
Abstract
Background: Tinnitus may be a disabling, distressing disorder whereby patients report of sounds, in the absence of external stimulus. Recent evidence supports the effectiveness of psychological interventions, particularly, cognitive behavioral therapy (CBT) based intervention for the reduction of tinnitus-related distress and disability. This study assessed the effectiveness of mobile delivered cognitive training exercises to reduce tinnitus-related distress. Materials and Methods: Out of 26 patients diagnosed with tinnitus, 14 participants completed all 48 levels of the app. Levels of pre-post intervention tinnitus intrusiveness and handicap were evaluated using the short Hebrew version of the Tinnitus Handicap Inventory (H-THI). Mood was assessed using a Visual Analogue Scale (VAS). Participants were instructed to complete 3–4 min of daily training for 14 days. Results: Repeated-measures ANOVA of completers showed a significant large-effect size reduction on H-THI scores. 50% of completers have shown reliable change (indicated by their Reliable Change Index [RCI] scores). No significant change was found in mood. Discussion: Several minutes a day of training using a CBT-based app targeting maladaptive believes may decreased patients' tinnitus intrusiveness and handicap. Conclusions: Mobile apps can provide access to CBT-based interventions, using an efficient, inviting and simple platform, addressing the ramifications of tinnitus symptoms.
Introduction
Tinnitus is the perception of sounds, often hissing or ringing, in the absence of any external stimulus. 1 The prevalence of tinnitus in the general population has been estimated between 8% and 30%. 2 No effective medical cures for tinnitus exist, nor has its etiology been fully understood. 3 Nevertheless, existing medical treatments may achieve amelioration in some patients.3,4
Although most individuals with chronic tinnitus adapt in the course of time, around 5–8% of these individuals report of tinnitus-related ongoing distress and disability.5,6 Only weak associations, however, have been shown between perceived psycho-acoustic characteristics of the tinnitus (e.g., loudness or pitch) and reported tinnitus-related distress and disability. 7 This has led researchers to focus on psychological vulnerability factors that may be associated with tinnitus-related distress and disability. 8
Consistent with this, cognitive behavioral therapy (CBT) has been shown to be effective in reducing tinnitus-related distress and disability.9,10 According to CBT models, maladaptive beliefs lead to catastrophic misinterpretations of tinnitus symptoms, and their potential meaning and consequences and attentional processes are central in patients’ struggle to habituate tinnitus-related distress. 11 Consequential predictors of tinnitus-related disability and distress are, therefore, maladaptive beliefs and cognitions such as overestimation of the psychological and physical consequences of tinnitus symptoms. 12 Face-to-face CBT was found to be effective in several recent systematic reviews and meta analyses, when it comes to treating tinnitus-related distress.8,13,14
Tinnitus has no effective treatment, leading to increased stress and frustration. CBT interventions increase patients' ability to cope with tinnitus, thus reducing their disability. 13 This has led tinnitus clinical guidelines to suggest CBT and various other psychological management strategies to address tinnitus-related distress and disability. 15
Many individuals, however, struggle accessing CBT related therapies, for reasons such as lack of trained psychotherapists, cost of treatments, and stigma associated with psychological treatments.10,16 The onset of the COVID-19 pandemic, associated burden on the healthcare system and restrictions in movement have further reduced access and availability of face-to-face psychological treatments. 17
Cognitive behavioral therapy has the advantage of computerized delivery (internet- and mobile-delivered CBT–based interventions) that allows greater availability and time-adjusted treatments at significantly lower costs. 18 Such computer-based CBT interventions were shown to reduce tinnitus symptoms and associated impairment.10,18,19 Moreover, mobile CBT apps may provide a useful, easy and available solution during lockdown due to COVID-19. Nevertheless, most CBT-mobile delivered app ignore the advantages of this platform when converting existing desktop treatments into mobile apps.
GGtude is a mobile platform comprising game-like, touch-screen, training exercises that are offered daily and are only a few minutes long (see GGTI intervention section below). Each training exercise targets maladaptive beliefs (e.g., catastrophizing of tinnitus-related sounds) identified as related to specific symptoms (e.g., body image, self-esteem and obsessive doubts). 20 Training with apps on this platform for a duration of 2 weeks have been shown to reduce a range of symptoms and maladaptive beliefs five published randomized controlled trials with non-clinical, high risk, and clinical samples.20–24
The GGtude platform comprises several elements suggested to reduce users’ maladaptive cognitive processes.20,24,25 For example, psychoeducation elements incorporated throughout the training may encourage users to persevere, and assist in understanding of basic CBT principles. 20 Daily training may increase users' awareness of their maladaptive inner dialog. Exposure to self-statements challenging their maladaptive beliefs may enhance users' accessibility to such statements and their capacity to generate adaptive self-statements.
The aim of the present open trial was to evaluate the potential efficacy of a mobile CBT mHealth app in reducing the distress and perceived degree of handicap associated with tinnitus. For that end, we created the GGTI, adapting the GGtude platform to target maladaptive beliefs specifically associated with tinnitus (e.g., catastrophic misinterpretations of tinnitus symptoms and their consequences). We hypothesized that tinnitus patients using the app for a period of 2 week would show amelioration of tinnitus-related distress.
Materials and methods
Demographic data for completers and drop-out participants. Statistical analysis for differences between groups.
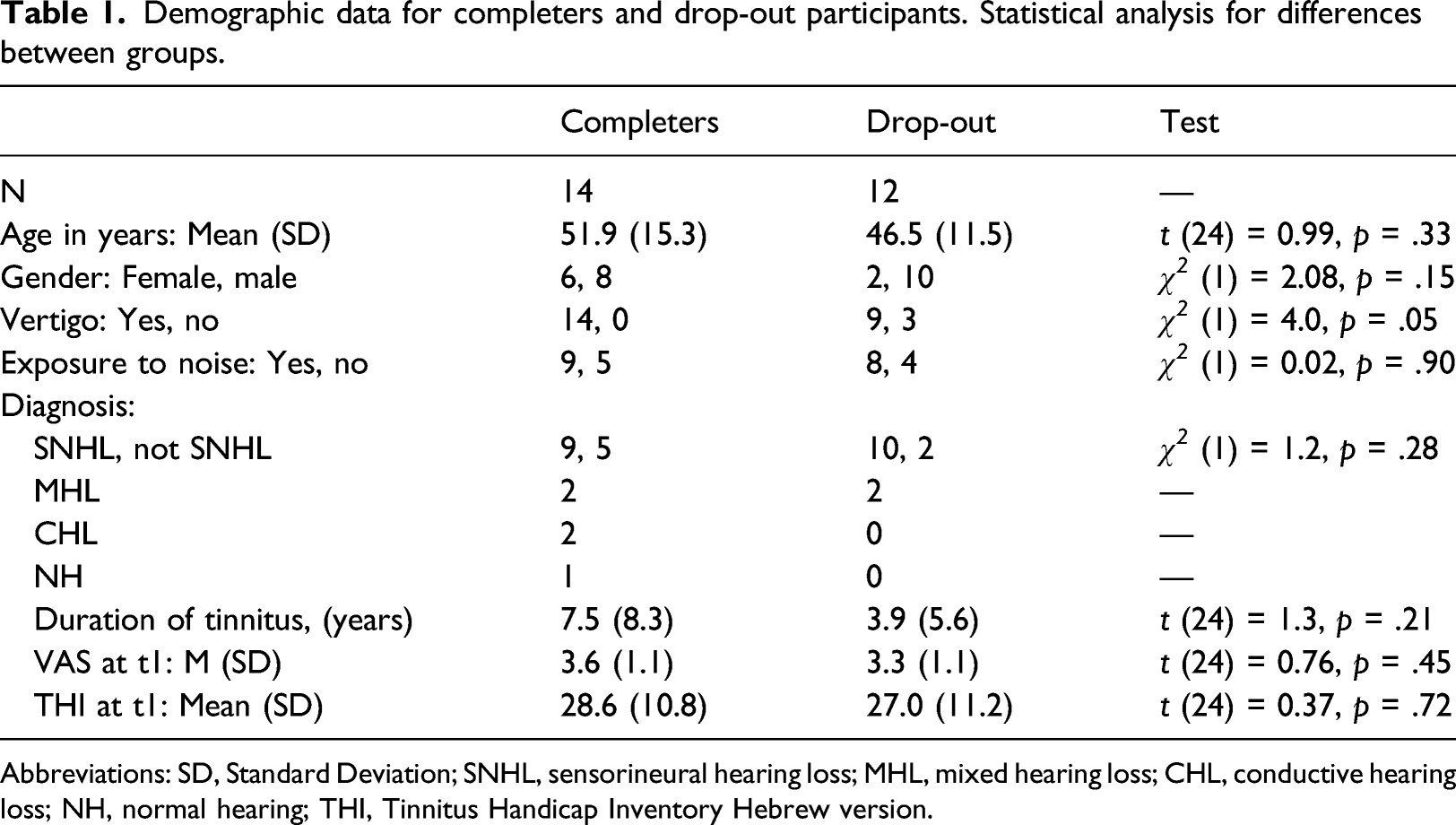
Abbreviations: SD, Standard Deviation; SNHL, sensorineural hearing loss; MHL, mixed hearing loss; CHL, conductive hearing loss; NH, normal hearing; THI, Tinnitus Handicap Inventory Hebrew version.
Patients with constant (subjective and non-pulsatile) tinnitus lasting more than 3 months were offered to use GGTI, in order to aid their coping with tinnitus. After signing an informed consent form, the app was downloaded to the participants' smartphone from iTunes or Google Play.
Intervention
“GG Tinnitus” (GGTI) is a module from the GGtude platform that was designed to challenge dysfunctional beliefs
23
believed to hamper adaptive coping with tinnitus symptoms. The main gameplay of the app consists of statements appearing at the middle of the screen (see Figure 1). Users are asked to respond to a statement on the screen by pulling it towards themselves (i.e., downwards) or pushing it away from themselves (i.e., to the top of the screen). For example, the app presents statements such as “There is only tinnitus in my life” (a dysfunctional statement) or “I can function even with noise in my ears” (an adaptive statement). Users are then asked to respond to dysfunctional statements by eliminating them (i.e., moving them upward and away from themselves) or to adaptive statements by embracing them (i.e., pulling them downwards and toward themselves). In this way, training with the app helps in facilitating flexibility of interpretations of thoughts, emotions, and events associated with tinnitus.
24
Screenshot of the app.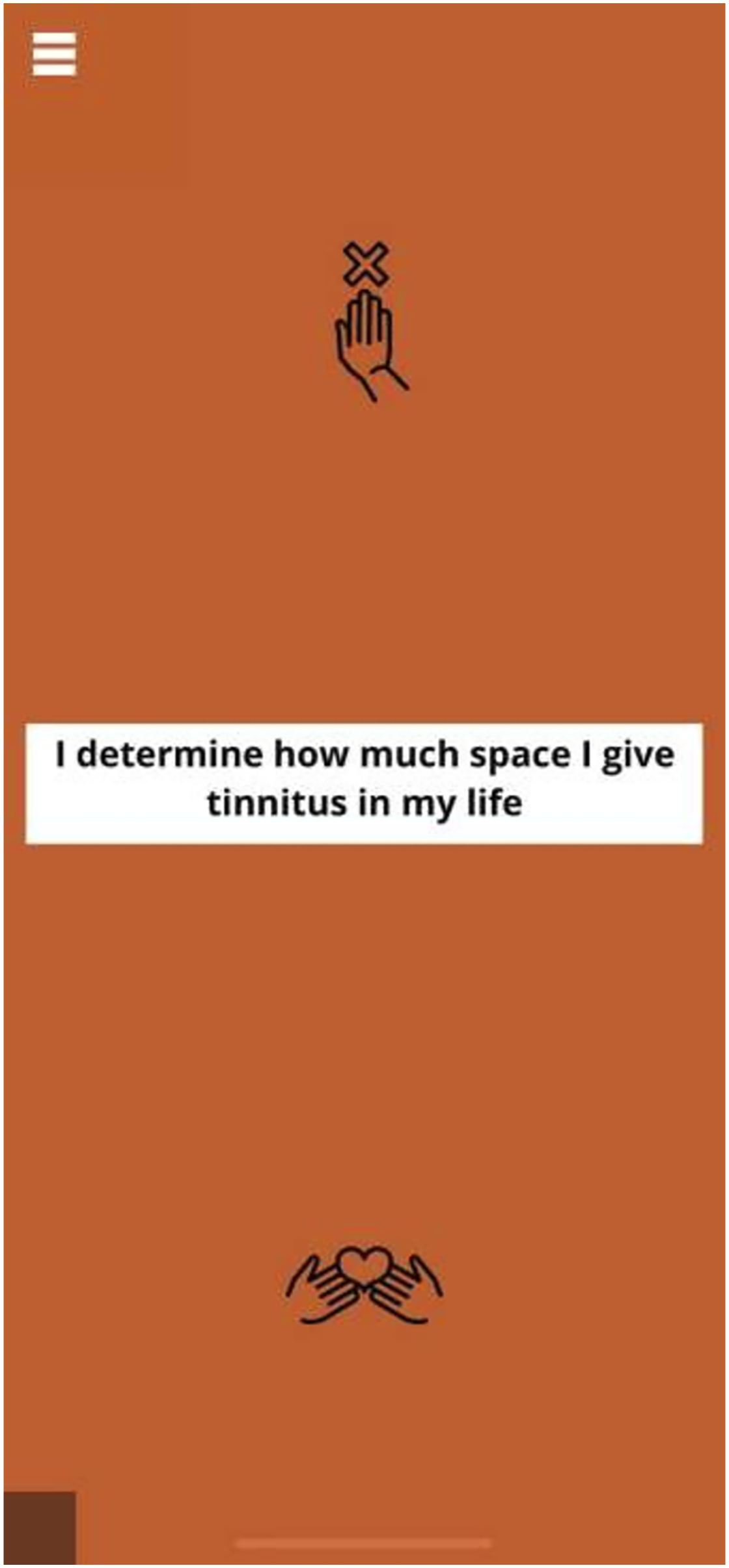
Users progressively complete 48 levels dedicated to tinnitus and associated maladaptive attitudes, such as dealing with the psychological and physical consequences of tinnitus, catastrophizing, reducing attention on tinnitus, uncertainty, and worry related to tinnitus. Prior to dealing with a belief such as catastrophizing, a screen is presented with the rationale for challenging that belief 23 (e.g., “Research shows that extreme and catastrophic interpretations of tinnitus-related sounds is associated with reductions in quality of life. Let’s try and reduce such catastrophizing”). Three levels are dedicated to each maladaptive belief. 23 For instance, level 24 (“New concept—Catastrophizing”), level 17 (“Catastrophizing of tinnitus”), and level 18 (“Reducing catastrophizing of tinnitus”) all address catastrophizing.
Once a level is completed, the users are given feedback which depends on the time it took them to complete the level (in order to inform the users about the length of time, 0 to 3 stars appear on the screen)—more stars appear if the users are quick. A brief memory quiz (i.e., Memory Boost) follows. In the Memory Boost game, the users are presented with three statements. The users are asked to recall which statement appeared in the level they have just completed. The responses result in either a “Correct!” or a “You’ll get it next time” message. The purpose of these feedback messages is to increase the participants' attention and their engagement. 23
After six levels relating to two beliefs (e.g., catastrophizing and negative thinking) are completed, users are presented with encouraging statements such as “Excellent! Now you’ve learned how to better deal with your catastrophizing and reduce your negative thinking tendencies”. 23 A screen suggesting the participants to halt the use of the app for that day appears after three levels are accomplished each day. Push notifications prompt participants to use the app daily. 23 The participants are recommended to train for a few minutes daily, preferably before sleep in order to increase memory consolidation. Participants are advised to complete the task in 16 days. App data includes the final level reached by the user. As progression of the app is linear (i.e., users cannot skip levels), we were able to ascertain whether users completed all levels of the app (or the final level reached). The recommended use of the app was 3 min a day. App data, however, did not include duration of use. In order to use GGTI, a smartphone with an operating system Android 4.2 or above or iOS 7 or above, is needed.
Assessments
The degree of users’ tinnitus intrusiveness and handicap was estimated using a short version of the Hebrew Tinnitus Handicap Inventory (H-THI), 27 including 12 questions, 28 at t1, (level 1 of the app—beginning, before using the app), t2 (level 24, half way through the app), and t3, (level 48, final level of the app) of the app.
Mood was assessed using a Visual Analogue Scale (VAS) depicting five faces, on a scale from 1 to 5, ranging from very sad to very happy face icons 29 (see Figure 1). This type of scales is used to assess pain and mood, particularly with children.30,31 The scale is commonly used in clinical settings, and since this scale is clear and easy to use, it is appropriate to use in smartphones.
Results
Twenty-nine patients were approached and given the app for use. Twenty-six participants consented to provide their full information, out of which 14 participants completed all the levels of the app in 15.42 days on average (SD = 11.4). Table 1 presents the full demographics of participants who completed the full protocol (completers) and drop-out participants. The groups were not significantly different in the following factors: age, gender, exposure to noise, diagnosis, and mood in the beginning of the study. However, all participants who completed the study reported vertigo, versus 75% of dropout participants.
Figure 2 indicates the improvement in THI assessment with testing time. This was statistically supported by a repeated-measures ANOVA of assessment level, with assessment time (t1, t2 or t3) as within participant factor, shows a significant linear trend, F (1,13) = 14.5, p = 0.002, d = 2.12, indicating a steady decrease in the H-THI score (28.57, 22.14, 22.0 for t1, t2 and t3, respectively). Follow up analyses did not find this linear trend to significantly interact with gender, exposure to noise, or diagnosis, F (1,12) < 1.2, p > .3. We further did not find the difference in assessment between t1 and t3 to significantly correlate with the duration of tinnitus, r (14) = 0.12, p = .73, with mood (VAS scores) as indicated in t1, r (14) = 0.31, p = .28, or with days for completion of the full protocol, r (14) = −0.01, p = .97. It is important to note that out of 14 participants, only 2 did not show a decrease in the THI assessment (one of which completed the task in 11 days, a shorter period than the requested one). Average THI scores for the three assessment times.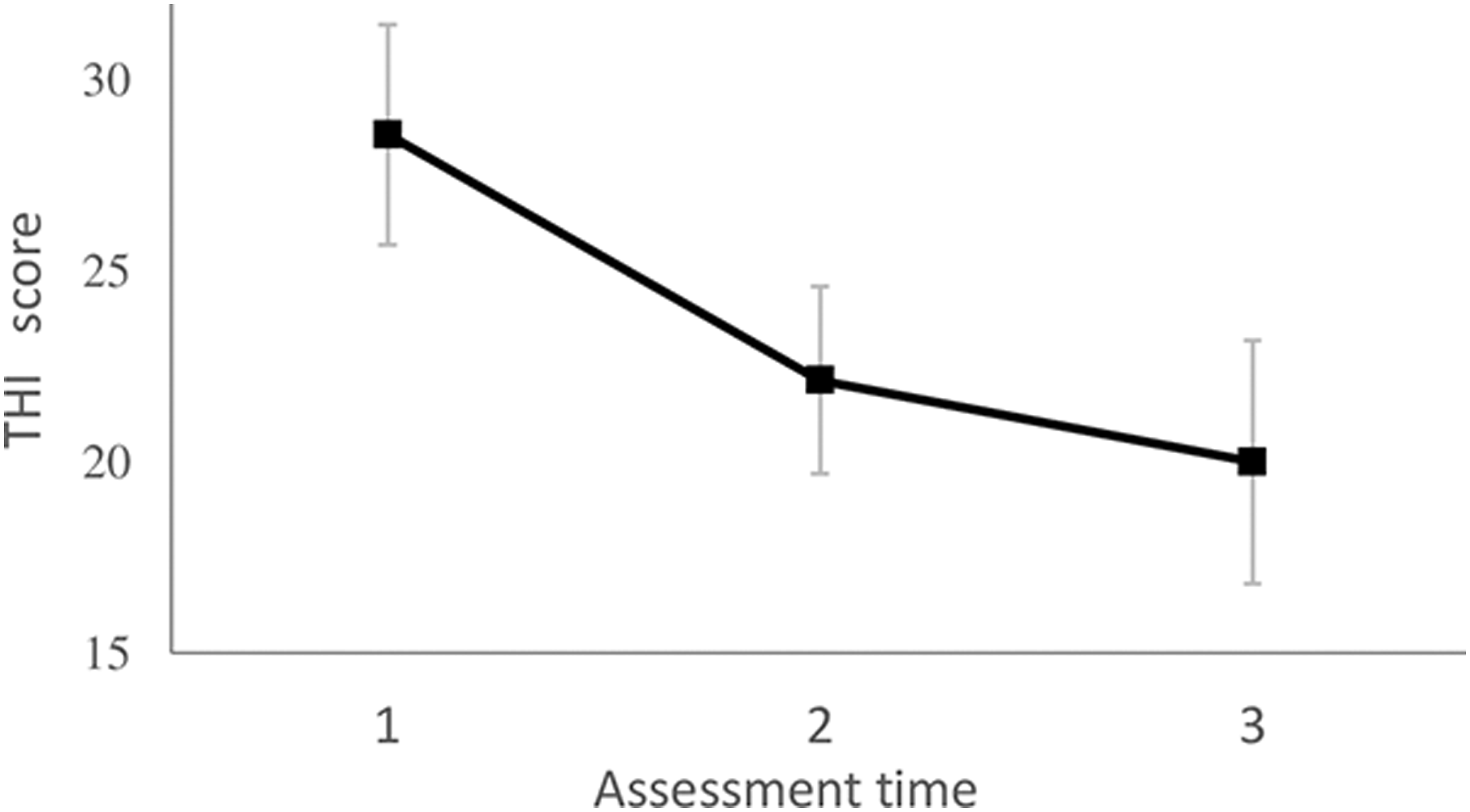
Reliable Change Index (RCI)
32
was used to assess the reliable change in THI for each participant. Reliable Change Index is based on estimates of a scale’s internal consistency and standard deviation for a given population. The threshold for reliable change is taken as 1.96 times the standard error of the difference between scores of a measure administered pre- and post-training. For the current study, the standard error of measurement (SE) was first calculated using:
Finally, RCI was calculated:
VAS, THI scores, and RCI of participants who completed all the levels of the app.
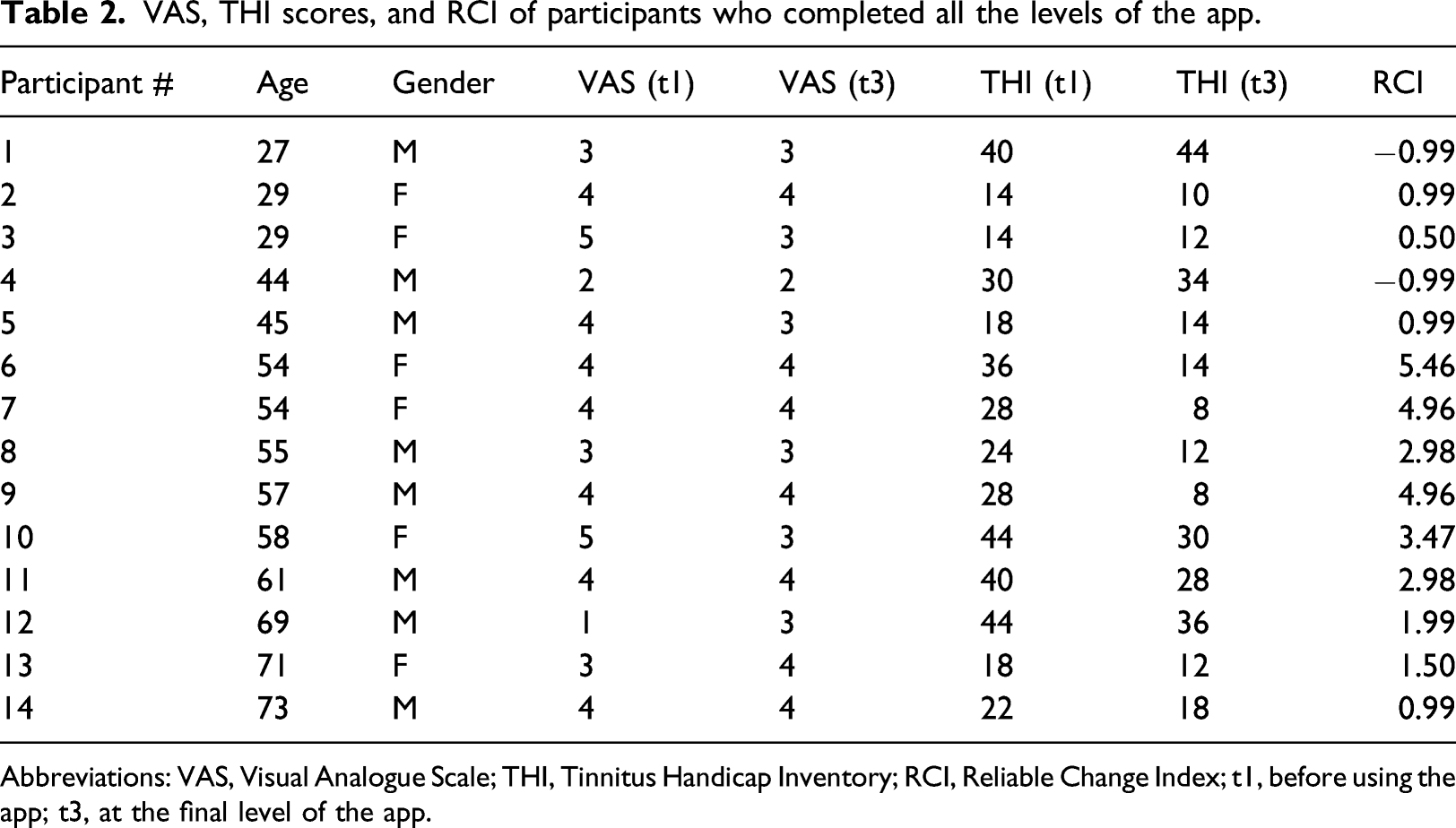
Abbreviations: VAS, Visual Analogue Scale; THI, Tinnitus Handicap Inventory; RCI, Reliable Change Index; t1, before using the app; t3, at the final level of the app.
A main concern in our study was whether older participants will be able to use the app to their advantage. We note that, the three participants aged over 65 (69, 71, and 73 years old) in the original sample were able to complete the full protocol. In a separate analysis conducted for these three participants aged over 65, the significant linear term for assessment time obtains, F (1,2) = 27.0, p = .035, d = 2.12. Another separate analysis for the 11 participants aged 27–61 years shows an increase in the advantage in tinnitus assessment between t1 and t3, as participants’ age increases, r (11) = 0.77, p = .006. Taken together, it is clear that the age of participants did not hamper the positive effect of app use on tinnitus assessment.
A similar repeated-measures ANOVA was conducted for mood assessment (VAS scores). Here, no significant linear trend for assessment time was found, F (1,13) = 0.27, p = .61. Planned comparisons further showed that mood at t1 was not significantly different than mood at t2 and t3, likewise mood at t2 and t3 did not differ, p > .6 for all comparisons. We note that VAS scores in t1 were not significantly correlated with THI scores in t1, r (14) = 0.29, p = .31. However, VAS scores in t2 and t3 were significantly correlated with the respective THI scores, r (14) = 0.60, p = .02 and r (14) = 0.56, p = .04, for t2 and t3. Importantly, the change in VAS scores from t1 to t3 was not significantly correlated with the change in THI from t1 to t3, r (14) = 0.03, p = .92.
Discussion
Tinnitus may be associated with significant disability and distress but to date, no evidence based medical treatment exists. 34 Clinical guidelines suggest psychologically based treatments such as CBT may reduce distress and disability associated with tinnitus.1,15 In this study, we examined the use of GGTI, a CBT-based smartphone app comprising of short game-like cognitive training exercises targeting maladaptive beliefs believed to maintain and exacerbate distress and disability associated with tinnitus.
We found that training several minutes a day, decreased the patients' tinnitus intrusiveness and handicap, as reflected in large effect-size reductions in their THI score. In addition, our findings indicated that more than 85% of participants that have completed the intervention showed an amelioration in their THI scores by the end of the training period and that 50% of completers have shown reliable change as indicated by their RCI scores.
These findings are in-line with previously published studies which demonstrated the effectiveness of face-to-face15,35 and internet delivered CBT interventions for tinnitus.10,18,19 Indeed, in a systematic review and meta-analysis of randomized controlled trials examining tinnitus management, 36 improvement was reported in most studies in which CBT for tinnitus (both face-to-face and online) was compared to non-CBT controls. In a more recent systematic review of internet-based interventions for tinnitus, 37 a medium effect for internet-based interventions was found. Consistent symptoms reductions in anxiety, depression, and insomnia were also found to be associated with internet-based interventions for tinnitus, but no significant effect was found for quality of life. These interventions were suggested as a routine care.
Our findings are also consistent with 5 previous randomized controlled trials (RCTs) using the GGtude platform. For instance, in a large (n = 315), fully remote RCT targeting severe mental illness (SMI) symptoms intent-to-treat analyses showed significant treatment × time interactions. Large effect size changes were observed for depression symptoms, self-esteem and recovery attitudes following app use. 21 Other RCTs using the GGtude platform have shown medium––large effect size reductions in pre-post measurements of body dysmorphic disorder symptoms20,38 and obsessive-compulsive disorder (OCD) symptoms in high-risk and student populations.23,24
No changes in mood rating were found across the three assessment occasions. The absence of changes in mood was unexpected as reductions in tinnitus-related distress were predicted to be associated with mood ratings. The intervention used in this study, however, did not directly target maladaptive beliefs associated with mood. The focus of the intervention was decreasing catastrophic interpretations of tinnitus symptoms and related cognitions. Indeed, previous studies using the GGtude platform have shown that modules that do not target mood directly (e.g., targeting relationship obsessive compulsive disorder symptoms), 24 do not show significant changes on mood measures. When modules targeting mood are included 21 reductions in depresses mood are found. An alternative explanation is that mood rating in the app reflect momentary changes in affect rather than ongoing mood. If this is the case, absence of differences in affect across assessment occasions may decrease the likelihood that THI scores reflect momentary changes in affect rather than general tinnitus related distress.
Pending replication, our findings lend support to CBT models of tinnitus-related distress. These models propose that individuals with tinnitus experience distress because they misinterpret symptoms, associated features and information about tinnitus symptoms in unhelpful and fear provoking and even catastrophic ways. 35 Distress is then maintained by various processes perpetuating such negative interpretations. Consistent with this proposal, our results suggest that targeting tinnitus-related maladaptive beliefs, including catastrophizing the physical and psychological consequences of tinnitus-related sounds, and the importance of over-monitoring such sounds, was associated with reductions in the distress associated with tinnitus symptoms. Indeed, previous studies have shown that using the GGtude platform is associated with significant reductions in maladaptive beliefs such as over-estimation of threat, intolerance of uncertainty and perfectionism.23,24,38,39 Since there is no specific treatment for tinnitus, 1 the findings from our study are very encouraging and suggest that mHealth applications may provide accessible, non-intrusive, cost-effective, and enjoyable tools for reducing negative cognitions and distress associated with tinnitus.
Despite the promising findings of this open trial, interpretations of the results should be taken with care and await replication. Our study is an open trial with no control group. The lack of control group prevents the interpretation of our outcomes solely to the intervention. Reductions in tinnitus-related distress as indicated by the THI may be attributed to various confounding factor such as mere passage of time, motivation, number of prior attempts to treat tinnitus, familiarization with mHealth, or even daily activities rate. Including a larger sample size and a control group (neutral or active) would significantly our ability to attribute the findings to the intervention.
In this study, the only measure of tinnitus severity used was the THI, since there is no objective measure of tinnitus. Although previous RCTs have shown using apps from the GGtude platform was associated with changes in response to behavioral tasks reductions on psychological processes relevant to the targeted problem 23 (e.g., maladaptive beliefs) and significant decreases in symptoms measures.21,24,38 We cannot exclude the possibility that the outcome found in this study was a mere result of the intervention training users to alter their answers to the THI. It is important to note, however, that the THI is considered the gold standard in evaluating tinnitus-related disability and includes questions mostly relating to symptoms such as difficulty in concentration and distress (e.g.: “Because of your tinnitus, is it difficult for you to concentrate?”; “Do you feel frustrated because of your tinnitus?”). In contrast, the statements in our mobile intervention do not relate to such experiences, and as such are highly unlikely to train the responder to particular responses. Furthermore, our findings suggest that 50% of the users showed reliable change on the RCI (rather than slight response changes, that may be due to training response) following app use. We therefore believe the effects found in our study reflect actual change in tinnitus-related distress, rather than the product of response training.
In addition, the study sample size was limited with a significant dropout rate. Drop out in such interventions with clinical populations are unfortunately not uncommon.19,29,40 Given the frustrating nature of tinnitus, it is not surprising to note that individuals were reluctant to even try new treatment methods. It is also possible that the fact the intervention is psychological rather than drug- or auditory-based, was aversive for some of the participants.
Future studies would benefit from use of more intense dropout reduction strategies (e.g., monitory compensation). This will allow for stronger attribution of the findings to the intervention used.
Conclusions
Consistent with finding showing the effectiveness of CBT treatments for tinnitus-related distress and pending replication, our results suggest that brief, daily, mobile delivered, cognitive interventions challenging catastrophic beliefs about tinnitus-related sounds may lead to a significant reduction in tinnitus-related distress.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: One of the authors of the paper (Guy Doron) is co-developer of GGTI. Guy Doron is also a co-founder of GGtude Ltd. GGTI is the subject of this evaluation and therefore has financial interest to GGtude Ltd.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.