
Abstract
Introduction
The adoption of prescription drug monitoring programs (PDMPs) has been a central pillar in the United States’ (US) response to the evolving opioid epidemic. PDMPs are state-administered centralized electronic database that collect and report controlled substance prescriptions. 1 These data systems are used by a variety of stakeholders including clinicians, who can log into an online portal to review prescribing histories for their patients. Currently, every state in the US has an operational PDMP, although there is variability in their administration, features, access, and implementation. 2 For example, most states currently mandate that prescribers register for the PDMP and many states mandate use in certain circumstances (e.g., new opioid prescriptions). Although the opioid crisis has progressed largely beyond prescription drug use and diversion, PDMPs remain useful tools for clinicians to monitor potentially high-risk or uncoordinated controlled substance prescribing. Additionally, access to PDMP data may also assist clinicians in other types of decision making such as confirming treatment appropriateness, modifying therapies, adding other non-opioid treatments, or referring to substance use treatment or prescribing risk mitigation measures. 3
Reports on the effectiveness of PDMP and policies governing their use have been mixed. This likely reflects heterogeneity of programs, their evolution over time, and methodologic differences in study designs evaluating these programs.4–6 Earlier studies examining older PDMP technologies with limited enrollment and few legal mandates were likely negative because the programs were not frequently used. The literature evaluating modernized PDMPs has been more positive, particularly for programs with use mandate, which legally require providers check the PDMP in specific prescribing circumstances. Studies of states with PDMPs with use mandates have shown reductions in schedule II opioid prescriptions, high dose prescriptions, concurrent benzodiazepine and opioid prescriptions, and prescriptions from multiple providers.7–11 Although the effect of PDMP implementation on opioid-related health outcomes is less certain, several studies have noted positive impacts on overdose, hospitalizations, and death.12–15
A common barrier cited by clinicians to using PDMP data in practice involves the time and effort required to register, log in to website portals, and navigate and interpret PDMP reports.16–18 A promising approach to enhance PDMP use and effectiveness is integration within the electronic health record (EHR) or other health information technology platforms. As such, state and federal health authorities have made integration of PDMPs a focus of infrastructure funding. Studies from several of these early integrations have shown that EHR integration can significantly improve how often clinicians query the PDMP.19,20
In 2019, Oregon Health & Science University (OHSU), the state’s only academic medical center, underwent PDMP integration within its EHR platform in primary care clinics over a 6-month period. Oregon’s PDMP has been operational since 2011, with a mandate for provider registration enacted in 2018. However, there are currently no PDMP use mandates in Oregon. The objective of this study was to evaluate the effect of this integration on clinician use of PDMP overall and across several clinician subgroups.
Methods
Study setting
The study was conducted in all twelve ambulatory primary care clinics affiliated with the OHSU academic medical center located in the Portland, Oregon metropolitan region. OHSU, the state’s only academic medical center, operates a hospital and multitude of ambulatory care clinics all using a common EHR platform (Epic™; Epic Systems Corporation). The main PDMP vendor in the US (Bamboo Health; previously Appriss Health) provides a single-point access product (PMP Gateway) of PDMP information within healthcare systems EHR workflows in 43 states, including Oregon. 21 The connection between OHSU’s EHR and PDMP is through Bamboo Health’s PMP Gateway which allows one-click PDMP accessibility, without the requirement to enter additional credentials after initial EHR login. No additional alerts, notifications, or decision support tools were incorporated as part of the integration. Study clinics were located on OHSU’s main Portland campus (n = 3), other locations in Portland (n = 2), Portland suburbs (n = 5), and in the Columbia River Gorge region 60 miles east of Portland (n = 2). Providers assigned to each clinic typically see patients at their designated clinic and only rarely serve patients in other clinics.
Study design
We use a stepped-wedge observational design to evaluate the effect of the PDMP EHR integration on PDMP query requests. The study period was May 2018 through September 2020. Integration within study clinics occurred in three waves on May 13, 2019, July 15, 2019, and September 16, 2019, with 4 clinics implementing the integration in each wave. Thus, each wave had at least 12 months of time before and after their clinic’s integration. Although the informatics department did not randomize clinics to implementation wave for administrative reasons, clinics were grouped to achieve relative balance across certain characteristics (provider types, region).
Data sources
The primary outcome was monthly PDMP queries by clinicians (including physicians, nurse practitioners [NPs], physician assistants [PA]) practicing within study clinics. PDMP query data were obtained from Oregon’s PDMP program which is administered by the Injury and Violence Prevention Program of the Oregon Health Authority. While PDMP query data are grouped by their source, either the traditional web portal or through the PMP Gateway, the state provided query data combined into one common dataset, without the ability to disaggregate. To identify affected clinicians, we extracted clinic provider data from OHSU’s EHR including DEA number (linking variable), clinic location (urban vs suburban or rural), provider type (i.e. MD/DO, NP, PA), age, and sex. State regulations place limits on the release of PDMP data to prevent individual identification. To meet these requirements, we collapsed NPs and PA into one category, and removed age from the analysis dataset. We also collapsed two pairs of smaller clinics into two larger single clinic clusters. One pair was in wave 2 and the other in wave 3. After linkage, DEA number was removed from the analysis dataset by state PDMP analysts to maintain privacy protections.
Statistical analysis
We used negative binomial general estimating equations (GEE) models to estimate changes in PMDP query counts from before to after integration. The primary covariate of interest was a time-varying indicator coded zero in the months prior to integration onset and one in the month of integration onset and all subsequent months. Our GEE model accounted for clustering at the clinic-level and adjusted for integration wave, calendar time, provider type (MD/DO vs NP/PA), sex, clinic urbanicity (urban vs non-urban) and pre-integration PDMP query rates, opioid prescribing volume, and clinic volume. Pre-integration provider query rates, opioid prescribing volume, and clinic volume were binned into quartiles for the analysis. To evaluate heterogeneity of treatment effect, we performed tests of interactions for these provider and clinic-level subgroups. We also tested models incorporating an interaction between time and the time-varying indicator of integration onset (time*integration) to examine trend changes in PDMP query counts from before integration to after integration.
Data analyses were performed using SAS Studio, version 3.6 Enterprise Edition (SAS institute). Analyses were conducted using PROC GENMOD and marginal means were requested for all categorical variables. Estimates for marginal means and incidence rate ratios were exponentiated to obtain values on the scale of the outcome variable. Statistical analyses were 2-tailed and p-values <0.05 were statistically significant.
Results
Clinic provider characteristics.
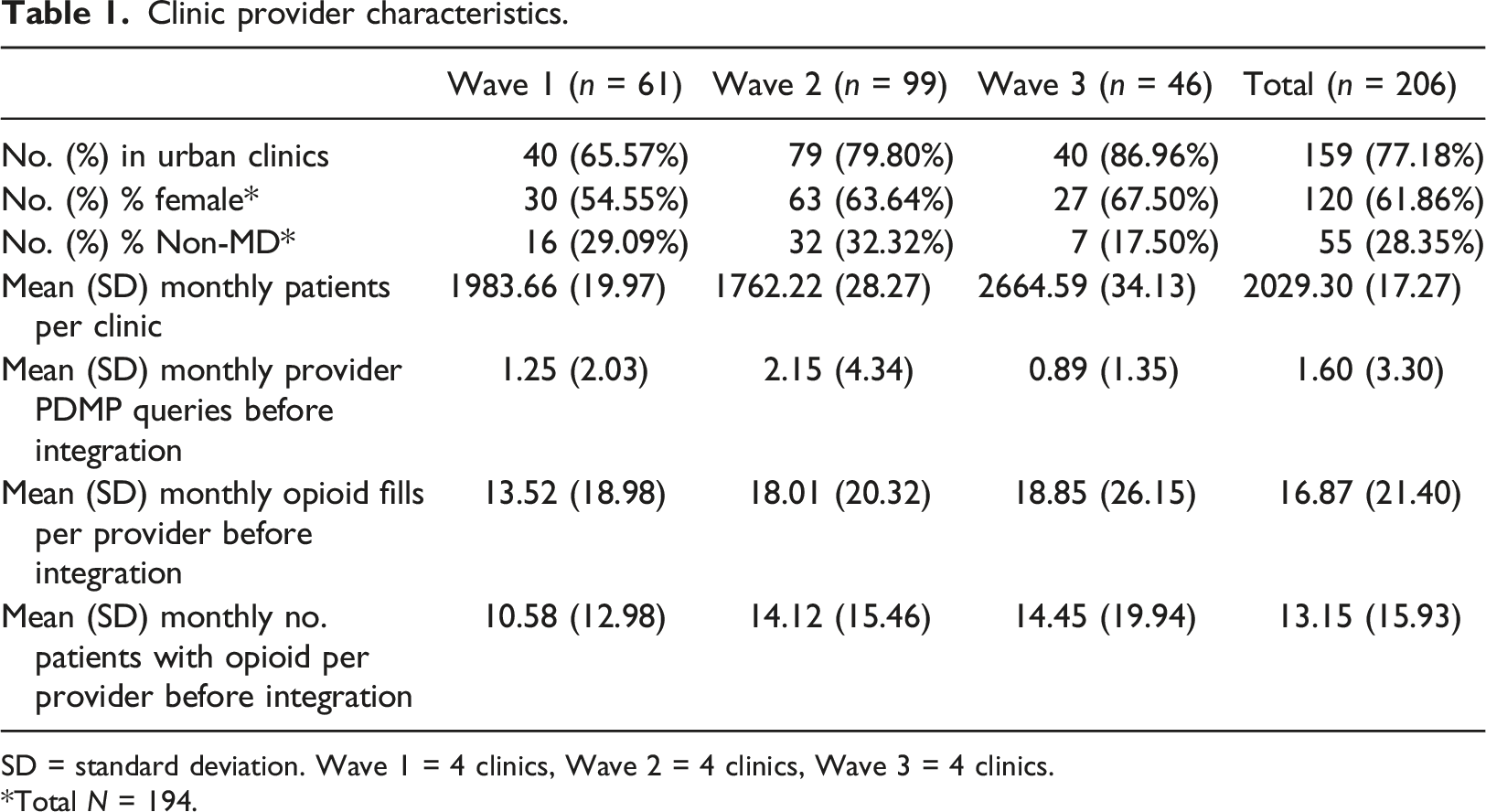
SD = standard deviation. Wave 1 = 4 clinics, Wave 2 = 4 clinics, Wave 3 = 4 clinics.
Total N = 194.
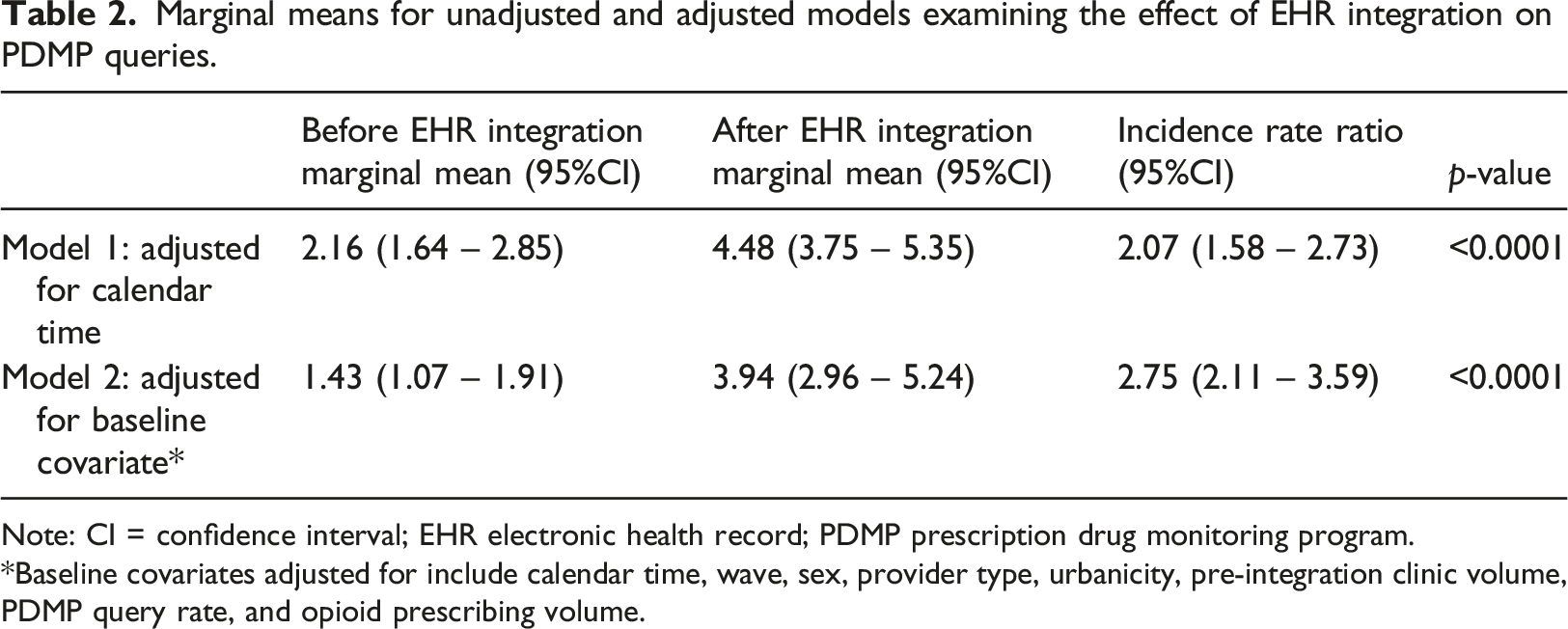
Figure 1 shows the average number of PDMP queries per provider per month before and after integration where implementation date was centered for each wave. PDMP Queries by wave are shown in Supplemental Figure s1. Table 2 summarizes GEE model marginal mean estimates. In the covariate adjusted model, the model-estimated mean number of queries per provider per month increased significantly after PDMP integration from 1.43 (95% CI 1.07 to 1.91) to 3.94 (95% CI 2.96 to 5.24); a 2.75-fold increase (95% CI 2.11 to 3.59; p < .0001). Model coefficients for unadjusted and covariate adjusted models are presented in Supplemental Table e1. Mean PDMP queries per provider per month. Note: EHR electronic health record; PDMP prescription drug monitoring program. Marginal means for unadjusted and adjusted models examining the effect of EHR integration on PDMP queries. Note: CI = confidence interval; EHR electronic health record; PDMP prescription drug monitoring program. Baseline covariates adjusted for include calendar time, wave, sex, provider type, urbanicity, pre-integration clinic volume, PDMP query rate, and opioid prescribing volume.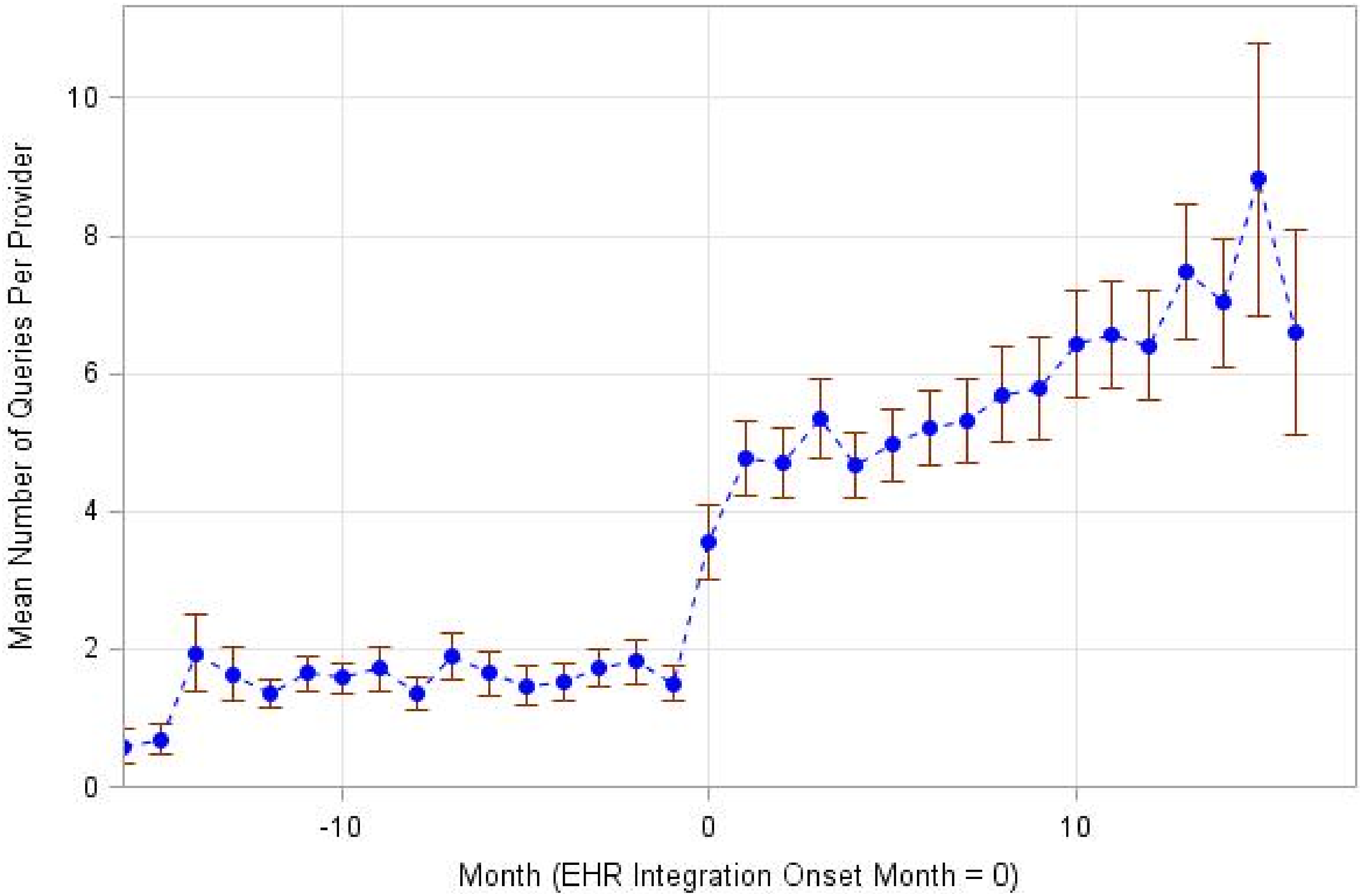
Aside from the integration variable, the only other covariates that were significant were pre-integration PDMP query volume and provider type. Providers in the highest quartile of PDMP use before integration queried the PDMP 6.05 (95% CI 3.74 to 9.78; p < .0001) times more than those in the lowest quartile. NPs and PA providers queried the PDMP 1.42 (95% CI 1.04 to 1.92; p = .03) times more than physician providers. The time*integration effect was not statistically significant, indicating no significant change in the trend in PDMP use after integration.
The only significant subgroup effect was across pre-integration PDMP use (interaction p-value <0.0001). As shown in Figure 2, providers in the lowest quartile of pre-integration PDMP use (Baseline (BL) Category 1) increased from 0.07 (95% CI 0.03 to 0.20) to 2.55 (95% CI 1.45 to 4.50) queries per month, a 36.78 fold (95% CI 16.91 to 79.95; p < .0001) increase. Providers in BL category 2 and 3 increased their PDMP use by 4.01 fold (95% CI 2.59 to 6.21; p < .0001) and 2.13 fold (95% CI 1.55 to 2.94; p < .0001), respectively. Providers in the highest quartile of baseline PDMP use (BL Category 4), who averaged 8.72 (95% CI 5.76 to 13.21) queries per month before integration, did not see a significant increase in queries after EHR integration. Coefficients for the full interaction model are presented in Supplemental Table s2. Model marginal means for monthly queries before and after EHR integration, by PDMP query rate quartile at baseline. Note: BL baseline; EHR electronic health record; PDMP prescription drug monitoring program.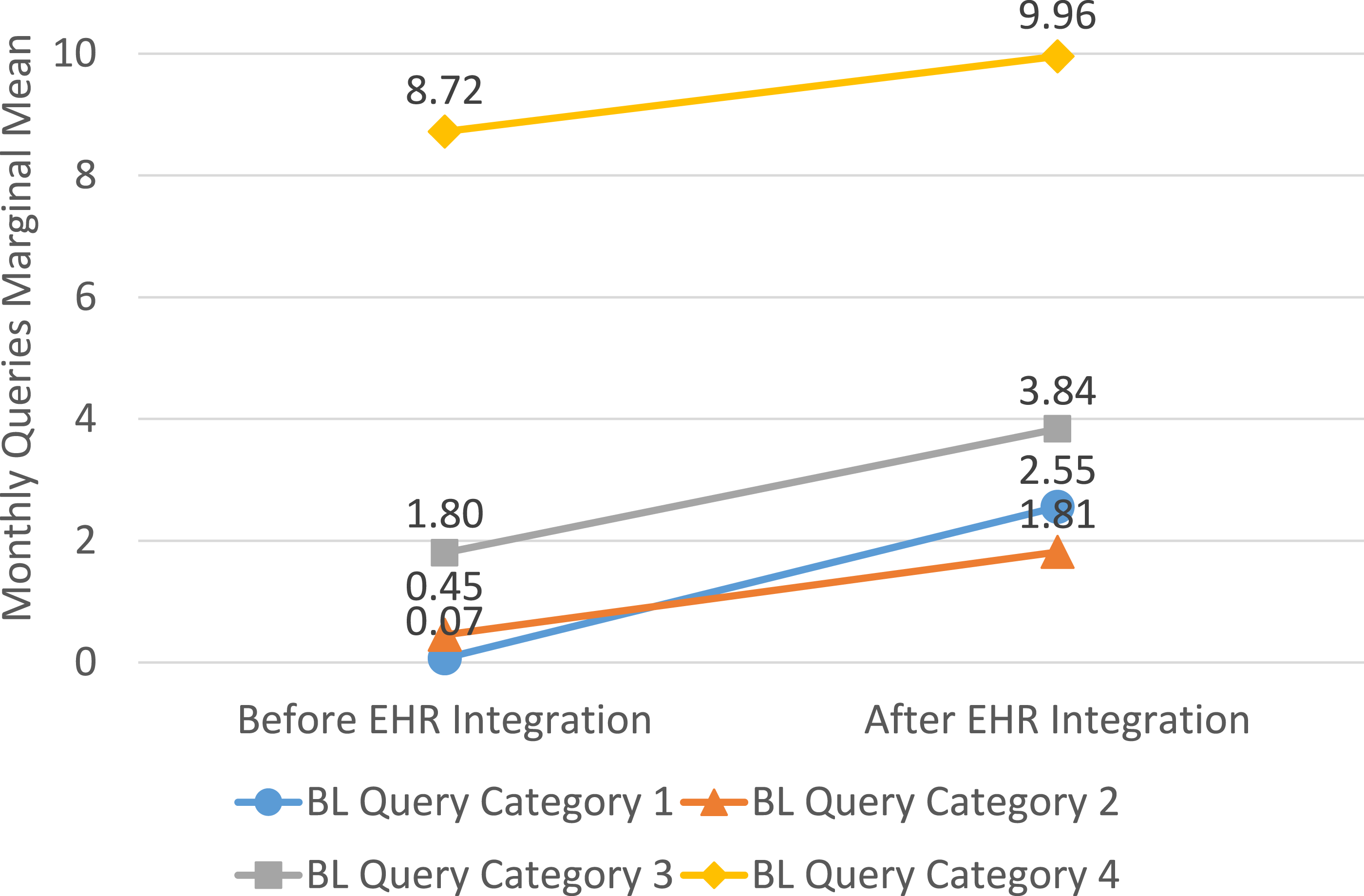
Discussion
In this study of primary care providers at one academic medical center, we found that integration of the PDMP in the EHR was associated with nearly a 3-fold increase in the number of PDMP queries requested. While the increase occurred rapidly following integration in all three waves, there was no change in the overall trend following integration. Non-physician providers (NPs/PAs) used the PDMP to a greater extent than physician providers. Providers who used the PDMP the least before integration saw the largest increase in queries after integration.
Improving the accessibility and functionality of state PDMP data is an important step in the evolution of PDMP utility. Although OHSU’s integration was among the first healthcare systems to integrate in the state, PDMP integrations have now been completed in more than 1200 facilities across Oregon. Results from this study are consistent with another state report, which indicates that almost three-quarters of prescribers in Oregon accessed the PDMP through the EHR with every controlled substance prescription they issued. 22 A large majority of prescribers in Oregon indicate that access to an EHR integrated PDMP enhanced their ability to provide efficient care and reduced unnecessary prescribing; most indicated improved communication and patient outcomes.
Our findings are also consistent with the growing number of studies that have assessed the effect of EHR integration on PDMP use. In national survey of office-based physicians, those who accessed the PDMP through the EHR were more likely to use it and indicate its use was very easy relative to those who accessed the PDMP through an outside system. 23 Another relatively small survey of providers (physicians, pharmacists) working in one academic medical center in Iowa, found that 58% of respondents indicated that PDMP integration increased the likelihood of reviewing PDMP profiles and 75% indicated that integration reduced the time required to evaluate the PDMP patient history. 24
Quantitative research evaluating PDMP integration efforts in the primary care setting has also been consistent. A study evaluating the integration of PDMP in the largest health system in Massachusetts (Mass General Brigham) in 2018 found that absolute number of PDMP queries increased 43% in the 6 months following integration. 19 Among primary care providers, the largest increases were seen for clinical nurse specialists (71%) and PAs (104%) compared to family medicine (30%) and internal medicine (39%) physicians. Although changes in PDMP use did not differ significantly by provider type in our study, non-physician providers (NPs/PAs) were significantly more likely than physicians to query the PDMP overall. A cluster randomized trial which evaluated PDMP integration in primary care clinics affiliated with an academic health system in Minnesota found a 60% increase in PDMP queries, with similar effects among physicians and NPs or PAs. 20 Higher PDMP use among NPs and PAs has been reported in other state-specific surveys of use. 25 Another study evaluating EHR-PDMP integration within the emergency department failed to increase PDMP use, suggesting integration alone however may not be sufficient for certain provider groups or settings. 26
The smaller relative increase in Massachusetts and Minnesota relative to Oregon could possibly be explained by the lack of a PDMP query mandate in Oregon. Oregon likely lags other states in provider PDMP use because it was among the last states to mandate registration (2018) and remains one of the few to have no state-wide use mandate. Massachusetts had a pre-existing PDMP query mandate for every schedule II or III opioid prescription which may explain the more modest overall increase in queries relative to Oregon where PDMP use remained optional. In Minnesota, a use mandate was implemented shortly after integration. However, despite the lack of a use mandate, pre-integration PDMP use was 4-5 times higher than Oregon, which may indicate differing practice norms across these states.
Limitations
Our study has limitations. First, data reported only reflect PDMP use among primary care providers in one academic medical center in one state using one specific vendor developed integration package (Bamboo Health PMP Gateway). While similar positive effects have been reported in health systems in other states, effect sizes varied, and it is unclear how these state and regional factors affected use. In particular, our findings may have limited application to lower resourced healthcare settings (e.g. community health centers, critical access hospitals), which already lag in their informatics capabilities. Future research should assess how these factors associated with EHR integrated PDMP use affect practice adoption. Although the intervention was evaluated using staggered, step-wedge design, clinic clusters were not randomly assigned and therefore changes in use may have been affected selection biases. Clinics were clustered and integration sequence assigned to provide relative balance across known characteristics, but unknown factors may have affected our findings. We only report the effect of integration on PDMP use. It is unclear how integration and increased PDMP use impacted controlled substance prescribing and clinical outcomes. Ecologic studies that have evaluated state-level variation in PDMP legal use mandates suggest that increased use is associated with reduced opioid prescribing and improved health outcomes.10,14 Additionally, our study did not measure the effect of integration on provider time savings, which has been shown to be a major deterrent of adoption.16–18 Further work to link PDMP dispensing data will enhance our understanding of the full impact of integration on controlled substance prescribing, utilization, and provide workflow.
Conclusions
Consistent with other recent studies, we find that integration of the PDMP in the EHR was associated with a significant increase in use in primary care clinicians in one academic medical center. The largest increases in queries were among those with the most infrequent PDMP use before integration. Throughout the study, NPs and PAs queried the PDMP more than physician providers. Despite the promise PDMP integration holds for increased use and improved outcomes, less than a quarter of office-based physicians and 10%-15% of hospitals report PDMP integration within their EHR.23,27 While nearly all states have enacted laws that permit PDMP integration into EHR and other health informatic platforms, barriers to integration including cost, EHR system interoperability, and information security remain.2,28 Further investment in EHR integration may be required to optimize PDMP use nationally.
Supplemental Material
Supplemental Material - Effect of integration of prescription drug monitoring program data in the electronic health record on queries by primary care providers
Supplemental Material for Effect of integration of prescription drug monitoring program data in the electronic health record on queries by primary care providers by Daniel M Hartung, Steven Z Kassakian and Michelle A Hendricks in Health Informatics Journal.
Footnotes
Author contributions
a. Concept and design: DH; SK; MH, b. Acquisition, analysis, or interpretation of data: DH; SK; MH, c. Drafting of the manuscript: DH, d. Critical revision of the manuscript for important intellectual content: DH; SK; MH, e. Statistical analysis: MH, f. Administrative, technical, or material support: DH, g. Supervision: DH.
Author’s note
Presented at AcademyHealth Annual Research Meeting June 27, 2023.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agency for Healthcare Research and Quality 5R21HS028119
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.