
Abstract
Keywords
Background and rationale
Patient-targeted googling (PTG) involves health and social care professionals using Internet search engines to source information about people in their care. 1 For the purposes of this review, ‘Googling’ is used as a general term to cover all available search engines. There are reports of the benefits of using PTG but also known risks and ethical tensions. These include harm to the patient-professional relationship, particularly for those with mental health conditions.2,3 Research literature indicates that PTG is used in professional practice for example, where there are concerns for patient safety.4,5 However, literature reports that professionals struggle to navigate the ethical tensions surrounding PTG and no research has yet provided guidance about when PTG is acceptable and why.
Professional registrants are accountable to regulators such as the Nursing and Midwifery Council (NMC) (regulating nurses, nursing associates and midwives in the United Kingdom, UK), State Medical Boards (regulating physicians in the United States of America, USA). They produce professional codes of conduct (e.g. NMC The Code, 2018 6 ; New Zealand Medical Council, Good Medical Practice, 2021 7 ) outlining the values and behaviours expected of registrants. They also produce guidance about specific areas of practice like social media use (e.g. Health and Care Professionals Council, HCPC, 2023. 8 Practitioners must be able to explain the rationale behind their actions or omissions, acting with a duty of care to the people in their care. When engaging in PTG they need to be able to account for their decision to use PTG and ensure that it does not breach professional codes of conduct.
Regulation is influenced by both ethics and law, when making professionally related decisions it is important to take an ethical, legal and regulatory approach. 9 Often, regulators provide guidance or a ‘rule’ for professionals to follow when making decisions but there is no such guidance for PTG.
Rationale
For over 10 years, literature has called for professional guidance, policy and/or training on the topic of PTG.5,6,10–13 It is acknowledged that there is guidance for professionals about the use of digital platforms such as social media. 12 However, these do not explicitly address the issue of PTG and are more focused on how professionals should behave online (i.e. their own digital footprint).
International research literature on the topic of PTG primarily focuses on mental health, counselling and psychotherapy professionals.2,6,14,15 Cox et al 2 conducted a narrative review like the one we report. Their data included research that was over 10 years old and only focused on counselling and psychiatry, it also focused on prevalence rather than opinion and perspectives. The Internet and available information on the Internet, along with people’s confidence with and perspectives of the Internet has changed significantly in the last 10 years.15–17
It is known that PTG is used by other health and social care professionals4,13 and that it can be of benefit to patients.10,18 However, in the absence of guidance and policy about how and why it can be used, which means that there are ongoing ethical tensions and governance issues associated with the use of PTG in practice. 2 This highlights a significant gap in knowledge and guidance about when, how and why it can be used to benefit patient care. Currently, there are no published narrative or systematic reviews that synthesise research literature across all fields of health and social care. And we are not aware of any research that offers practical recommendations or guidance about why and how PTG should be used.
This narrative review is therefore the first to thematically synthesise current research literature and make practical recommendations for professionals considering using PTG in their practice.
Research questions
The SPICE (setting, population/perspective/intervention/evaluation) framework was used to structure our research question, ‘What are health and social care professionals’ (legal and ethical) perspectives/opinions of PTG and in what circumstances is it professionally acceptable to engage in PTG?’
This question allowed for research evidence across health and social care to be included (not solely mental health and counselling) but also allowed for thematic analysis of why it is being used, how it is being used, what ethical tensions exist and how these may be mediated. Our aim was to fill a gap in knowledge by producing practical recommendations for the use of PTG in practice so that practitioners can use it for the benefit of patient care within the remit of professional codes of practice. 19
Methods
A narrative review was selected as opposed to other approaches as it allowed for the synthesis of different opinions, perspectives and a broad range of research methodologies.20,21 This allowed for the generation of theories from international, contemporary research on PTG. 19 The key steps as reported by Sukhera 17 were followed.
Six databases were searched, The Allied and Complementary Medicine Database, CINAHL, MEDLINE and APA PsycInfo and ProQuest. These databases were selected based on the relevance to health and social care professionals. The search was conducted 1st July-31st August 2023.
The review protocol was registered on PROSPERO CRD42023474248. The quality Scale for the Assessment of Narrative Review Articles (SANRA) 20 was used to develop the protocol and in the comprehensive reporting of this review.
Searching
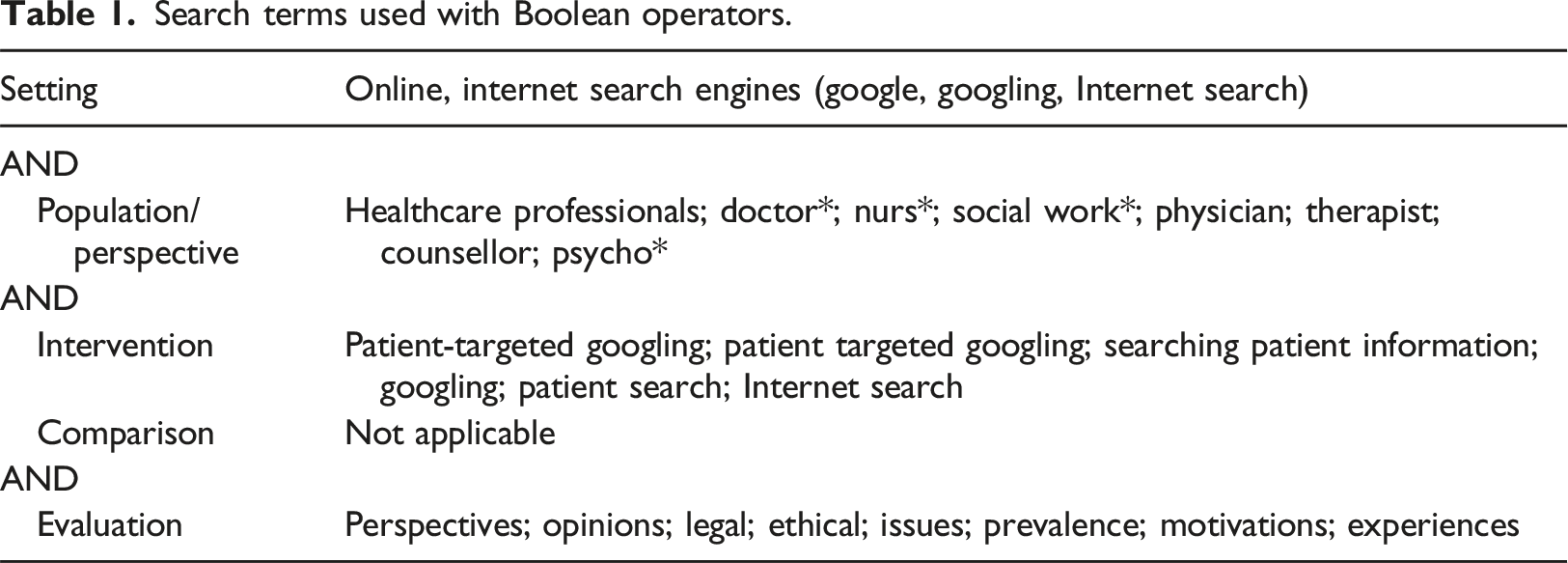
Screening
All types of empirical research were included in the review to capture a broad range of opinions/perspectives.20–23 Articles that were not published in English or that focused on patient/public perspectives were excluded. Given the significant diversification of the Internet and use of it in the last 10 years, 15 articles were only included if they were published from 2013 onwards. This ensured that the included research was contemporaneous. Studies must have included registered health and social care professionals.
Sampling
The lead author read through each title and abstract to assess eligibility against the screening criteria. Following initial screening a full text review was carried out to assess eligibility. Three of the authors reviewed each full text article prior to proceeding with quality appraisal. References in the eligible articles were reviewed for other potentially relevant studies not identified via the database searches.
Analysis
Data was extracted from the aim, results and discussion sections of each article and tabulated using Microsoft Word. Publication details, author, year and location were recorded along with design, sample size, participant characteristics, analysis method(s), results and conclusions.
A five-stage thematic analysis described in Fryer 21 was employed after uploading the included articles into NVivo One (a piece of qualitative analysis software that allows for highlighting and coding of common themes/topics in documents). This approach was chosen because it aligned with the aims of our research question, (a) explanation of what and why a phenomenon is how it is and, (b) conceptualisation and theorisation of a phenomenon to make practical recommendations. Themes were generated as part of the analysis process which involved familiarisation with the research data, development and application of codes, review high level themes (reported in results) and generate conclusions (reported in discussion). Supplementary file one provides an example of the coding framework that emerged.
Quality appraisal
Each article was quality appraised using Joanna Briggs Institute (JBI) quality appraisal tools. 22 These were chosen as they reflected the diverse nature of methods used in the published research on the topic of PTG. Articles were appraised by two researchers from social work and mental health/health visiting backgrounds. A third reviewer was available where there was disagreement between first and second reviewers and to ensure robustness of quality assessment and synthesis. Scores of 70%–100% were considered high quality, 50%–69% of medium quality and 49% or less, of low quality.
Results
Summary of included articles
Following the literature search, 156 items were found. Of these, 22 were removed before screening, and following screening, 109 were excluded. Primary reasons for exclusion were because the articles were not focused on PTG, were not research or were outside of the years of scope for this review. Twenty-five were reviewed in full text and 19 included in the final review.
A summary of article location, field of focus and methodology.
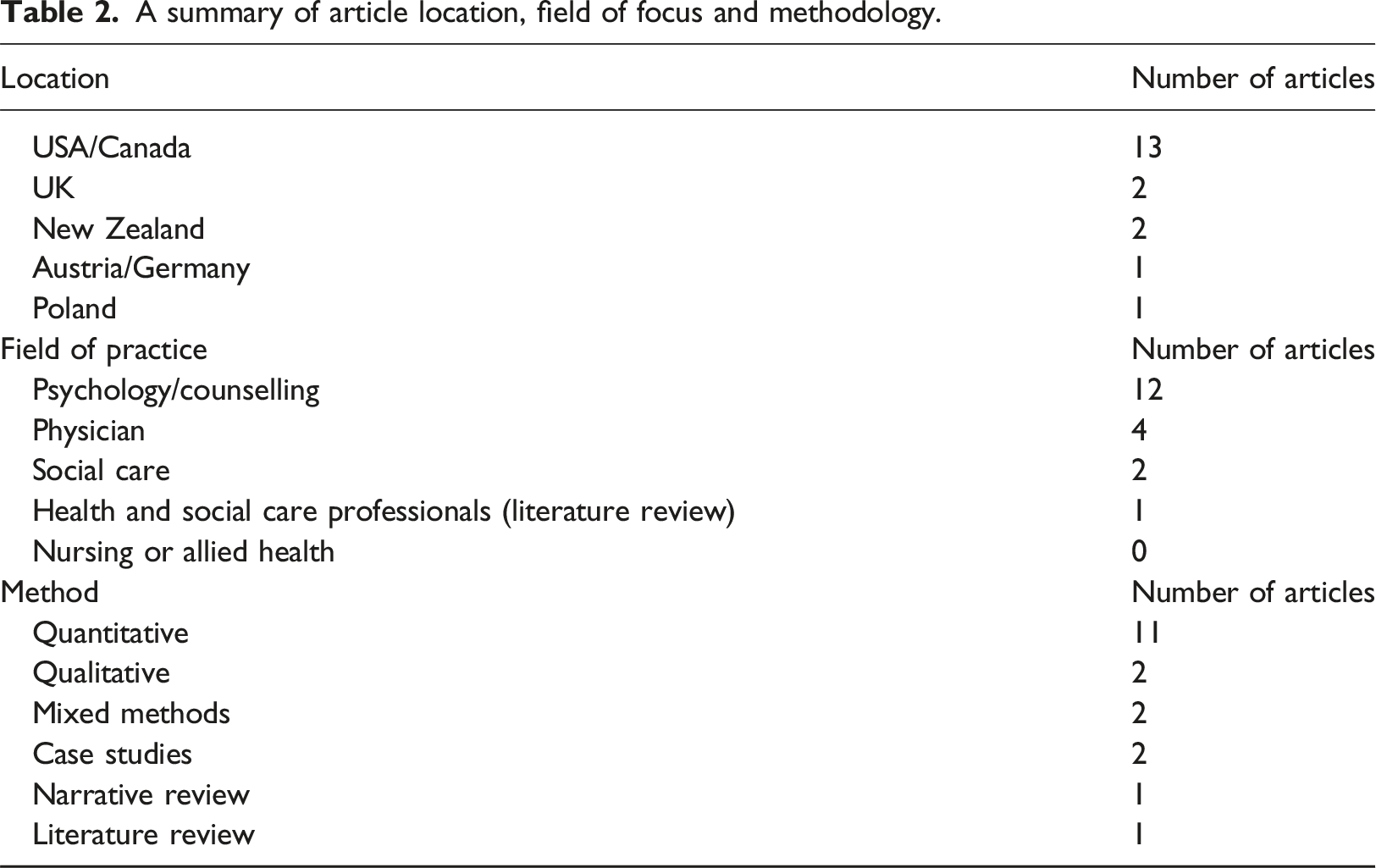
Cox et al 2 conducted a narrative review and was included as it met our eligibility criteria. The references included in Cox et al were used to identify any articles that had not been included in our results. Three of the articles included in Cox et al 2 review were published before 2013 and therefore, outside of our eligibility criteria.
Case examples presented in Baker et al 10 and Ince et al 16 , although not deemed to be ‘empirical’ research, did score highly for this type of study. These articles were important as they provided real world examples of how PTG had positive impact on care and practice. The two low scoring articles1,3 were a pilot study and a literature review respectively. Gershengeren 1 was limited in quality primarily because it was a small single centre pilot study and Zurzyka et al 3 was limited in quality due to lack of detail about method.
Summary of themes
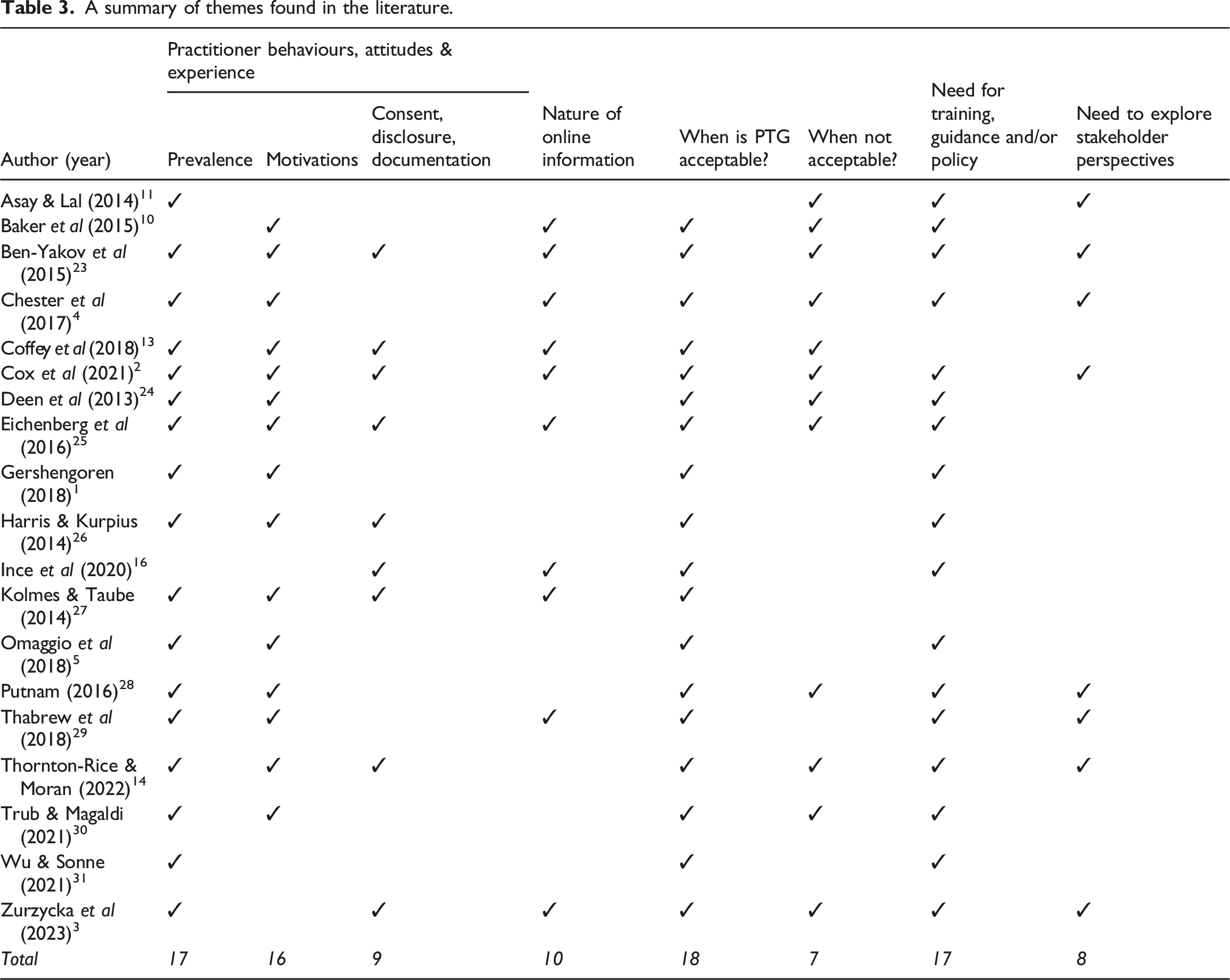
A summary of themes found in the literature.
Practitioner behaviours, attitudes & experience
Prevalence
Prevalence of PTG was diverse, ranging from 16.7% 4 and 98%, 2 the lowest percentage were final year medical students and highest psychology doctoral students. This finding indicates potentially large disparities in practices relating to PTG across health and social care. PTG seems to most commonly be used in mental health related fields and emergency departments. Possibly because there is increased prevalence of safeguarding concerns or risk of harm that require immediate attention in these environments.24–28
Motivations for PTG
Reasons for PTG reported by professionals included curiosity, safeguarding, emergency situations, criminal and civil forensic investigations.1–5,7,13–15,19,26–32 There is ethical debate about the act of PTG and noted tensions between providing good patient care, adherence to professional regulatory standards and ethical frameworks that underpin these (apart from Ince et al 16 and Baker et al 10 ). Of the research that reported on the ethical perspectives on PTG, most articles claimed that it is unethical. However, many of these went on to conclude that there is a need for training and regulatory guidance. This might suggest that professionals want regulatory ‘permission’ to conduct PTG in specific circumstances and would like guidance about when it is deemed ethical by regulatory bodies.
Motivations for PTG were rationalised in three main ways, (i) it’s publicly accessible information, (ii) ‘what they don’t know won’t hurt them’ and (iii) the assumption that everybody does it. 30 These do present ethical tensions; the information is publicly available but not everyone is aware of their privacy settings and may not fully understand or be aware of what they are sharing online.33,34
Consent, disclosure & documentation
Consent (the type of consent; written or verbal) and disclosure were common tensions reported in the literature with some arguing that it is required and others claiming it is not.2–4,7,19,26,28 The lack of regulatory guidance on PTG meant that it was unclear whether consent should be obtained from the patient and if not, whether the act of PTG should be disclosed to the patient. Also, the issue of whether the act and outcome of PTG should be documented in patient notes was considered by nine of the included articles but none came to a firm conclusion about best practice.
Nature of online information
The need to be mindful of the reliability, authenticity and [clinical] relevance of online information was noted by over half the articles either implicitly or explicitly. Particularly in Coffey et al 13 who examined how forensic clinicians used PTG as part of criminal and civil evaluations (e.g. child custody cases, competence evaluations, personal injury cases) to assess mental state, corroborate information, observe any posts relating the presenting legal issues and observe behaviours PTG because they deemed there to be more reliable sources of information that could be used in decision making (e.g. police, family doctors), they also noted that a person’s online presence does not always reflect the reality of the ‘offline’, physical space of a person
When is PTG acceptable, what actions should be taken and why?
PTG was deemed to be within regulatory requirements based on the need to adhere to a duty of care to a patient and where justification could be provided within the confines of a professional code of conduct (e.g. safety and safeguarding concerns, emergency situations). 2
Positive outcomes of PTG reported included improving care quality, understanding the patient, therapist sense of safety (safeguarding for both the therapist and the patient) and mediation of risk. Kolmes & Taube 27 noted that it has the potential to improve professional objectivity, therapeutic relationship and facilitates the treatment process. However, other research, particularly those where the professional group was not in psychology or counselling argued that PTG could pose a risk to professional objectivity and damage the professional-patient relationship. This is due to the potential for crossing professional boundaries (especially where simple curiosity was the motivating factor to engage in PTG).2,4,6,15,26 There were two articles where PTG had been used in clinical decision-making, presenting three case examples in total. Ince et al 16 presented a case where a psychotic patient requested that the clinical team review his social media posts which facilitated a quicker and accurate diagnosis of his condition. Baker et al 10 presented two cases where PTG was used to validate conflicting information being offered by a patient. The other was to contact a patient many years after a diagnosis to communicate critical information about their genetic status and where all other routes of communication had been exhausted.
When is PTG not acceptable and why?
Curiosity as a reason to use PTG was reported in the literature but also noted as a reason not to conduct PTG. It is viewed as crossing professional boundaries, a known breach of professional codes of conduct1,2,4,5,29,32 and often associated with a sense of guilt after the event. 30 A sense of guilt after the event could be because, on reflection, the individual could not justify the benefit to the patient or that the professional realised this could potentially be a breach of professional codes of practice (e.g. crossing professional boundaries). Curiosity as the sole reason to conduct PTG could also be viewed as an unreasonable violation of privacy, dignity and confidentiality, 1 or highlight concerns about the professionals’ wider ethical practice and motivations. However, it could be viewed as a genuine inquisitiveness and desire to improve care. 1
The need for research, guidance, education and training
17 of the 19 articles concluded that there is a need for guidance, policy and/or education and training on the topic of PTG. This suggests that professionals recognise a purpose for it in clinical practice but would like more clarity from regulators about when it is acceptable to be used. Although only eight articles concluded that there is a need for research with stakeholders such as patients and the public to establish their perspectives about when and why PTG would be viewed to be acceptable. This type of research could be of value for informing the development of guidance, education and training.
Discussion
Principal findings
This review has thematically analysed current research literature that discusses the ethical and regulatory implications of PTG. Most articles concluded that there is a need for professional guidance, education and training. In the absence of professional guidance, our review has identified common themes in research literature and drawn conclusions about situations when it may be acceptable, and what actions should be taken to ensure that it is ethical and within regulatory codes of conduct.
PTG is evidently a part of clinical practice in some fields, most commonly in the field of mental health and psychology. However, that is not sufficient to conclude that it does not occur in other fields such as nursing and allied health or social work and indeed, some of the excluded anecdotal articles were in these fields. 32
Findings suggest that there is a role for PTG in health and social care practice but only in specific circumstances for the benefit of patient care and outcomes and that certain actions should be taken if a professional engages in PTG. Conversely, there are certain circumstances when PTG is not acceptable or appropriate.
Recommendations
Our review is internationally relevant and original. Like the included research literature in this review, we know PTG is being used in a range of countries (reported prevalence from 16.7% 4 to 98% 2 ) and by a range of professional groups but there is ethical debate about when and why it should be used for the benefit of patient care. In comparison to other literature reviews on PTG,2,3 our review has uniquely included available research across health and social care (not solely counselling and psychiatry) and offers practical recommendations (rather than descriptions of prevalence, attitudes and behaviours) about when PTG is acceptable and, most importantly, why. The evidence base reported in the available body of research has never been synthesised and reported in this way before.
Recommendation 1: Consent, disclosure and documentation in PTG
Unlike other research literature, our review is the first to suggest a resolution to the ongoing ethical debate on the topic of consent, disclosure and documentation in PTG.
Firstly, our review has identified the ethical issue of consent in PTG and the wider need to explore the concept of consent when choosing to use PTG. We argue that there is not a need to obtain consent for PTG for the following reason. Cornock 9 notes that in emergency situations where a patient is alone and unable to consent or where they lack capacity, then professionals may act in the best interests of the patient.
A useful definition of consent from Department of Health and Welsh Office 33 ‘the voluntary and continuing permission of the patient to receive a particular treatment, based on an adequate knowledge of the purpose, nature, likely effects and risks of that treatment including the likelihood of its success and any alternatives to it’ p67. Therefore, consent to PTG does not always need to be obtained because it is not ‘treatment’; it is information and evidence gathering (knowledge) to potentially inform treatment, safeguard or mediate risk. However, there must be clear rationale and documentation of PTG of which curiosity is not suffice. 2
We argue that any action taken as part of clinical care and/or decision making should be documented as part of good clinical record keeping. 34 Therefore, our review concludes that in the absence of professional guidance, the act of PTG, rationale for it and outcome (i.e. what was found and used in informing treatment) should be documented in patient records.35,36
Disclosure of the act of PTG would be based on the circumstances and benefit/impact for the patient. For example, if used in forensic environments for the purposes of decision making about criminal or civil matters it may be necessary to share this evidence with the medical and legal teams involved. 13 Or it may be that the patient requests that PTG be used and therefore, it may be necessary to share the outcome with them or relevant people. 16
Recommendation 2: Is PTG acceptable, when and why?
Thornton & Moran 14 concluded that autonomy and beneficence should be considered as ethical principles when deciding about whether to use PTG. We recommend that, as with any clinical decision it should be made with consideration of autonomy, beneficence, non-maleficence and justice and within the remit of regulatory codes of practice.12,37 Our findings conclude that PTG is acceptable if there is a clear benefit to patient care in emergency situations, if the patient requests it, if there are safeguarding concerns or risk of harm (prevention of harm), to validate the authenticity of information or where all other routes of sourcing information have been exhausted.13,14 However, PTG should not be used as the routine and/or primary source of information/evidence for decision making due to the nature of online information and its currency, authenticity and accuracy.
Recommendation 3: The need for education, training and professional guidance
Many regulators do have guidance about the professional use of social media yet despite this, the need for training in the use of social media has also been widely reported in research literature, and there are parallels that can be drawn with PTG. 36
As our review was the first to include health and social care broadly it concludes that there is a need for training, education and guidance for professionals [relevant to their field of practice and legal and ethical norms in their geographic location/organisation]. This should include information about when PTG is acceptable and what actions should be taken to ensure professional codes of practice are maintained. This should include the recommendations we have outlined above but also to help reduce the risk that information sourced online does not distract from routine clinical decision making.
As professional guidance and training programmes evolve it is recommended that research literature, future research into the impact of PTG, particularly on vulnerable groups, but also all stakeholder perspectives of PTG including nursing and allied health professions and regulators.4,26,30,31
Strengths and limitations
This review is novel because it is the first to synthesise findings from research literature about what ‘is’ acceptable in PTG, when and why. It contributes to the ongoing international debate about whether PTG by professionals in health and social care globally is acceptable. It makes recommendations for professionals in the current absence of regulatory guidance, training and policy on the use of PTG.
The nature of professional regulation globally means that countries where formal regulation does not exist or those that are ‘least’ regulated will be underrepresented in published research literature. It did exclude conference proceedings due to the lack of detail provided, and that is required for the thematic analysis we employed.
There were only three studies that included an in-depth qualitative component. Also, the significant number of articles focused on mental health and psychology mean that conclusions should be considered with caution if seeking to draw comparisons for fields such as nursing, allied health and social work. Our findings also need to be taken in the context of regulator codes which vary by geographic location and profession, and this is reflected in our recommendations.
Our review did not consider practitioners who a not registered with a regulator (but work in health and social care with patients) and are accountable to their employing organisation as this was outside of the scope of this study. But no studies of this nature were found as part of our search strategy.
It was not possible to quantify the negative outcomes of PTG for patients, as those reported in the literature were reported as anecdotal/speculatory rather than explicit examples of when it has resulted in a negative outcome.
None of the included research reported on PTG outside of clinical practice and the motivations for this (e.g. chatting via social media after using PTG to deliberately contact a patient or past patient). Regulatory codes report 12 that this type of behaviour is unprofessional, it could also indicate malintent and wider concerns about fitness to practise relating to professional boundaries. 37
Conclusion
PTG is an emerging area for research and practice and with up to 98% of trainees and clinicians reporting the use of PTG the need for further research and guidance about when and how to employ PTG is evident. Future research needs to explore, in depth, perceptions from clinical practice, medico-legal fields, patients and regulatory bodies from all fields of health and social care. This would promote consensus and therefore inform the development of guidance and policy. It will be important to develop training and education interventions/activities for health and social care professionals. In the interim, the findings of this review may be useful to health and social care professionals who have and do use PTG in making decisions that are ethical and within regulatory principles. It recommends that further research with stakeholders should continue to inform organisations and regulators in developing education, training and professional guidance for PTG.
Supplemental Material
Supplemental Material - When and in what circumstances is patient-targeted googling acceptable for health and social care professionals? A narrative review and thematic analysis
Supplemental Material for When and in what circumstances is patient-targeted googling acceptable for health and social care professionals? A narrative review and thematic analysis by Gemma Ryan-Blackwell, Jessica Jackson and Sharif Haider in Health Informatics Journal
Supplemental Material
Supplemental Material - When and in what circumstances is patient-targeted googling acceptable for health and social care professionals? A narrative review and thematic analysis
Supplemental Material for When and in what circumstances is patient-targeted googling acceptable for health and social care professionals? A narrative review and thematic analysis by Gemma Ryan-Blackwell, Jessica Jackson and Sharif Haider in Health Informatics Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
This study is a narrative review of literature and did not require ethical review or approval. There were no human participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.