
Abstract
This study investigated the feasibility and usability of a personalized mobile health (mHealth) app for self-management during the year following breast cancer surgery. Twenty-nine participants were instructed to use an app and smart band immediately after discharge. Only 18 completed the study. Their perceived necessity and satisfaction for main domains and app were assessed at 1, 2, 4, 6, 9, and 12 months. A self-reporting questionnaire assessed usability at 12 months. Consequently, retention rate as measures of feasibility showed a mean of 75.8%. Exercise and diet management were the most accessed app domains. Perceived necessity was higher than satisfaction. The mean usability score was 80.2. Most participants found the app useful and effective as a delivery for healthcare. Further, 94% of them were willing to pay for and recommend it. Thus, mHealth app can help breast cancer patients improve their healthy behaviors and healthcare further. This study provides insights for designing long-term randomized controlled trials using mHealth interventions.
Introduction
In 2020, a total of 9,958,133 people died of cancer worldwide, and of these, 684,996 died of breast cancer, making it the fifth leading cause of cancer death. 1 Among female patients diagnosed with breast cancer, the highest incidence was observed in those aged between 40–49 years (9,432 patients, 33.6%) in 2018. 2 Regarding the care continuum, such patients receive standard care, including breast preservation or resection, chemotherapy, radiotherapy, hormone therapy, and targeted therapy.3,4 With appropriate treatment, the 5 year relative survival rate approximated 93% between 2013–2017, based on the Korea Central Cancer Registry data. 5
Despite advances in medical treatment and increased survival rates, 6 breast cancer is considered to be a chronic disease, 7 and postoperative breast cancer patients experience various problems, affecting their health-related quality of life.8,9 They endure side effects (i.e., pain, nausea, vomiting, and lymphedema) post-surgery and during treatment,10,11 leading to healthcare burdens long after the completion of treatment. 12 From the perspective of healthcare, self-management becomes crucial and promotes participation in health care activities. 13 Moreover, breast cancer patients prefer managing their own health and supportive care from health professionals. They eventually need long-term self-management support which reflects individual needs.14–17
In an increasing population of breast cancer patients with different supportive care needs, mobile applications can be useful and widely available for patients with post-operative breast cancer, without restrictions of time and space. 18 While the majority of mobile applications for patients with breast cancer have dealt with contents for raising awareness, prevention, early detection, and care management,19,20 few have addressed the personalized self-management needs of breast cancer patients, especially from the time of surgery, during primary treatment, and in the post-primary treatment phase. Mobile applications for self-management can provide resources and functionality suitable for patients and caregivers, such as monitoring and tracking symptoms, motivation for self-management and receiving educational information for medication, exercise, and diet, as well as interaction or sharing information with peer survivors. 18 Kapoor, Nambisan 18 found that out of 423 mobile applications of self-management for breast cancer survivors, only nine met the criteria for content analysis based on the chronic care model, and highlighted the importance of comprehensive resources to meet the users’ needs.
In recent years, mobile health (mHealth)-based self-management for breast cancer patients has proved promising and can provide continued care personalized as per the patient’s needs.18,21 Thus, such services have been delivered via mobile application (app) developed to cater to individual care needs.22–24 A meta-analysis verified the significant effects of mHealth-based self-management intervention on self-management behavior, functional exercise compliance, self-efficacy, health-related quality of life, incidence of lymphedema, and anxiety. 21 The intervention duration in this meta-analysis was mostly three to 6 months, and it has paid little attention to provide a mHealth app with Internet of Things devices, including comprehensive medical/behavioral management in the long-term. Given the long-term needs of individualized self-management and the efficacy of mHealth interventions, it is necessary to investigate the feasibility and usability of such interventions after surgery.
Therefore, our team developed a comprehensive mobile app (called Breast Cancer by Second Doctor). 25 To the best of our knowledge, there is no comprehensive mobile app developed specifically for providing personalized content based on the classification of user information for self-management after surgery. The goal was to support integrated and long-term self-management immediately after surgery and throughout the treatment process. This app was built to classify user information for personalized rehabilitation according to five key criteria: general user information, breast operation type, lymph node surgery type, chemotherapy and hormonal therapy, and change in treatment after surgery. Additionally, it could connect to a smart band, such as one worn on the wrist, which then acts as a step counter and tracks heart rate and sleep.
This study’s primary objective was to examine the prospective longitudinal feasibility and usability of personalized care services using the initial app version with the main self-management components. Exploratory aims included assessing the potential barriers to its implementation identified through patient suggestions/feedback. Our findings can help decide the subsequent direction of app development and strategize randomized clinical trials involving a larger study population. 26
Materials and Methods
Study participants and experimental design
This single-arm study was conducted in a single-center of South Korea between April 2019 and February 2021. After consultation with the division of breast surgery and the department of rehabilitation medicine, patients who were to be discharged from the hospital after surgery were invited to participate in the study. All eligible patients were informed of study procedures on the day of discharge.
The selection criteria were as follows: patients who were in the immediate postoperative period and before chemotherapy, radiotherapy, or hormonal therapy; had their unilateral breast cancer (stage 0–III) treated surgically, were aged 20–70 years, and were smartphone users (iOS and Android). Patients who only underwent surgery, had no plans of receiving therapy, and had metastases or recurrence in other organs were excluded.
This study applied a longitudinal prospective design, with participants using a personalized mHealth app (Breast Cancer by Second Doctor, Medi Plus Solution, Seoul, South Korea) for 12 months. Each participant received a code to enter into the app after surgery and entered their personal health data while signing up. The healthcare professionals provided a tutorial for the app and demonstrated its contents. As soon as the treatment was determined, the participants entered their treatment information to personalize the app contents. The participants used the app and wore a DoFit device (NF-B20, Medi Plus Solution, Seoul, South Korea) immediately after discharge post-surgery.
The following data were collected: need for and satisfaction with each app domain at 1, 2, 4, 6, 9, and 12 months post-surgery; satisfaction with and usefulness of services offered by the app at 12 months; and analysis of access rate, number of content views, and usage for each app domain using a smart band for 1 year (i.e., recording exercise, physical activity, and diet).
Participants were instructed to always wear the DoFit or as frequently possible, even during physical activity and sleep. They were assisted over phone calls or texts for a minimum of 1 month after enrollment to accustom them to the app and wearing and syncing its data with the DoFit. Thereafter, there were no regular reminders. However, if no data were reported for 4 weeks on the monitoring platform, healthcare professionals enquired into the reason behind this and helped resolve any issues with the app or DoFit.
Study app
To develop Breast Cancer by Second Doctors, the research team included a breast surgeon, two physical and rehabilitation medicine physicians, two physical therapists, two exercise experts, and two nutritionists. The development team (two professional developers and two service planners) had experience in developing an mHealth app for chronic disease management; pregnancy; and patients with stomach, colon, and prostate cancers. The app design team included two designers with extensive expertise in designing applications for cancer patients. 11 domains and evidence-based contents were determined by a consensus of all experts. Of these, eight main features of the app included personalized health information and education on exercise, nutrition, and disease according to surgery, treatment type, side effects, and comorbidities; personalized exercise management after surgery; physical activity management; diet management for breast cancer patients; sleep management; comorbidity management (weight, blood pressure, blood glucose); medication and smoking management; and expert consultation. To provide personalized content, the following information was included in the algorithm: breast surgery type, lymph node surgery type, surgery date, hospital discharge date, and current treatment (e.g., chemotherapy, radiation therapy, and hormonal therapy). General user information was also included, such as the name or nickname, sex, birth date, height, weight, chronic diseases (e.g., hypertension, diabetes, and hyperlipidemia), current food intake (e.g., vegetables, fruit, fish, meat, and rice), and smoking habits. This app was developed to be compatible with both Android and iOS devices and for easy transfer of data via Bluetooth-enabled wearable smart devices like smart bands, blood pressure gauge, glucose monitors, and scales. Healthcare professionals could use a web-based open architecture management for easier tractability and monitoring of the app usage patterns. The detailed descriptions of app development and service flow have been indicated in a prior work. 25
Feasibility
Retention rate
The feasibility of the app during the 12 month period was assessed by evaluating the participants’ finding access rate. The individual access rate was calculated by the number of days of accessing the app divided by the number of intervention days (360 days), and this was expressed as a percentage.
Patterns of app use
To explore changes in the app usage pattern across treatment courses and based on participant interest, we examined the number of content views in the five domains (tailored information and education, exercise management, diet management, physical activity management, sleep management) during the year. The total number of content views of the 18 participants who completed the study was collected at each time interval (0–1, >1 to ≤2, >2 to ≤4, >4 to ≤6, >6 to ≤9, and >9 to ≤12 months post-surgery). The proportion of views of each domain relative to total number of content views at each time was calculated. Additionally, the usage pattern of “exercise management”, “physical activity management”, and “diet management” were examined as key domains.
Usability
We reconstructed the questionnaire previously developed by the authors of this study to observe the long-term changes after surgery regarding individuals’ need, satisfaction with key domains, and the app at each postoperative time point to prove users’ satisfaction and usefulness of this app service at the end of the 12 months test period. 27 To update the contents to be more personalized after the end of the study, we asked the reasons behind not needing this service or dissatisfaction with it indicated by the participants.
Need and satisfaction for key domains and app
To identify an individual’s perceived need for each domain and how it changes over time, participants were asked to indicate one of five responses regardless of whether they used each domain on a questionnaire. They also indicated the level of satisfaction with the following key domains: tailored information and education (for disease, exercise, and diet management), information on side effects and medical precautions according to treatment timing and type, exercise management, diet management, and sleep management. Additionally, level of necessity and satisfaction with the overall app was evaluated.
This questionnaire was administered at 1, 2, 4, 6, 9, and 12 months after surgery. It included two questions on each domain and five response options: “How much did you need each domain/app?” ((1 = never feel the need to use, 2 = feel no need to use, 3 = neutral, 4 = feel need to use, and 5 = feel a high need to use), and “How satisfied are you with each domain/app?” (1 = very dissatisfied, 2 = dissatisfied, 3 = neutral, 4 = satisfied, 5 = very satisfied). When a participant responded with feel no need to use or never feel the need to use/dissatisfied or very much dissatisfied, the researchers asked for reasons and suggestions. In addition to measuring the level of need and satisfaction, we asked participants to prioritize each domain from one to five for investigating individual needs and satisfaction.
Satisfaction and usefulness of app service
The questionnaire on satisfaction and usefulness of the app included a mix of closed and open questions. Participants filled it in at 12 months after surgery. It comprised a 14-item usability scale, identifying which items received a positive response, scored on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). The scores for the 14 items were converted to a total of 100 points. We replaced “smart aftercare service” with “breast cancer by second doctor” for each question. If participants answered with strongly agree, agree, or neutral to the question on intention to pay for the app and the willingness to recommend it to others, the questionnaire had room for participants to cite multiple responses along with their reasoning. Additionally, they answered a 15th item, which was regarding when this service was most helpful. For this too, the participants could provide multiple responses. We also considered technical challenges, such as hardware (smart band), app, network, and inexperienced user operation.
Statistical analysis
Descriptive statistical analysis was used for the need and satisfaction survey scores for each domain, content views, and the total usability score. To analyze the ranked multi-responses, a frequency analysis for each rank was performed using SPSS version 18.0 (SPSS Inc. Chicago, IL, USA). In the need and satisfaction ranking survey, a weighted value was assigned from the first (500%) to the fifth rank (100%), in the order of importance. The final rank for each domain in the need and satisfaction questionnaire was determined according to the sum of the weight values.
With the expectation of content views, the pattern of app usage was analyzed in terms of physical activity management (step count/day) and diet management, recorded by calculating individual patient-level reporting rate. 28 This calculated by the total number of days self-management divided by the total number of follow-up days of each participant. In exercise management, the exercise frequency (times/week) of each participant was computed, and the median frequency was reported for compliance rate because the distribution of exercise usage was not normally distributed. The compliance rate with the volume of any exercise (aerobic exercise, arm and shoulder exercise, and exercise diary) was calculated by the number of exercises performed divided by the prescribed number of exercise sessions (five times weekly). 29 Lastly, the number and ratio (%) of participants who exercised more than five times weekly, regardless of session time and exercise type, were calculated.
Results
Participants
Characteristics of the study participants (N = 18).
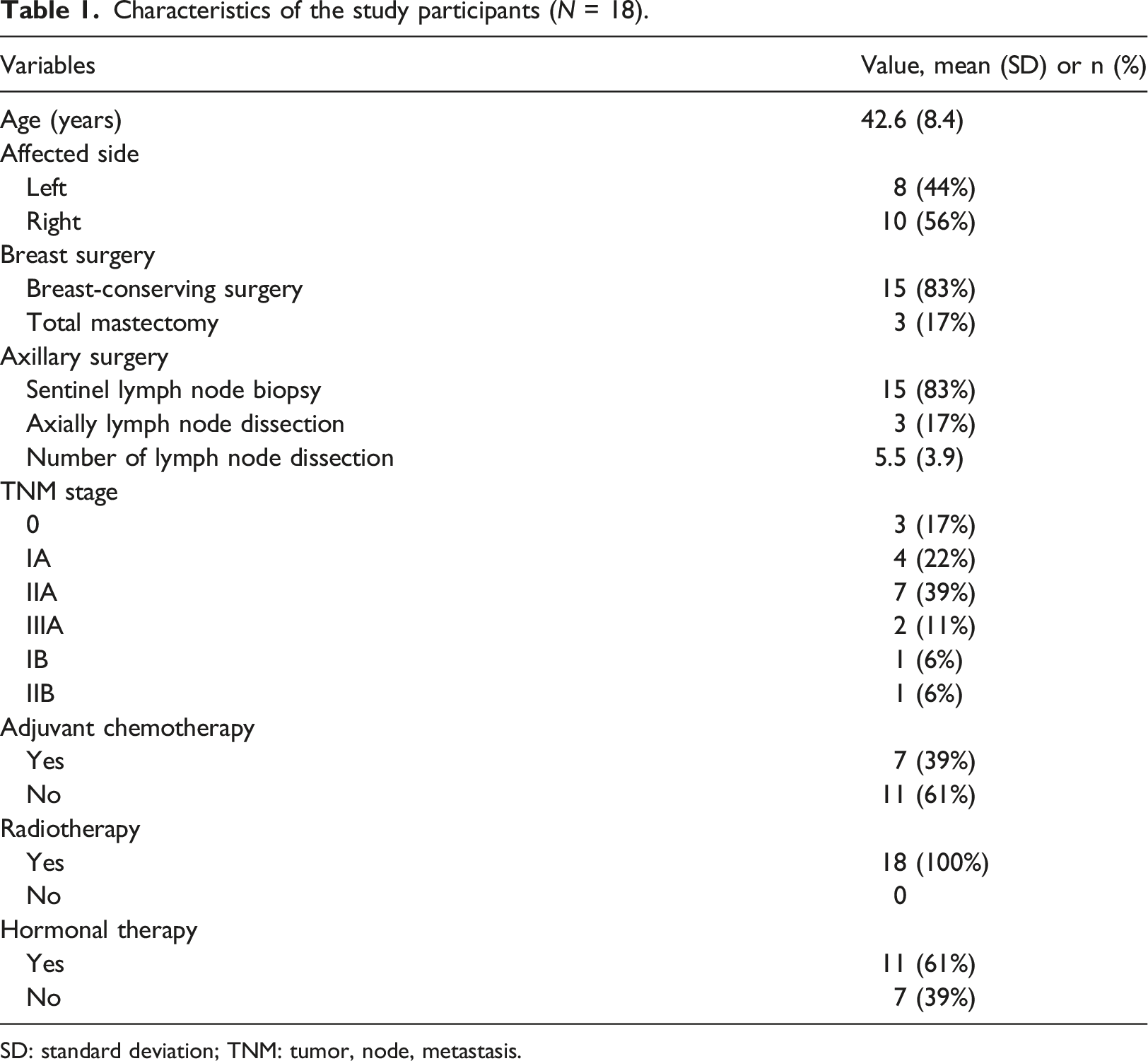
SD: standard deviation; TNM: tumor, node, metastasis.
Feasibility assessment
Retention rate
The individual finding access rate of the app was evaluated during the intervention period (360 days). Mean retention rate was 75.8% (standard deviation [SD] 19.9%, range 41.7%–100%) and median retention rate was 78.8% for the entire 12-month period.
Patterns of app use
The total number of views at 2 months after surgery dropped to half compared to 1 month after surgery, and since then, the number of views remained steady. The total number of content views during 0–12 months post-surgery was 35,930 and at each time interval as follows: 0–1 month, 6,209; >1 to ≤2 months, 3,684; >2 to ≤4 months, 6,278; >4 to ≤6 months, 5,831; >6 to ≤9 months, 7,490; and >9 to ≤12 months, 6,438. Exercise management (12,076 times) and diet management (13,712 times) were the most frequently accessed domains after surgery. Regarding the viewing rate of contents over time (Figure 1), participants accessed exercise management at a constant rate (range 30.3–37.9), and views for diet management gradually increased. During the initial 6 months, physical activity management was frequently accessed, and tailored information and education, and sleep management views gradually decreased. Proportion of content views of each domain to total views at each time interval.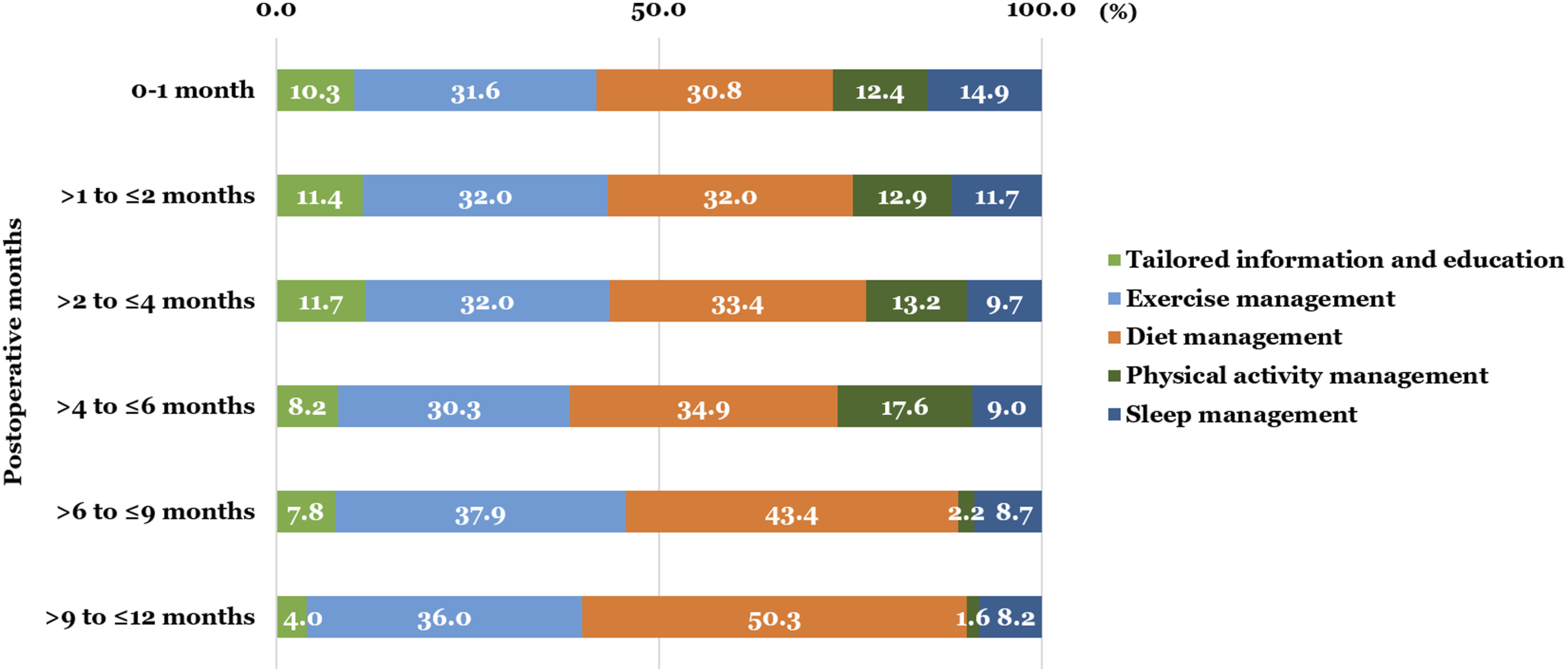
In exercise management, the total number of exercise sessions recorded was 4,700, with “aerobic exercise with smart band” (2,250) having the highest frequency, followed by “arm and shoulder exercises” (1,766), and “exercise diary” (684). At 1 year, the median number of exercise sessions per week was 3.3 times, and this decreased to 2 times/week over time (Figure 2(a)). High compliance with exercise was found at a median of 60% at 1 year. 30 days after surgery (before primary treatment), the proportion of participants exercising more than five times weekly accounted for 83% (15/18), but it decreased by about half as soon as they started treatment, and it decreased to less than 50% after 5 months of starting treatment. (A) Median number of sessions of exercise performed per week and (B) Median number of steps per day per week.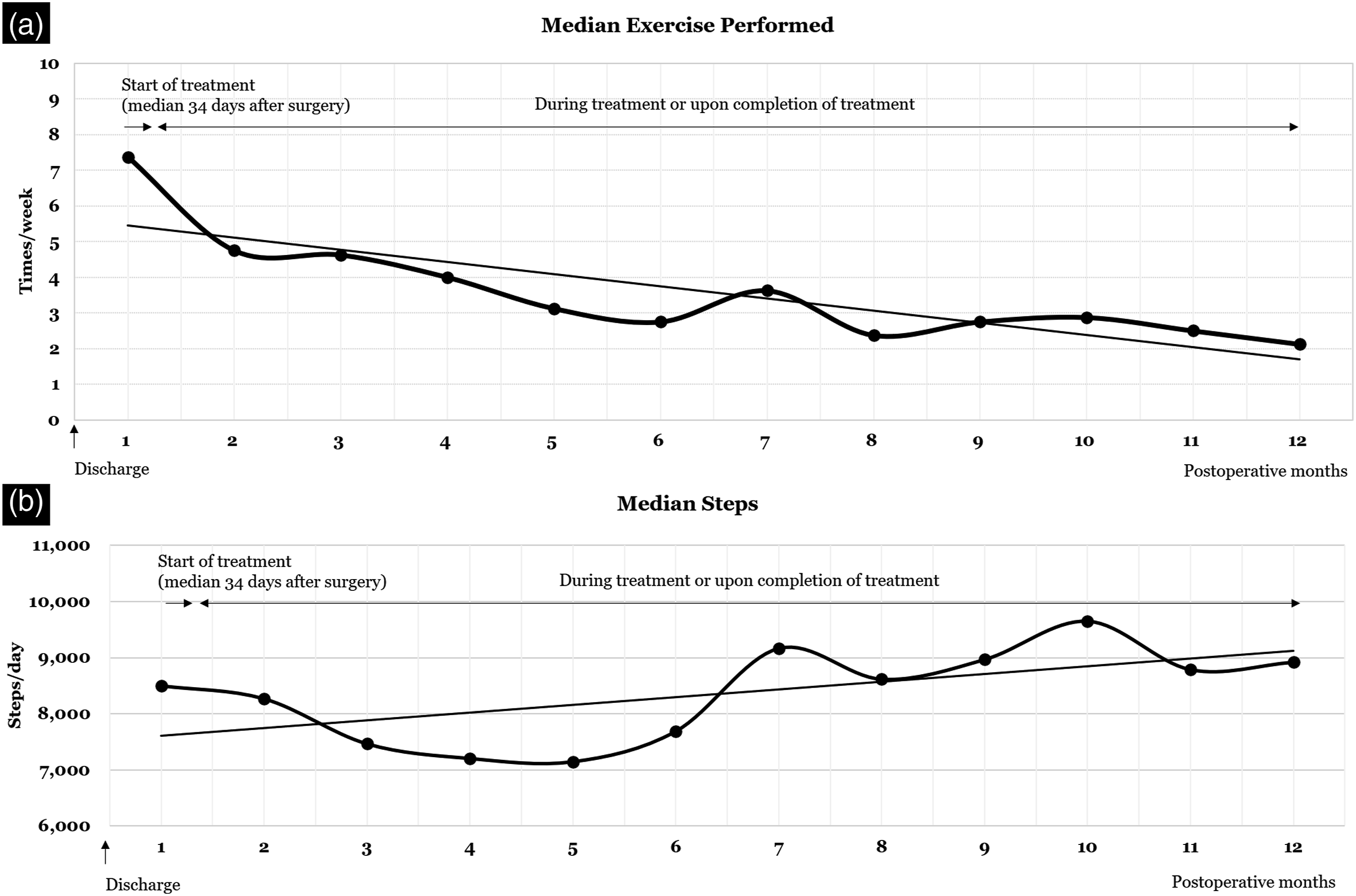
In diet management, the total number of recordings was 2,366. The patient-level individual reporting rate was 12.3%. The reporting rate of 10 participants (52.6%) was less than 20%, indicating that they did not use this domain after surgery or during treatment. The number of participants at 21–40%, 61–80%, and 81–100% were 2, 1, and 5, respectively, indicating few participants who consistently used this function, regardless of their treatment course.
In physical activity management, 18 participants wore and synced their smart band to the app to collect physical activity data during the follow-up period. Most participants used smart bands well despite technical challenges and undergoing treatment. The median individual patient-level reporting rate of 18 participants was 95.8%. 16 participants (89%) had an individual reporting rate of more than 81%. The reporting rates of two participants (11%) were 42.6% and 77.2%, respectively. Before primary treatment, the median step count/day was 8,500, and after the initiation of treatment, it gradually decreased to about 7,000/day. Six months after surgery, the step count recovered to more than 9,000, and 8,000–9,000 steps were maintained thereafter (Figure 2(b)).
Usability assessment
Need and satisfaction for main domains and app
Mean score in needs and satisfaction over time.
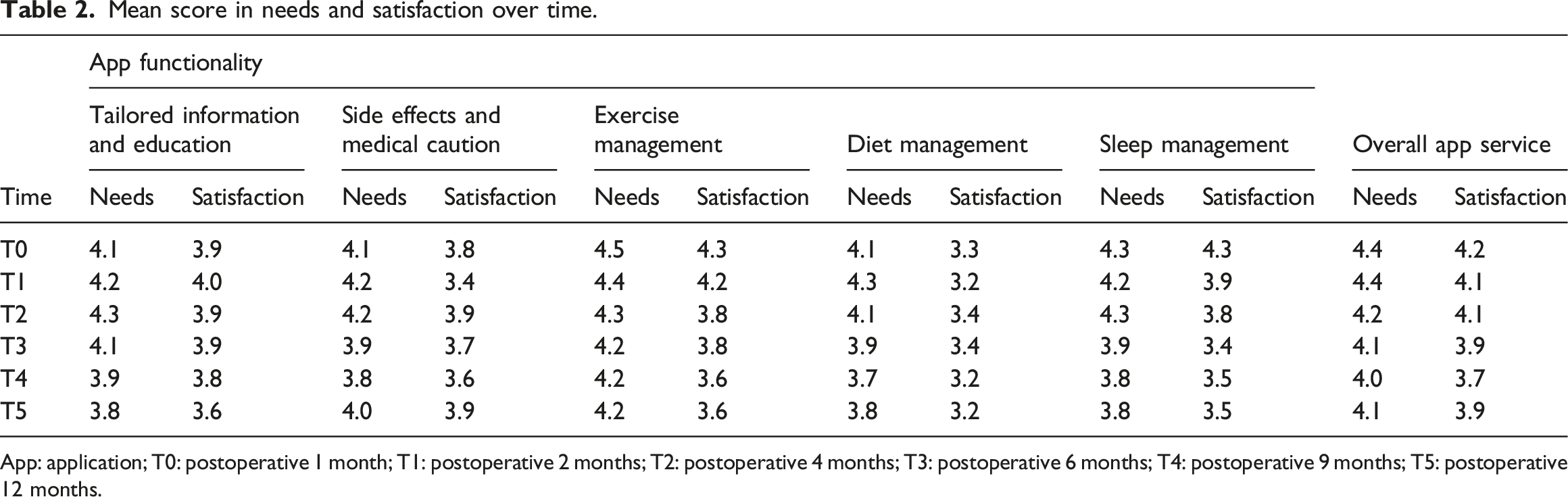
App: application; T0: postoperative 1 month; T1: postoperative 2 months; T2: postoperative 4 months; T3: postoperative 6 months; T4: postoperative 9 months; T5: postoperative 12 months.
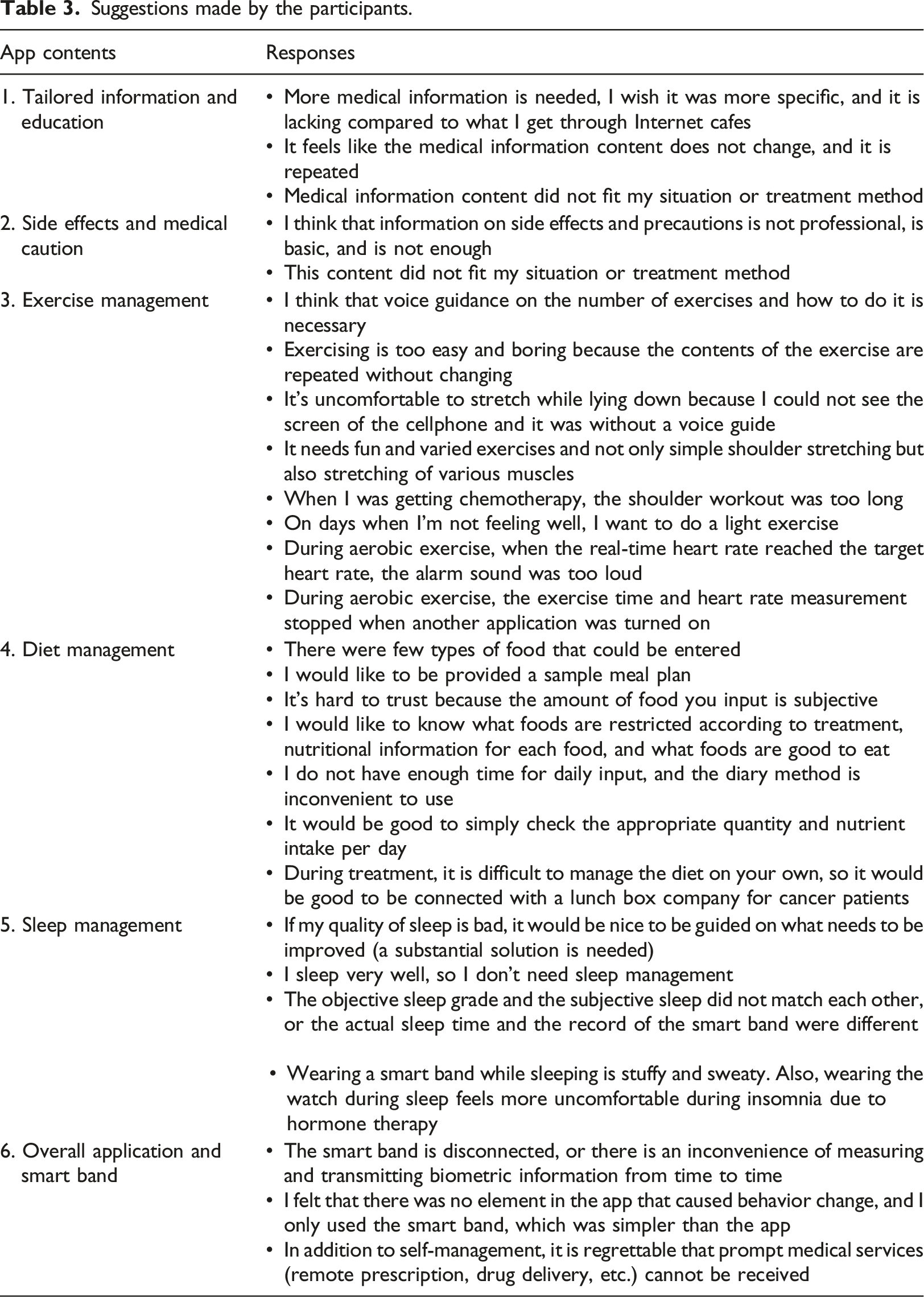
Suggestions made by the participants.
Satisfaction and usefulness in app service
Usability score results, as rated by participants.
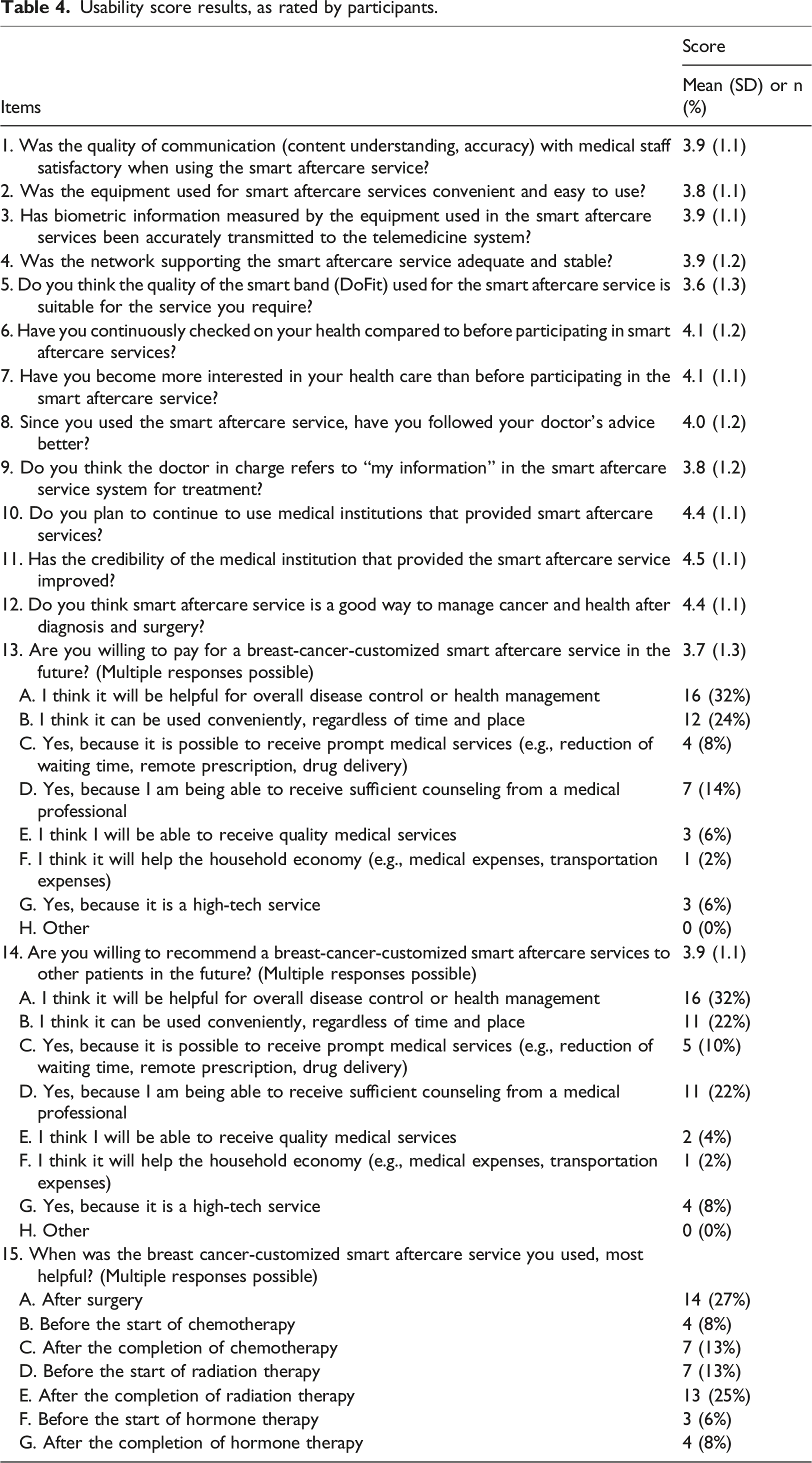
All participants agreed or strongly agreed that this app service was suitable for health management after surgery. There was high agreement in that 94% (17/18) of participants became more interested in their health care, and 89% (16/18) checked their health status more frequently than before participating in the study. Additionally, 94% (17/18) of the participants were willing to use this app service for a fee. Their main reasons were that it could be used conveniently regardless of time and place (12/18) and to manage the overall disease or health (16/18). 17 participants were willing to recommend it to others because they had received sufficient counseling from healthcare providers; a similar reason was provided for item 13 (11/18). Results showed that 83% (15/18) of participants thought that the use of an app with a smart band was most helpful after surgery, and 78% (14/18) found it most helpful after radiotherapy. Additionally, seven out of eight participants who underwent chemotherapy found it most helpful after receiving chemotherapy compared to pre-treatment. There were several technical challenges (78%, 14/18), such as broken or malfunctioning smart bands (8/18), app errors (2/18) or network errors (5/18), and inexperienced user operations (3/18).
Discussion
This study investigated whether a personalized mHealth app with a smart band, which provides comprehensive and tailored content, can be used by breast cancer patients undergoing different types of treatment during the 12-month period post-surgery. It proved feasible and useable, as demonstrated by good level of access rate with intervention (mean 75.8%) and usability score (mean 80.2). Although there were some technical barriers to using the app and smart band, most participants indicated their willingness to recommend it to other patients and pay for it.
During the intervention period, the participants’ access rate (mean 75.8%) demonstrated its feasibility for long-term health management following surgery. Our findings are similar to other studies reporting the same outcomes. For example, in a feasibility and randomized controlled trial of 150 healthy Korean adults in their 30s and 40s that implemented a 12-weeks mHealth app intervention based on the user’s subhealth status for use in everyday life, the user finding access rate of the app was 75.1% (SD 15.9%, range 22–100%), which reflected a good engagement for the entire 3-month period. 30 The definition of retention (interchangeably used to adherence, compliance, completion, engagement) in our study does not align with previous studies providing mHealth intervention during 1 year. These studies,31,32 which showed the retention to be 80–90%, indicated the rate of participants who completed the study or the intervention. In the current study, we presented the retention rate based on opening/logging into the app, as reported in the systematic literature review. 33 Therefore, comparing retention rates may be partially limited. Given the previous findings, our study demonstrated good level of engagement with the personalized app in early- and late-middle-aged patients with breast cancer. This indicates that the integrated mHealth app service is acceptable among patients following breast cancer surgery due to the needs of individual long-term care.
Our study evaluated satisfaction and usefulness in comprehensive app service among the aspects of usability (easy to use and satisfaction, system information arrangement, and usefulness). 34 Our findings of usability are consistent with other studies evaluating usability of mHealth apps for postoperative care of patients with breast cancer using quantitative measures or/and interviews. In a study that carried out preliminary testing, four breast cancer patients who used the app for 8 weeks post-surgery indicated 4.6/5 rating (Likert scale) with an mHealth app for upper-limb dysfunction and symptom mentoring for prompting self-management. 35 During 30 days following surgery, using mHealth app for monitoring of postoperative quality of recovery at home, 31 breast cancer patients rated overall high satisfaction (mean 3.9/4.0) on a scale from 1 (poor) to 4 (excellent), and all of them were willing to use this app in the postoperative period. In another feasibility study, which conducted a 2-month intervention using a mobile app with an activity tracker and telephone coaching survivorship care planning program for breast cancer survivors, 81% (17/21) of participants rated the overall quality of the app as at least “good,” 71% (15/21) rated it as “easy to use,” and all of them reported the app-based intervention as “quite or very useful.” 36 These findings are comparable with our findings wherein 17 of 18 participants (97%) were willing to use this app service for a fee and recommend it. Other mHealth apps for self-management support of breast cancer patients including similar functions as our app showed good usability and acceptability, but they did not directly report the score of usability.37,38
Our findings suggest that the most important function among the domains in postoperative breast cancer patients was personalized exercise; information related to treatment and health was also prioritized. The most-viewed domains were exercise and diet management. These findings are supported by previous studies. Secondary analysis revealed that when 80 Latina breast cancer survivors used the smartphone-based health management for 6 weeks, their greatest concerns were exercise and nutrition. 39 A study investigated unmet self-management needs of patients with breast cancer and showed that the highest proportion (14.2%) accounted for “exercising more” among self-management items. 40 In another study 41 that examined the unmet needs of 332 Korean breast cancer survivors using the Comprehensive Needs Assessment Tool, “information and education,” such as correct diet was the highest unmet need among domains and accounted for 80% of the top 10 unmet needs. However, ranking and score of satisfaction with diet management was lower than all needs. Presumably, the participants might be less satisfied because there were few types of food to be able to enter into the app at the beginning of the intervention. They who are in the work force or caring for children said that there is no time to enter food logs, and some participants found it hard to believe in the nutrient ratio due to subjective input. Considering the challenge of satisfying everyone’s situation, we should provide simpler and more practical services, for example, educating about food to eat or avoid according to treatment type.
Our participants made some suggestions for improvement in the future. Some felt that the contents were not personalized and lacked in terms of tailored information and education, and side effects and medical caution. Previous studies reported that the younger patients were more likely to report needing help with self-management, and Asian women need more information compared to Western women.16,40 Also, participants in this study who were relatively young Korean breast cancer patients may have higher expectations for self-management using mHealth care. In exercise management, the participants suggested adding voice guidance to describe the exercises, adding a wide range of exercises, and having the ability to customize the exercise program based on their condition. Unexpectedly, there were a range of suggestions for further improvement of the diet management contents, such as providing services like sample meals or lunch boxes for patients who have difficulty managing their diet and more convenient and accurate ways to input the intake, for instance, by taking pictures of the food. The main issues with sleep management included discrepancies between the sleep quality measured by the smart band and what the patient reported and discomfort in wearing a smart band while sleeping due to stuffiness, sweat, or insomnia caused by hormonal therapy. Moreover, they needed information or education about things that they could do to improve the sleep quality. Addressing participants’ suggestions for each domain could help improve and personalize self-management based on mHealth interventions further. Although we did not examine the influence of factors (e.g., age, gender, and intention to use) on usability and app usage, this longitudinal research concentrating on patients post-surgery along the trajectory of breast cancer will enable a dynamic understanding of patient needs and steps that need to be taken to develop an improved app.
The results from this study should be generalized with caution. First, the sample size was small and comprised relatively young participants (30–50 years) with mild to moderate disease severity and fewer lymph node dissections (less than 10). Future clinical trials should include older patients, those in advanced stages of cancer, and those undergoing total mastectomy or axillary lymph node resection and closely examine their needs. Second, due to the heterogeneous treatment type and low number of participants, the usage of mHealth app with smart band tended to vary. Moreover, the potential causative factors affecting longitudinal app usage and the correlation between app use and these factors were not investigated. To explore this relationship clearly, future research should be based on the theory used to understand patients’ behavior of using technology-assisted systems for health management. 42 Third, we used non-standardized usability questionnaires to measure the app specific- and longitudinal usability, such as needs and satisfaction in the main function as well as satisfaction and usefulness within the dimension of usability. Therefore, it is hard to compare the previous findings yielded from the use of validated questionnaires, such as the System Usability Score, user version of the Mobile Application Rating Scale, and the Computer System Usability Questionnaire. We thus recommend using objective and validated questionnaires in randomized controlled trials with a larger and more diverse sample.
Conclusion
This study confirmed the feasibility and usability of the personalized mHealth app intervention for long-term support and self-management in the 12 months following breast cancer surgery. Our findings are practical and noteworthy from the longitudinal perspective and use a novel self-management tool after breast cancer surgery. These can be used in trial designs to consider the duration of intervention, determine the timing of a reminder if needed, and provide targeted solutions based on perceived usefulness about self-management component changes over time. There is also a need to develop the reasonable alternative by considering patients’ suggestions and inconveniences in terms of using the app or smart band.
Footnotes
Authors’ contributions
JYL wrote the manuscript with support from JHH and performed user evaluation and data analysis. All authors were involved in the implementation of the study and interpreted the results. JHH, JHY, and YK designed the project and developed a theoretical framework for the study. All authors discussed the results and commented on the manuscript. JHH directed and supervised the project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea [grant number NRF-2017R1A2B4010795] and Medi Plus Solution [PHO0201191].
Ethics
The Institutional Review Board (approval number 2018–10-062) of Samsung Medical Center approved this study. All patients participated voluntarily and provided written informed consent before enrollment.