
Abstract
Background
Malaria contributes 20% of outpatient cases in health facilities in Uganda. Data also show that there is a severe shortage of skilled health care personnel in sub-Saharan Africa. Electronic Medical Record (EMR) systems have been shown to provide benefits to health care providers and patients alike, making them important for low resourced settings.
Methods
A comparative study was performed from March 2018 to March 2019 in which an integrated EMR system was implemented with treatment guidelines for malaria, and its effect was evaluated on malaria outpatient case management in one Ugandan health facility. Another health facility was used as a control site.
Results
Malaria outpatient visits were 1.3 h shorter in the EMR group (p < .0001), and 80% more participants in the EMR group had age and weight information available to clinicians at the point of prescribing (p < .0001). Fewer participants in the EMR group had recurring malaria with no statistical significance (p = .097). Malaria surveillance reporting was significantly more accurate at the EMR intervention site (p < .05).
Conclusion
The EMR system probably improved malaria outpatient case management by reducing outpatient visit durations, improving the availability of patient age and weight information to inform prescribing and improving the accuracy of malaria surveillance reporting.
Introduction
The African region has the highest burden of malaria globally. According to the World Malaria Report 2020, the region contributed 94% of global malaria cases in 2019, with approximately 215 million cases. 1 Half of these cases were from 5 countries in Africa, namely Nigeria with 25%, the Democratic Republic of the Congo with 12%, Uganda with 5%, Mozambique with 4% and Niger with 3%. Approximately 51% of all malaria deaths globally in 2019 were also from 6 countries in Africa. These were Nigeria (23%), the Democratic Republic of the Congo (11%), Tanzania (5%), Mozambique (4%), Niger (4%) and Burkina Faso (4%). 1
Malaria is known to be caused by 5 species of parasites of the genus plasmodium that affect humans. The most deadly of these, plasmodium falciparum, is predominantly found in Africa. 2 Prompt diagnosis and treatment of malaria can cure a patient, preventing the development of severe malaria and reduces the length of time that patients carry malaria parasites in their blood, which in turn reduces the risk of onward transmission. The World Health Organization recommends that every suspected malaria case be confirmed by microscopy or a rapid diagnostic test before treatment.
In Uganda, malaria is endemic throughout the country, with active transmission in 99% of the country. All people in Uganda are at risk of contracting malaria, especially children under 5 years of age and pregnant women are the most vulnerable. 3 Malaria accounts for 20% of outpatient cases in health facilities and for 5% of the total deaths reported at health facilities across the country. Uganda has implemented the test and treat policy which aims to treat all individuals suspected of having malaria only after a parasitological test has confirmed the diagnosis. However, approximately 32% of treated malaria cases are still based on clinical diagnosis. In addition, malaria has an indirect impact on the country’s economy due to loss of workdays because of sickness, decreased productivity and decreased school attendance. 4 The socio-economic impact of malaria on the Ugandan population includes personal expenditure on consultation fees, drugs, transport and subsistence at a distant health facility. A single episode of malaria costs a family on average 9 US dollars, or 3% of their annual income. This has substantial financial consequences on families especially poor families in malaria-endemic areas. The agricultural sector and industries also suffer due to loss of labour hours and decreased worker productivity. 4
In addition, there is a severe shortage of skilled health care personnel in sub-Saharan Africa with the region having a very low density of qualified doctors per population, with most countries in the region having a range of 0 – 5 physicians per 10,000 people. 5 Lower level cadres such as nurses, midwives and community health workers account for the biggest proportion of the health workforce. The region has a shortage of health workers which has been amplified by the continued migration of skilled health professionals. 6
Electronic medical record (EMR) systems have been shown to provide benefits to health care providers and patients alike, but little evidence is documented of their use in the clinical management of malaria cases. Hardly any documentation exists on the integration of national standard treatment guidelines for malaria into electronic medical record systems to provide clinician support for the management of malaria cases. For instance, a search of PubMed using the MeSH terms (“Electronic Health Records” OR “electronic Medical Records”) AND Malaria returned only 13 results with just one paper documenting the use of an EMR system in the clinical management of malaria. A search of Google Scholar for integration of standard treatment guidelines for malaria into an EMR system also did not return any papers. While this does not imply that no work has been done in this regard, it highlights the need for more evidence on the effect that EMR systems can have on the management of malaria, which is endemic in many sub-Saharan African countries with low resourced health care systems that need the potential benefits therein.
Electronic medical record systems have proven useful in ensuring the assessment of patients according to clinical practice guidelines leading to improvements in quality of care measures, 7 and computerised clinical practice guidelines have yielded improvements in patient care. 8 Electronic medical record systems have also been beneficial in providing decision support to care providers, 9 and clinician decision support functionality has reduced data errors, patient missed appointments and patient waiting times. 10 Electronic medical record systems can also help to avert medical errors, 11 overcome challenges in medical records management and back-office hospital administrative functions 12 and ensure that patients who are eligible for care receive it early. 13 They have been shown to improve clinician workflow efficiency and patient load handling, 14 improve the completeness of clinical records, 15 improve provider regulatory compliance 16 as well as enable efficient reporting to the government. 17 In addition, clinical case surveillance for malaria has been noted to be important for malaria control, 18 and strong malaria surveillance systems help in the elimination of malaria. 19
Despite these benefits, EMR systems have also been shown to account for a proportion of patient safety incidents in hospitals 20 and to contribute to clinician mental overload through inappropriate alerts. 21 The need to validate the outputs of electronic medical record systems in clinical practice has also been noted to be important to ensure the accuracy of the outputs that they produce. 22 This highlights the need for careful design and configuration when implementing EMR systems to ensure that they appropriately cater for the varying requirements of patients and providers.
Aim of the study
The aim of the study was to assess the effect of an integrated electronic medical record system incorporated with standard treatment guidelines for malaria on malaria outpatient case management in a low resourced health care setting in Uganda with limited medical personnel.
Methods
A comparative pilot study with an intervention and control arm was performed in which an integrated electronic medical record system with standard treatment guidelines for malaria was implemented in a low resourced health care setting in Uganda, and its effect evaluated on malaria outpatient case management over a 12 month period.
System selection and customisation
A set of functional requirements was developed for the system, which included capabilities for patient registration, vital signs and history data capture, laboratory results integration, prescription and dispensing of medicines functionality, as well as the ability of the system to incorporate treatment guidelines for malaria. Medicines’ inventory management functionality requirements for the system included the capability to define medicine and health supplies in a product catalogue, ordering and receipt of products from suppliers, requisitioning and issuing of medicines and health supplies from a storage location to user units, as well as linking of dispensing of medicines to requisitioned stock. Technical requirements for the system included the ability for the system to run in a networked environment, availability of enhanced security features within the system, segregation of roles for users in the system, the robustness of the database platform on which the system is implemented, plus the ability to customise reports in the system.
The usability requirements of the system were also considered taking into account the submission from the Healthcare Information and Management Systems Society that usability is one of the most important factors hindering widespread adoption of electronic medical record systems. 23 Particular emphasis was put on system ease of use as this had been identified to possibly have the most positive influence on EMR system usability. 24 A number of existing open source and proprietary electronic medical record systems were assessed on the specified system requirements, and 2 systems were identified for potential use in the study. These were OpenMRS integrated with OpenHMIS, and RxSolution integrated pharmaceutical management system. RxSolution was selected for use in the study as it met all the technical and functional requirements highlighted earlier and particularly for its in-built comprehensive medicines’ inventory management functionality and capability to incorporate treatment guidelines that could be availed to clinicians at the point of prescribing.
The system was set up in a networked client-server environment within a rural health facility with a server workstation and computers at various clinician points within the health facility linked through a local area network. The server was set up in the medicines store, and computers were set up in the laboratory, outpatient clinicians’ examination room and the health centre’s outpatient dispensing point. Uganda’s 2016 clinical guidelines
25
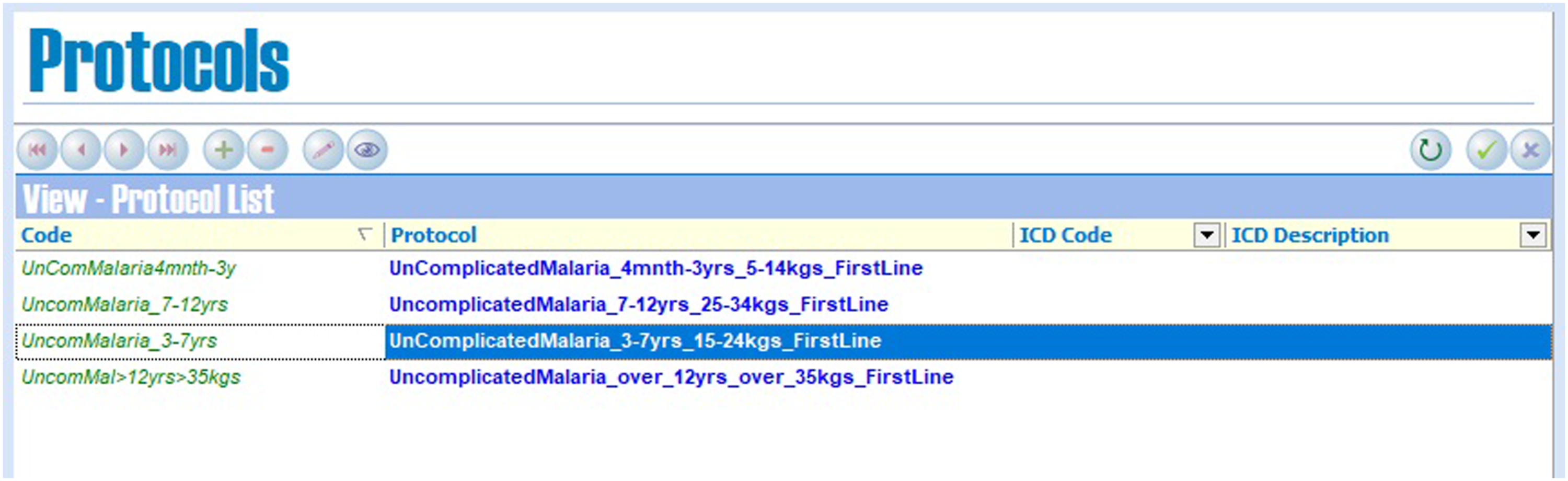
for the management of malaria cases were incorporated into the RxSolution software, which was deployed for use by clinicians at the mentioned points of care. Figure 1 and Figure 2 below show the setup of guidelines for the treatment of uncomplicated malaria within the RxSolution system. Uncomplicated malaria treatment regimens setup in the RxSolution system to inform anti-malarial medicines prescribing by clinicians. Uncomplicated malaria treatment protocols setup in the RxSolution system from the standard treatment guidelines to inform appropriate dosing for different patient age and weight categories.
Study site selection
In the comparative pilot study, the integrated EMR system was implemented in one health facility in rural Uganda and the malaria outpatient case management outcomes at this facility were compared with those from another health facility at the same level of care used as a control site. The study site selection criteria included the following: that the facilities were located outside Uganda’s capital city; were lower level public health facilities that are not hospitals; provided diagnostic and treatment services for malaria including laboratory, clinical and pharmaceutical services; and had a demonstrated lack of staffing of doctors.
The study intervention site where the EMR system was implemented was Buwambo Health Centre IV, a public health facility in Wakiso district in Uganda, while Kajjansi HCIV, another public health facility also in Wakiso district, served as the study control site. Health Centre (HC) IV public facilities in Uganda provide preventive, promotive, outpatient curative, maternity, general inpatient, emergency surgery, blood transfusion and laboratory services. Wakiso district is the second most populated district in Uganda with a population of about 2,007,700 and covers a total area of 2807.75 square kilometres. The district is sub-divided into eight administrative units called constituencies. Buwambo HC IV is located in a constituency with a total population of approximately 368,694 people (47% male, 53% female), while Kajjansi HCIV is located in a constituency with a total population of approximately 244,309 people (48% male, 52% female). 26
Buwambo is a primarily rural farming community while Kajjansi is a mix of farming and semi-urban small scale trading communities. Buwambo Health Centre IV was chosen for its rural setting and fairly close proximity to Uganda’s capital city, Kampala. The facility is located approximately 30 km from the capital city. During the study period, 2 clinical officers, 2 nurses, 1 dispenser, 1 nursing assistant and 2 laboratory assistants manned its outpatient department. A medical officer who doubled as the facility in-charge provided only administrative oversight of the department, and a records assistant for the facility provided records management oversight.
Kajjansi Health Centre IV, a similar level health facility in a semi-urban setting also in Wakiso district, was chosen as a control site due to its close proximity of approximately 20 km from the capital city and comparable service delivery and population characteristics with the intervention site. During the study period, 2 clinical officers, 3 nurses, 1 dispenser, 2 laboratory assistants and 1 records assistant manned its outpatient department. One of the clinical officers doubled as the facility in-charge and additionally provided administrative oversight for the whole facility.
Sample size determination
The statistical significance level of the study was set at 95% (α = 0.05) and the power of the study (1 - β) at 0.80. A binary outcome (non-continuous) study design was followed in which the average pre-study level of the facility’s performance across key study variables was estimated to be 60%. The study sought to detect a 10% minimum difference in outcomes between the 2 groups. The following sample size determination formula proposed by Noordzij et al. 2010
27
was used to determine a sample size of 353 participants per study group.

n = [(1.96 + 0.842)2 x (0.7 x 0.3 + 0.6 x 0.4)]/0.12 = 353 participants per study group.
Study variables
To assess improvement in the outpatient management of malaria cases in the study, the following variables were assessed: i. The average duration of malaria outpatient visits in each group during the study period. ii. The percentage availability of participants’ medical records with age and weight information at the point of prescribing in each group during the study period. iii. The percentage of participants with recurring malaria in each group during the study period. iv. The accuracy of malaria surveillance reporting for each group during the study period.
Study implementation
The comparative pilot study was comprised of 2 groups; an EMR intervention group and a study control group. The intervention group consisted of participants managed for malaria with the additional support of the integrated EMR system at the intervention site, while the control group consisted of participants managed using existing malaria case management procedures without any study intervention at the control site. Malaria case management with the additional support of the EMR system involved making Uganda’s national 2016 malaria standard treatment guidelines with defined anti-malarial medicines doses available to clinicians through the computerised system at the point of care. Clinicians had the freedom to use or ignore the guidelines in the computerised system. Records of participants treated for malaria at the study control site during the study period were reviewed for comparison.
Eligibility for study participation at the intervention site included a positive malaria parasitology test and willingness to sign documented consent for study participation. Participants at the intervention site signed consent to participate in the study before enrolment because clinicians there used a study EMR system with digitised clinical guidelines for uncomplicated malaria during their treatment. While at the study control site which had no EMR system implemented, verbal consent was obtained from participants whose records were reviewed or their guardians.
At the intervention site, consent was obtained differently for the various participant age groups. All adults aged 18 years and above had to provide their individual documented consent to participate in the study. For minors aged 13 - 17 years, documented consent was provided by their parents or guardians, along with minors providing documented assent as applicable. Documented assent was obtained from those minors with an appropriate level of comprehension in this age group. While for minors aged 12 years and below, documented consent was provided by their parents or guardians for their study participation. The assent form for minors was simplified compared to the consent forms for adults or parents and guardians. The study was approved by two biomedical research ethics committees.
Enrolled participants at the study site and malaria patients at the control site who consented were interviewed at the end of each outpatient visit during the study period. Data from both study groups were subsequently analysed to evaluate the outcomes of malaria case management in the two groups. Participants in each group were questioned about the duration of their outpatient visits, and the number of participants with both age and weight information available at the point of prescribing in each group was counted from facility records.
Participants with recurring malaria were identified from positive malaria diagnoses at subsequent outpatient visits to the same health facility during the study period. The accuracy of malaria surveillance reporting was assessed from physical comparison of cases reported to the Ministry of Health surveillance system and those recorded in the facility registers. A report was deemed accurate if the numbers reported matched the cases recorded in the facility outpatient registers with a ± 5% margin of error. For each site, reports submitted for seven consecutive months during the study period were analysed.
Data collection and analysis
Data on the study variables from participants in the intervention group were primarily collected through the integrated EMR system’s SQL Server database during the study period. Data from the control site were collected from paper-based records. Participant interview questionnaires, facility paper registers and health management information system (HMIS) reports were also used to collect study data at both study sites. Data sets from the sites were subsequently exported to Microsoft Excel as well as GraphPad Prism 8 for comparative and statistical analyses. Tests for significance were performed on the study results to ascertain the effect of the integrated EMR system on the study outcomes. The study data collection setup aimed to complete data collection at each study site once the required sample size of participants was attained.
Study duration
The study ran for 12 months, from March 2018 to March 2019, within which period the required study data were collected from both study sites. Data collection at the study control site started 3 months prior to data collection at the intervention site due to system customisation and setup before clinical use.
Assumptions
It was assumed that the supporting clinical processes required for the management and treatment of malaria cases at both study sites were available throughout the study period. It was also assumed that participants had a roughly good idea of the time they arrived at each health facility and that clinical weighing scales were available to clinicians at both study sites for measurement of participants’ weight.
Limitations
Only 349 participants were recruited in the study intervention group out of the required sample size of 353 participants. As a comparative pilot study, the subjects were not representative of the entire country where the EMR system was implemented but rather explorative of potential benefits to a health facility when an EMR system is used in malaria outpatient case management. The study sample size also limited the number of study participants that could be followed up for recurrent malaria episodes. The EMR system also did not provide decision support to clinicians beyond recommending anti-malarial medicines dosing. Participant clinic arrival times were also got from participant post visit interviews.
Results
Disaggregation of participant age groups based on malaria treatment guidelines.
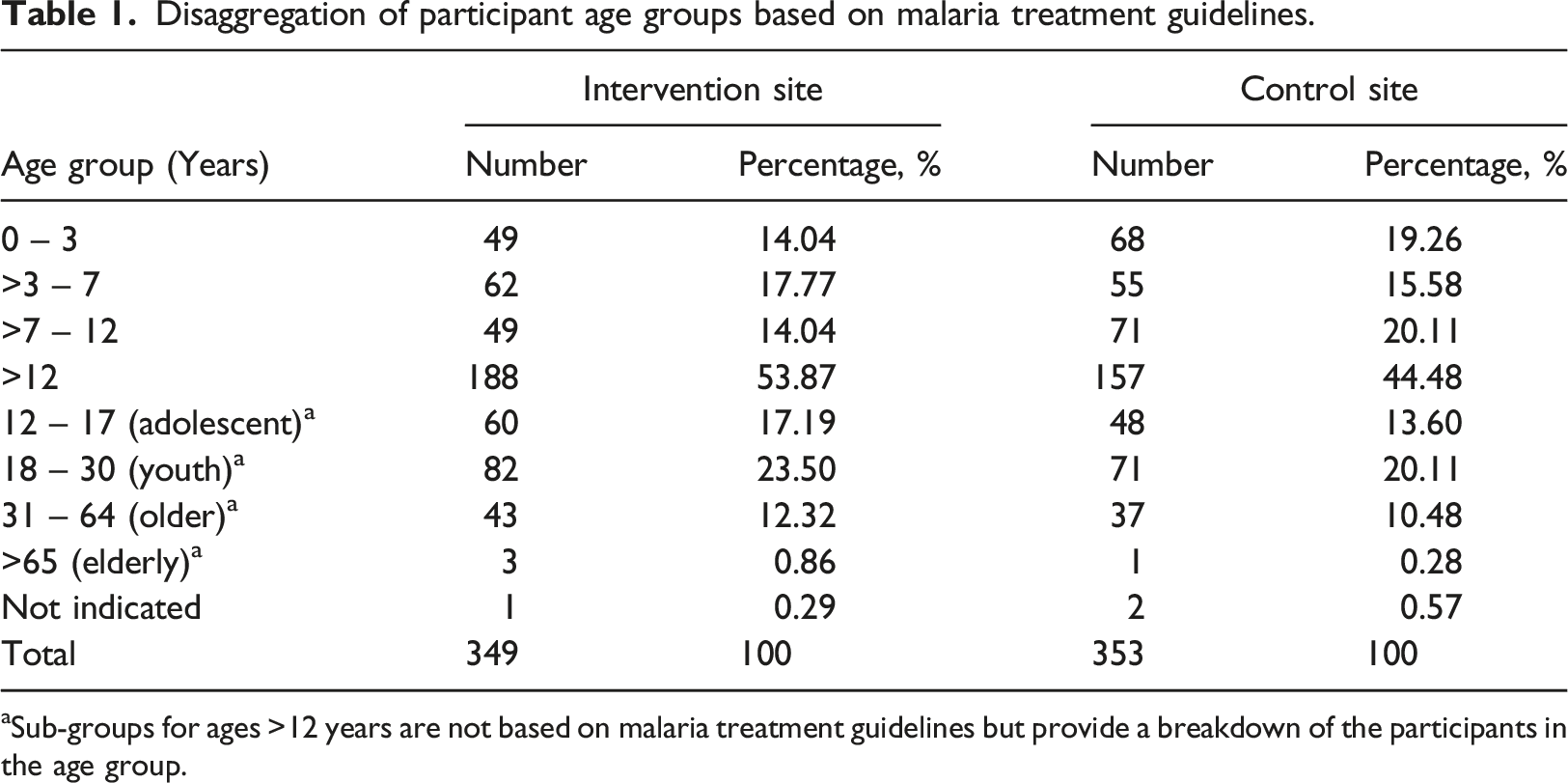
aSub-groups for ages >12 years are not based on malaria treatment guidelines but provide a breakdown of the participants in the age group.
Results of the study across three of the study variables.
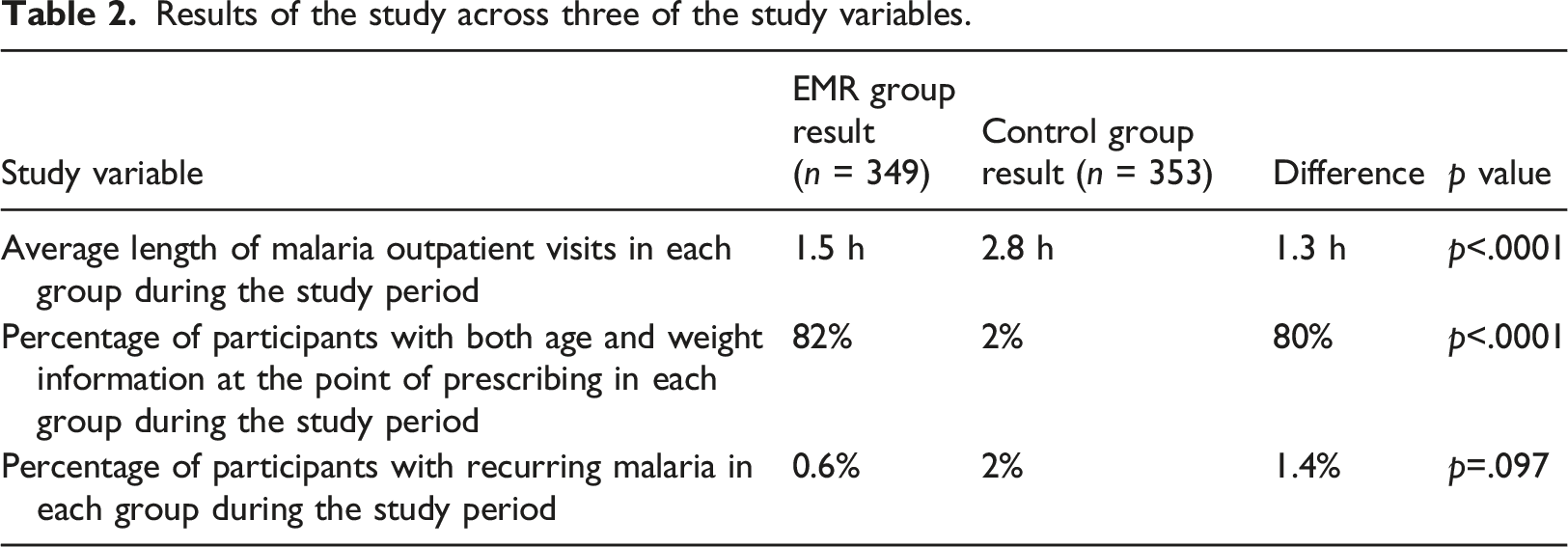
In the intervention group, information on weight and age required for prescription was available for more than 80% of patients compared to only 2% of patients in the control group and outpatient visits took significantly less time.
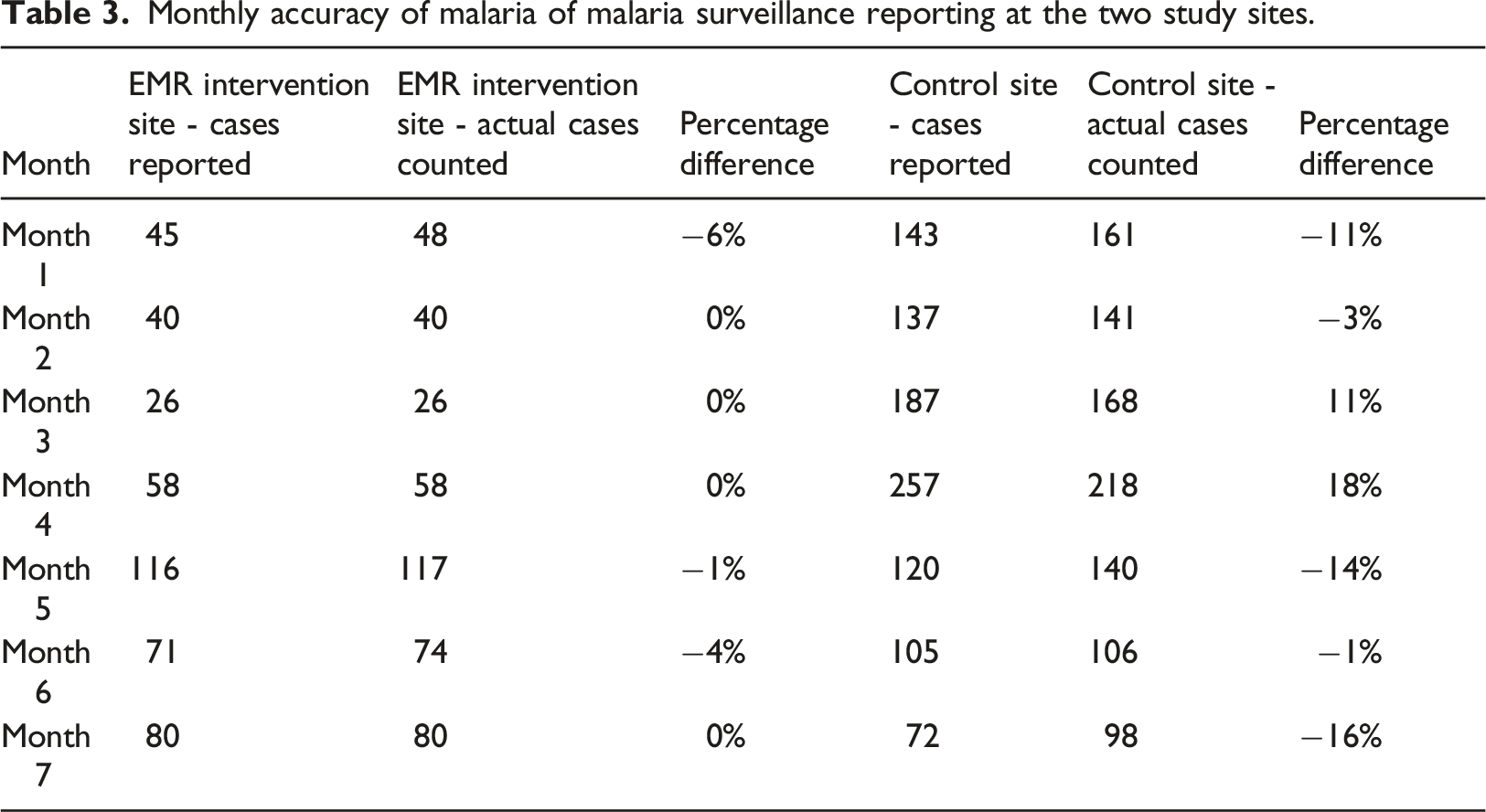
Accuracy of malaria surveillance reporting in each group during the study period
Monthly accuracy of malaria of malaria surveillance reporting at the two study sites.
Discussion
The study aimed to assess the effect of an integrated electronic medical record system on malaria outpatient case management in a low resourced health care setting in Uganda. The shortage of health professionals in sub-Saharan Africa and the high number of malaria cases in sub-Saharan African countries that are malaria-endemic amplifies the need to equip clinicians with relevant computerised tools to support more effective management of malaria cases and to strengthen malaria clinical surveillance.
A systematic review of literature on the implementation of computerised clinical guidelines revealed that significant improvements in care processes were achieved after the implementation of computerised clinical guidelines. 8 Computerised clinical guidelines were also noted to provide improvements in care processes in an integrative review though the same review noted that evidence of their effect on patient safety remained limited. 28 A 2015 study 7 showed that implementation of a standardised flowsheet developed from clinical practice guidelines within an EMR system improved the assessment of patients and other quality of care measures.
The state of malaria surveillance systems was also noted to be insufficient to support the planning and implementation of targeted interventions toward malaria elimination, yet electronic data collection and reporting systems could contribute to overcoming these gaps. 29 Malaria surveillance data in the national health management information system of Uganda collected through monthly health facility summary forms was noted to be of questionable quality, and a patient based malaria surveillance system was shown to have much higher quality data. 30
The results of the study showed that implementation of the integrated EMR system could potentially significantly reduce malaria outpatient visit durations and also improve the availability of patient age and weight information to clinicians to inform prescribing of anti-malarial medicines. Because of the statistical significance of these results, the study tentatively demonstrated that integrated EMR systems could provide clinical benefits to patients and clinicians alike in the outpatient management of malaria cases. Shorter visit durations could reduce fatigue in patients and clinicians, and increased availability of relevant information to inform prescribing could help clinicians to give the right anti-malarial medicines doses to patients who would also recover better when given optimal dosing.
While no statistical significance was identified for the difference in recurrence of malaria between both study groups, perhaps due to the small number of participants with recurring malaria in both groups, it is worth noting that fewer participants in the study intervention group had recurring malaria compared to the study control group. The significant and more consistently accurate malaria surveillance reporting trend achieved at the EMR intervention site even without automation of the surveillance report, also demonstrated the potential that integrated EMR systems could provide when implemented in health facilities to enhance reporting of the correct number of malaria cases seen in health facilities which would better inform planning for anti-malarial commodities for patients and malaria control and prevention strategies.
Conclusion
Overall, the integrated EMR system potentially significantly improved malaria outpatient case management by reducing outpatient visit durations, enhancing the availability of patient age and weight information to clinicians to inform anti-malarial medicine prescribing and improving the accuracy of malaria surveillance reporting. This led to the conclusion that integrated EMR systems have the potential to improve malaria outpatient case management in a low resourced setting. More rigorous studies with larger sample sizes and a higher number of intervention sites are necessary to ascertain these benefits.
Footnotes
Acknowledgements
The authors would like to acknowledge the Wakiso district health office in Uganda and the staff of Buwambo and Kajjansi health centres where the study was implemented.
Authors’ Contributions
Both authors were involved in the study design and development of the study protocol. MK gathered the data and wrote the first draft of the manuscript. MM guided the writing and statistical analysis and was involved in editing and compilation of the final manuscript. Both authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MK got involved with scale up of the RxSolution software in health facilities in Uganda after the study began. This however did not influence the study design or results. MM declared no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Health, Fogarty International Centre (grant number: 4D43TW007004). The funder was not involved in the design of the study or collection, analysis and interpretation of data or writing of the manuscript.
Ethics Approval
The study was approved by the University of KwaZulu-Natal Biomedical Research Ethics Committee reference number BFC422/15 and the Makerere University School of Medicine Research Ethics Committee reference number 207-148.
Abbreviations
EMR: Electronic Medical Record
HMIS: Health Management Information System
MeSH: Medical Subject Headings
MRS: Medical Records System
SQL: Structured Query Language