
Abstract
Mobile devices and corresponding applications (apps) offer a unique potential for clinical work improvement. Healthcare employees already use them for a variety of clinical purposes. Even though their use might affect patients’ health and data security, they have rarely found their way into organizational knowledge management strategies. We present the current state of research regarding the prevalence, patterns, and trends of smartphone and tablet usage among physicians in clinical practice. Five electronic databases were searched for quantitative studies. The extracted data were systematically analyzed and visualized in boxplots. The results show an increasing prevalence of smartphones and medical apps in clinical practice, especially among junior physicians. Current applications can be subdivided into four categories: Communication and Organization, Documentation and Monitoring, Diagnostic and Therapeutic Decision Support, and Education. Among them, there is a large number of applications with a direct impact on physicians’ clinical actions and therefore on patients’ health and data security. In consequence, healthcare organizations should systematically integrate mobile devices and apps into their knowledge management strategies, including a modern IT infrastructure and training courses. Further studies are necessary to identify organizational and external factors that support an efficient mobile device usage during clinical practice.
Introduction
Healthcare organizations (HCOs) are subject to constant changes.1–4 In clinical practice, the impact of these changes can be noticed in several aspects: The complexity of disease patterns and medical care processes is increasing. This requires an interdisciplinary collaboration and coordination of large teams resulting in high communication needs. Furthermore, employees are directly exposed to rising patient expectations, new work requirements, high workloads and pressure to perform.5,6 At the same time, scientific and technological advances lead to an exponentially growing amount of data, information, and knowledge. In order to manage complex, data-intensive healthcare processes, there is a high demand for modern information and communication technologies (ICTs), embedded in a system of structured knowledge management (KM). 7 KM within an organization can be defined as the business process for generating, gathering, storing, organizing, sharing and using data, information and knowledge to achieve organizational goals e.g., to increase process efficiency, improve decision-making, support evidence-based practice and promote innovation.8,9
Mobile devices (e.g., smartphones, tablets) play an important role in the implementation of modern KM concepts in organizations, and thus also in HCOs. According to BinDhim and Trevena, the history of smartphones can be divided into a pre-iPhone era and a post-iPhone era. 10 In the pre-iPhone era, there were mobile phones, but only a few (office) applications existed and these were mostly developed for professionals. It was not until the first generation of iPhones was launched in 2007 that the rapid development of smartphones and application software (apps) began. They quickly became an important part of our daily lives. The market for tablet computers began to grow strongly with the introduction of the iPad device in 2010. According to Ramdurai, the use of apps in healthcare is still in its infancy. It has increased in recent years and will continue to grow rapidly. 11 Thus, the use of mobile devices in everyday life and in particular in clinical practice is a quite novel phenomenon with high innovation potential.
Mobile Health (mHealth), as an innovative subdiscipline of healthcare, focuses on the digital support of patients and medical professionals through mobile devices and corresponding apps. Mobile devices have tremendous advantages over stationary personal computers or telephones for clinical practice. They enable the generation, reception, processing, transmission and storage of digital data, information and knowledge relevant to patient care regardless of location and time.12,13 These features make them ideal tools for daily clinical collaboration. Due to highly developed cameras and sensor technologies, some types of devices offer a wide range of opportunities for an increased usage as diagnostic tools. 14 Together with appropriate apps, they can support physicians’ clinical work and moreover play an important role in digitization processes in hospitals.
The results of existing reviews already indicate the great importance of mobile devices for various aspects of clinical practice. In their systematic review, Martin et al. 15 examined the influence of mobile technology on teamwork and communication in hospitals. They found potential benefits of mobile technology for the workflow, accessibility, and the quality and efficiency of communication within and between teams. Dexheimer and Borycki analyzed the use of mobile devices in emergency departments in their scoping review. Despite the low level of research evidence, they saw great potential for an increased use of mobile devices, especially for decision support and charting. 16 Mickan et al. 17 analyzed randomized trials on the use of mobile devices in clinical practice. Mobile devices proved to be particularly effective when it came to accessing information, adherence to guidelines and clinical decision making. A Cochrane Review pointed to an improvement in intersectoral communication and care management when using mobile devices. 18
Mobile devices and apps have a high potential for driving medical innovation and KM improvement in clinical practice. Nevertheless, their application in a particularly sensitive area such as healthcare should be reviewed thoroughly. High demands are placed on the quality and safety of mobile devices and apps used for clinical purposes. In addition to the protection of patient and hospital data, the primary focus here is on patient safety. The use of mobile devices gives rise to numerous new liability scenarios, which thus makes this topic particularly relevant to clinic management.
The aim of this review was to systematically analyze quantitative data extracted from studies on the use of mobile devices by physicians in clinical practice in order to be able to derive concrete statements on the prevalence, patterns, and trends of usage. This opens up a new perspective on the use of mobile devices and, together with the information from former reviews, the particular relevance of mobile devices in clinical practice can be viewed in its entirety.
Methods
For this systematic review, the authors applied the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 item checklist. 19 The protocol for the review was registered on INPLASY (INPLASY202250087). 20
Search strategy
Five electronic databases (PubMed, Scopus, APA PsycInfo, Web of Science, Business Source Ultimate) were searched in April 2021 for studies analyzing the prevalence and patterns of mobile device usage (smartphones and tablets) of physicians in clinical practice. The last search was run on 25 April 2021. The following Boolean search string was created for the advanced database searches (Title/Abstract): (smartphone* OR “mobile phone*” OR “mobile application*” OR “cell phone*” OR “smart device*” OR “mobile device*” OR “mobile technolog*” OR tablet*) AND (physician* OR doctor* OR hospitalist* OR resident* OR “medical professional*” OR “medical practitioner*” OR “medical staff” OR clinician* OR surgeon* OR intern OR interns) AND (hospital* OR clinic* OR inpatient) AND (survey* OR questionnaire*)
Study selection
Records identified from the database search were exported and duplicates were removed. The remaining records were screened by title and abstract. Finally, full-text articles were assessed for eligibility. Irrelevant articles were excluded after each step. The data collection was performed by the first author and independently checked by the second author.
Inclusion and exclusion criteria
Studies included in this review are quantitative (or had a mixed methods design with relevant quantitative information), used a cross-sectional, self-report questionnaire-based research design, and were published in peer-reviewed journals in English or German (2012–present). Only results presenting physicians’ behavior were considered for the analysis. Results for groups of individuals other than physicians among the study population (i.e. medical students or nurses) were not included.
Data extraction
A data extraction sheet was developed. It was pilot-tested on the first five included studies and refined accordingly. The following data were extracted from the included studies: author(s); year of publication; year of data collection; journal; country; number of hospitals/medical centers; medical specialty; sample characteristics (structure, size); mobile devices; fields and prevalence of application. The results obtained were independently reviewed by the second author. In case of disagreement, consensus was reached by discussion.
Quality assessment
The quality of the included studies was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Studies Reporting Prevalence Data. 21 This checklist consists of nine items covering different methodological topics (e.g., sample frame, sample size, validity, response rate). There are four options to answer: Yes | No | Unclear | Not applicable. A maximum quality rating is 9 (all Yes), a minimum is 0 (all No or Unclear). Since there is no classification in terms of quality levels given by JBI, we decided to rate the quality of the studies with eight or nine points as “High”, the quality of the studies with 5–7 points as “Moderate”, and the quality of the studies with less than five points as “Low”. Based on the quality assessment, we excluded all studies with a low quality level from the quantitative analyses.
Data synthesis
In a final step, the data were prepared for analysis by summarizing and grouping them into four categories (Communication and Organization, Documentation and Monitoring, Diagnostic and Therapeutic Decision Support, Education). For each of the individual usage patterns (e.g., telephone calls, calendar, photography), a boxplot was created. Boxplots are an established method for visualizing data distributions and group differences. The box itself represents the middle 50% of the data, bounded by the lower quartile (25%) and the upper quartile (75%) (Figure 1). The horizontal line in the box is the median. The interquartile range is the range between the upper and lower quartiles. The vertical lines represent the minimum and maximum values, if they are within a range of 1.5 * interquartile range. Outliers (>1.5 * interquartile range) are represented by a dot. The crosses (X) indicate the arithmetic mean.22–24 To create the boxplots, data on the frequency of use (corresponding to the reported averages in each study) for each pattern were extracted from the individual studies. In our case, a boxplot shows how the data from the individual studies on, for example, the use of mobile devices to perform medical calculations are distributed. If enough data were available, comparisons were made between studies that included both junior and senior physicians and studies that only included junior physicians in their study population. Junior physicians are medical school graduates who have entered a residency program or similar (e.g., residents, trainee doctors, trainees, interns, fellows) whereas senior physicians have completed residency program and now supervise junior doctors (e.g., attendings, trainers, consultants, faculty members, academic physicians or higher positions). In order to identify temporal trends, we split the considered time period: Studies whose data collection began between 2010 and ‘14 were compared with studies whose data collection took place after 2014. Components of a boxplot.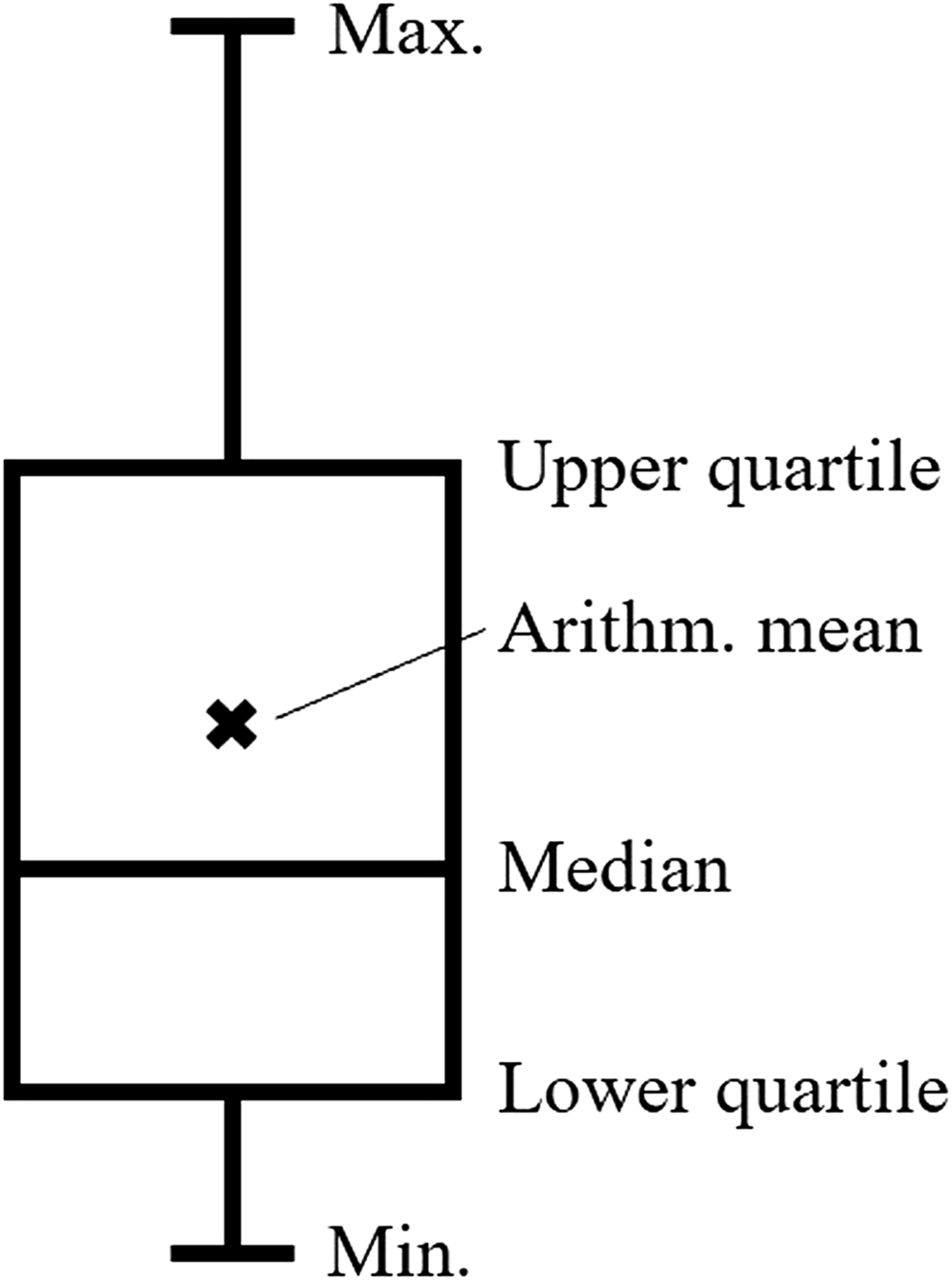
Results
Study selection
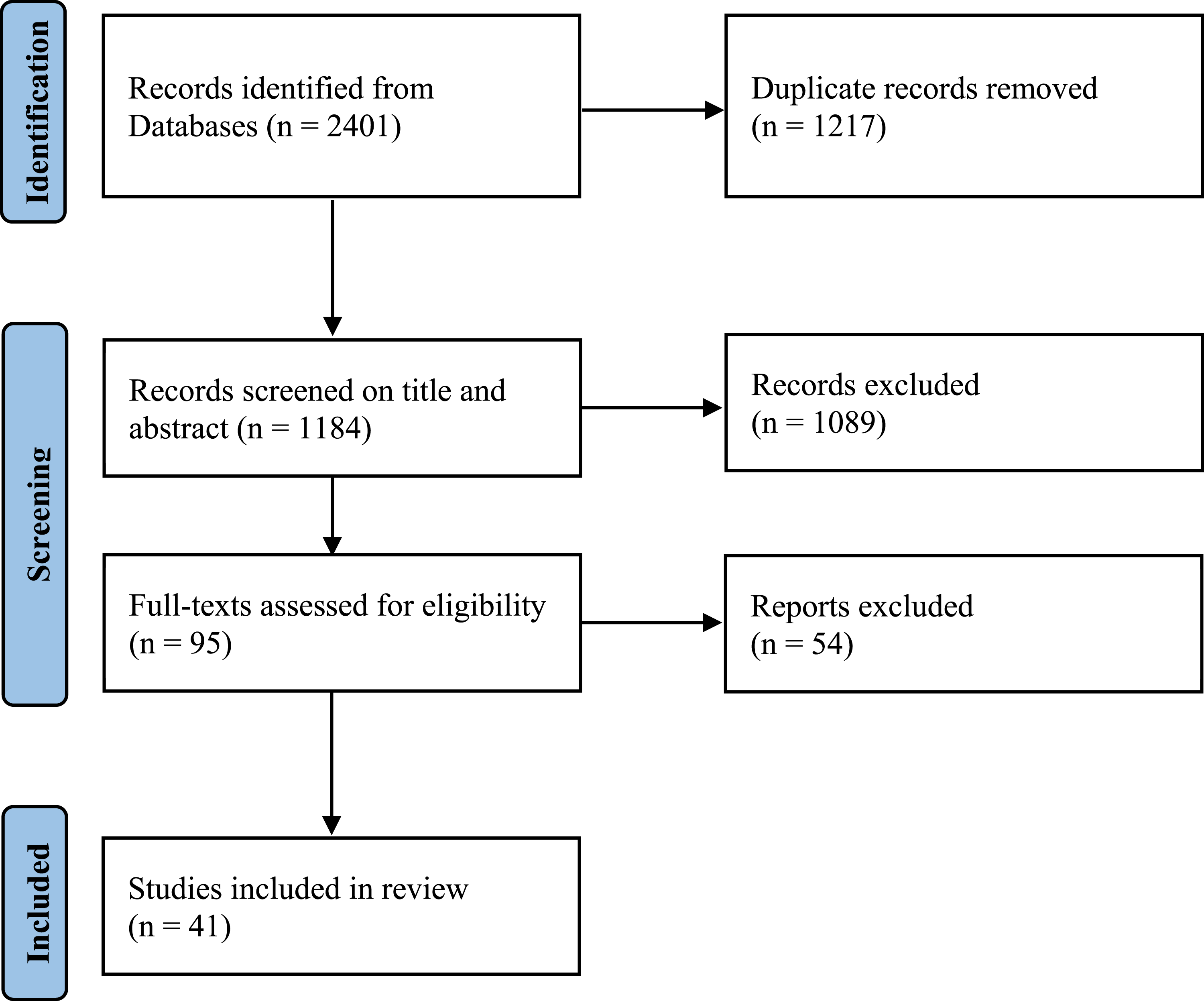
A total of 2401 records were identified through the database search. After duplicates had been removed, 1184 records were screened by title and abstract. Full-texts of 95 studies were assessed for eligibility. Fifty-four studies had to be excluded after full-text review due to a lack of specific information on the research topic, while 41 studies met the eligibility criteria and were therefore included in the systematic review. Figure 2 represents the identification and selection process using an adapted version of the PRISMA 2020 flow diagram.
19
Study identification and selection process using the PRISMA 2020 flow diagram.
19
Study characteristics
Table 1 [Appendix] displays basic study characteristics for each included study. This review summarizes the results of 41 studies from five different continents (Africa, Asia, Australia/Oceania, Europe, and North America). Most studies were conducted in high-income countries. However, a few studies also show results from emerging and developing countries. The number of hospitals/medical centers observed in each study varies: eight studies were conducted in a single hospital/medical center, another eight studies used data from two hospitals/medical centers. Most studies (n = 25) addressed three or more hospitals/medical centers. Furthermore, the number of participants included in the studies varies: The study with the smallest number of participants contains data from 36 participants, the biggest study had 3306 participants.25,26 More than half of the studies (n = 26) analyzed medical device usage across different medical specialties. The other studies focused on one particular specialty (e.g., Cardiology, Dermatology, Pathology). Most studies (n = 26) included both junior and senior physicians, while 15 studies specifically concentrated on junior physicians. Regarding the types of mobile devices, 23 studies analyzed smartphone usage only, and three studies focused on tablet usage. All other studies looked at a mix of devices.
Most of the studies only performed descriptive data analyses and simple correlation analyses. Based on this, they described the patterns of physicians’ mobile device usage, their motivation and perceived barriers. Only seven studies systematically analyzed factors facilitating and/or hindering mobile device usage (e.g., by means of the Technology Acceptance Model or organizational attributes).27–33
Assessment of risk of bias
Table 2 [Appendix] provides a detailed overview of the assessment of the quality of the included studies. A total of eight studies received a high quality rating (8 or nine points). The quality of 26 studies was rated as “Moderate”. According to our rating, seven studies were of low quality (less than five points). The most relevant causes for a potential bias are an inappropriate sample frame, an inadequate sample size, an insufficient coverage of the sample, invalid methods, and a low response rate.
Prevalence of mobile device usage and fields of application
The vast majority of studies reported a high prevalence of mobile device and app usage in clinical practice. In almost all studies with relevant information, the rate of smartphone ownership among physicians was over 90%. On average, more than 80% of the participants reported smartphone usage during clinical practice. Tablet ownership and usage were on a lower level: Slightly more than a half of the physicians asked owned a tablet and around a third used it during clinical practice. Medical apps were used by around two thirds of the doctors surveyed (Figure 3). General device ownership and usage in clinical practice.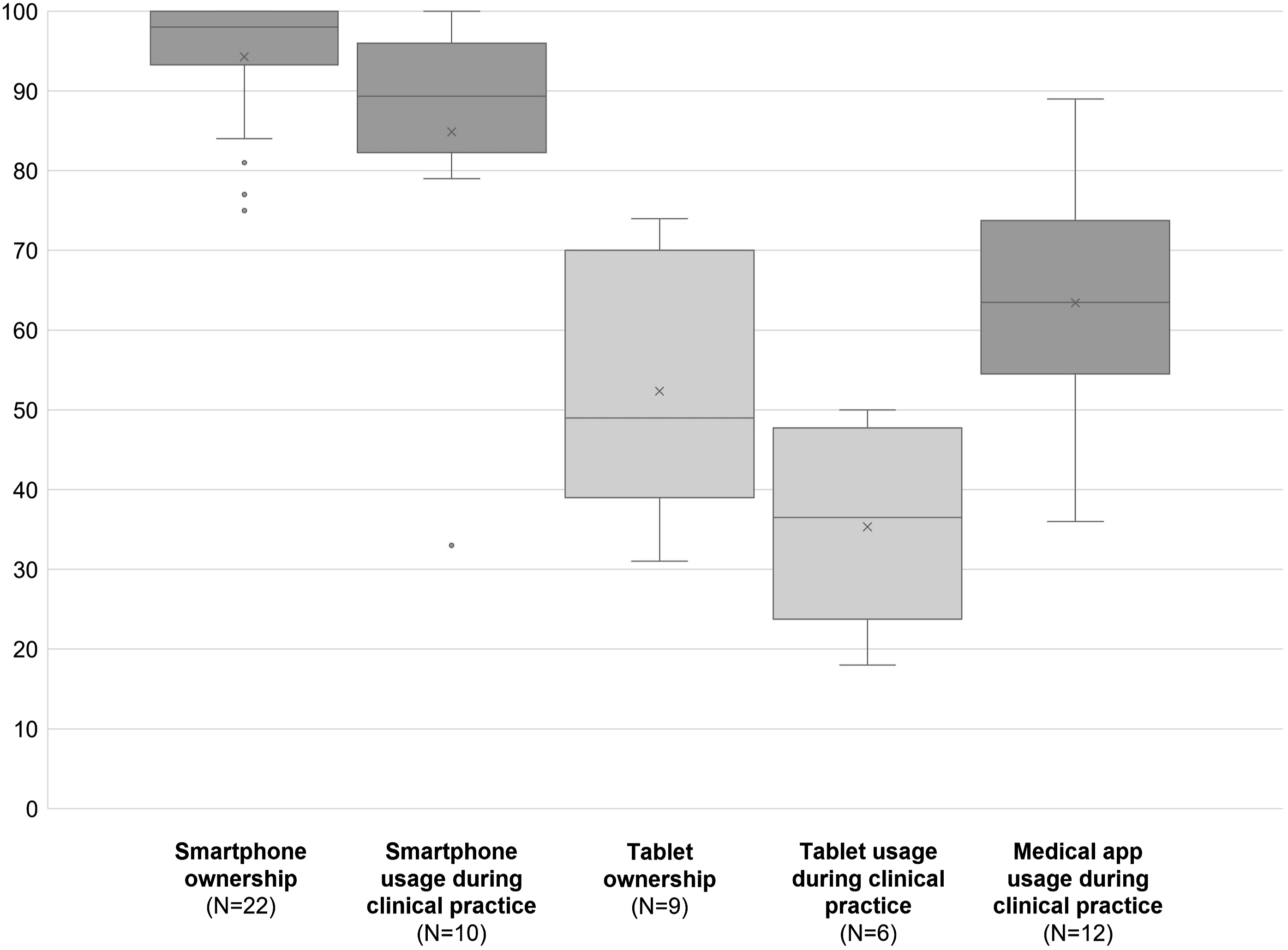
To structure the results for different mobile device applications in clinical practice, we formed four categories: Communication and Organization, Documentation and Monitoring, Diagnostic and Therapeutic Decision Support, Education. The categorization was based on the structures chosen by Maassen et al. 28 and Kameda-Smith et al., 34 and was modified according to our own research results. Table 3 [Appendix] summarizes our review findings concerning the fields of applications of mobile devices and apps by physicians during clinical practice.
Communication and organization
Most studies documented regular usage of mobile devices by physicians for a variety of communication reasons (e.g., to communicate critical alerts; to discuss patient information, tasks, or events; to answer pagers). A broad diversity of communication channels was described. The two most frequently mentioned types were e-mails as well as text and data messaging. Furthermore, physicians used their mobile devices, especially smartphones, for phone calls. The prevalence of usage was between 70 and 85% for all three communication channels. Junior physicians seemed to use their mobile devices as often as their senior colleagues for the purpose of text and data messaging and emails, slightly less for phone calls. Studies also highlighted social media use. Other communication channels mentioned were video calls, 35 patient portal, 36 web/video conferences,25,28 hospital/healthcare app 32 and telemedicine. 37 Although physicians interacted with different internal and external communication partners, the communication with staff (colleagues, educators, nursing staff, students, and support) seemed most important. Many physicians also used their mobile devices to get into contact with patients and their families. Some studies reported usage for private reasons (personal email, private communication) as well.28,29,35,38
Regarding organization, around two thirds of the physicians used digital calendars and scheduling functions. Additionally, some studies also mentioned notes or to-do-lists as mobile device applications.29,35,39 Other applications in this context were related to workflow support,
28
patient tracking,
40
physician orders,41,42 organization of contacts,
43
and PDF organization (Figure 4).
44
Prevalence of usage patterns regarding communication and organization.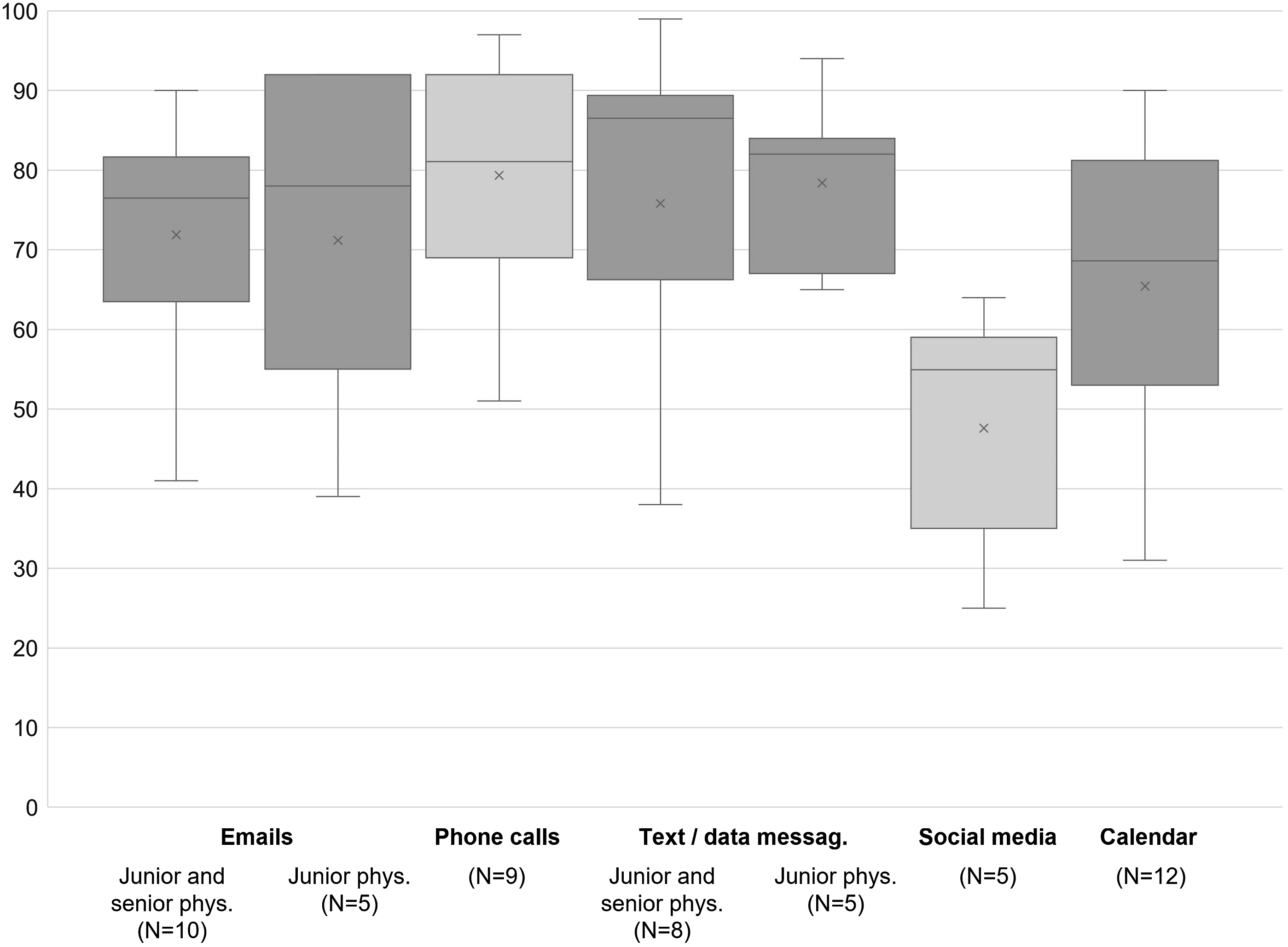
Documentation and monitoring
In this category, photography was the most popular application of mobile devices. More than half of the physicians used their mobile devices to take pictures/videos of patients, specific body areas, diagnostic studies or radiological images for a variety of reasons: diagnosis, monitoring disease or treatment progress, enabling digital follow-ups, communication with/advice from colleagues, education, research, and backups.
Mobile devices also gave physicians the opportunity of a remote access to electronic medical records (EMRs) and hospital information systems (HISs) and therefore to confidential patient data. Around one third of the physicians surveyed was already using this function in clinical practice. Furthermore, studies reported physicians’ usage of mobile devices for record keeping. This could be for procedure and case documentation,41,44–47 protocols,39,40 and reports
38
as well as coding and billing.26,32,48 However, during clinical practice physicians rarely performed record keeping via mobile devices. A few studies also pointed to the use of dictation functions,28,35,38 patient information storage,
25
and electronic logbooks (Figure 5).25,49 Prevalence of usage patterns regarding documentation and monitoring.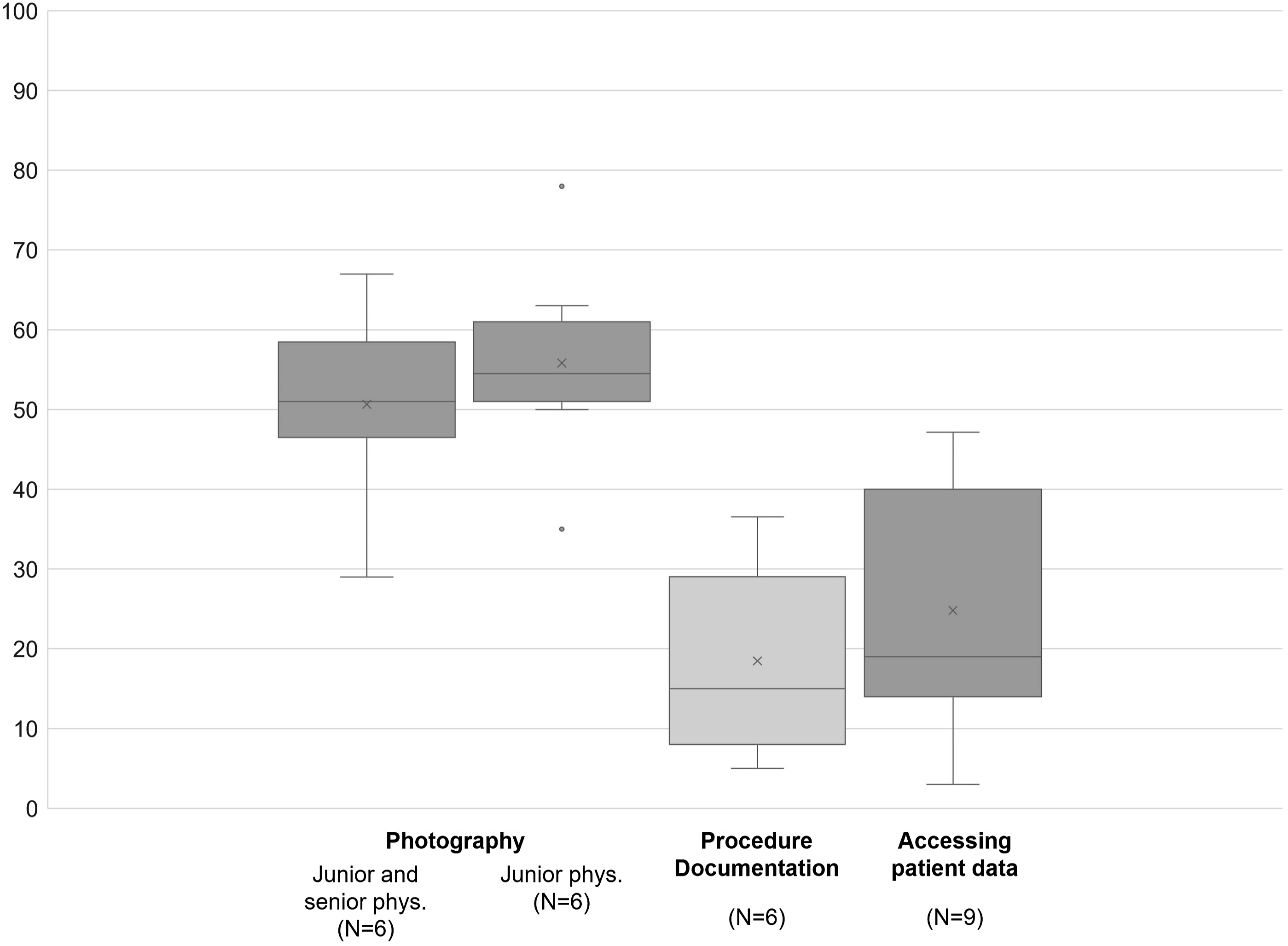
Diagnostic and therapeutic decision support
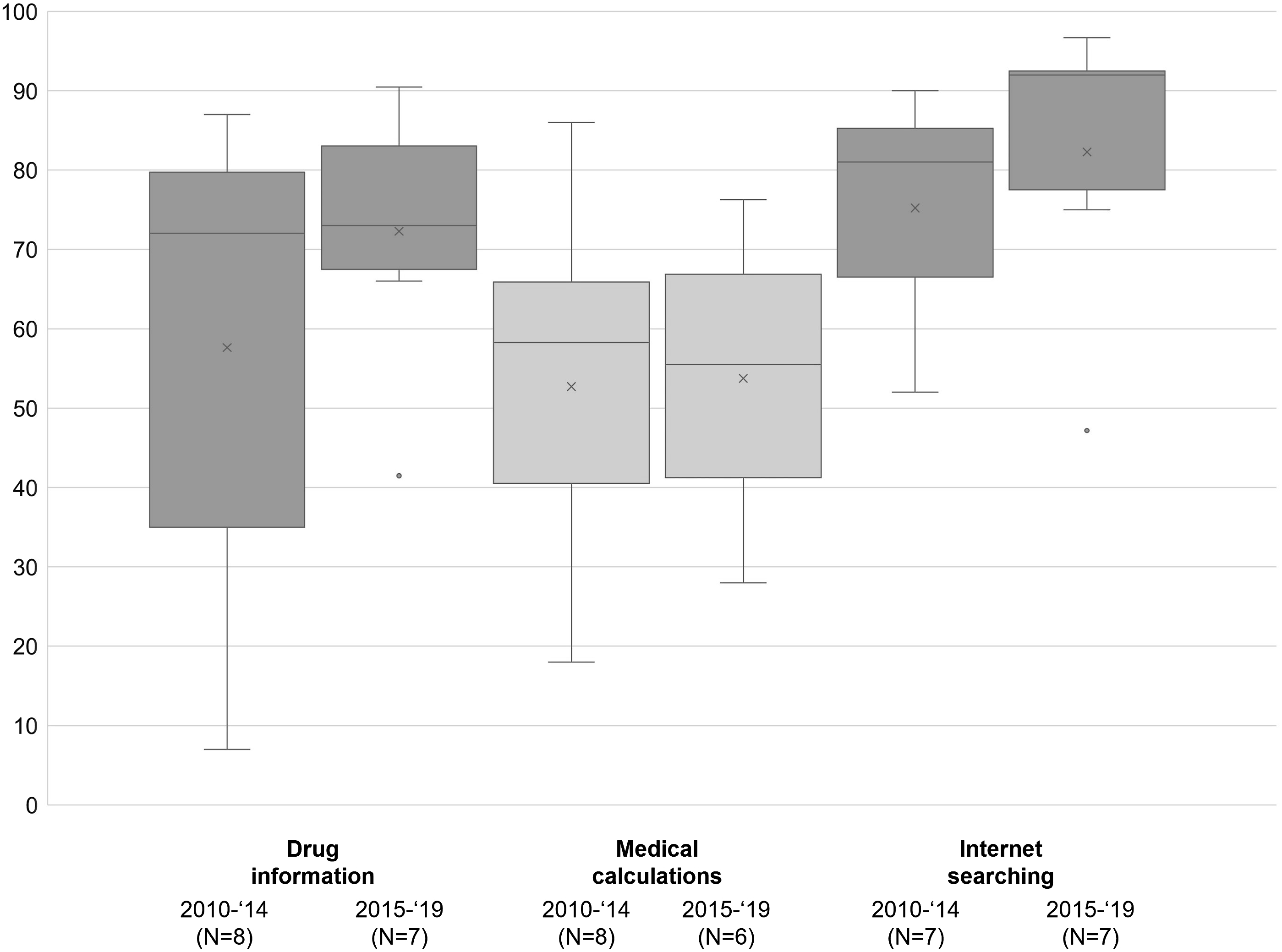
In this context, we define decision support as the use of mobile devices and apps to back physicians’ diagnostic or therapeutic process by providing additional digital information sources. A majority of studies analyzed the opportunity of obtaining digital information on drugs by using a mobile device and installed apps accordingly. The results showed that a majority of both junior and senior physicians accessed drug information sources via mobile devices, with a higher prevalence among junior physicians. Different types of drug information were mentioned: references, formularies, interactions, dosages, preparation, administration, pill identification, and indications.
Medical calculators were a second frequently mentioned decision support tool for physicians during clinical practice. We define medical calculators as any formula-based software application with a user-friendly interface that enables healthcare professionals to automatically calculate medical scores, indices or probabilities that support diagnosis and therapy.50,51 In every medical field there are calculators for a variety of issues. For instance, they can help to estimate dosages, risks, or due dates. Medical calculations via mobile devices seemed to be more prevalent among junior physicians: The usage rates for this purpose were much higher among studies analyzing junior physicians (∼65%) than for studies analyzing both junior and senior physicians (∼50%). Different apps/websites were mentioned that offer a broad variety of clinical calculators for every medical specialty, e.g. UpToDate,32,36,52,53 Medscape,34,37,39,48,53–56 Epocrates.34,37,48,52
A few studies also reported the usage of medical apps specifically designed to support physicians of a particular medical specialty.33,34,43,55 Furthermore, some studies described mobile device usage during differential diagnosis.35,37,38,53 Other relevant support tools highlighted by the studies included electronic guides/guidelines,25,26,28,32,37,39,40,48,49,52 data books,
57
handbooks,25,39,49,56 symptom trackers,
44
and examination tools (Figure 6).
44
Prevalence of usage patterns regarding diagnostic and therapeutic decision support.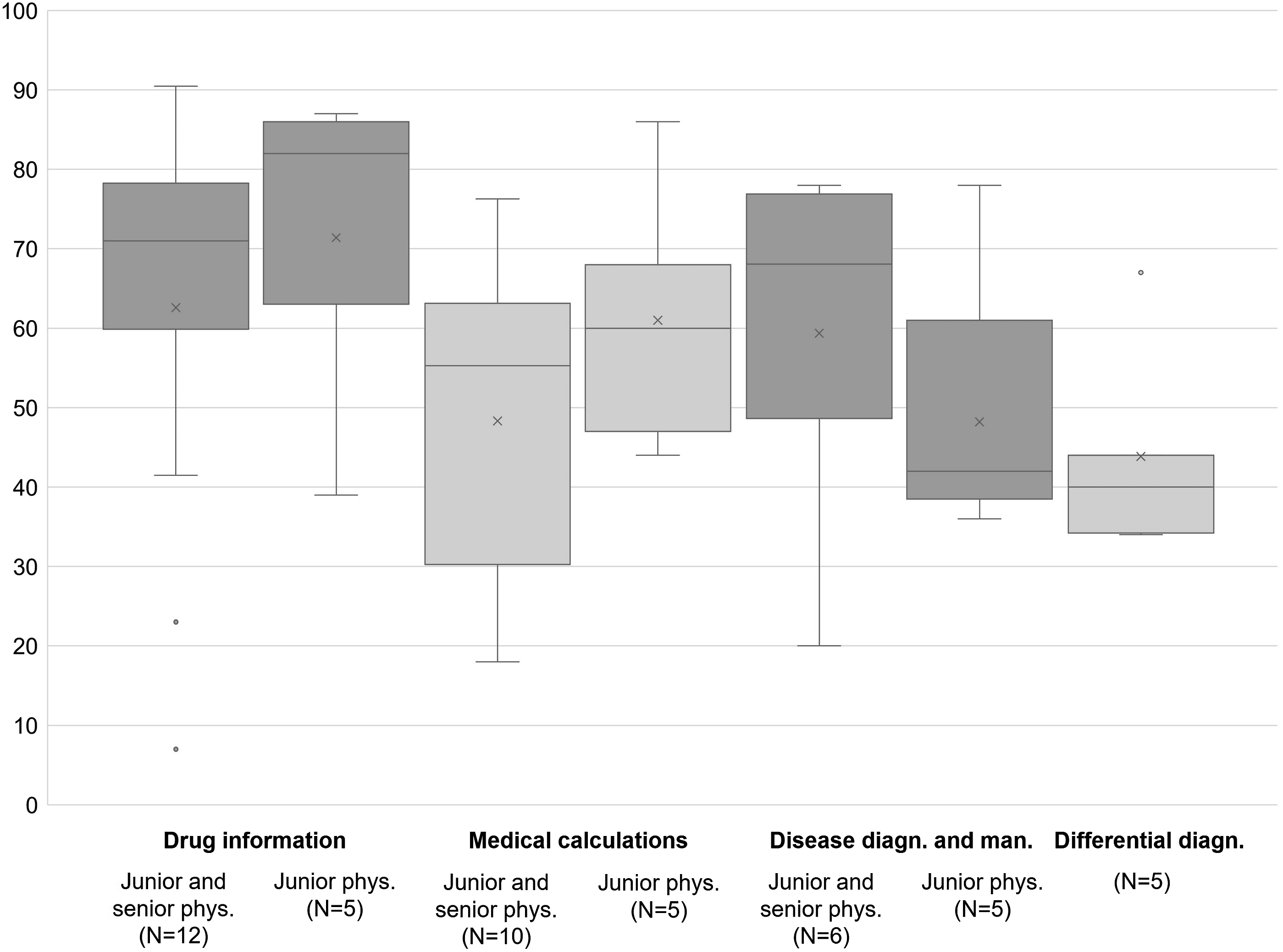
Education
Physicians used their medical devices to gather information for research, their personal education, and training. They acquired general medical knowledge and informed themselves about news and medical updates. A few studies also reported device usage for patient information and education.
The Internet/Web was mentioned most frequently as a source for easily accessible (medical) information (e.g., via Google or Wikipedia). The prevalence among the physicians surveyed was around 80%. E-books, digital textbooks/dictionaries and journals were further digital resources that physicians accessed using their mobile devices at work. Around half the physicians used their mobile devices to access these information sources. In addition, there were several apps that contained, among others, extensive information on current medical topics (e.g., Medscape, UpToDate). Other digital resources for medical knowledge acquisition mentioned in the studies were podcasts,
44
flashcards,
25
videos,
41
study/exam material,42,48 patient education material,41,42,48,58 and product/device information (Figure 7).
48
Prevalence of usage patterns regarding education.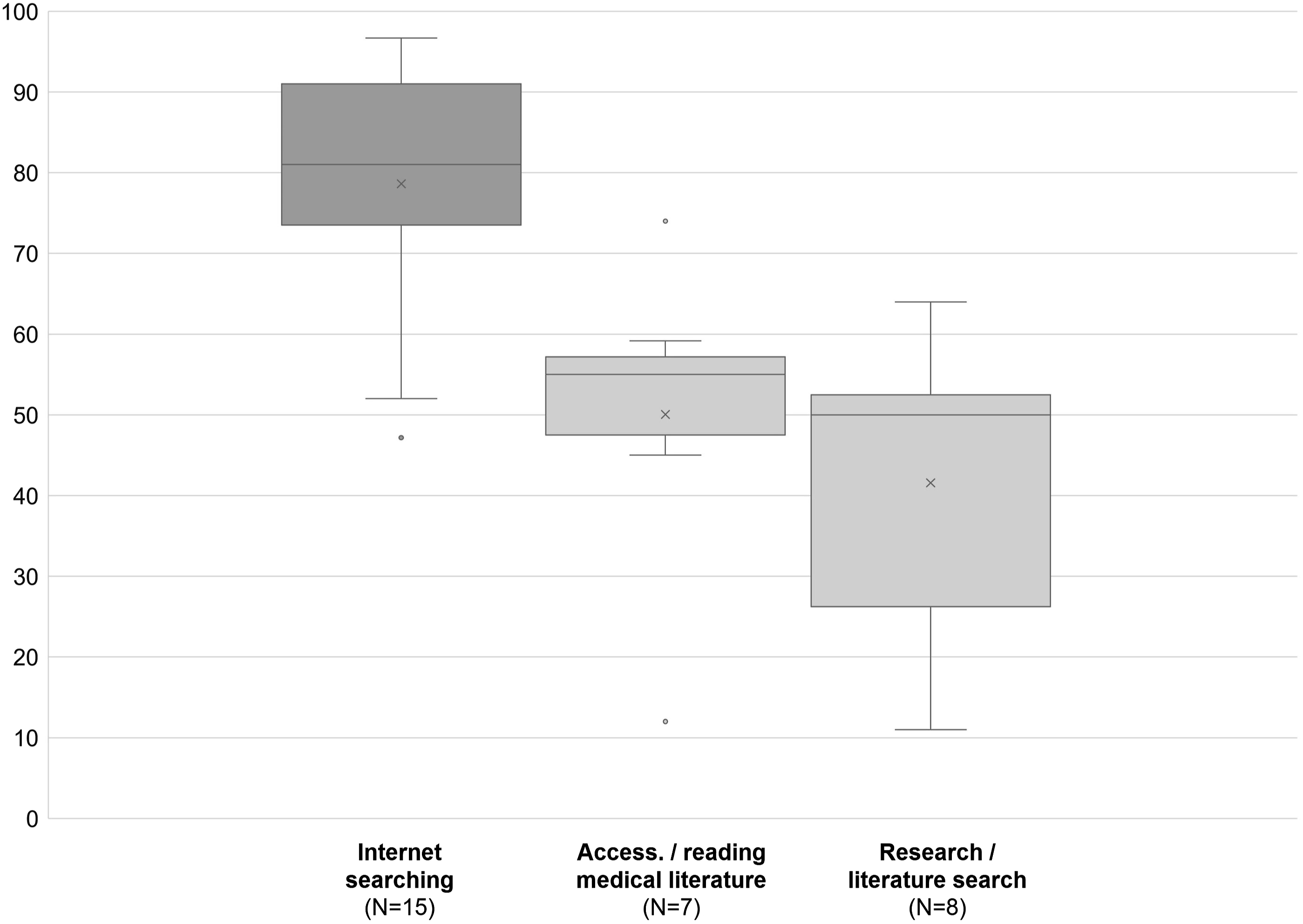
Trends of mobile device usage patterns
Based on the year of data collection, we performed comparisons between early and later studies. The results are visualized in Figures 8 and 9. For most of the usage patterns a clear trend can be seen: The use of mobile devices during clinical practice has increased. A growing proportion of physicians was using the various functions that smartphones and tablets offered to support their daily work. Trends in mobile device prevalence and usage patterns over time (based on the year of data collection). Trends in mobile device prevalence and usage patterns over time (based on the year of data collection).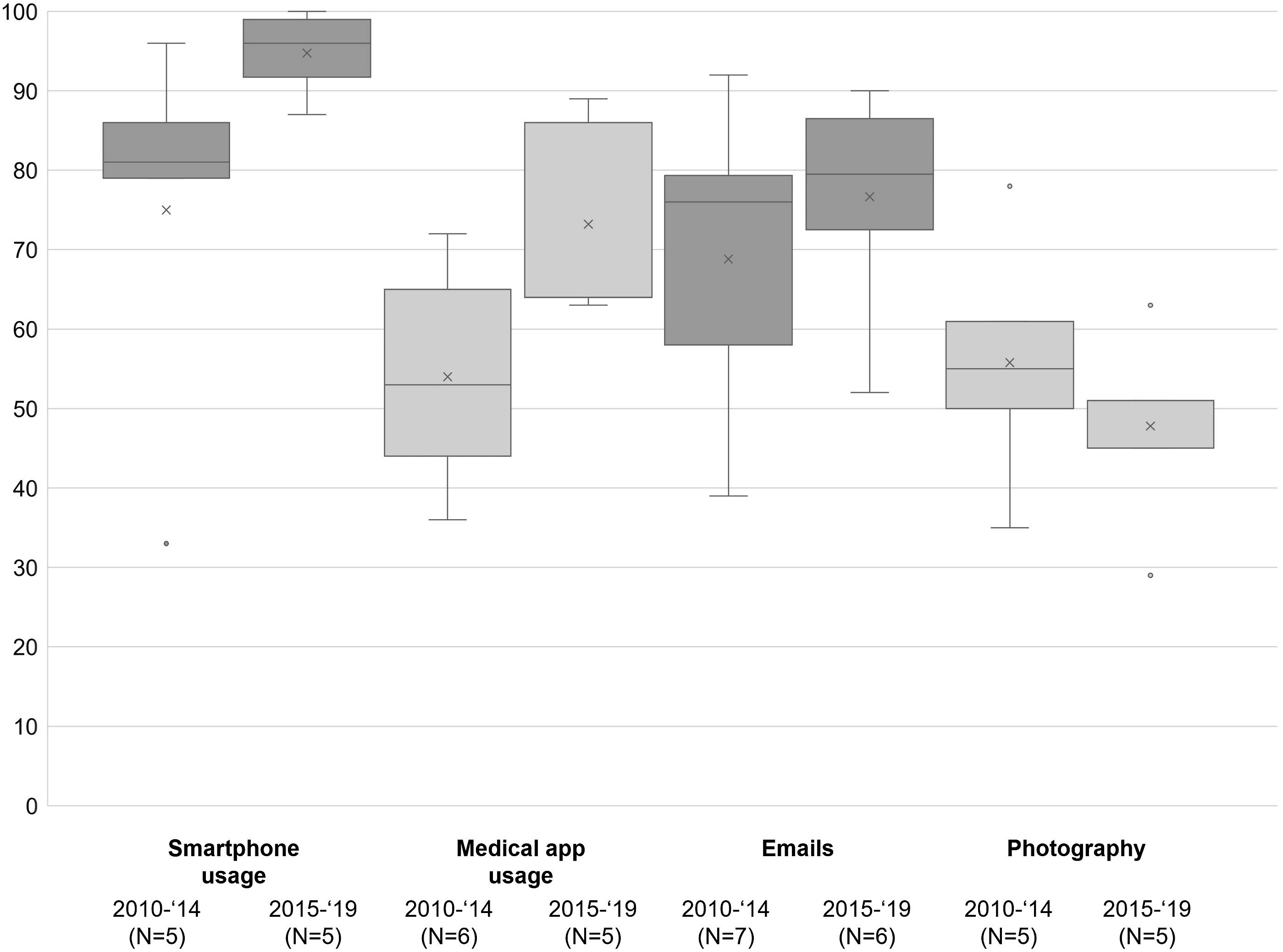
Discussion
High potential to improve clinical care and knowledge management
To the best of our knowledge, this review is the first offering a systematic appraisal of the current prevalence, patterns, and trends of mobile device usage by physicians in clinical practice based on data from quantitative studies published over the past decade. It highlights the already existing, very diverse influences of mobile devices on physicians’ actions and decisions, and therefore indirectly on patients’ health. Over the past decade, mobile devices, and smartphones in particular, have become an important means of providing digital support for physicians in everyday clinical practice offering a great variety of applications. Physicians use them, among others, for different communication purposes. Through the coordinated use of mobile devices, physicians could better support each other in decisions about diagnosis and therapy, even if they are not on site. The entire patient flow in healthcare organizations requires a high level of interdisciplinary coordination within and between teams, which could be made more efficient by using mobile devices. Compared to one-way pagers or telephones, smartphones have significant advantages in terms of flexibility, reception and efficiency of information transmission.32,38,40,59 The organization of everyday work can also be facilitated by mobile devices. In particular, the electronic calendar/scheduling function should be mentioned here.28–30,35,38,40,41,43,45,46,60,61 Due to their widespread availability and highly developed cameras and screens, mobile devices are often used for clinical photography.33–35,38,40,41,43,46,54,56,57,59,61 Often, there are no suitable alternatives to document procedures, cases, radiological or laboratory results for educational purposes or to have them available at the point-of-care. Furthermore, mobile devices provide the opportunity of remote access to electronic medical records and hospital information systems.28,31,36,42,43,48 Information can be obtained flexibly, and independently of time and location (e.g., at home or directly at point-of-care). Mobile devices already serve physicians as a digital vehicle for modern knowledge generation. Diagnostic and therapeutic decision support tools have a high potential for clinical innovation. The results show that junior physicians in particular use mobile devices in case they need specific drug information or medical calculations.32,33,38–41,47,53 This could be, because it allows them to compensate for their lack of experience and secure their own assessments. With the help of patient-specific, software-supported medication/drug information and medical calculations, patient-centered healthcare could be substantially improved. Multi-media medical education via apps could complete a modern training of physicians.62,63 Due to the high prevalence of a large number of usage patterns, the overall influence of mobile devices on clinical practice can already be rated as considerable. The described trends suggest that this influence will continue to increase in the future. Innovative areas such as digital diagnostic and therapeutic decision support tools could improve care in remote regions and provide essential data to physicians with little experience.
Relevant safety risks and security threats
Despite the great benefits for clinical practice, the use of mobile devices also poses several risks and threats to patient safety, information security, and data protection. A few of the included studies addressed these aspects and in some of them, physicians expressed concerns about the risks and threats and saw the need for organizational support.27,28,36,41,46,57,60,61 This resulted in three main measures suggested by the authors to increase the security of mobile device usage in clinical practice: education/training, regulations/guidelines/guidance, and technical support.25,34–36,38,40,41,44,46,49,56,57,60,65
Without sufficient organizational education and training, there is a high risk that patient safety, information security, and data protection are not adequately considered during clinical practice, e.g., when sharing patient data or trusting in medical calculator results. To avoid risks and liability issues during app usage, a thorough examination of those apps for suitability/intended purpose and safety as well as a plausibility check of the results provided are always required before diagnostic or therapy decisions are made based on their information. During clinical routine, this can barely be guaranteed by physicians. Here, medical societies or authorized organizations could come up with concrete recommendations to support physicians. In addition, it is important to have a clear legal basis for physicians’ actions concerning mobile device usage, including laws and guidelines from the government.
One aspect that has rarely been discussed in the studies included in this review are patient health risks due to inadequate hygiene measures during the application of mobile devices. Due to the COVID-19 pandemic, this point is becoming highly topical and important for healthcare organizations. Several other researchers have already analyzed and described the risk of transmission of nosocomial pathogens by mobile devices. 64
Practice implications
The variety of existing applications of mobile devices by physicians during clinical practice will increasingly raise the question of how HCOs want to deal with this development in the future. So far, the organizational implementation of a modern KM strategy, which includes a safe, secure, and professional use of mobile devices, has trailed far behind the actual usage patterns. ICT usage requires the improvement of the necessary infrastructure. In many studies physicians indicated that a poor Wi-Fi signal or even a lack of internet connection hindered their usage of mobile devices.29,35,37,52,59,61 However, a functioning ICT infrastructure represents the basis for organizational expansion within the four categories of mobile device usage mentioned in this review. When this is realized, solutions that are already in place but hardly implemented in the organizations (e.g., secure apps for internal communication) can quickly be integrated into clinical KM.
Next to infrastructural improvements, physicians will also need to be made even more aware of the opportunities and risks of using mobile devices and apps for clinical purposes. In this regard, HCOs could make a decisive contribution to increasing the sensitivity of physicians. External support is required to create high quality solutions for all, even for smaller and less funded organizations. Especially highly innovative fields such as decision support could benefit from cross-organizational solutions, for example provided by medical societies or authorized organizations.
Limitations and future research
Our review provides a broad overview of mobile device applications by physicians in clinical practice. However, several methodological limitations concerning the review process must be taken into account when interpreting the results of this review. Both authors jointly determined the search strategy, inclusion criteria and methods of result presentation. Despite the careful selection of the search terms, some studies may not have been found. All evaluation steps were carried out independently by the two reviewers. If the authors had different evaluations, this was discussed and agreement was reached. Nevertheless, there may be potential bias. The result classification into corresponding categories could also be associated with a bias potential due to subjective assessment. Furthermore, the diversity of researcher-designed questionnaires led to heterogeneous results that had to be summarized for the review. This can lead to information loss or misinterpretations. This review is based on five literature databases and does not include grey literature. In addition, only studies in English or German from 2012 to the present were considered, which could also have resulted in a study selection bias. However, the first iPad was launched in 2010 and we do not expect tablet use during clinical practice before then. Of the 41 studies considered, seven (17%) were of low quality. Due to the small proportion, we assume that these studies only have a small influence on the quality of our findings and do not influence the general argumentation. The number of participants included in the studies varies a lot. This must be taken into account when interpreting the results, because some studies represent data from physicians of only one hospital/medical center, while others represent data from national surveys.
The included studies raise questions about the specific motivation of physicians when using mobile devices for a particular purpose. It can be assumed that various aspects (e.g., organizational, personal, technical, external) influence user behavior. To better understand mobile device usage patterns, physicians’ motivation, and limiting factors, further research is needed. Here we see a particular need for qualitative research on physicians’ opinions, perceptions and concerns regarding risks and threats to patient safety, information security and data protection, and how to overcome them. This background could then help to define factors that influence the effectiveness of mobile device implementation into the KM strategies of HCOs. The consideration of the Golden Triangle consisting of people, process, and technology (PPT) could provide new insights into the context of a successful application of mobile devices to improve the level of achievement of organizational goals.
Conclusion
Mobile devices already support physicians during clinical practice in a variety of ways. Smartphones in particular can improve the processes of communication, organization, documentation, monitoring, decision support and, education. To increase clinical performance, support their employees, and simultaneously ensure patient safety and data security, HCOs should systematically implement mobile devices and apps into their KM strategies. In order to justify which organizational and external factors have an influence on the quality and quantity of mobile device usage during clinical practice, further studies are necessary that include focus group and/or correlation analyses. External support could, for example, come from medical societies that provide cross-organizational digital information with a high level of safety and security.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The APC is paid for under the ATLAS project “Innovation and digital transformation in healthcare” funded by the State of North Rhine-Westphalia, Germany [grant number: ITG-1-1].
Informed consent/ Patient consent
There are no human participants in this article and informed consent is not applicable.
Trial registration number/date
The protocol for the review was registered on INPLASY (INPLASY202250087) on 22 May 2022. INPLASY (INPLASY202250087).
Ethical Statement
Approval is not needed because of the article type.
Appendix
Included studies. For each study data on author(s), year of publication, country, medical specialty, study population, number of participating physicians, number of hospitals/medical centers, considered mobile devices, and considered fields of application was extracted.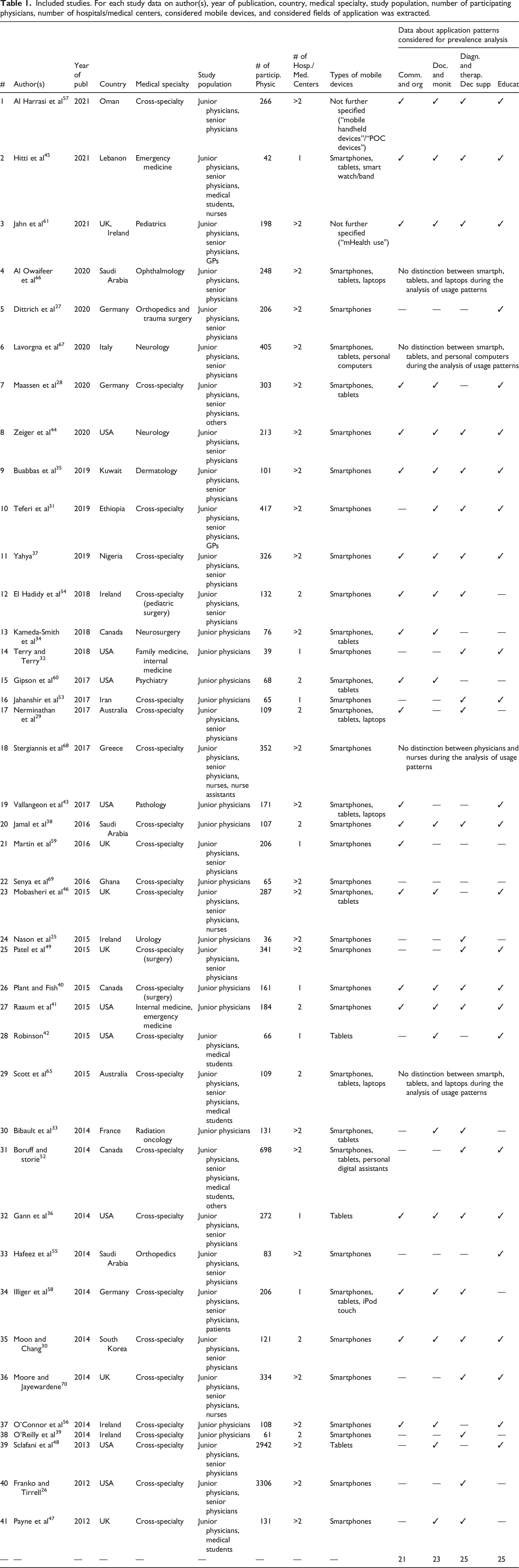
#
Author(s)
Year of publ
Country
Medical specialty
Study population
# of particip. Physic
# of Hosp./Med. Centers
Types of mobile devices
Data about application patterns considered for prevalence analysis
Comm. and org
Doc. and monit
Diagn. and therap. Dec supp
Educat
1
Al Harrasi et al
57
2021
Oman
Cross-specialty
Junior physicians, senior physicians
266
>2
Not further specified (“mobile handheld devices”/“POC devices")
✓
✓
✓
✓
2
Hitti et al
45
2021
Lebanon
Emergency medicine
Junior physicians, senior physicians, medical students, nurses
42
1
Smartphones, tablets, smart watch/band
✓
✓
✓
✓
3
Jahn et al
61
2021
UK, Ireland
Pediatrics
Junior physicians, senior physicians, GPs
198
>2
Not further specified (“mHealth use")
✓
✓
✓
✓
4
Al Owaifeer et al
66
2020
Saudi Arabia
Ophthalmology
Junior physicians, senior physicians
248
>2
Smartphones, tablets, laptops
No distinction between smartph, tablets, and laptops during the analysis of usage patterns
5
Dittrich et al
27
2020
Germany
Orthopedics and trauma surgery
Junior physicians, senior physicians
206
>2
Smartphones
—
—
—
✓
6
Lavorgna et al
67
2020
Italy
Neurology
Junior physicians, senior physicians
405
>2
Smartphones, tablets, personal computers
No distinction between smartph, tablets, and personal computers during the analysis of usage patterns
7
Maassen et al
28
2020
Germany
Cross-specialty
Junior physicians, senior physicians, others
303
>2
Smartphones, tablets
✓
✓
—
✓
8
Zeiger et al
44
2020
USA
Neurology
Junior physicians, senior physicians
213
>2
Smartphones
✓
✓
✓
✓
9
Buabbas et al
35
2019
Kuwait
Dermatology
Junior physicians, senior physicians
101
>2
Smartphones
✓
✓
✓
✓
10
Teferi et al
31
2019
Ethiopia
Cross-specialty
Junior physicians, senior physicians, GPs
417
>2
Smartphones
—
✓
✓
✓
11
Yahya
37
2019
Nigeria
Cross-specialty
Junior physicians, senior physicians
326
>2
Smartphones
✓
✓
✓
✓
12
El Hadidy et al
54
2018
Ireland
Cross-specialty (pediatric surgery)
Junior physicians, senior physicians
132
2
Smartphones
✓
✓
✓
—
13
Kameda-Smith et al
34
2018
Canada
Neurosurgery
Junior physicians
76
>2
Smartphones, tablets
✓
✓
—
—
14
Terry and Terry
32
2018
USA
Family medicine, internal medicine
Junior physicians
39
1
Smartphones
—
—
✓
✓
15
Gipson et al
60
2017
USA
Psychiatry
Junior physicians
68
2
Smartphones, tablets
✓
✓
—
—
16
Jahanshir et al
53
2017
Iran
Cross-specialty
Junior physicians
65
1
Smartphones
—
—
✓
✓
17
Nerminathan et al
29
2017
Australia
Cross-specialty
Junior physicians, senior physicians
109
2
Smartphones, tablets, laptops
✓
—
✓
—
18
Stergiannis et al
68
2017
Greece
Cross-specialty
Junior physicians, senior physicians, nurses, nurse assistants
352
>2
Smartphones
No distinction between physicians and nurses during the analysis of usage patterns
19
Vallangeon et al
43
2017
USA
Pathology
Junior physicians
171
>2
Smartphones, tablets, laptops
✓
—
—
✓
20
Jamal et al
38
2016
Saudi Arabia
Cross-specialty
Junior physicians
107
2
Smartphones
✓
✓
✓
✓
21
Martin et al
59
2016
UK
Cross-specialty
Junior physicians, senior physicians
206
1
Smartphones
✓
—
—
—
22
Senya et al
69
2016
Ghana
Cross-specialty
Junior physicians
65
>2
Smartphones
—
—
—
—
23
Mobasheri et al
46
2015
UK
Cross-specialty
Junior physicians, senior physicians, nurses
287
>2
Smartphones, tablets
✓
✓
—
✓
24
Nason et al
25
2015
Ireland
Urology
Junior physicians
36
>2
Smartphones
—
—
✓
—
25
Patel et al
49
2015
UK
Cross-specialty (surgery)
Junior physicians, senior physicians
341
>2
Smartphones
—
—
✓
✓
26
Plant and Fish
40
2015
Canada
Cross-specialty (surgery)
Junior physicians
161
1
Smartphones
✓
✓
✓
✓
27
Raaum et al
41
2015
USA
Internal medicine, emergency medicine
Junior physicians
184
2
Smartphones
✓
✓
✓
✓
28
Robinson
42
2015
USA
Cross-specialty
Junior physicians, medical students
66
1
Tablets
—
✓
—
✓
29
Scott et al
65
2015
Australia
Cross-specialty
Junior physicians, senior physicians, medical students
109
2
Smartphones, tablets, laptops
No distinction between smartph, tablets, and laptops during the analysis of usage patterns
30
Bibault et al
33
2014
France
Radiation oncology
Junior physicians
131
>2
Smartphones, tablets
—
✓
✓
—
31
Boruff and storie
52
2014
Canada
Cross-specialty
Junior physicians, senior physicians, medical students, others
698
>2
Smartphones, tablets, personal digital assistants
—
—
✓
✓
32
Gann et al
36
2014
USA
Cross-specialty
Junior physicians, senior physicians
272
1
Tablets
✓
✓
✓
✓
33
Hafeez et al
55
2014
Saudi Arabia
Orthopedics
Junior physicians, senior physicians
83
>2
Smartphones
—
—
—
✓
34
Illiger et al
58
2014
Germany
Cross-specialty
Junior physicians, senior physicians, patients
206
1
Smartphones, tablets, iPod touch
✓
✓
✓
—
35
Moon and Chang
30
2014
South Korea
Cross-specialty
Junior physicians, senior physicians
121
2
Smartphones
✓
✓
✓
✓
36
Moore and Jayewardene
70
2014
UK
Cross-specialty
Junior physicians, senior physicians, nurses
334
>2
Smartphones
—
—
✓
✓
37
O’Connor et al
56
2014
Ireland
Cross-specialty
Junior physicians
108
>2
Smartphones
✓
✓
—
✓
38
O’Reilly et al
39
2014
Ireland
Cross-specialty
Junior physicians
61
2
Smartphones
—
—
✓
—
39
Sclafani et al
48
2013
USA
Cross-specialty
Junior physicians, senior physicians
2942
>2
Tablets
—
✓
—
✓
40
Franko and Tirrell
26
2012
USA
Cross-specialty
Junior physicians, senior physicians
3306
>2
Smartphones
—
—
✓
—
41
Payne et al
47
2012
UK
Cross-specialty
Junior physicians, medical students
131
>2
Smartphones
—
✓
✓
—
—
—
—
—
—
—
—
—
—
21
23
25
25
Risk of bias assessment.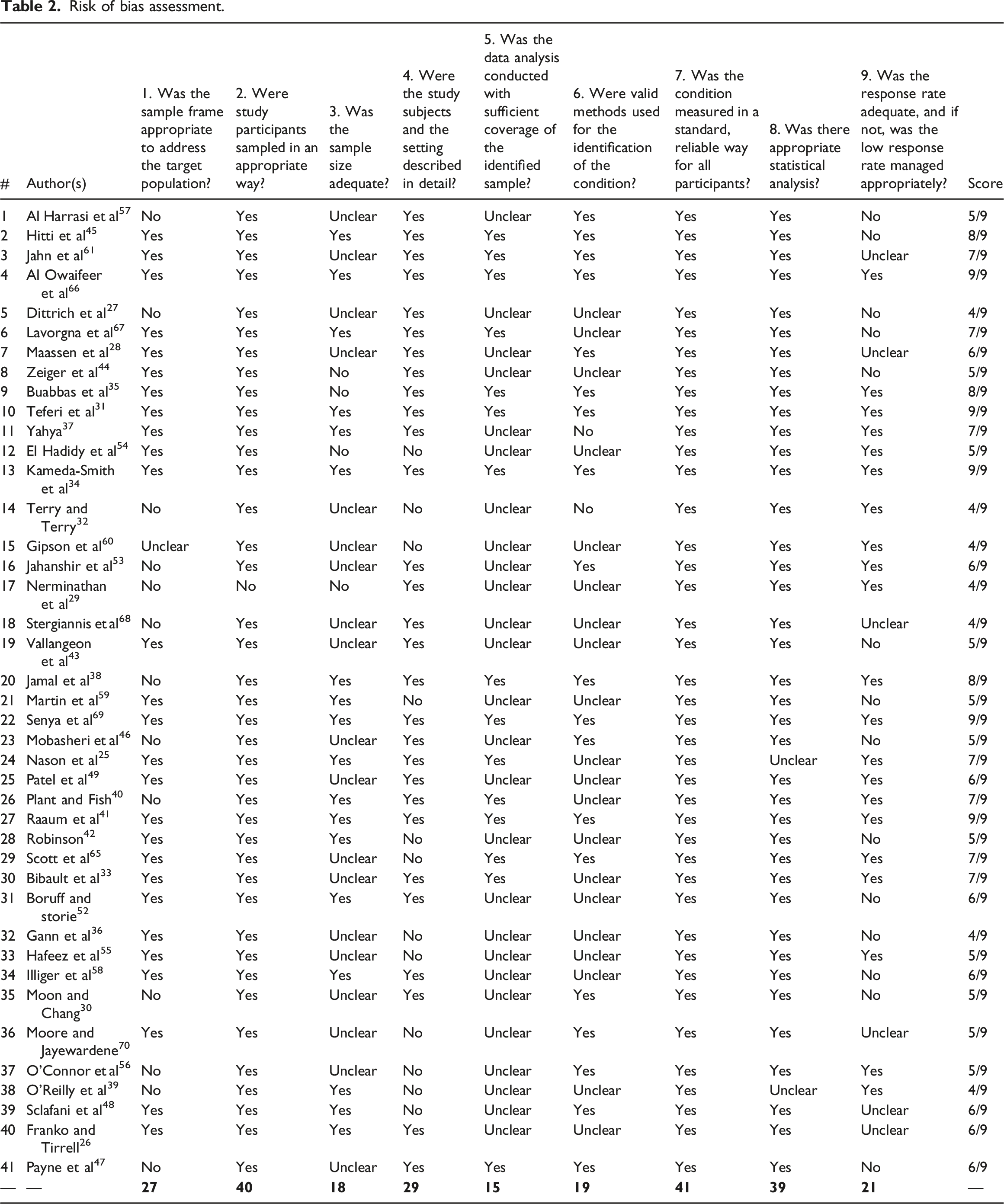
#
Author(s)
1. Was the sample frame appropriate to address the target population?
2. Were study participants sampled in an appropriate way?
3. Was the sample size adequate?
4. Were the study subjects and the setting described in detail?
5. Was the data analysis conducted with sufficient coverage of the identified sample?
6. Were valid methods used for the identification of the condition?
7. Was the condition measured in a standard, reliable way for all participants?
8. Was there appropriate statistical analysis?
9. Was the response rate adequate, and if not, was the low response rate managed appropriately?
Score
1
Al Harrasi et al
57
No
Yes
Unclear
Yes
Unclear
Yes
Yes
Yes
No
5/9
2
Hitti et al
45
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
8/9
3
Jahn et al
61
Yes
Yes
Unclear
Yes
Yes
Yes
Yes
Yes
Unclear
7/9
4
Al Owaifeer et al
66
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
9/9
5
Dittrich et al
27
No
Yes
Unclear
Yes
Unclear
Unclear
Yes
Yes
No
4/9
6
Lavorgna et al
67
Yes
Yes
Yes
Yes
Yes
Unclear
Yes
Yes
No
7/9
7
Maassen et al
28
Yes
Yes
Unclear
Yes
Unclear
Yes
Yes
Yes
Unclear
6/9
8
Zeiger et al
44
Yes
Yes
No
Yes
Unclear
Unclear
Yes
Yes
No
5/9
9
Buabbas et al
35
Yes
Yes
No
Yes
Yes
Yes
Yes
Yes
Yes
8/9
10
Teferi et al
31
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
9/9
11
Yahya
37
Yes
Yes
Yes
Yes
Unclear
No
Yes
Yes
Yes
7/9
12
El Hadidy et al
54
Yes
Yes
No
No
Unclear
Unclear
Yes
Yes
Yes
5/9
13
Kameda-Smith et al
34
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
9/9
14
Terry and Terry
32
No
Yes
Unclear
No
Unclear
No
Yes
Yes
Yes
4/9
15
Gipson et al
60
Unclear
Yes
Unclear
No
Unclear
Unclear
Yes
Yes
Yes
4/9
16
Jahanshir et al
53
No
Yes
Unclear
Yes
Unclear
Yes
Yes
Yes
Yes
6/9
17
Nerminathan et al
29
No
No
No
Yes
Unclear
Unclear
Yes
Yes
Yes
4/9
18
Stergiannis et al
68
No
Yes
Unclear
Yes
Unclear
Unclear
Yes
Yes
Unclear
4/9
19
Vallangeon et al
43
Yes
Yes
Unclear
Yes
Unclear
Unclear
Yes
Yes
No
5/9
20
Jamal et al
38
No
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
8/9
21
Martin et al
59
Yes
Yes
Yes
No
Unclear
Unclear
Yes
Yes
No
5/9
22
Senya et al
69
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
9/9
23
Mobasheri et al
46
No
Yes
Unclear
Yes
Unclear
Yes
Yes
Yes
No
5/9
24
Nason et al
25
Yes
Yes
Yes
Yes
Yes
Unclear
Yes
Unclear
Yes
7/9
25
Patel et al
49
Yes
Yes
Unclear
Yes
Unclear
Unclear
Yes
Yes
Yes
6/9
26
Plant and Fish
40
No
Yes
Yes
Yes
Yes
Unclear
Yes
Yes
Yes
7/9
27
Raaum et al
41
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
9/9
28
Robinson
42
Yes
Yes
Yes
No
Unclear
Unclear
Yes
Yes
No
5/9
29
Scott et al
65
Yes
Yes
Unclear
No
Yes
Yes
Yes
Yes
Yes
7/9
30
Bibault et al
33
Yes
Yes
Unclear
Yes
Yes
Unclear
Yes
Yes
Yes
7/9
31
Boruff and storie
52
Yes
Yes
Yes
Yes
Unclear
Unclear
Yes
Yes
No
6/9
32
Gann et al
36
Yes
Yes
Unclear
No
Unclear
Unclear
Yes
Yes
No
4/9
33
Hafeez et al
55
Yes
Yes
Unclear
No
Unclear
Unclear
Yes
Yes
Yes
5/9
34
Illiger et al
58
Yes
Yes
Yes
Yes
Unclear
Unclear
Yes
Yes
No
6/9
35
Moon and Chang
30
No
Yes
Unclear
Yes
Unclear
Yes
Yes
Yes
No
5/9
36
Moore and Jayewardene
70
Yes
Yes
Unclear
No
Unclear
Yes
Yes
Yes
Unclear
5/9
37
O’Connor et al
56
No
Yes
Unclear
No
Unclear
Yes
Yes
Yes
Yes
5/9
38
O’Reilly et al
39
No
Yes
Yes
No
Unclear
Unclear
Yes
Unclear
Yes
4/9
39
Sclafani et al
48
Yes
Yes
Yes
No
Unclear
Yes
Yes
Yes
Unclear
6/9
40
Franko and Tirrell
26
Yes
Yes
Yes
Yes
Unclear
Unclear
Yes
Yes
Unclear
6/9
41
Payne et al
47
No
Yes
Unclear
Yes
Yes
Yes
Yes
Yes
No
6/9
—
—
—
Review findings concerning fields of applications of mobile devices and apps by physicians during clinical practice.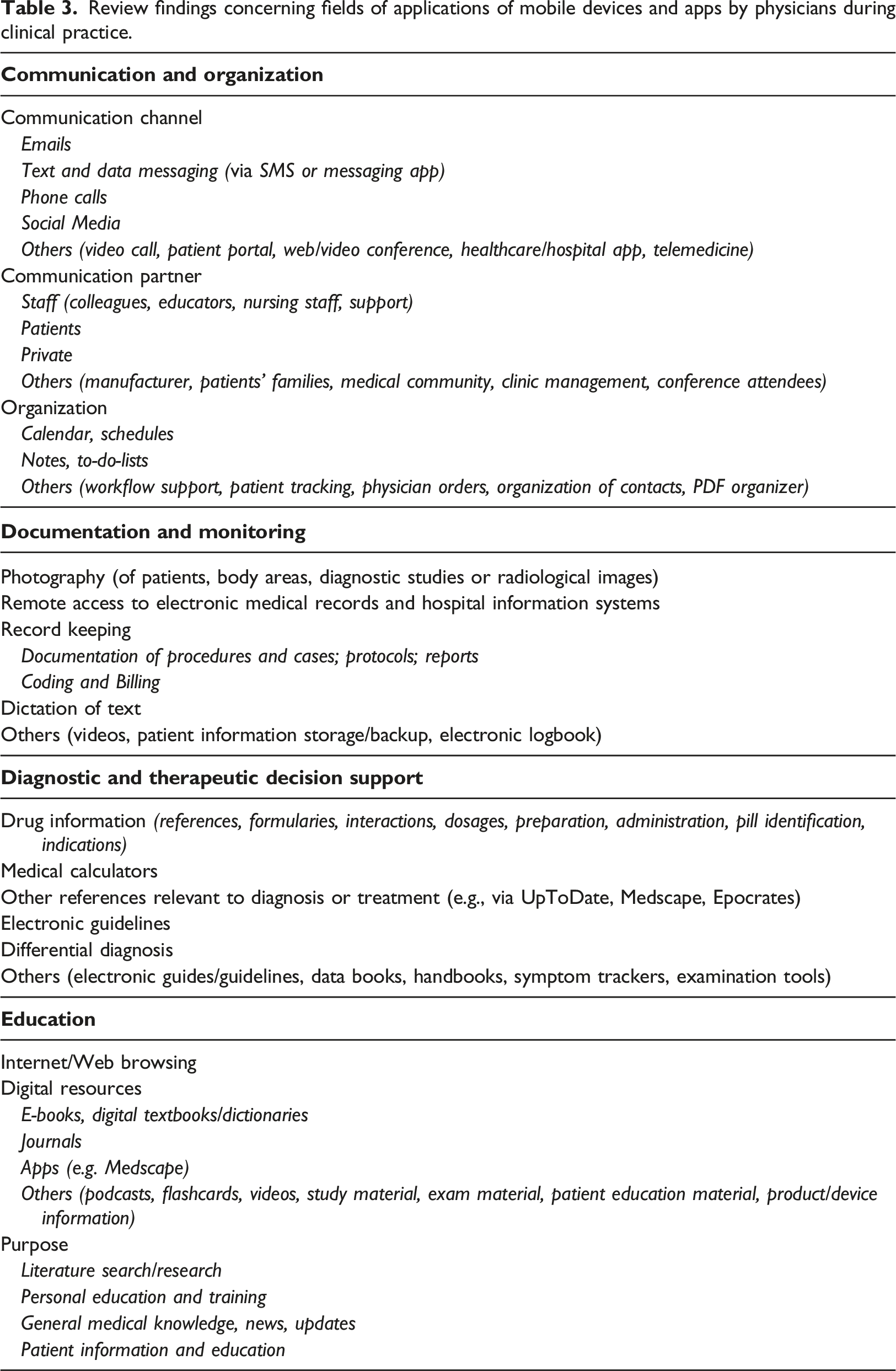
Communication channel
Emails
Text and data messaging (via SMS or messaging app)
Phone calls
Social Media
Others (video call, patient portal, web/video conference, healthcare/hospital app, telemedicine)
Communication partner
Staff (colleagues, educators, nursing staff, support)
Patients
Private
Others (manufacturer, patients' families, medical community, clinic management, conference attendees)
Organization
Calendar, schedules
Notes, to-do-lists
Others (workflow support, patient tracking, physician orders, organization of contacts, PDF organizer)
Photography (of patients, body areas, diagnostic studies or radiological images)
Remote access to electronic medical records and hospital information systems
Record keeping
Documentation of procedures and cases; protocols; reports
Coding and Billing
Dictation of text
Others (videos, patient information storage/backup, electronic logbook)
Drug information (references, formularies, interactions, dosages, preparation, administration, pill identification, indications)
Medical calculators
Other references relevant to diagnosis or treatment (e.g., via UpToDate, Medscape, Epocrates)
Electronic guidelines
Differential diagnosis
Others (electronic guides/guidelines, data books, handbooks, symptom trackers, examination tools)
Internet/Web browsing
Digital resources
E-books, digital textbooks/dictionaries
Journals
Apps (e.g. Medscape)
Others (podcasts, flashcards, videos, study material, exam material, patient education material, product/device information)
Purpose
Literature search/research
Personal education and training
General medical knowledge, news, updates
Patient information and education