on the initial 5 years of a regional interoperability program, we examine the challenges and dynamics of creating a unified system across organizational boundaries.
Methods
A longitudinal multi-methods approach was utilized, collecting data through interviews with health and social care personnel involved in project governance, meeting observations, and document analysis. This provided an in-depth understanding of the processes and challenges of developing the regional interoperability program.
Results
This study reveals a dynamic negotiation process and evolving governance structures that must continuously adapt to integrate diverse systems. Key findings include challenges in reconciling multiplicity and heterogeneity, the importance of social learning and stakeholder adaptation, and the role of ongoing negotiation and collaborative group construction in implementing interorganizational infrastructures.
Conclusion
This study underscores the necessity of continuous adaptation and negotiation among stakeholders in establishing effective governance of integrated care infrastructures. Social learning and active participation play pivotal roles in overcoming the challenges associated with system integration. Strategic insights from this research can guide stakeholders in developing sociotechnical solutions for digital interorganizational infrastructures in integrated care.
Keywords
Introduction
Aspirations to improve the efficiency, quality, safety, equality, and experience of care for both patients and clinicians – termed by some authors the quintuple aim 1 – are driving attempts to digitally integrate health and social care at scale. The present emphasis on integrated care and patient centricity, with care services to be designed and built around patient needs, encourages the integration of health and social care services within ecosystems of care, generally based on geographic proximity.2–4 While some early movers in the National Health Service (NHS) of England – the nation-wide state institution providing universal and free-at-the-point-of-delivery healthcare – launched such implementations in 2014, most regional health information exchange initiatives – originally entitled Interoperability Programmes, then Local Health Care Record Exemplars, and then Shared Care Records – have been implemented since 2018.5–7 These initiatives are intended to provide health information exchange services and information systems interoperability between primary, secondary, and social care within the same geographic area. 8 Contrary to nationwide efforts, these implementations are not centrally governed; rather, they are organized locally, with representatives from clinical entities within a region overseeing the delivery of each project.
While the promise of transformation through integrated health information systems has been present for many years, implementation and adoption has proved challenging and results have varied.9,10 Large-scale information systems are expected to connect and facilitate the flow of information between multiple actors. In contrast to horizontal data integration within a linear supply chain or between entities and organizations providing specific services,11–13 the development of shared digital spaces for cross-boundary data integration is substantially more complicated. The need to accommodate a non-hierarchical and dynamic supply chain results in a complex ecosystem, in which care is delivery through fragmented and often overlapping services distributed across diverse clinical organizations and actors.
The process of clinical data integration and interchange across the NHS in England has not been straightforward. The complexity of healthcare and the multiplicity of NHS organizations have created a disorganized and fragmented ecology of platforms, resulting not only in problems relating to expenditure and the duplication and fragmentation of data but in limitations to systems interoperability. 14
Integrating and sharing data across multiple organizational boundaries on a large geographical scale is a complex, ongoing socio-technical process. It involves numerous actors, lengthy negotiations, diverse organizational cultures, asymmetrical data exchange, political tensions, and overlapping regional administrative organizations. 15 This paper examines the governance of designing and implementing a regional Shared Care Records (SCRs) within the NHS, aimed at integrating diverse health and social care entities.
Technically, SCRs are e-health platforms designed for use across organizational and occupational boundaries, integrating information from various providers like GP surgeries, specialists, hospitals, laboratories, and pharmacies.16,17 While SCRs and interoperability are distinct concepts, they share similarities and are used interchangeably in this project. SCRs integrate, store, and manage clinical information across boundaries, whereas interoperability encompasses the broader process of exchanging, interpreting, and effectively utilizing information among various technological components.18,19 By examining the governance processes during the conceptualization, prototyping, and implementation of this platform, this study explores the complexities of establishing large-scale information infrastructures for integrated care within NHS England.
Methods
This qualitative study examines the initial 5-year development period (2014-2019) of an NHS interoperability program and SCR platform across a 500 mi2 region in Southwest England. By employing a longitudinal and multisite approach, we gained comprehensive insights into the evolution and governance of a large-scale interoperability initiative. 20 The author conducted this study as a researcher in large-scale information infrastructure innovation, with training in computer science, organizational studies, and social science.
Data collection
Data was collected from public documents, observations of governance meetings, and 50 interviews with NHS and social care personnel involved in the project’s governance and development. Interviewees were purposively selected from participating organizations, including Hospital Trusts, Local Authorities, GPs, and NHS administrative entities (e.g., Commissioning Support Unit, Clinical Commissioning Groups, and Integrated Care Systems). Additional interviews were conducted with experts from other regions engaged in similar interorganizational efforts. The author had no prior interaction with participants before the study. Interviews, lasting 40–60 min, were conducted either online or in person at NHS workplaces.
Interview questions were developed in alignment with the research objectives and informed by a review of relevant literature. The questions were original and did not require copyright permissions. A pilot study with five participants was conducted early in the data collection process to refine and validate the questions, addressing any ambiguities. Participants were initially contacted via email and provided informed consent after being informed about the study’s purpose, the researcher’s qualifications, and his interest in the topic. No patients or their caregivers were interviewed. Follow-up interviews were conducted with six participants based on their roles in the project, further exploring topics and validating initial findings. Non-participant observation of six governance meetings, totaling 12 h, provided additional qualitative insights into meeting dynamics and discussions.
Data analysis
Transcribed interviews and observational notes were analyzed by the author using qualitative analysis software NVivo12. We conducted a longitudinal and interpretive analysis to identify key sociotechnical themes in the development of the interoperability program. These themes encompass the sociotechnical dynamics and challenges associated with enhancing large-scale digital infrastructure, negotiating agendas, configuring governance frameworks and implementation processes, and integrating the installed base of sociotechnical systems at local settings. Data saturation was reached after 40 in-depth interviews, with no new themes emerging beyond the 40th, only reinforcing existing ones. Analysis also involved examining relevant public documents and official websites, as well as the organizational and digital trajectories of participant entities.
Theory and conceptual framework: Infrastructures in the making and the potential for connecting multiple organizational contexts
As information systems grow in complexity, encompassing a broader scale, scope, and diverse components, they take on the characteristics of an infrastructure of systems interconnecting with other systems. 21 In this context, we employ the term Information Infrastructures (IIs) to describe systems of systems that evolve over an established base of other systems.22–25 The concept of IIs transcends mere structures of information to encompass the networks facilitating information circulation, the hardware for storage and processing, the software managing this information, 26 and the actors shaping its use and practices. 27 The development of IIs is characterized by a diversity of agendas, contexts, and user bases,28,29 as well as the design constraints imposed by the installed base of pre-existing systems and practices. 23
While many regions and small countries aspire to integrate previously separate healthcare services and establish access to integrated clinical data, achieving system integration at scale poses a significant sociotechnical challenge. This challenge requires effective governance, and configuring such governance in non-hierarchical scenarios is not a straightforward task. 30 It is imperative, however, not to assume the potential for connectivity and evolution of IIs. The development and progression of IIs depend on aligning and coordinating various elements through the stages of emergence, construction, stabilization, and evolution. Designing and constructing IIs involve a detailed negotiation process within intricate and varied environments. These processes must address not only multiple agendas and interests but also unseen factors that can profoundly influence the outcomes and utilization of the infrastructure. For instance, features that are commonplace in one community may possess different contents or meanings in another, emphasizing the need for careful consideration of contextual variations in II design, implementation and use.29,31
As Figure 1 illustrates, this study adopts a processual perspective of the ongoing design and utilization of IIs, commonly referred to as “infrastructuring”.32–34 This concept describes a continuously generative system of interrelated activities intended to advance the infrastructure.
33
Notably, this dynamic lacks clear guidance from a singular “visible hand,” as boundaries between actors and processes are often ambiguous, and there is a lack of shared terminologies and perspectives among stakeholders.
32
Within these conditions, learning plays a pivotal role in II development. Social learning, defined as the reciprocal and evolving process between users and artifacts over time, underscores the significance of the adoption phase for technology to achieve functional maturity.35–37 We extend on this concept to encompass the collective learning process that stakeholders from diverse communities of practices and organizations undergo when collaborating to articulate, design, and implement complex IIs. Conceptual framework: Development of Information Infrastructures.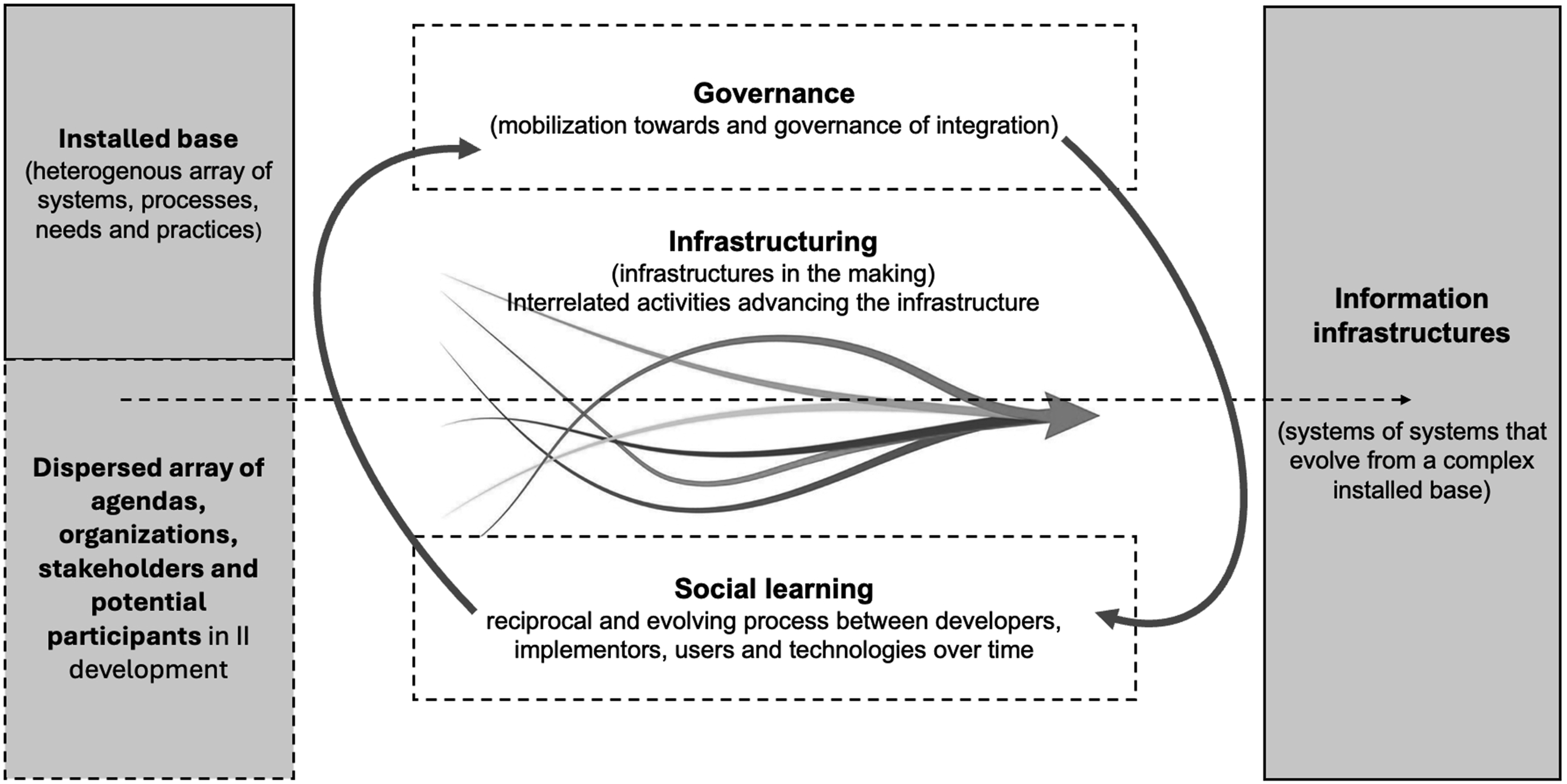
Case study: Infrastructuring a regional SCR in NHS England
In 2014, with the introduction of the Five Years Forward View, 38 the NHS implemented new policies intended to foster a more collaborative approach between health and social care entities, and more efficient methods for exchanging, integrating, and accessing data. Unlike the highly centralized model of the previous and somewhat limited National Programme for IT (NPfIT), the new plan advocated the development of regional digital infrastructures to enhance interoperability. 14 This case details the initial 5 years of the infrastructuring process for a regional SCR in South West England. Commencing in 2014, the region was an early interorganizational initiative adopter. The project aimed to consolidate clinical and care information from over 120 organizations spanning primary, secondary, and social care. These entities were distributed across a geographic area of around 500 square miles, serving a population of approximately 1,000,000 inhabitants.
According to the official narrative, the project was framed as an interoperability program with three primary objectives: facilitating the sharing of clinical data between health and social care; enhancing interactions between patients and health professionals; and bolstering health intelligence by applying actuarial thinking to health data.39,40 The organizations projected to integrate and share data included two acute Hospital Trusts, over 100 GP surgeries, six Local Authorities providing Social Care, and a large Mental Health Hospital Trust that, having gained international recognition for delivering improvements in care quality through world-class use of digital technologies and information, had been awarded the status of Global Digital Exemplar. 41 All these organizations had high levels of autonomy in resource administration and decision making. The installed base of Electronic Medical Records (EMRs) and SCRs across the region encompassed several systems: GP surgeries in primary care employed EMIS, Vision, TTP, and Microtest; the Mental Health Trust used RiO; an Acute Trust had recently implemented Cerner; and another Trust was migrating from a “best of breed” approach to a yet-to-be-procured EMR. For Local Authorities providing Social Care, record systems included RAISE, Liquid Logic, Opentext, EDMS, PARIS, and Frameworki.
The regional project was intended to create an additional layer to facilitate interoperability, data exchange, and integration among these systems, and thus enhance care, foster inter-organizational collaboration, and improve efficiency. The process of infrastructuring commenced under the auspices of two NHS region-based administrative bodies, who convened the participating entities, promoted the initial idea of interoperability, and, in collaboration with representatives from participant organizations, managed to establish an interorganizational governance body for the project.
The governance body supervised the design, implementation, and adoption of the interoperability platform. Following numerous discussions, negotiations, iterations, and proofs-of-concept regarding the meaning of interoperability at a regional level, an infrastructure was conceptualized. This infrastructure required the extraction, normalization, and storage of locally-based data dispersed across the heterogeneous installed base of EMRs and SCRs into a central regional repository. As illustrated in Figure 2, data were integrated and fed into multiple components: a SCR containing integrated patient information for use by health and social care professionals; a Patient Portal, in which the integrated data was rearranged for use by patients and/or caregivers; and Population Health Management, providing analytics at a regional level for use by policymakers and NHS administration. Infrastructure for regional integrated care interoperability.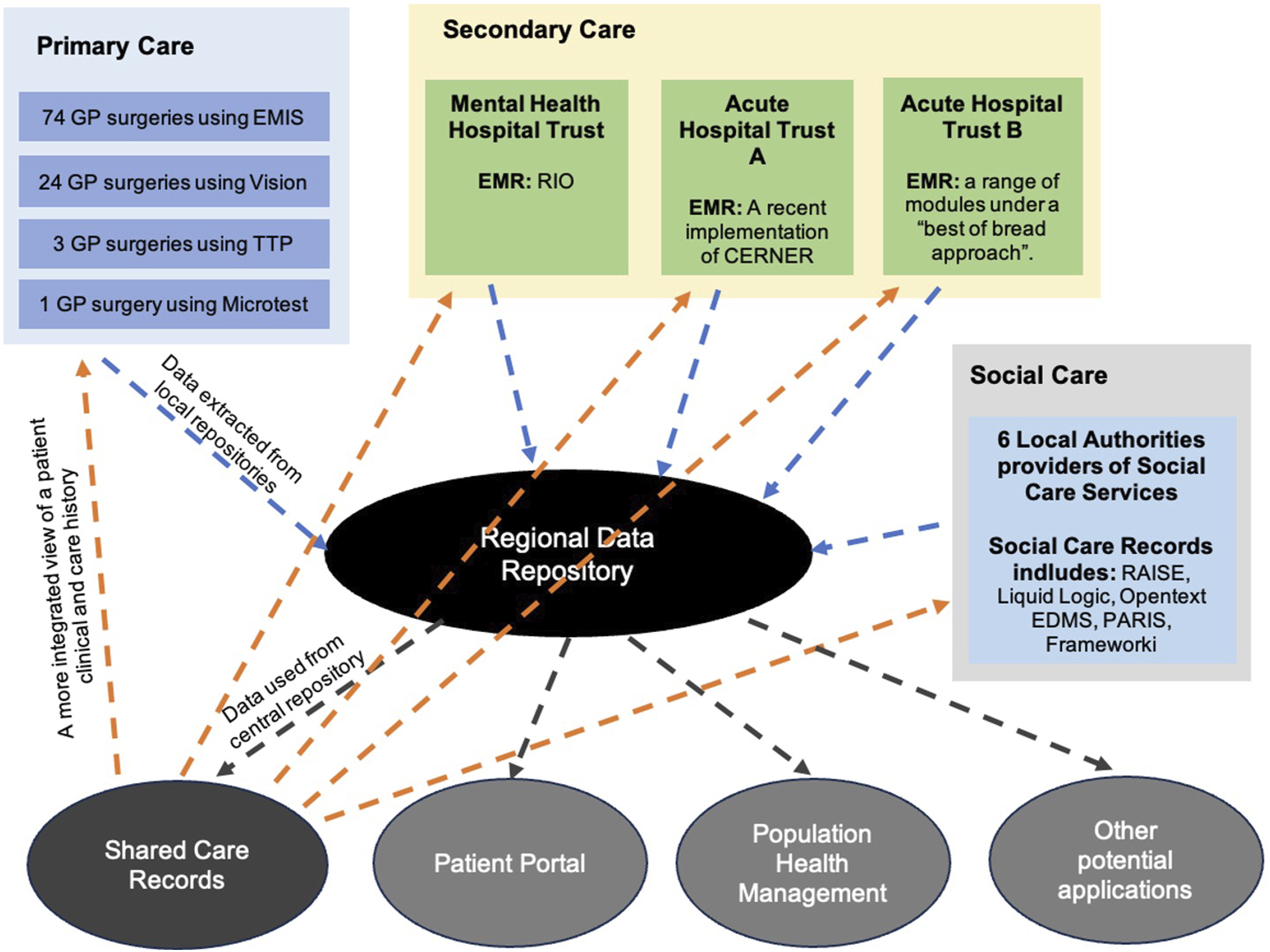
In order to organize governance and implementation of the project based on these components, three distinct implementation groups, called workstreams, were established. The workstreams comprised a variety of stakeholders from the range of organizations involved in the project. While the workstreams differed in terms of individuals, objectives, and outcomes, there were common members across the groups.
In alignment with the goals of integrated care, patient centricity, and interoperability, the principal and initial component of the project was the development of the SCR. From 2014 to 2019 the infrastructuring process for the SCR underwent various stages. As Figure 3 illustrates, there were at least four non-linear stages. The first stage (A) involved mobilization and defining a vision for interoperability. The second stage (B) included design, proof-of-concept pilots, and negotiating the data-sharing agreement. The third stage (C) encompassed selecting a supplier and the procurement process. The final stage (D) included implementation, adoption, and post-implementation. Future steps (E) contemplated potential further development and evolution of the platform. Stages in the implementation of the interoperability programme.
A lack of experience in digital interorganizational projects, along with inadequate regional protocols and entities to effectively support governance, led to slow coordination, decision-making, and learning. The first SCR version was launched after 5 years. As this minimum viable dataset had limitations, future iterations of the platform will focus on improving both the quality and breadth of integrated data, while advancing the implementation of Patient Records and Population Health Management Workstreams.
Discussion: Multiplicity, heterogeneity and learning in the governance of infrastructuring
The infrastructuring process followed a dynamic, non-linear progression, oscillating between conceptualizations, prototypes, and proofs of concept. This phase also included procuring, launching, and adopting the SCR platform, and the emergence of various uses. The concurrent development of the Patient Portal and Population Health Management components relied on the same infrastructure and data repository as the SCR.
Tensions that arose over the initial 5 years were particularly evident in relation to the conceptualization of integration and negotiation of a data sharing agreement among the involved parties. Conceptualizing the overall project entailed ongoing negotiations regarding meanings and functions, and development was significantly shaped by socio-technical dynamics throughout this initial 5-year period of collaborative work. Given the findings of this study, we make the following recommendations for governance of large-scale interorganizational interoperability projects:
Negotiating from an installed base where multiplicity and heterogeneity are the norm
The process of infrastructuring this II was characterized by an established ecosystem of care serving as the installed base, encompassing participant organizations, their services, goals, processes, practices, platforms, types of data, and users. 3 Realizing a vision for a digital infrastructure that would address and satisfy diverse contexts, practices, needs, and agendas required ongoing discussions, repeated negotiations, and multiple decisions. 42 The adoption of goal-oriented approaches, such as using patient priorities to guide a vision of care delivery, enhanced the integration process. 43
Consensus, while essential, can impede profound transformation. 44 Progress in a complex negotiation may require concessions to actors with the power or capacity to impose their agenda or demands. Empirical evidence shows that in the absence of prior experience, established structures, and pathways, pioneers must learn on the go, investing time and resources in a complex, uncertain, and risky learning curve. As a result, achieving the necessary level of group energy and building momentum can be time-consuming. A protracted learning curve and lack of group energy can jeopardize participant interest and continuity of the project.
Making sense of the project
While integration may initially appear straightforward, implementing this concept is a complicated process: new knowledge domains and inherently uncertain and ambiguous situations can emerge throughout the developmental phases, 45 and interpreting novel frameworks often lead to confusion and a lack of clarity. Interpreting these new frameworks frequently led to confusion among the stakeholders of this interoperability project. We observed that ongoing and diverse conversations were required to ensure the workstreams maintained progress, and that framing these discussions within a coherent narrative enhanced the overall process. 46 Continuous participation in workshops and events was crucial for advancing the project and addressing its complexities.47,48 From a governance perspective, creating spaces and opportunities for openly presenting ideas and concerns was crucial. Throughout the interoperability program, these spaces enabled both individual participants and broader, heterogeneous groups to carefully consider and visualize diverse opinions, and played a vital role in supporting social learning, the diffusion of ideas, and sense-making. These elements were essential for successfully implementing the SCR, as they fostered an environment where stakeholders could collectively navigate the complexities of the integration process.
Complexity and governance
As established institutional arrangements must be renegotiated, the process of moving to patient centricity produces and is shaped by friction. 49 Collective governance for integrated care relies on a complex configuration of expectations, constructive relationships, effective contributions from actors, and accountability-based results. 50 However, IIs are expected to evolve, and many of their benefits will only manifest over the long term. 51 As this case study illustrates, the development of a new shared II supporting technical interoperability demands a long-term configuration of interorganizational governance, capable of managing a diversity of expectations, the challenges of establishing an initial coherent vision between entities that may previously have been in competition, and the complexity of the installed base. As a multitude of visions and needs will generate tensions that must be continuously discussed and negotiated, working together as a heterogeneous group is a continuous learning experience.
The creation of dedicated operational linkages between participant firms 52 is integral to the governance framework. From a project orchestration standpoint, this entails the ability to articulate tangible benefits for participant organizations, the continual construction and management of relationships, and the establishment of conducive spaces and processes for design, discussion, and decision-making. Ensuring the sustained participation of organizations within the project is a crucial aspect of governing interorganizational projects of this nature.
Data asymmetries and overlapping
Significant gaps and asymmetries in levels of digitalization exist both within and between all clinical entities. 53 This diversity of contexts and systems results in variations and inconsistencies in the quality and type of data available across different systems. The challenges in reconciling agendas and tensions, managing asymmetries between systems, and addressing local needs while creating value for all participants in a digitalization project escalate as the number and diversity of actors, systems, practices, and incentives increase. 54
The implementation of integrated care models is complex due to the diversity of organizations and information systems, coupled with asymmetries in digital capacity and experience. In this regional interoperability program, unanticipated issues, tensions, delays, and limitations arose from disparities in digital maturity and data quality among participant organizations, the multitude of actors, systems, and data, and the overlap in NHS regional administrative agendas. Data quality disparities stemmed from distribution across multiple repositories and the varied nature of collection points. Primary care, which began digitalization decades earlier, produced rich longitudinal data repositories. In contrast, the fragmented secondary care sector focused on specialized services, with some Hospital Trusts still implementing Trust-wide EMRs during the project’s initiation. Social care data were less structured and more contextual. The diversity of information systems across the region led to data asymmetries, gaps, and overlaps that hindered integration.
This project underscores the challenge of determining data inclusion in an SCR when integrating diverse sources. Including too much data can impact usability and create challenges, particularly for frontline users managing complex information. Criteria such as providing a functional view of patient history, improving support for patient communication, reducing information requests from GP surgeries, and assessing data quality can guide decisions on the common dataset for a minimum viable solution. In developing this SCR, the dataset included medications, allergies, and indications of long-term conditions.
Network and membership
As interorganizational information systems, SCRs contribute to linking multiple organizations, practices, information systems, and data within an ecosystem of care, and facilitating integrated care by articulating complementary and interrelated services in a more efficient way. 3 Once the key actors had been identified in the initial phases of this project, it was crucial to persuade them to participate.54,55 Mobilizing autonomous actors is a significant challenge in ecosystem-wide developments, 56 partly due to the difficulty of defining or articulating a vision. 57 An overarching initial vision of integration, coupled with a transparent delineation of the specific local benefits for each organization, can provide essential support for mobilization.
As SCR development involves a process of group construction, a group of participant organization representatives must be configured and aligned to oversee governance of the process, and convergence and interaction among actors maintained throughout the infrastructuring process. 54 Previous collaborations between some participant organizations, together with geographical proximity and access, played a vital role in shaping the network in this regional interoperability program, facilitating in-person interaction through meetings and workshops across the region. These dynamics contributed to strengthening the governance group and reinforcing inter-organizational alliances. However, over time, earlier discussions, decisions, and experiences became ingrained in the taken-for-granted, common knowledge of the group, enhancing cohesion but also making this knowledge difficult to visualize, express or challenge. As user needs were identified, the vision enriched, and expectations made more explicit, this common knowledge became a potential barrier for future membership. Recognizing this phenomenon is crucial as it enables the creation of mechanisms for knowledge transfer when incorporating new participants and scaling up the project.
A critical trade-off concerning the inclusion of new actors beyond the confines of the original region can arise at some point of the infrastructuring process. While there may be pressure to expand the system by incorporating additional Hospital Trusts, GP surgeries, and Local Authorities, existing evidence indicates that complications tend to escalate with an increase in scale.51,58 The decision to introduce new entrants may depend on strategic necessity and political considerations, the stability and maturity of the II, the compliance of potential new entrants with interoperability standards, the commitment of new entrants to the dynamics of the interorganizational group, and the functionality and maturity of governance processes.
Limitations of this study
As access was only available to the perspectives of a certain amount of key governance stakeholders, the diversity of organizational representation was limited, and local-level decisions and dynamics within individual organizations were not taken into account. A reliance on documents and to reconstruct the early stages of the project may have introduced interpretive biases and, due to the need to protect patient confidentiality, we were unable to observe e-health technology users. Lastly, the focus on a single region limits comparability, which is crucial for a more robust understanding and assessment of common challenges and hypotheses.
Conclusion
The healthcare industry encompasses highly specialized services, practices, and processes with diverse data and user needs based on specialization, context, and location. While satisfying local data needs is critical, it is equally important to efficiently interchange, access, and integrate data across settings. This represents a foundational condition for enhancing the quality, safety, efficiency, and sustainability of care. Following the international failure of many nationwide one-size-fits-all digitization projects – including NPfIT – due to the scale and complexity of services and entities, data integration efforts in NHS England shifted to modernizing local EMRs to comply with contemporary standards and setting-wide integration. Over the past decade and almost in parallel, policies promoting integrated care have underscored the need to align local practices, systems, and data needs with broader healthcare ecosystem requirements through interorganizational interoperability.
This study elucidates the governance challenges in developing large-scale IIs for integrated care. Our findings highlight the ongoing dynamics of negotiation, learning, and collaboration necessary for successful implementation in a complex healthcare landscape. Integrating diverse organizations and platforms requires reconciling various expectations and tensions, mobilizing stakeholders, and managing asymmetries in the existing infrastructure. While effective governance must adopt standards and technologies that facilitate integration, stakeholders also need collaborative skills to manage complex relationships, foster group dynamics, and build trust. Geographical proximity, access, and frequent interaction are crucial, supported by coordination tools for discussions, negotiations, and sense-making activities. Effective governance of interoperability programs requires understanding two related dynamics: infrastructuring as infrastructures in the making and social learning as the process of making sense of technology.
Footnotes
Acknowledgements
The author wishes to extend their gratitude to the Programme for Competitiveness, Innovation, and Human Capital, Ministry of Science and Technology of Costa Rica, for their support of this research. Appreciation is also due to the National Health Service of England for providing access and allocating time essential for the successful completion of this study.
Author contributions
Andrey Elizondo is the sole author of this study, responsible for its design, data collection, analysis, manuscript writing, and subsequent revisions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Program for Competitiveness, Innovation and Human Capital, Ministry of Science and Technology of Costa Rica. Funding grant number: MICITT-PINN-OF-0481-2017.