
Abstract
This study aimed to examine health information technology-related incidents and identify risks associated with multiple patients’ management. Sources of information comprised interviews with healthcare professionals and three small sets of local voluntary incident reports using two sampling strategies, purposive and snowball sampling. Incident reports, in the form of free-text narratives, were aggregated for analysis using the Health Information Technology Classification System and thematic analysis. Of 95 incidents, 176 issues were identified, comprising 77% (n = 136) technical issues, and 23% (n = 40) use or human-related issues. Human issues were over two times more likely to harm patients (OR 2.25, 95% CI 1.01 - 4.98) than technical issues. Incidents that affected multiple patients’ care accounted for 70% (n = 66) of the total sample, and large-scale events comprised 39% (n = 26) of the incidents that affected multiple patients' care. Systematically identifying and characterizing such incidents should be prioritized for health information technology implementations.
Introduction
Over the last few decades, supporting health information technology (HIT) systems have been introduced to enhance workflow and make healthcare delivery more efficient.1,2 However, their introduction has encountered substantial problems, including planning, design, and implementation, and management has generally been sub-optimal. 3
Healthcare is a socio-technical complex system. An inappropriate design and use of HIT systems, such as Electronic Health Records (EHR) 4 or the e-prescribing system integrated with the EHR, add a layer of complexity to the existing complex healthcare system.4–6 New and often unforeseen HIT risks emerge during and after implementation, adding complexity to medical encounters due to either human or technical factors. 7 Human factors refer to “the scientific discipline dealing with interactions among humans and other elements of a system that optimize human wellbeing and overall system performance.” 8 Technical factors refer to the practices and devices that can affect the operation of an organization. 9 The consequences of these problems can range from inconvenience, delays in care delivery, and workflow interruptions to severe patient harm and potential effects on the entire system and multiple facilities.4,10 “Large-scale adverse events are individual events or a series of related events that injured or increased the risk that many patients would be injured because of health care management.” 11
The collection of incident reports is one of the most crucial safety management tools in the healthcare system. 12 Studying and analyzing incident reports, which are free-text narratives, helps identify and characterize issues, for example, problems arising from complicated and unintended interactions between human and HIT systems, which would not be affordable with a standard prospective study design.
One of the central aspirations of Swedish society has been digital transformation, not least of healthcare, a goal that shapes Sweden’s economy and society as a whole. 13 However, to a great extent, this has not been accompanied by the characterization and identification of the problems faced by the relevant digital systems. The study of incidents reports is common in countries like the UK, 10 the US, 14 and Australia,15,16 but unusual in Sweden. Therefore, a study of HIT incident reports will illuminate the current challenges faced by digital systems in Swedish healthcare to meet today’s societal challenges, such as a sustainable healthcare system.
The objective of this study is to examine reported HIT-related patient safety events collected from various sources in Swedish healthcare to identify the nature of the risks and consequences associated with those incidents. The study also aims to determine how multiple patients' care management has been affected as well as the risks associated with large-scale events to a certain extent.
Methods
Data collection
Incidents in relation to Swedish healthcare were collected. These comprised interviews with healthcare professionals and three small sets of voluntary incident reports from various healthcare sources.
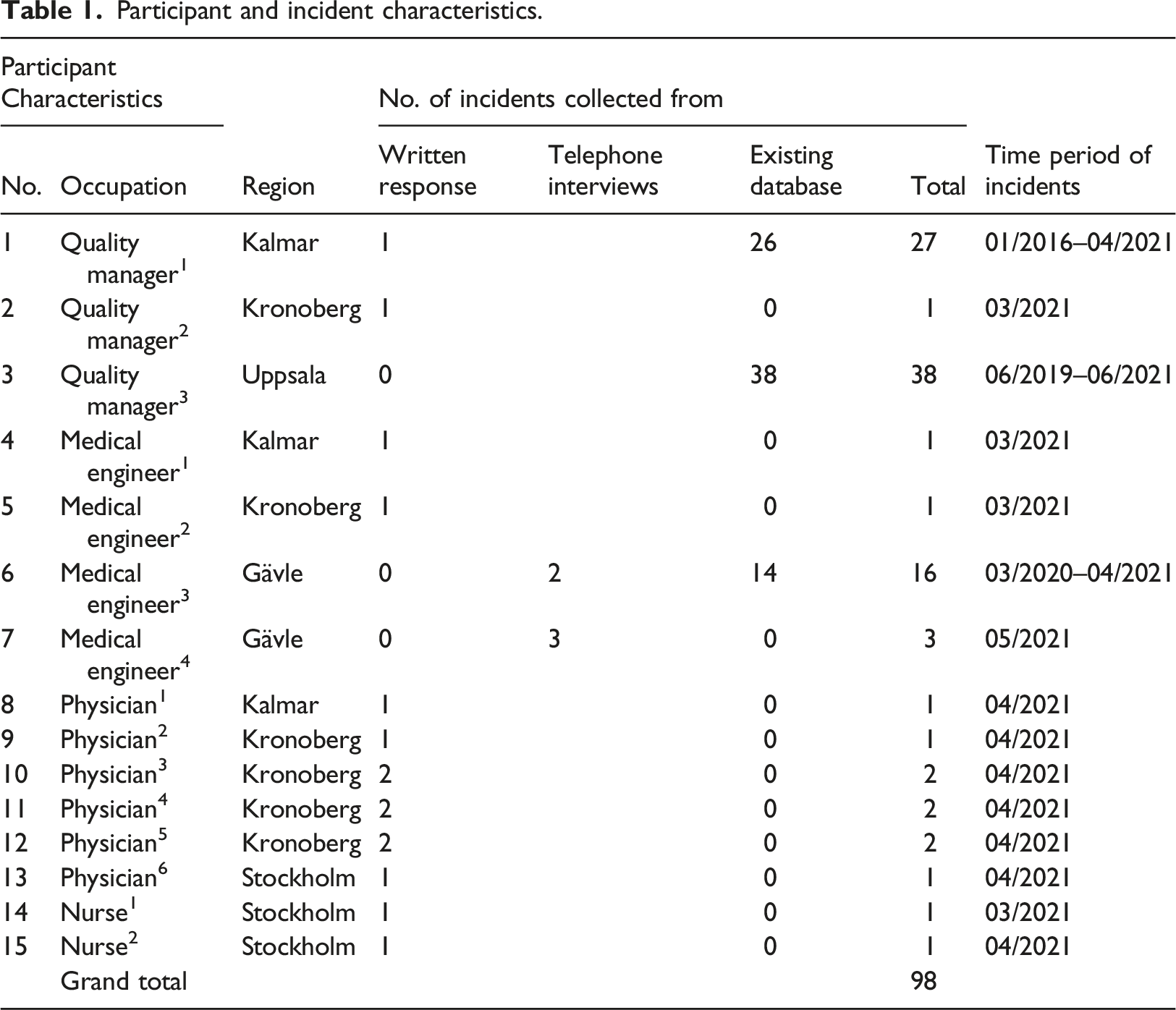
Participant and incident characteristics.
Four open-ended interview questions were developed as an interview guide in English (and later in Swedish) to collect data. Potential participants were approached via email both in English and Swedish with the four questions, a short introduction to the study, relevant information about the researchers, and a participant information sheet. The participants could reply to the interview questions either in writing (via email) or through telephone (in a semi-structured interview) and provide a set of existing incident reports from their local database. All Swedish responses and incident reports delivered were translated into English. A follow-up communication was made with the participants to extract additional information about the context. The open-ended questions were as follows:
Would you please briefly describe an eHealth-related incident/adverse event you have experienced? What were the contributing factors leading to that incident/adverse event? How did that incident/adverse event affect the patients, healthcare professionals, or the organization? What actions were taken by the healthcare team or the organization to prevent or minimize that incident/adverse event?Interview questions
Data analysis
All incident reports collected from various sources were free-text narratives, which were aggregated for analysis using both deductive and inductive approaches. The deductive approach used the HIT classification system (HIT-CS) proposed by Magrabi et al., 10 and the inductive method used thematic analysis proposed by Braun and Clarke. 17 The analysis entailed familiarizing the free-text narratives and then highlighting and drawing out possible relevant concepts described by keywords and phrases. The identified concepts were cross-checked to ensure that they did not fall under any categories of the existing framework of HIT-CS. The list of extracted concepts was then checked to determine wider patterns or themes. The identified themes were then examined to ensure their suitability for grouping and presentation.
Two investigators were involved to independently examine incident descriptions and identify the types of issues and consequences. More than one type of issue could have been identified from a single incident description. In such cases, the primary incident type was considered for interrater reliability (kappa score calculations). If there was disagreement, the incident was re-examined, and the investigators reached a consensus. Thematic analysis was performed mainly by the principal investigator, and the second coder cross-checked the analysis. The incident was re-examined in the event of any difference of opinion, and a consensus was reached between the independent coders through discussion.
Incidents that affected more than one patient’s care were considered and categorized as incidents affecting multiple patients’ management. Incidents involving multiple patient care deliveries were reported on single incident report forms and counted and classified as single incidents.
18
Incidents were considered as large-scale if they affected: (a) Ten or more HIT system users, patients, or their records at one or more sites, such as hospitals; or (b) multiple components or HIT systems, such as multiple computers at a site, one or more servers, or the entire computer network.
10
The results are presented mainly in the frequency of occurrence. The degree of patient harm was evaluated using the UK national levels (low, moderate, severe, and death). A ratio (r) of association was calculated to provide an idea of the relative extent to which consequences were associated with each incident type. Sub-group analyses of the incidents concerning patient harm versus human and technical factors and large-scale events with respect to consequences were undertaken using the Pearson χ2 test and Fisher’s exact test.
Ethical approval
Ethical advice (Dnr 701-2021) was received from the Ethical Advisory Board in South East Sweden on March 4th, 2021, prior to this study. No personal or sensitive information was collected. The datasets of incident reports were filtered to deidentify any personal or sensitive information by the respective management before providing them to us.
Results
A total of 74 healthcare professionals were contacted using both sampling strategies, of which 20% (n = 15) confirmed their participation. A detailed list of participant characteristics and the number of incidents collected from each participant is provided in Table 1.
Of all reports, 95 were included for analysis, and three were excluded. Inclusion criteria for an incident were that the report had HIT implications and adequate information for coding. The overall period of the incidents ranged from January 2016 to June 2021 (see Table 1). Interrater reliability for the primary incident type was
Types of issues with health information technology systems and their use
Type of issues and consequences identified and their frequency using the HIT-CS (total sample, n = 95).
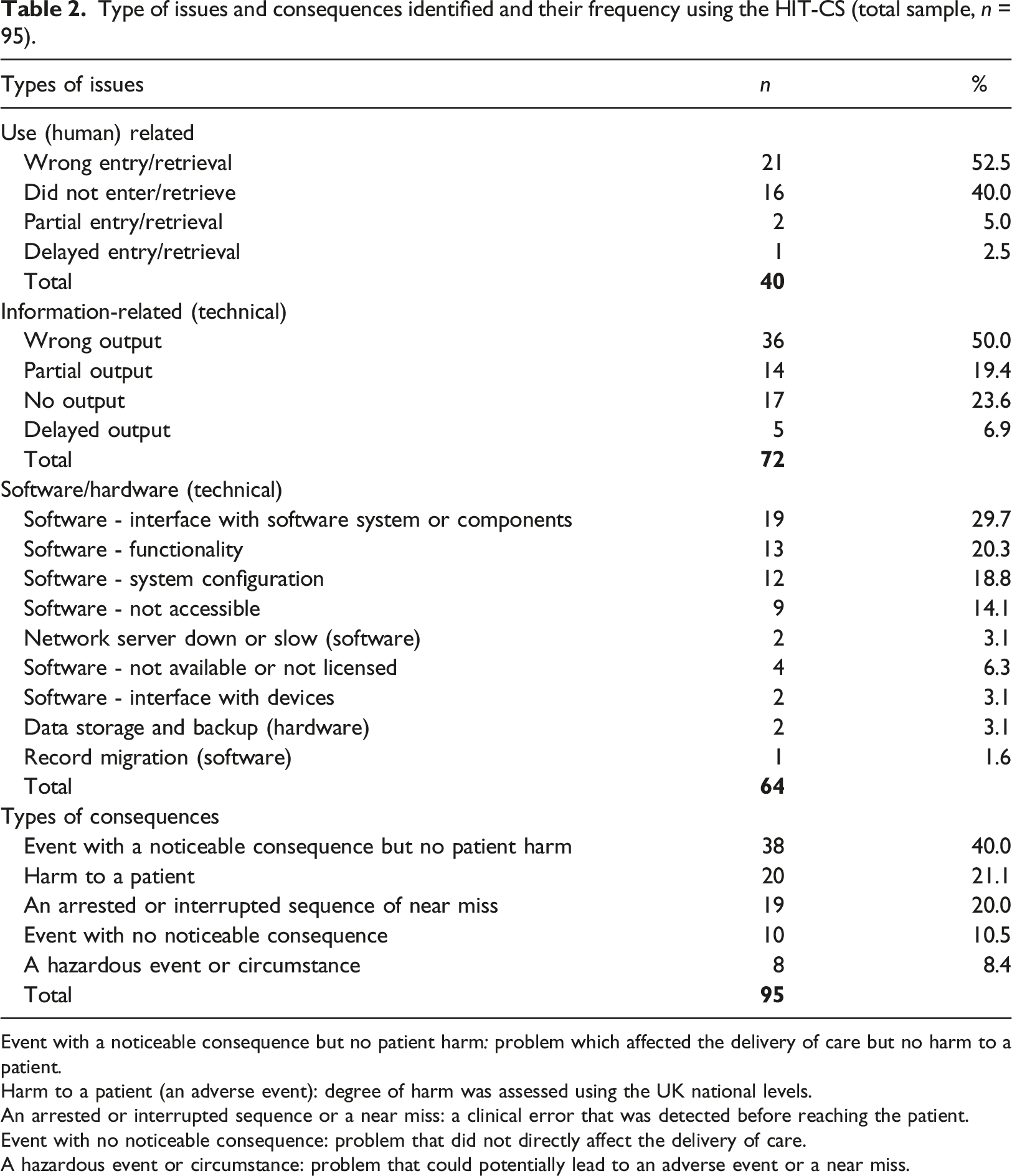
Event with a noticeable consequence but no patient harm: problem which affected the delivery of care but no harm to a patient.
Harm to a patient (an adverse event): degree of harm was assessed using the UK national levels.
An arrested or interrupted sequence or a near miss: a clinical error that was detected before reaching the patient.
Event with no noticeable consequence: problem that did not directly affect the delivery of care.
A hazardous event or circumstance: problem that could potentially lead to an adverse event or a near miss.
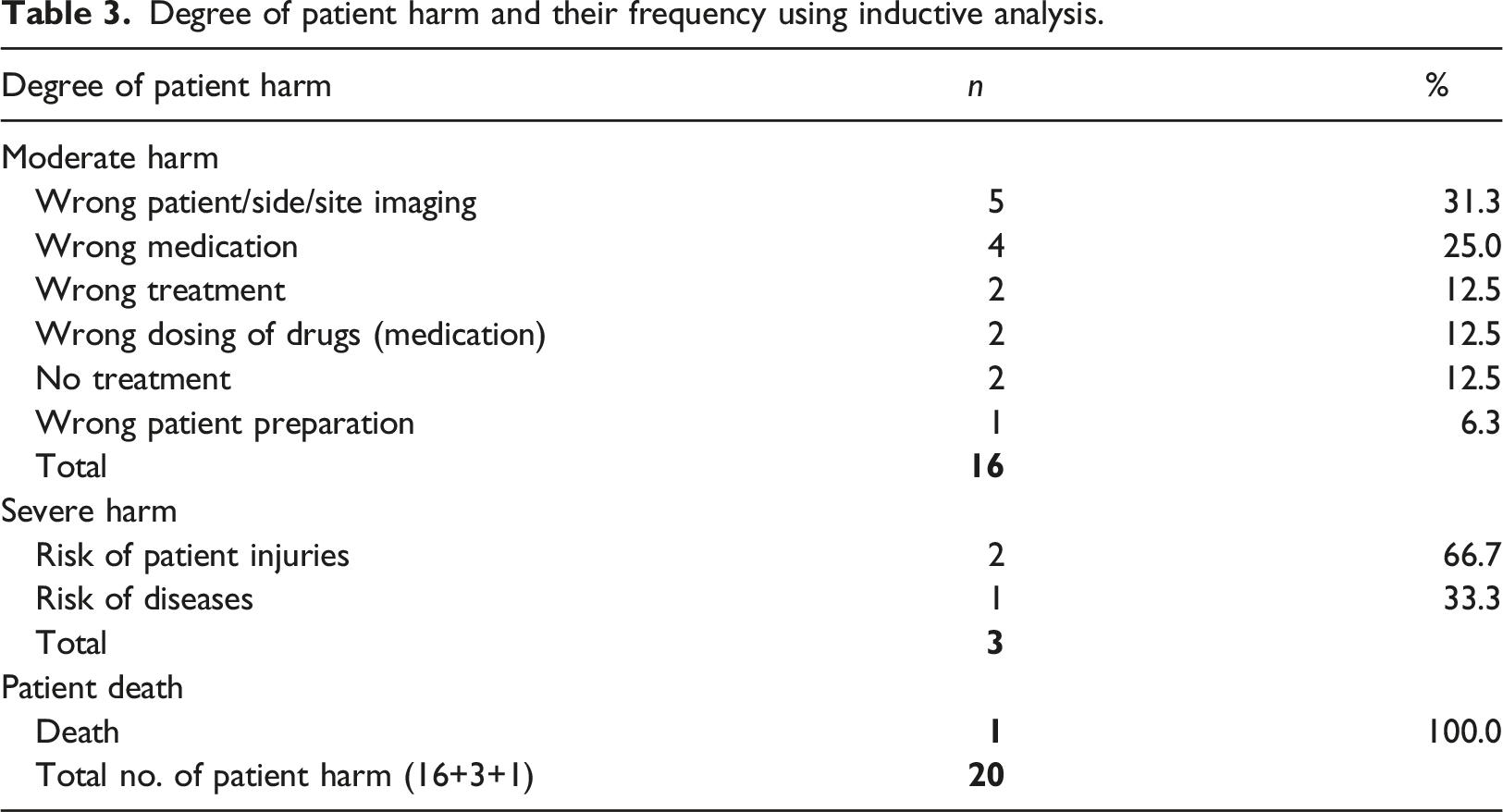
Consequences of health information technology incidents
Degree of patient harm and their frequency using inductive analysis.
Problems involving human factors were more likely to harm patients (Odds ratio 2.25, 95% CI 1.01 - 4.98).
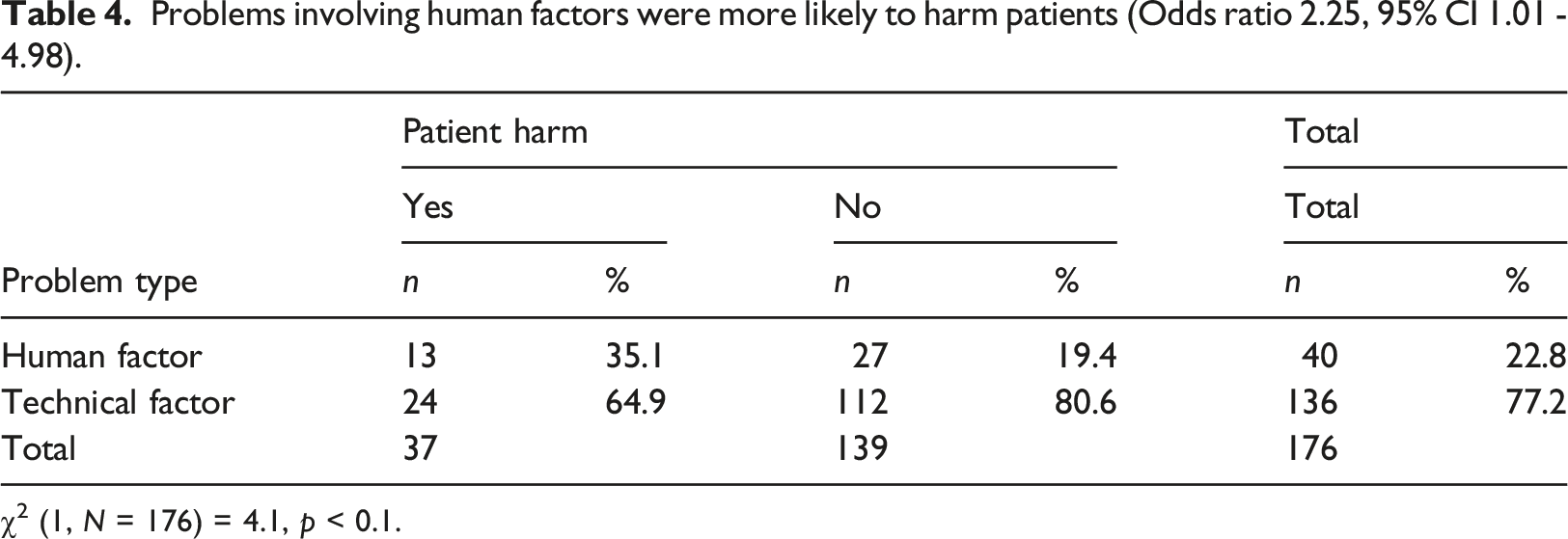
χ2 (1, N = 176) = 4.1, p < 0.1.
The severity of consequences is graded as: harm to a patient, an arrested or interrupted sequence or a near miss, incidents with a noticeable consequence but no patient harm, incidents with no noticeable consequence, a hazardous event or circumstances, or complaints. 10 However, no incident in our study had consequences identified as complaints.
Incidents affecting multiple patients’ management
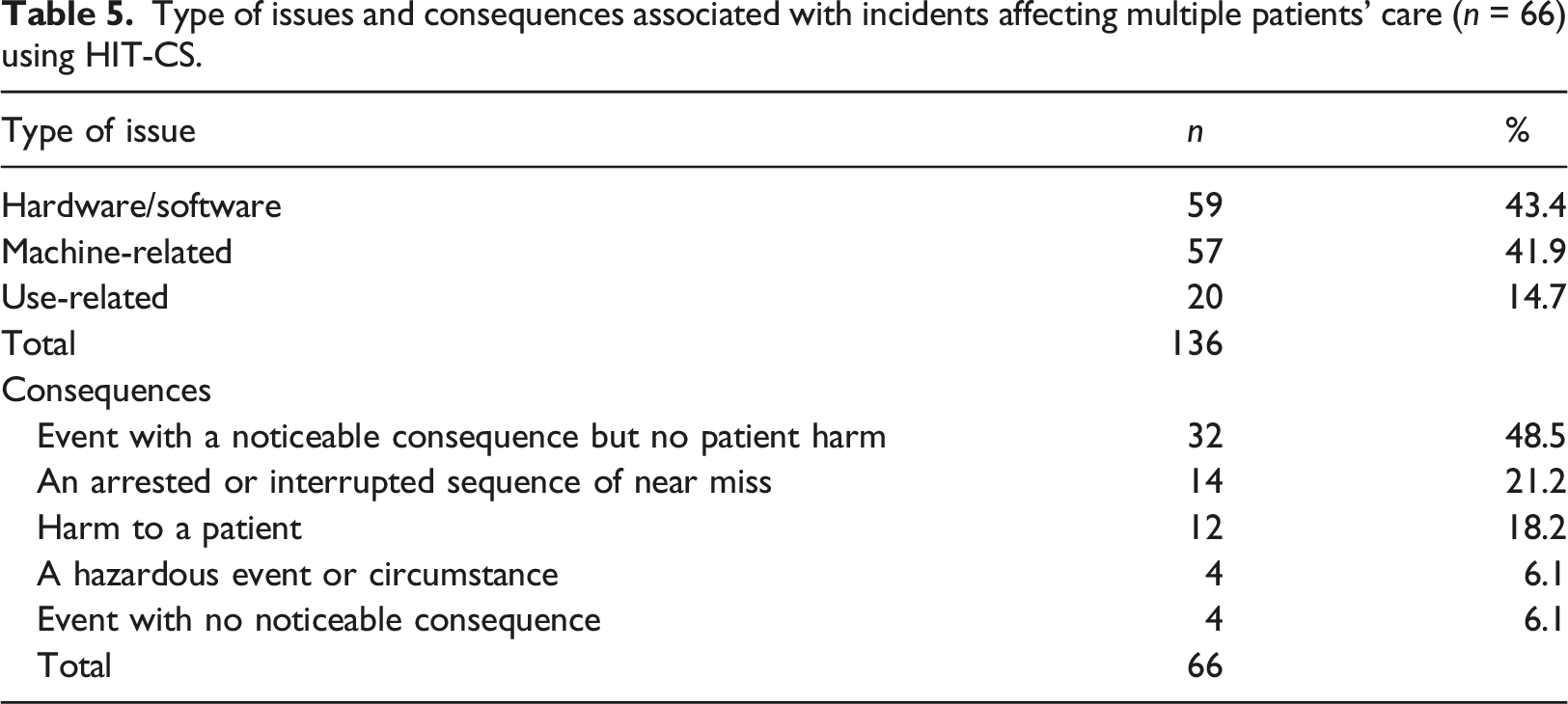
Type of issues and consequences associated with incidents affecting multiple patients’ care (n = 66) using HIT-CS.
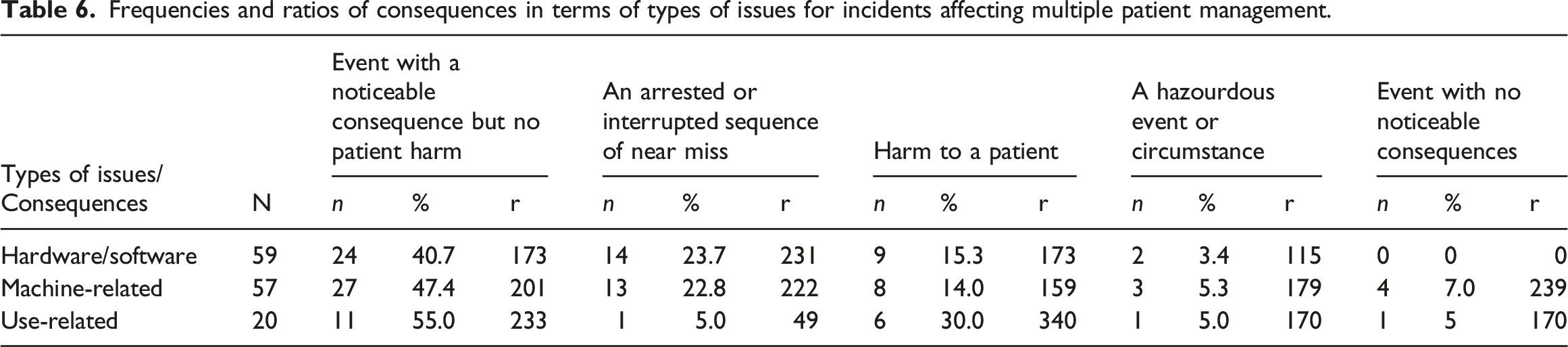
Frequencies and ratios of consequences in terms of types of issues for incidents affecting multiple patient management.
Large-scale events
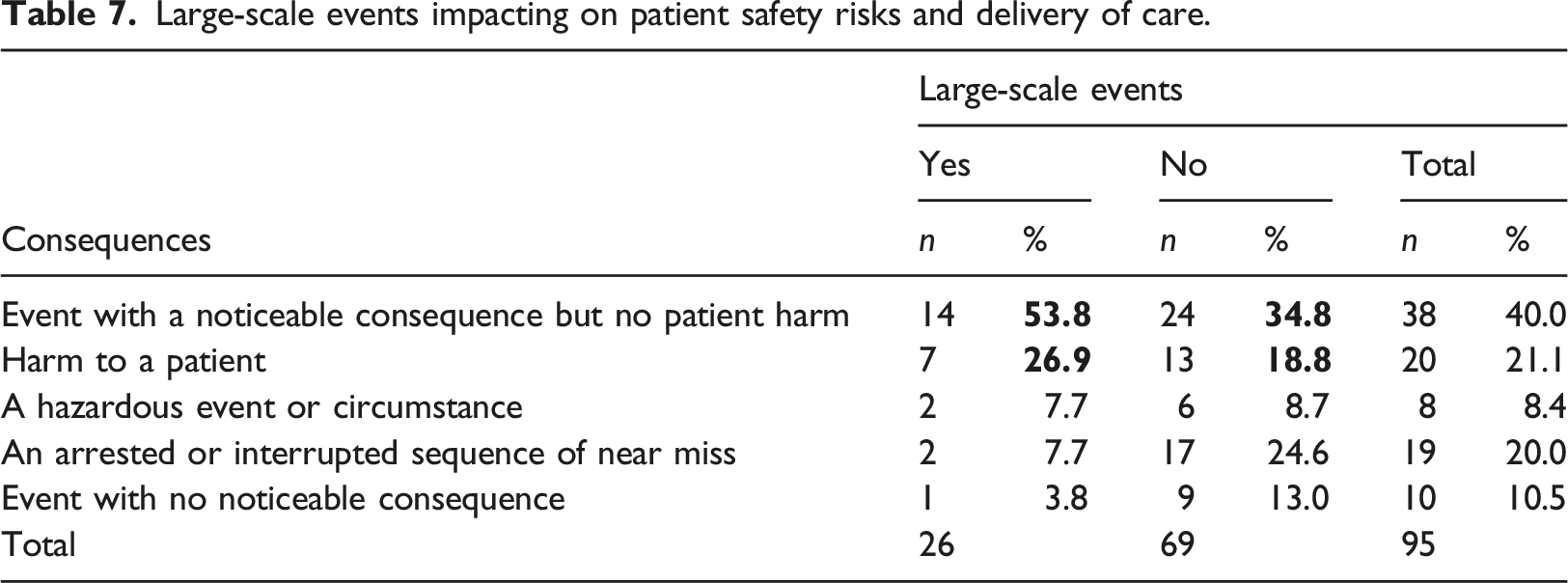
Large-scale events impacting on patient safety risks and delivery of care.
Type of systems and system issues involved in large-scale events (n = 26) using inductive analysis.
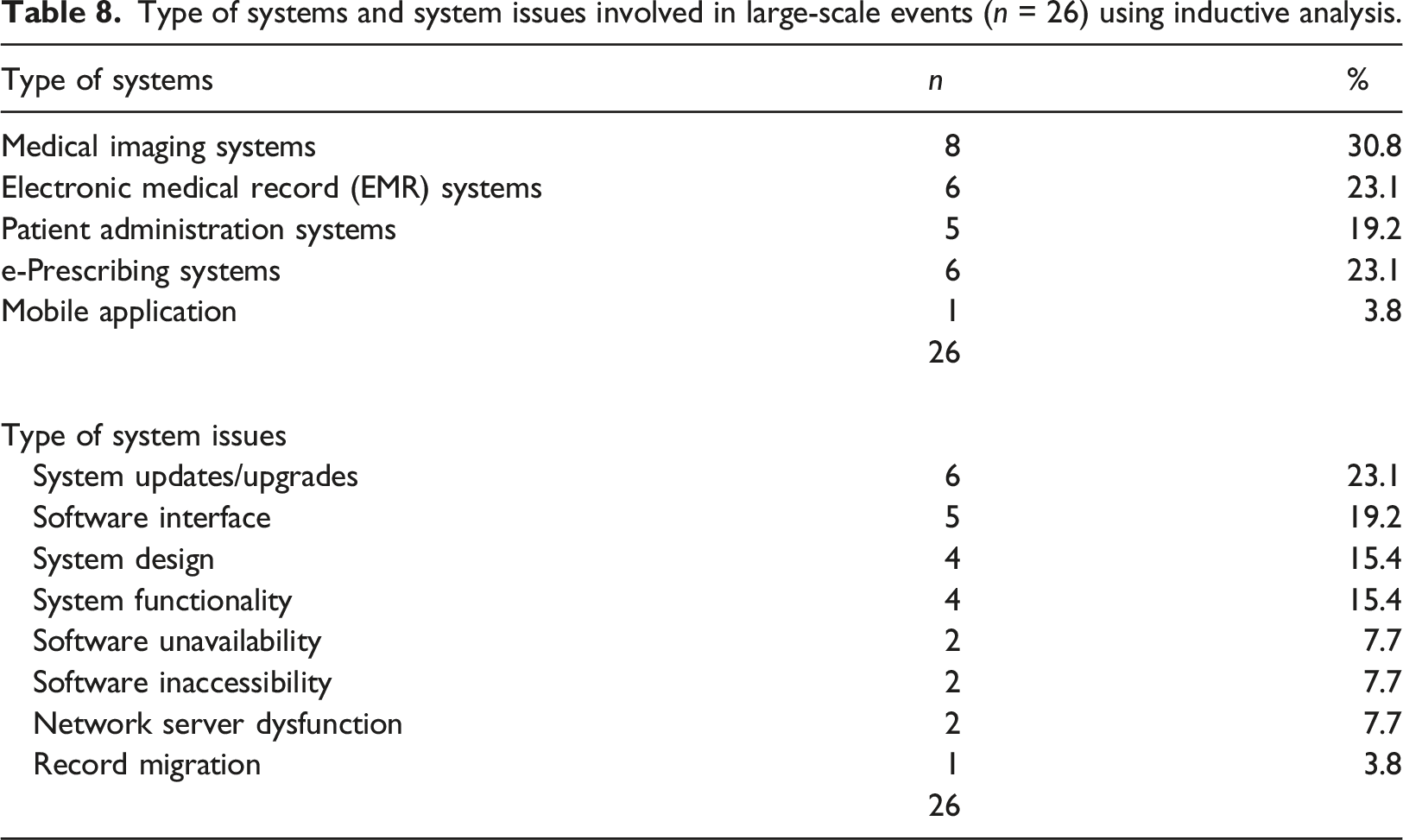
Over half (58%) of the large-scale events were associated with system updates/upgrades (n = 6), system interface (n = 5), and system design issues (n = 4). A few events also involved software issues, multiple network server dysfunction, and record migration (see Table 8). These events were also associated with limited access to student health records due to the Data Protection Act, continued lack of electronic coordination between EMR and e-prescribing systems, and system updates.
Problems associated with the e-prescribing system, i.e., the lack of coordination between medical and pharmaceutical modules, affected the greatest number of patients. For example, the inability to transfer 30 medical prescriptions due to incorrect generation of patient ID, and the disappearances of 40 prescriptions from the temperature curve in inpatient care, caused both patient and staff consequences. Issues related to system updates, such as launching a new Android operating system version of the mobile application for chat-based psychological treatment, caused frustration among patients and therapists because patients could not download and use the application for three days.
Discussion
The present study constitutes an opportunity to explore HIT-related incidents occurring in day-to-day Swedish healthcare and examine the risks to patient safety affecting multiple patients’ care management. A list of system deficiencies was identified: lack of interoperability, incompatibility, lack of support and coordination between two or more systems, components or modalities, and data protection protocol. These defects caused the systems to dysfunction for a brief or extended period, impacting multiple patients' management, and causing patient and staff inconvenience and patient harm.
In this study, system design and updates problems were implicated in the genesis of each type of category, causing significant delays in care delivery, moderate and severe patient harm, and additional manual work for the staff. A specific issue with the HIT systems is that a single unexpected failure can affect many people and disrupt workflow. 16 The large-scale events encompassed 27% of the incidents involving many aspects of the HIT system. Various aspects of these events involved problems with patient data, such as multiple medical images, reports, referrals, examinations, and appointments, which significantly impacted patients, staff, and the organization. A similar percentage of large-scale events (23%) was reported by Magrabi et al. 10 in their assessment of 850 medical incidents impacting patient safety in England’s national program for health IT. However, in comparison, our study identified these events to significantly affect both care delivery and patient harm.
Humans have always been the weak link in any socio-technical system, which inevitably contributes to HIT-related issues. 18 Issues due to human factors may include incorrect, delayed, or partial entry of patient details or information; healthcare professionals' lack of awareness of HIT issues; and inadequate training and competence.15,19,20 Human factors contributed to more deleterious consequences than technical, which were over-represented, being twice as likely to cause harmful consequences for patients. Similar results, but with a higher odds ratio (OR 3.98, 95%CI 1.90–8.34; p < 0.001), were found in the study by Magrabi et al. 10 Of 20 instances of patient harm in this study, 13 were triggered by human factors, including the one patient death. The same study by Magrabi et al. 10 reported that all three patient deaths were caused by human factors, whereas Jabin et al. described two (of three) deaths as associated with human factors in their study. 18 Nevertheless, humans function as both the cause and the cure of failure. 21 The human acts as an engineer or technician, to fix novel problems that arise in the socio-technical complex system, such as a human-device interface issue. 22
However, these consequences and conclusions need to be treated with caution, since the numbers are small and the underlying mechanisms are unknown. It may be easy to identify that software was not licensed or that prescriptions were lost or missing. Still, the exact mechanisms of underlying problems usually remain obscure. For example, software update to fix bugs and improve the systems may lead to further issues, and the mechanisms behind those issues may be more complicated to identify and correct. The Boeing Aircraft Corporation faced a problem of similar nature in 2019, regarding a “fix” in their new 737 Max aircraft to prevent a tendency to pitch the aircraft’s nose up. This software “fix” went wrong and resulted in the deaths of 346 people in two consecutive accidents, thus the explicit mechanism of the issue has been more challenging to identify and fix. 18
Implications for practice
Systematic steps must be taken to address and overcome such failures as much as possible, 11 which depend on the nature and cause of the incidents. For example, Schultz et al. 23 proposed a range of strategies to reduce and manage the risks of a large-scale HIT-related incident, whereas Jabin et al. 16 devised a set of recommendations associated with HIT system issues affecting multiple patients' care management. An appreciation of the comprehensive picture is necessary. Introducing or implementing a new HIT system, or an existing poorly embedded system, can have a massive impact on both staff and patients. For example, few issues encountered amongst the incidents reported in this study have their roots in the systems that were installed.
The following implications for healthcare improvement are recommended as preventive and corrective strategies based on the reflections arising from the literature and the results of this study. These implications will help overcome the continuous socio-technical challenges that healthcare organizations often encounter, particularly regarding HIT systems. ➢ ➢ ➢ ➢ ➢
Strengths and limitations
This research study was carried out during the COVID-19 pandemic, a busy and difficult moment for healthcare professionals. The pandemic has been assumed to be the cause of low response rates in this study and the smaller sample size than expected, combined with a narrower geographical range, including only five regions. Moreover, the set of incident reports provided from the existing local databases was similar in nature to some degree; for instance, they contained similar HIT systems. As illustrations, the set of 26 incidents from the local database was associated with ‘medical records’ alone. However, the overall characteristics of the incidents were different and had some instructive information, such as summarizing the consequences and patient safety risks. Widespread incident reports contained heterogeneous systems (e.g., e-prescribing, decision support, patient administration systems) reported from various stakeholders (e.g., quality managers, doctors, nurses, medical engineers).
The study focused on collecting incident reports rather than a number of study participants. We expected to include 80–150 incident reports, which would be sufficient for identifying the current challenges encountered by healthcare in terms of HIT systems and recommendations to mitigate those challenges. While varied data sources were involved – including retrospective incident reports from voluntary incident reporting systems and healthcare professional interviews – no methodological or theory triangulation was performed. Any such triangulation or data saturation 30 would require additional resources and time and, therefore, were beyond the scope of this study.
In recognition of the inherent limitations of incident reporting, no absolute frequencies can be provided, and one needs to be cautious about what is proffered rather than what we would like. Nevertheless, retrospective reporting remains the only way to gain insight into infrequent failures, provided that reports are collected efficiently and in greater detail. 31 The collected incident reports were limited by content knowledge since three incidents had to be excluded due to reporters’ lack of expertise in relevant technology. Participants' lack of willingness to participate also posed a limitation. 32 For example, one participant asserted never having encountered any such event. Moreover, the interviews were conducted only once (by the principal investigator), and no follow-up interview was conducted, limiting the validity of the already acquired information. 30 Other limitations included the varying quality of the collected data, 33 the principal investigator’s bias in framing the interview questions, 30 and the time-consuming process of the comprehensive research study.30,33
In 2016, a new national strategy for the digitalization of Swedish health and social care was launched – “Vision for eHealth 2025.” This marked the beginning of a new era in the digitalization of health and social care in Sweden and is now gradually replacing regional digital agendas. Local authorities and regions have shown varying progress in their digitalization efforts. 34 In the five-year period (2016–2021) for which this study collected data, a transition of emerging themes in relation to HIT incidents was observed. For example, incidents reported earlier in the period indicated “patient details” related issues, particularly concerning the EMR. In contrast, at the end of the period, “system issues” regarding e-prescription and medical imaging systems predominated. However, this observed transition may not be considered to measure the effect of the HIT systems and the life cycle of their implementation during this time frame (2016–2021) due to the decentralized nature of regional healthcare.
The findings extracted from the analyses, particularly the inclusive categories of the problems and consequences, are similar to those previously identified in Australia 18 and England. 10 This indicates that the data entailing patient safety incident reports, the findings, and the lessons learned may be suitable and pertinent elsewhere for quality improvement and risk management studies.
We believe that new characteristics of the existing issues may have arisen, and new and unexpected problems may have been found during this time period. Data collection included semi-structured interviews, which were analyzed with the HIT-CS to ensure that the meaning of analysis was shared by the primary and secondary coders. 30 Interrater coding reliability test, using kappa score calculation, was performed to determine the consistency between the coders. The primary coder was previously involved in investigating and coding an extensive data set of incident reports, and the secondary coder underwent extensive incident-analysis training. Both inductive and deductive approaches were used for analysis to extract more insights and meaningful information. For example, inductive methods were used for drawing out information that may not have been possible using deductive analysis.
Conclusion
The present study provided in-depth knowledge about adverse HIT system-related incidents in Swedish healthcare and their effects on clinical workflow and patient care delivery. By examining the data through multiple lenses, such as inductive and deductive approaches, this study suggests that the most likely effect of large-scale events associated with HIT systems affected the care management of multiple patients rather than just individual patients. For example, multiple patients were affected by delays and interruptions in care delivery and patient harm, including death. Systematically identifying and characterizing such incidents affecting multiple patients' management should be a high priority and professional practice for all major HIT implementations.
Footnotes
Acknowledgements
The authors wish to thank Sofia Backåberg, senior lecturer at the Department of Health & Caring Sciences, Linnaeus University, and staff at the Medical Product Agency for their help and support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work has been a part of the Postdoctoral Fellowship at the eHealth Institute, Department of Medicine and Optometry, Linnaeus University, Sweden. A publishing grant was received from the Linnaeus University as a part of University Library’s research support.