
Abstract
The use of mobile personal health records (m-PHR) has been little studied at the organizational level. This study was to investigate the relationships of various hospital-related factors with m-PHR use in Korean hospitals. Downloads of m-PHR applications for 101 hospitals were examined from May 26 to 30 June 2022. The dependent variable was the number of m-PHR downloads, and the major independent variables included six technological, organizational, and environmental factors. As technological factors, the number of computed tomography and magnetic resonance imagery devices were significantly associated with downloads (RR = 1.119, CI = 1.022–1.226, p = 0.016; and RR = 1.155; 95% CI = 1.024–1.302, p = 0.019, respectively). At the organizational level, the number of physicians, adjusting for the number of beds, and the number of medical information management staff showed significant associations (RR = 1.059, CI = 1.019–1.100, p = 0.004; and RR = 1.026, CI = 1.002–1.050, p = 0.033, respectively). From an environmental standpoint, downloads were positively associated with the proportion of the local population of working age (20–59 years) (RR = 1.102, CI 1.022–1.189, p = 0.012). Healthcare policymakers should pay close attention to these factors to advocate for the widespread use of m-PHR applications.
Keywords
Introduction
A mobile personal health record (m-PHR) is an Internet application that allows patients to access and manage their health data from smart mobile devices while securely and confidentially communicating with authorized medical providers.1–3 By adopting m-PHR systems, healthcare institutions (e.g., hospitals and clinics) improve patient consultations and provide various convenient services.4,5 To install an m-PHR, patients must download an application from their service provider’s digital marketplace.
The number of application downloads varies substantially among healthcare institutions. According to the Google Play Store, 6 between 10,000 and 100,000 instances had been downloaded per Korean hospital as of 20 May 2022. It is assumed that each download corresponds to a valid patient enrollment and registration. According to an empirical study, the number of downloads exceeded 160,000 at one Korean university hospital. 7
Notwithstanding the rapid rate of adoption and the evident importance of m-PHR applications,8–10 few studies have examined the factors associated with their use at the organizational and provider levels. Although several pioneering studies have investigated the use of mPHR and patient portals,11–13 those studies dealt with use at the individual user’s and patient’s levels. This research gap is probably due to the lack of sufficient data and feasible study settings. However, this could be easily remedied in Korea, where many hospitals are implementing m-PHR systems while collecting relevant data. 14
Therefore, the research question of this study was, “why does the number of m-PHR downloads vary across hospitals?” We suspected that the answer may be related to the amount of hospital resources (e.g., staff and equipment), as hospitals with more resources would presumably have increased information processing capability, which is necessary for m-PHR application support. 10 In turn, the population of patients would be correspondingly large. It was also surmised that the number of downloads may be related to environmental factors (e.g., local demographics and working conditions).
Notably, a 2021 study targeting Korean hospitals with more than 100 beds found that m-PHR adoption was correlated with nurse staffing and the number of computed tomography (CT) devices. 15 A similar study that examined the adoption of general mobile health (m-health) capabilities found that it was closely associated with the number of hospital beds. 16 Hence, we expected that the same processes may be in play in terms of m-PHR application downloads.
Several studies have presented the possibility that m-PHR downloads are associated with community demographics (i.e., m-health applications are used more by young working individuals).17,18 Hence, we expect that the absolute population size and its working conditions may also be relevant factors.
Based on those empirical studies, this study offers the following hypotheses: the number of m-PHR application downloads is positively correlated with the number of CT devices (HI), the number of magnetic resonance imaging (MRI) devices (H2), the number of medical staff (H3), the number of medical information managers (H4), the absolute population size of the local community (H5), and the proportion of local community residents who are of working age (H6).
Studies on the use or downloads of m-PHR applications at the organizational or provider level are important from several perspectives. First, studies at the provider level with empirical quantitative data are very scarce, although there are many studies at the individual patient level. This leads to the following questions: Assuming that many hospitals are providing m-PHR applications, why are there variations in their downloads? What accounts for differences among hospitals? There are few studies on this issue. However, we should first obtain relevant measurements in order to make improvements. 19 Second, if we can identify barriers to mPHR application downloads at the organizational level, we could make some suggestions on policy changes to promote downloads. For example, if downloads of m-PHR applications are concentrated in specific age group, policy suggestions could be made to enhance use by other groups.
Therefore, the research question of this study was, “what are the main factors associated with the download and use of m-PHR in Korean hospitals?” and the purpose of this study was to test hypotheses and possible correlations with hospital-related and environmental characteristics regarding mPHR download and use by hospitals. Identifying these factors would make it possible to accelerate application download and use by patients by modifying those factors.
Methods
Study setting
This study was conducted in Korea, where the National Health Insurance System fixes the prices of medical care based on unit costs, depending on the service type. Thus, many healthcare providers compete for patients. Notably, in Korea’s healthcare delivery system, patients are free to choose any small hospital or clinic they prefer, whereas tertiary hospitals require referrals.20,21 There were approximately 320 general hospitals and 45 tertiary hospitals as of 31 December 2021. This study excluded small hospitals and clinics (medical and dental) due to their very low m-PHR adoption rate. However, tertiary hospitals were included as they generally offer services for 20 or more medical specialties and are associated with medical schools. In Korea, general hospitals are defined as having between 100 and 300 beds, provided they have seven or more specialties; hence, they were also included. Hospitals with nine or more specialties typically have at least 300 beds. 15 A decision letter from the Institutional Review Board informed us that it was not necessary to obtain informed consent from the study subjects due to use of publicly available secondary health insurance administrative dataset.
Study design and data sources
This study adopted a cross-sectional study design in which all variables were observed at a single point in time (i.e., December 2021). However, some environmental factors were calculated based on a 5 years average from 2016 to 2021. We collected m-PHR application adoption data from May 26 to 30 June 2022. Data collection was based on a previous research study on m-PHR. 15 The values were confirmed both by contacting the hospitals again and using Google Play Store.
To logically analyze the hypotheses identified in the introduction, we categorized our variables of interest using criteria from previous studies22,23 that investigated the possible reasons for organizational technology adoption based on the technology–organization–environment (TOE) framework. Following the TOE model, this study identified six variables, as described in the next section.
In organizational theory, technological constructs have been defined as the means, activities, and knowledge for transforming inputs into outputs in firms. 24 Medical equipment, such as CT and MRI devices, represents technology in hospitals because they are extensively used to provide healthcare to patients. For these reasons, this study selected these two items as indicators of the technological context. Organizational constructs refer to the internal features of firms, such as the managerial structure, organizational size, and number of employees. 25 The number of employees in certain specialty areas of human resources in hospitals could be clearly considered as an organizational construct. This study selected the number of physicians and health information management staff as indicators of the organizational context because these personnel play important roles in hospitals and m-PHR adoption should be indirectly supported by these two professional groups. Environmental constructs include anything external to firms, such as governmental entities, policies, customers, and market competition. 26 From the customer perspective, the population of the local area and the proportion of the working-age population could be considered as environmental constructs. This study selected these two variables because potential m-PHR users would be drawn from the local residential population.
This study obtained key data items from the Healthcare Big Data Hub (https://opendata.hira.or.kr) maintained by the Korean Health Insurance Review and Assessment Service. Environmental factors (e.g., total population and working-age population) were acquired from the Korean Statistical Information Service (https://kosis.kr/index/index.do) based on population census data from 2016 to 2021.
Dependent and independent variables
The single dependent variable of this study reflected the number of m-PHR application downloads per hospital as provided by the Google Play Store. The six independent variables comprised the number of CT and MRI devices (technological factors), the number of physicians per 100 beds and medical information managers (organizational factors), and the total and working-age populations of the area (environmental factors). Only health information management (HIM) personnel holding medical recorder licenses were counted as health information managers. The proportion of the working-age population was calculated by dividing the number of people between 20 and 59 years of age by the total population in the local area and multiplying by 100. This study did not adjust any variables based on the hospital’s number of beds, apart from the number of physicians, as those results may have been distorted if the absolute population size had been used. We added several control variables based on best practices gleaned from prior efforts, including location, foundation date, and years of operation.10,15,27–29
Statistical analysis
This study first examined the descriptive statistics of the study subjects without using comparative study groups; thus, mean values with standard deviations, minima, and maxima are presented for numeric independent variables, and categorical independent variables are presented as proportions. This study checked for correlations among independent variables before adding them to the model to prevent multicollinearity issues. The number of beds was found to be significantly correlated with staffing levels and the numbers of CT and MRI devices. Thus, we excluded this variable from the final model. We also applied the modified Park test to diagnose the family of distribution and to choose the correct residual value for the generalized linear models,30,31 leading to our use of the gamma distribution. Thus, the generalized linear models were constructed with link = log and distribution = gamma using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Results
General characteristics of the study hospitals
General characteristics of the study subjects.
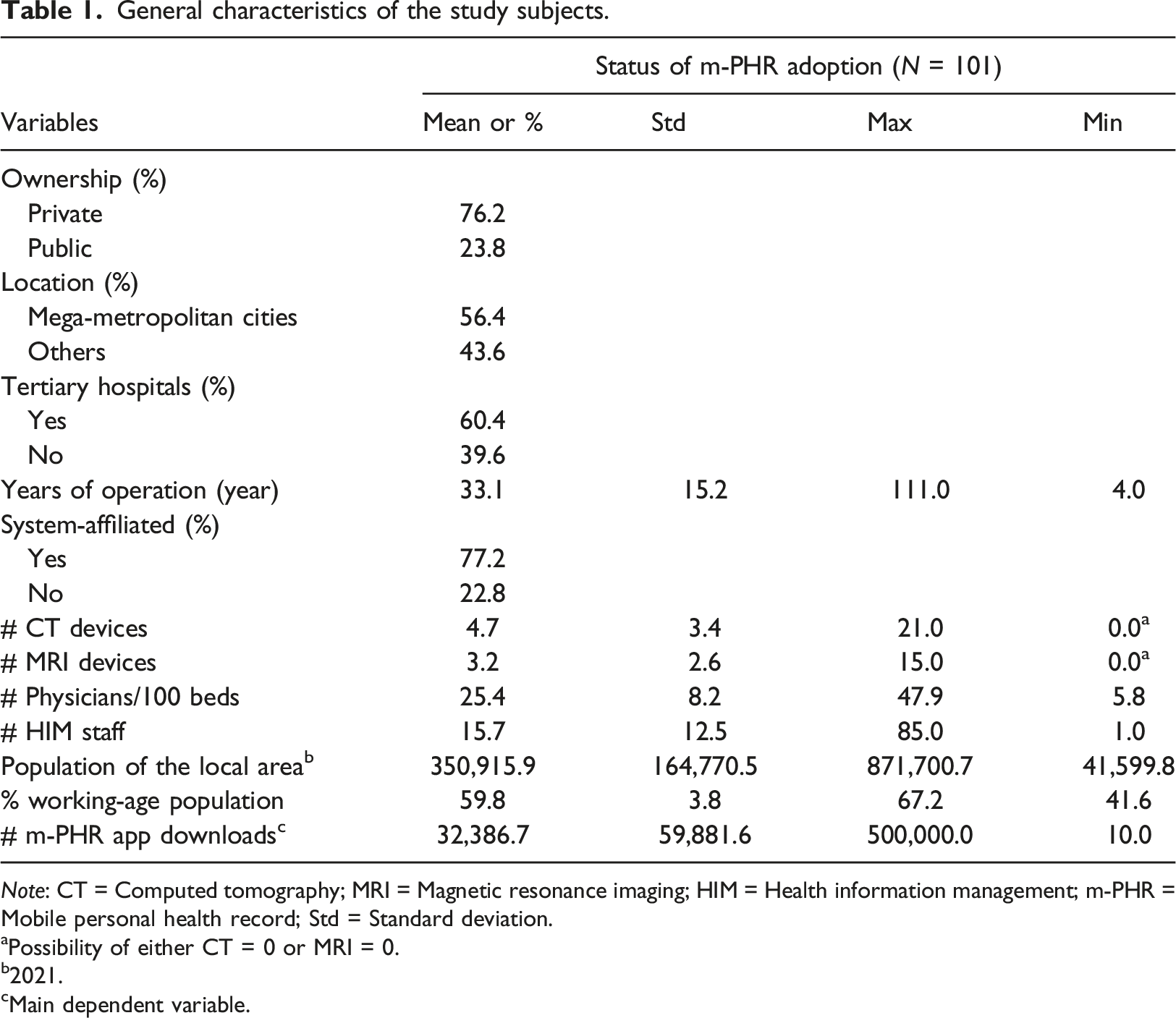
Note: CT = Computed tomography; MRI = Magnetic resonance imaging; HIM = Health information management; m-PHR = Mobile personal health record; Std = Standard deviation.
aPossibility of either CT = 0 or MRI = 0.
b2021.
cMain dependent variable.
Technological factors associated with the download of mobile personal health records applications
Associations of the number of CT and MRI devices with m-PHR application downloads.
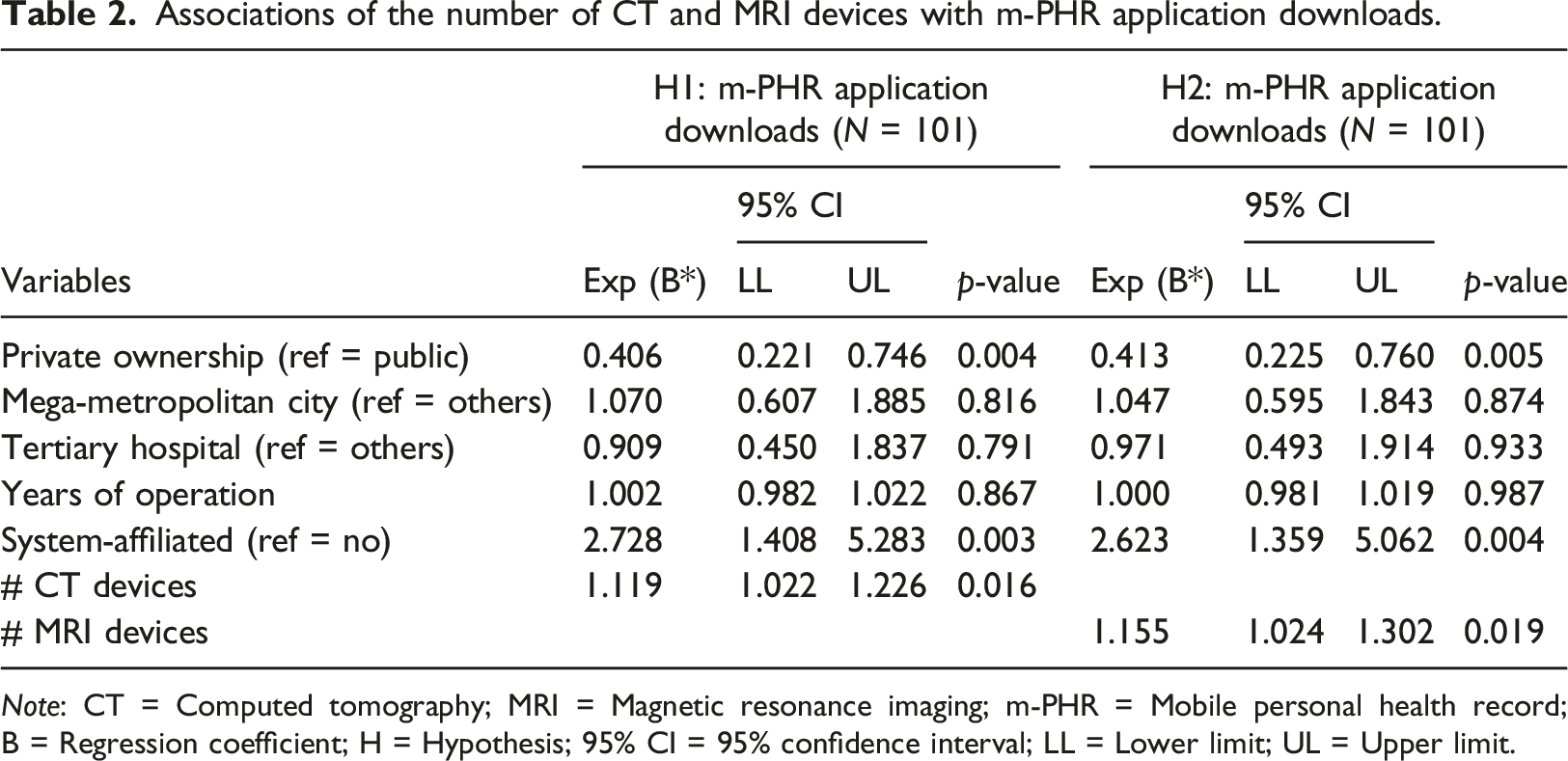
Note: CT = Computed tomography; MRI = Magnetic resonance imaging; m-PHR = Mobile personal health record; B = Regression coefficient; H = Hypothesis; 95% CI = 95% confidence interval; LL = Lower limit; UL = Upper limit.
Organizational factors associated with the downloads of mobile personal health records applications
Associations of the number of physicians and health information management staff with m-PHR application downloads.
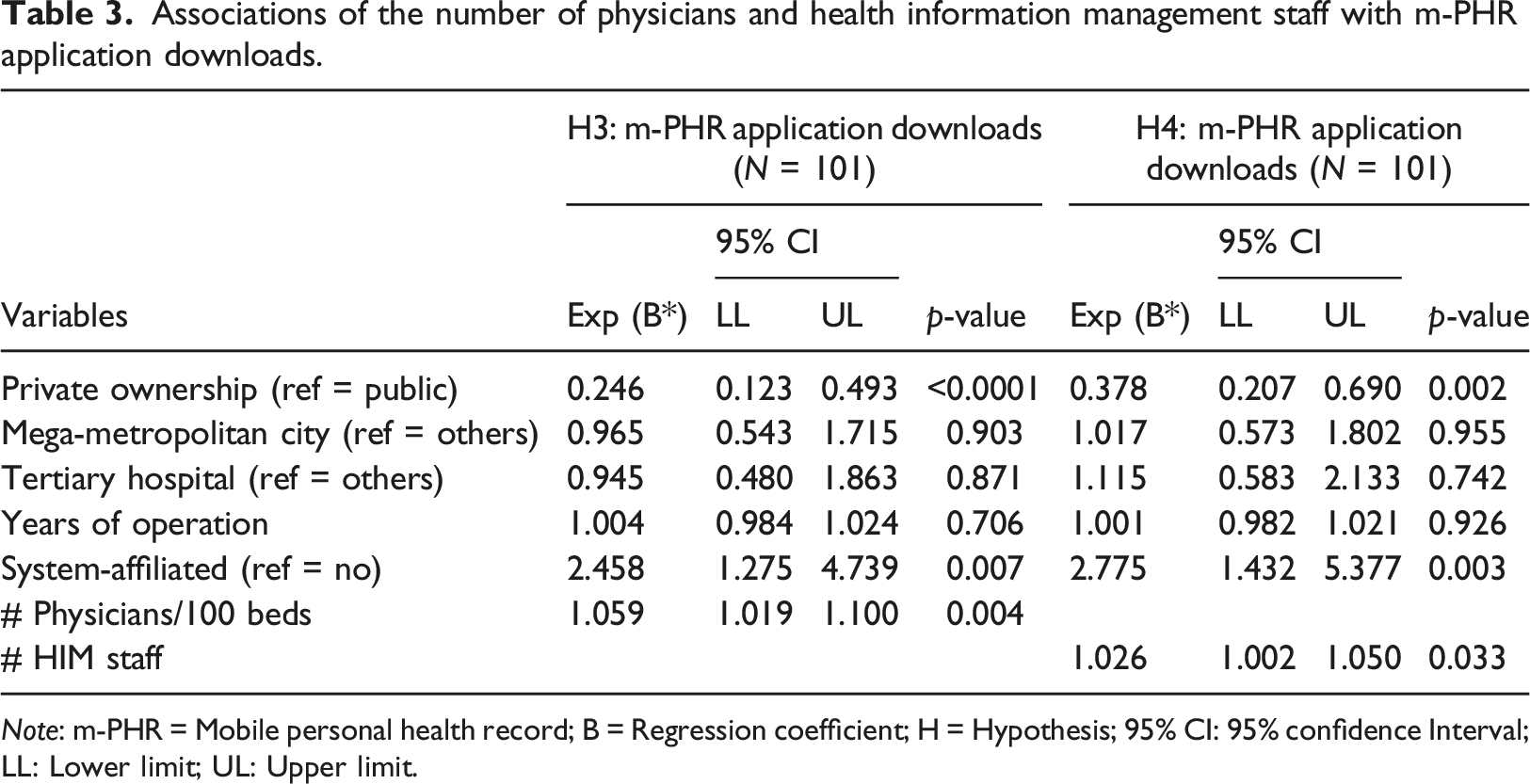
Note: m-PHR = Mobile personal health record; B = Regression coefficient; H = Hypothesis; 95% CI: 95% confidence Interval; LL: Lower limit; UL: Upper limit.
Environmental factors associated with the downloads of mobile personal health records applications
Residential population features and the number of m-PHR application downloads.
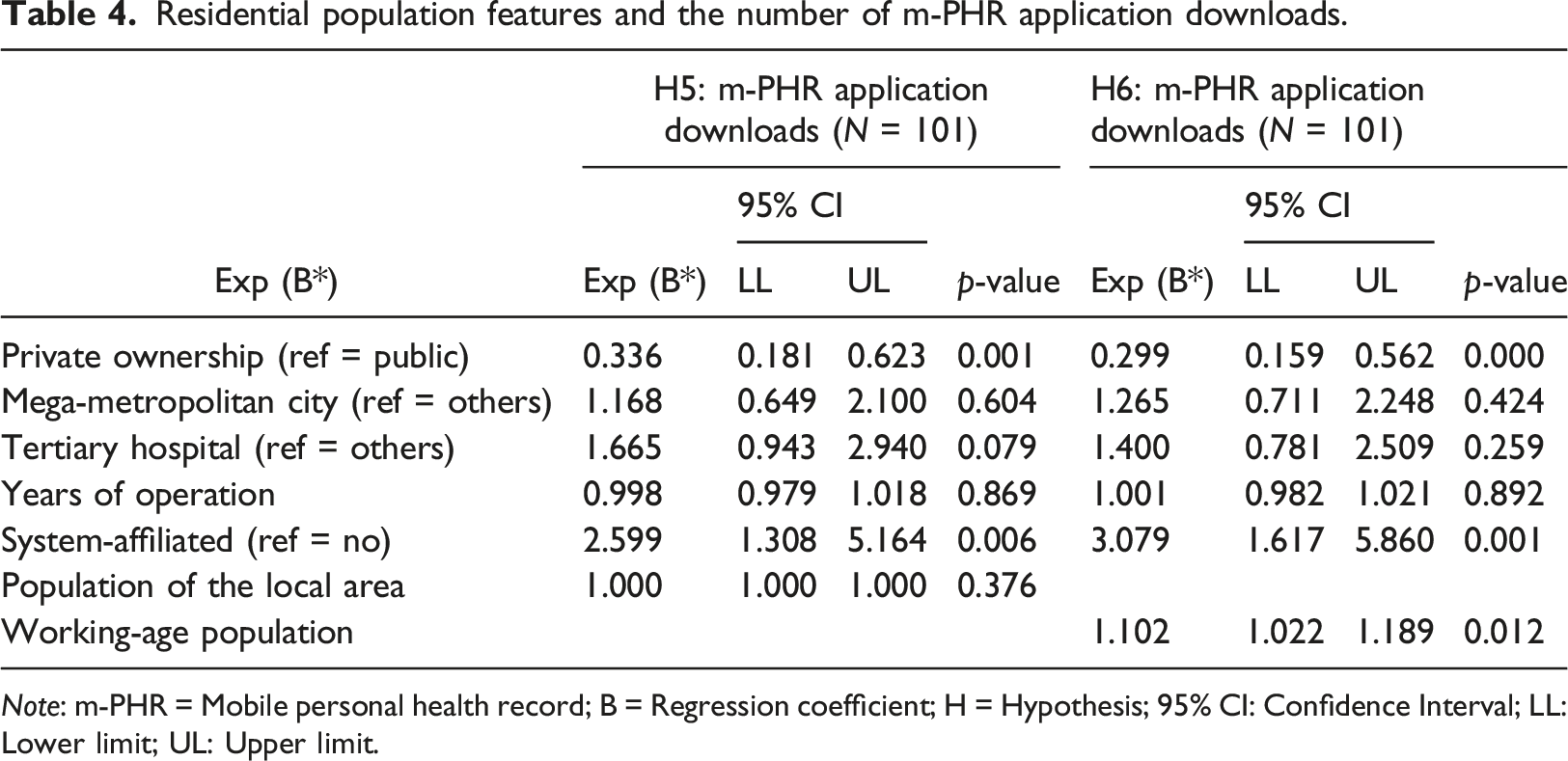
Note: m-PHR = Mobile personal health record; B = Regression coefficient; H = Hypothesis; 95% CI: Confidence Interval; LL: Lower limit; UL: Upper limit.
Figure 1 presents summary results on the relationships between the number of m-PHR application downloads and all targeted main independent variables after controlling for institutional covariates. For a one-unit increase in the independent variables, the percent increase was highest for the number of MRI devices, followed by the number of CT devices. Relationship between the download volume of m-PHR applications and six targeted independent variables/*: statistical significance at p-value = 0.05.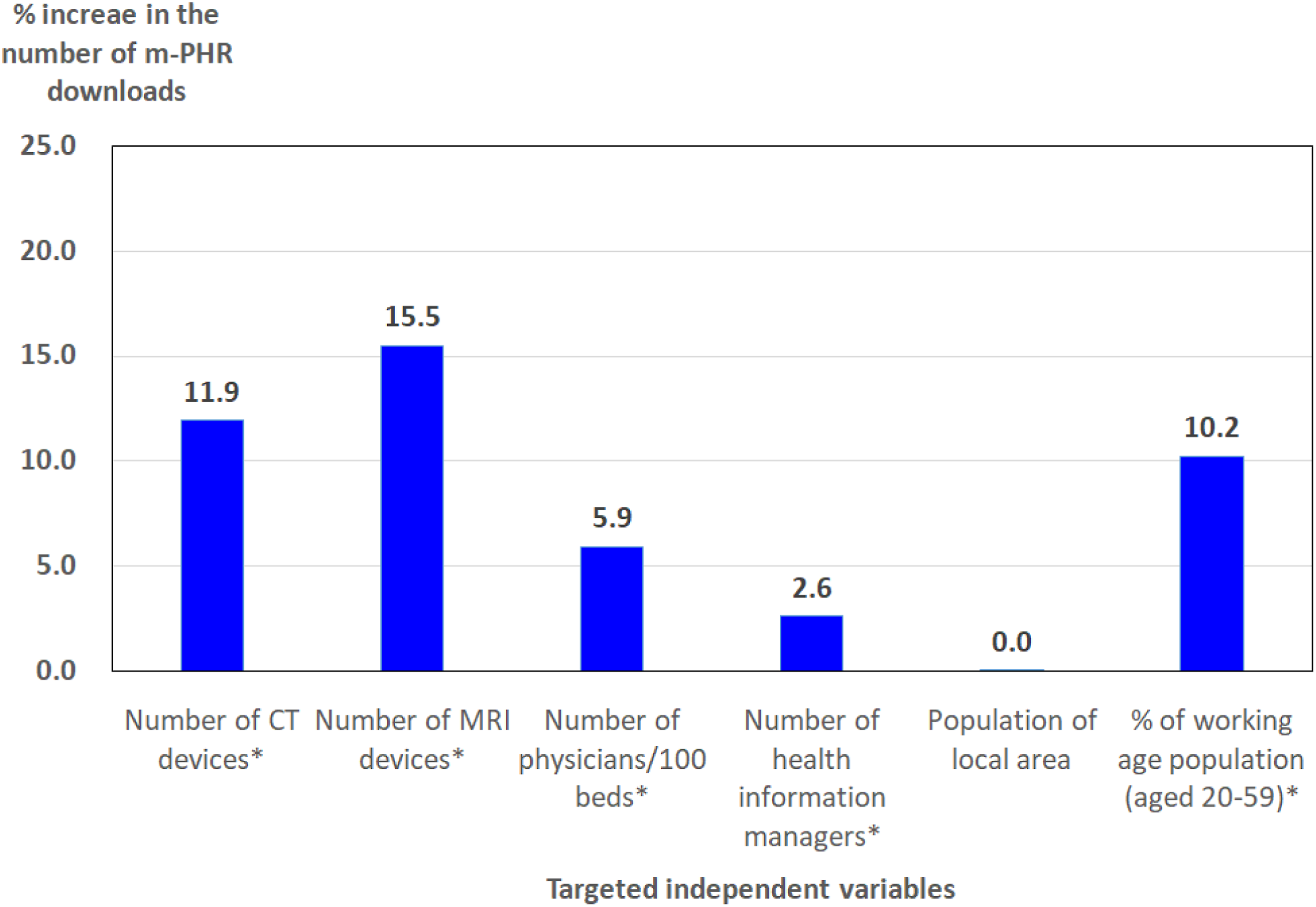
Discussion
This study investigated the main factors associated with the number of mobile personal health records (m-PHR) downloads and use with respect to a selection of Korean healthcare institutions. Six hypotheses were tested to explore the effects of organizational, technological, and environmental factors on the number of downloads, and we found that five out of six were supported after controlling for hospital covariates (i.e., medical equipment, medical staff adjusting for the number of beds, HIM staff, and local working-age population).
Regarding the technological factors, our results align with previous research finding that the amount of medical equipment was significantly associated with m-PHR adoption. 15 Although the dependent measures differed, it is still noteworthy that these results aligned. Hence, a certain level of triangulation was accomplished. PHR systems tend to increase patient satisfaction and provide at least an intangible return on investment. 32 The same is true for the influential organizational factors, as the sophistication and power of diagnostic capabilities have a major impact on diagnosis accuracy. It will be necessary to conduct additional research to better understand the return on investment for these technologies in more detail.
Regarding organizational factors, the number of downloads was significantly associated with the number of physicians and HIM staff. Interestingly, this finding aligns with those of prior studies, according to which m-PHR adoption was correlated with nurse and HIM staffing, and that of m-health was associated with hospital size.15,16 This study used the number of m-PHRA application downloads as the dependent variable, whereas prior studies focused on the adoption of general mobile medical information technologies. It seems obvious that hospitals with more resources would have advantages in this respect, and there are indeed positive relationships. However, it is important to understand which specific factors are the most influential.
Regarding the environmental features, it is interesting (albeit also expected) that the number of m-PHR application downloads increased with the proportion of the local resident population of working age. Most importantly, this was found to be true regardless of the absolute number of residents. This result complements those of other studies in which digital tools, such as smartphones, were found to be used most by younger people. 17 Thus, healthcare institutions should pay attention to local demographics and align their marketing efforts accordingly. For example, it is necessary for healthcare institutions to develop m-PHR systems that can be easily used by older people. They need not only to focus on marketing efforts, but also to create high-quality m-PHR systems in order to expand potential users.
Notably, compared with other m-health systems, m-PHR applications are especially helpful for chronic disease management; 32 hence, healthcare institutions aware of this fact can advocate more strongly for m-PHR use in the most affected communities. Additional studies (perhaps longitudinal) are needed to assess these potential benefits.
Furthermore, this study found that system-affiliated status, which was controlled for, was also consistently associated with the number of m-PHR downloads. This finding also aligns with that of a previous study conducted in the United States on the factors affecting the adoption of hospital information systems. They found that hospital market factors (e.g., system affiliation and preferred provider type) were significantly correlated. 33 This confirmation indicates that affiliated hospitals may have advantages when introducing m-PHR systems from an economy-of-scale perspective.
We noted three limitations in the conduct of this study. First, we focused on the raw number of m-PHR application downloads, assuming that each was unique and legitimate. In the future, methods of distinguishing the intent, efficacy, and attribution of application use should be considered. Second, this study did not consider the length of time (experience) hospitals spent employing and managing m-PHR systems owing to the lack of data. To minimize the effects of experiential advantages, this study controlled for the total number of years of hospital operations. Third, both the data and the interpretations of the results are only applicable to Korea; hence, the findings may be difficult to generalize globally, especially due to differences in healthcare systems. We suggest that future studies overcome some of these limitations by collecting a wider variety of data samples while using more generalizable methodologies.
Despite these limitations, our study results have several important implications from the standpoint of the academic contribution and originality of the study. First, this is the first study that has investigated the specific relationships between m-PHR application downloads and three hospital constructs based on the TOE model. From an academic point of view, the hypotheses based on the TOE framework explained the relationships well, as shown by the fact that five out of the six hypotheses were supported. These study results align with those of previous studies and help understand why many studies are adopting the TOE framework. Second, this is the first study using the number of m-PHR application downloads as an outcome variable, showing its originality. The topic of this study directly relates to m-PHR use, and this study has crucial implications for many nations, including Korea, that are planning nationalized m-health systems.34,35 Finally, many researchers might think that the number of m-PHR downloads and use by patients would be related to specific characteristics of hospitals. However, our study results show that these factors are not affected by a single factor, but by various factors reflecting hospitals’ technological, organizational, and environmental context. Good infrastructure such as medical and technological staff and advanced medical technologies may be related with adoption and download or use of m-PHR application. Thus healthcare policymakers need to understand this fact in order to accelerate the download and use of m-PHR applications by patients. Supporting hospitals to have better internal and external infrastructure would be one of political alternatives. For example, recommending hiring more staff on healthcare information managers to hospitals and providing recommendable standard guidelines on m-PHR development would be possible alternatives. It is necessary to support healthcare institutions in improving their organizational and managerial infrastructure and to develop high-quality m-PHR applications with easy-to-use interfaces. Healthcare institutions such as hospitals also need to develop high-quality, user-friendly m-PHR systems and make efforts to expand their target users to include older people.
Conclusion
This study found that the number of computed tomography (CT) devices, the number of MRI devices, the number of physicians adjusting for the number of hospital beds, the number of health information management staff, and the proportion of the working-age population of the local area were the main factors associated with the download and use of m-PHR in Korean hospitals. These results indirectly suggest that hospitals with advanced technological resources, organizational management and stable market conditions may be early adopters of m-PHR systems, which leads to an increased number of m-PHR application downloads. From a policy standpoint, the results of this study also suggest that the government needs to support hospitals in improving their internal and external operating environments regarding m-PHR operations in light of the finding that hospitals with good infrastructure and resources had more m-PHR application downloads. Hospitals may also need to develop high-quality m-PHR application systems with easy-to-use interfaces and extend the user base to include the elderly because the main users who downloaded m-PHR applications were concentrated in a specific age group.
Footnotes
Acknowledgments
The authors wish to thank Dr Byung Kwan Choi and Dr Dong Hwan Kim, Department of Neurosurgery, Pusan National University Hospital and College of Medicine, Korea, for providing extensive and important information on m-PHR system adoption status in Korea and giving us excellent comments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study obtained Institutional Review Board approval on 26 May 2022 (IRB number: jjIRB-220,526-HR-2022–0503). No consent to participate was required for this study.