
Abstract
Creating a learning health system could help reduce variations in quality of care. Success is dependent on timely access to health data. To explore the barriers and facilitators to timely access to patients’ data, we conducted in-depth semi-structured interviews with 37 purposively sampled participants from government, the NHS and academia across Scotland. Interviews were analysed using the framework approach. Participants were of the view that Scotland could play a leading role in the exploitation of routine data to drive forward service improvements, but highlighted major impediments: (i) persistence of paper-based records and a variety of information systems; (ii) the need for a proportionate approach to managing information governance; and (iii) the need for support structures to facilitate accrual, processing, linking, analysis and timely use and reuse of data for patient benefit. There is a pressing need to digitise and integrate existing health information infrastructures, guided by a nationwide proportionate information governance approach and the need to enhance technological and human capabilities to support these efforts.
Background
There are considerable variations in the quality of care across the National Health Service (NHS).1,2 These variations could potentially, at least in part, be addressed through the creation of a national learning health system (LHS). The National Academy of Medicine has defined a LHS as an entity ‘. . .in which science, informatics, incentives, and culture are aligned for continuous improvement and innovation, with best practices seamlessly embedded in the delivery process and new knowledge captured as an integral by-product of the delivery experience’. 3 LHS thus encompasses a whole systems approach whereby the system at scale learns in a cycle of three information flows: (i) data to knowledge, (ii) knowledge to practice, and (iii) practice to data, 4 (Figure 1) towards improving health outcomes.5–10
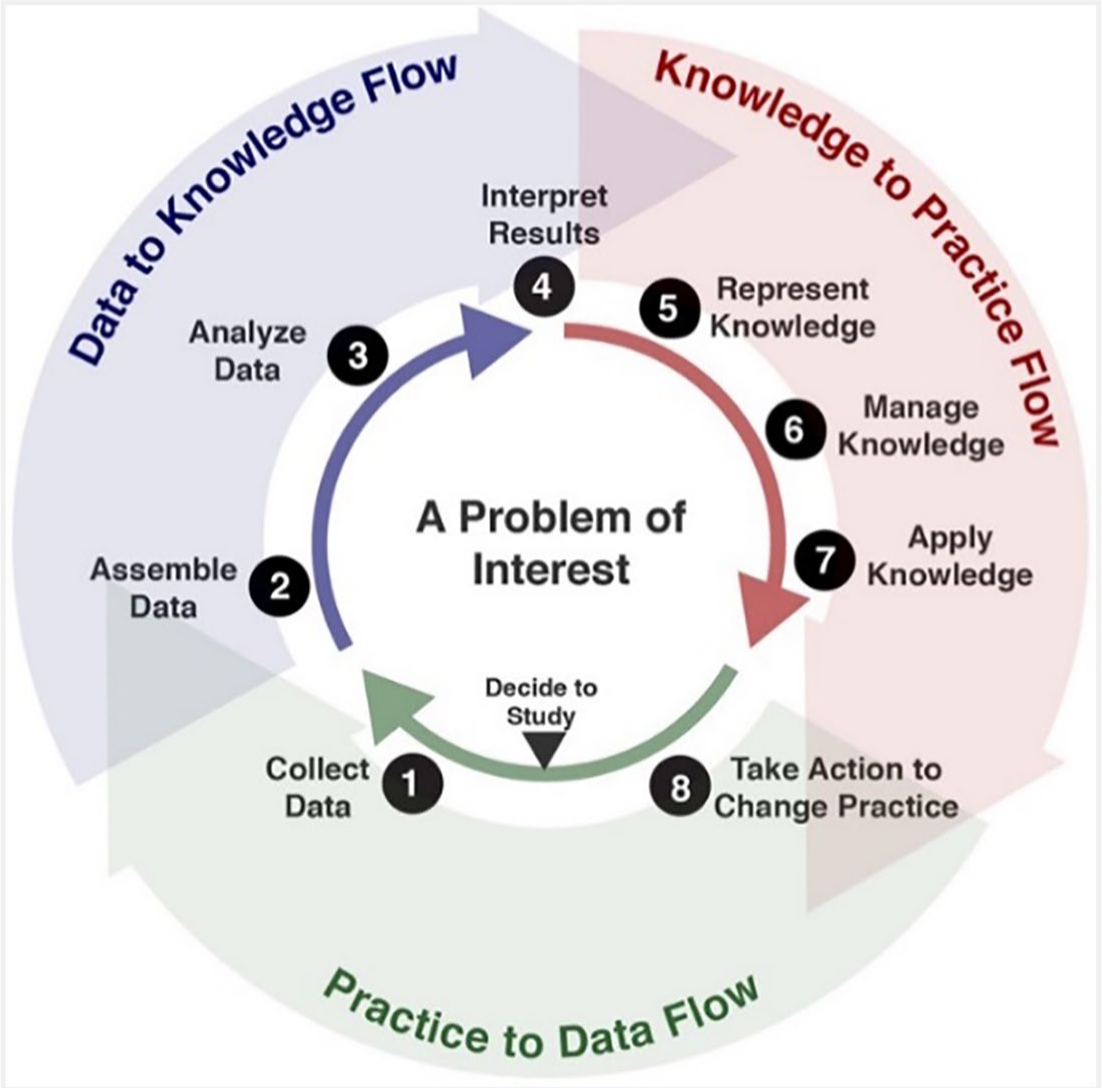
The learning health cycle of the learning health system with three information flows and eight steps. 4 Reproduced from https://doi.org/10.1002/lrh2.10054 (CC BY-NC 4.0)
The proponents of LHS outlined a strategy map with a vision and their foundational elements (e.g. clinical data, information technology, evidence standards, patient engagement), characteristics (e.g. person-centred, care-driven learning, networked leadership), collaborative actions (e.g. clinical effectiveness research, best practices, value incentives) and goals (i.e. value based on health outcomes and costs).11,12 To help transition from concept to practical application, the Geisinger Health System group described a framework with nine components: data and analytics; people and partnerships; patient and family engagement; ethics and oversight; evaluation and methodology; funding; organisation; prioritisation and deliverables. 13 To guide design and implementation of LHS a high-level architectural framework was proposed recently, based on conceptual and empirical LHS literature, with six decision layers: performance layer (helps identify, relate, and measure context-specific goals), scientific layer (guides towards context specific definition, outcomes, such as how data are collected and analysed, or how results are implemented), organisational layer (models the social dimension with governance and organisational structure), data layer (supports data description, quality assurance), information technology layer (supports the technical dimension) and the ethics and security layer (facilitates ethical and privacy measures adopted). 14
Since there are wider determinants of health, emphasising only on healthcare in LHS is misplaced.15,16 For example, the impacts of housing on mental health, road planning on traffic accidents, taxation on sugary drinks, smoke free public places, age limits on alcohol consumption, etc. Hence there should be focus on overall health in LHS. 15 To appropriately use this comprehensiveness in Canada, a recent framework described four elements characterising LHS, wherein (i) participatory leadership, inclusiveness, scientific rigour, person-centredness, equity, solidarity form the ‘core values’, (ii) infrastructure and resources are the ‘pillars’ and the specific structures that enable more rapid learning and improvement are the ‘accelerators’, (iii) the pillars support the fundamental ‘processes’ of execution, routinisation and acceleration of learning cycles, which in turn seek to (iv) strike an optimum balance of enhancement patients and providers experiences enhancement, population health and health system costs as ‘outcomes’. 17
There are several approaches to LHS. Some are built around clinical registers with harmonised data to describe populations with specific diseases or characteristics and monitor their outcomes such as the Swedish Rheumatology Quality Registry, 18 ImprovingCareNow, 19 National Platform for Rare Diseases Data Registry of Japan (RADDAR-J); 20 some based on EHR systems such as Optum Labs, 21 CancerLinQ, 22 Geisinger Health System (GHS); 13 some based on patients’ personal health records such as Scalable Collaborative Infrastructure for a Learning Healthcare System (SCILHS); 23 research databases such as the Northwestern University Clinical and Translational Sciences (NUCATS) Institute; 24 Prescription of Genetic Testing in the Gynaecological Cancer Risk; 25 centralised data warehouses such as TRANSFoRm, 26 EHR4CR; 27 in smaller geographies Group Health Co-operative in Seattle, 28 Comparative Effectiveness Research Translation Network (CERTAIN) in Washington, USA; 29 themetically linked network at larger geographies such as the paediatric research network PEDSnet; 30 part of national strategies such as US National Patient-Centred Outcomes Research Network (PCORnet), 31 England’s Academic Health Science Networks.32,33
Although LHS frameworks have been available since the concept of LHS was introduced in 2007 with several instances of existing LHS (mentioned above), yet but there are still very few reports of LHS being implemented. This is especially surprising since research groups were working on health data reuse much before that. A review in 2016 found only 13 publications on LHS implementation results from ten research intiatives. 34 They reported three directions of LHS implementation: (i) clinical data reuse,19,22,23,26,29–31,35 (ii) patient reported outcomes,36,37 (iii) collaborative learning-oriented. 38 The learning and innovation in LHS could be accelerated with the use of algorithms, machine learning, data mining and advances in artificial intelligence. 39
Scotland is well positioned to achieve a LHS since it has rich data assets across the lifespan of the population, with an unique patient identifier. This enables linking patient records across healthcare; and has policy in place to integrate healthcare, social care and administrative records.40,41 Providing personalised healthcare is dependent on the ability to access data across primary and secondary healthcare, social care and administrative records in near real-time to support clinical decision making. 41 Electronic health records (EHR) have facilitated the development of LHS by provisioning repurposing of clinical information to support quality improvement, research, population health and health system analytics. 42 One of the aims of LHS is personalisation of healthcare interventions. Inputs from patients on their reported symptoms, goals, expectations and outcomes could help to interpret and better understand the ‘patient data shadow’ already extant in EHRs and contribute to personalised care, improve accuracy of prediction models and improve the quality of clinicians’ decision making.43,44 These could be addressed through innovative approaches in the LHS towards continuous improvements in quality, safety, outcomes, and health care efficiency. 45
The NHS National Programme for IT (NPfIT), one of the most ambitious projects undertaken in UK public sector, costing approximately £10 billion, collapsed due to the lack of end-user engagement and public trust in care.46,47 Furthermore, there had been several NHS data breaches that have made the public wary.48–59 This has led to a risk averse culture which does not sufficiently consider the risks of not using data for public benefit and slackens the LHS agenda in all over UK.51,60
NHS Scotland operates through 14 regional NHS Health Boards which have overall responsibility for the health of their population. These 14 Health Boards are supported by seven special Health Boards which operate nationally. All of these Health Boards have their own information systems and information governance (IG) processes across primary, secondary and social care. Within and across regions these information systems and IG are rarely integrated for continuum patient care. These create the challenges for accessing data within/across regions.
We sought to understand the barriers to and opportunities for exploiting NHS Scotland’s increasingly digital infrastructure to continuously enhance healthcare provision and health outcomes.
Methods
Study design
We conducted a qualitative study in Scotland, using semi-structured interviews with a guided questionnaire across the data lifecycle and convened a round-table discussion, exploring attitudes relating to perceived barriers and facilitators for accessing patient data, mitigation approaches and implications for practice and policy.
Sampling and recruitment
Policymakers, health service managers, healthcare professionals (HCP), academics and analysts were contacted individually. Purposive and snowball sampling were used, that is participants with knowledge of the NHS Scotland information systems landscape and dataset(s) or who were instrumental in decision making roles from the NHS, Scottish Government and academia were targeted and they were asked from whom we could get further insights. 61
Data collection and handling
The study period was May-December 2017. The round-table discussion was carried out in November 2017, informed by the initial analyses. All participants were invited to the round-table. Participants were interviewed face-to-face at The University of Edinburgh or over the telephone in closed rooms in respective workplaces between September-November 2017. One interview had two participants from the same team. Interviews were informed by topic guides (Appendix 1), which were trialled on two individuals, one clinical academic and another non-clinical academic. The interviews explored current mechanisms of accessing data, the current information systems, the challenges faced in accessing data, potential facilitators, and international examples of excellence. Interviews were digitally recorded and transcribed verbatim by a professional transcriber. Interviews continued until thematic saturation was reached (i.e. no major new themes were emerging). 62
Data analyses
The framework approach was used and the seven procedural stages for thematic analyses of qualitative data were followed.63,64 In the first two stages, after transcription of audio files, which was supplemented by researcher field notes, we familiarised ourselves with the data by reading the transcripts repeatedly and making notes. In the third stage, we coded interview transcripts inductively with the help of QSR NVivo 11 software in an iterative process of attributing labels to small sections of meanings within the interviews, moving back and forth and comparing data and labels. In the fourth stage, the analytical framework moved into development phase by grouping into logical and meaningful categories nested in a hierarchical tree structure, much aided by Nvivo (Appendix 2). An ‘other’ category had existed at that stage, which primarily referred to innovations, exemplars, government directives, etc. A combination of deductive thematic analysis, informed by the literature on harnessing information systems to improve patient care,65–74 LHS,4,6,9,10 data privacy legislation,75–77 and public policy,78,79 and a more inductive iterative approach that allowed new themes to emerge from the data were used. 80 In the fifth stage, we applied this analytical framework to code further transcripts. To allow emerging findings to inform subsequent interviews, analysis was undertaken on an ongoing basis. In the sixth stage, the categories were charted into a framework matrix forming sub-themes. After an internal review of the findings, the initial findings were reported to the participants of the round-table. Input from the round table was coded. The two data sources were integrated at the participant level. In the final stage, themes relating to the aims of the study were developed to provide a larger meaning and recommendations through identifying commonalities and differences between different stakeholder groups, and by testing relationships between different parts of the data.63,64 In relation to reflexivity, the research team considered their own backgrounds and potential biases and tried not to allow their preconceived notions to colour the interpretation of the data.81,82 Before writing this paper, a short report on the findings and interpretations was submitted to the funder.
Reporting
The COREQ (COnsolidated criteria for REporting Qualitative research) and STARE-HI (STAtement on Reporting of Evaluation studies in Health Informatics) guidelines have been used to guide reporting.83,84
Results
Of the 68 people who were approached, 40 people agreed to be interviewed (58%). Interviews were carried out with 37 individuals with three individuals unavailable for interview during the study period. There were 11 face-to-face interviews and 26 over telephone. The average duration of the interviews were 39 (minimum 21, maximum 57) minutes. Characteristics of the 37 participants are presented in Table 1. At the round table there were 17 participants (46%), of whom two joined by tele-conference.
Characteristics of participants.
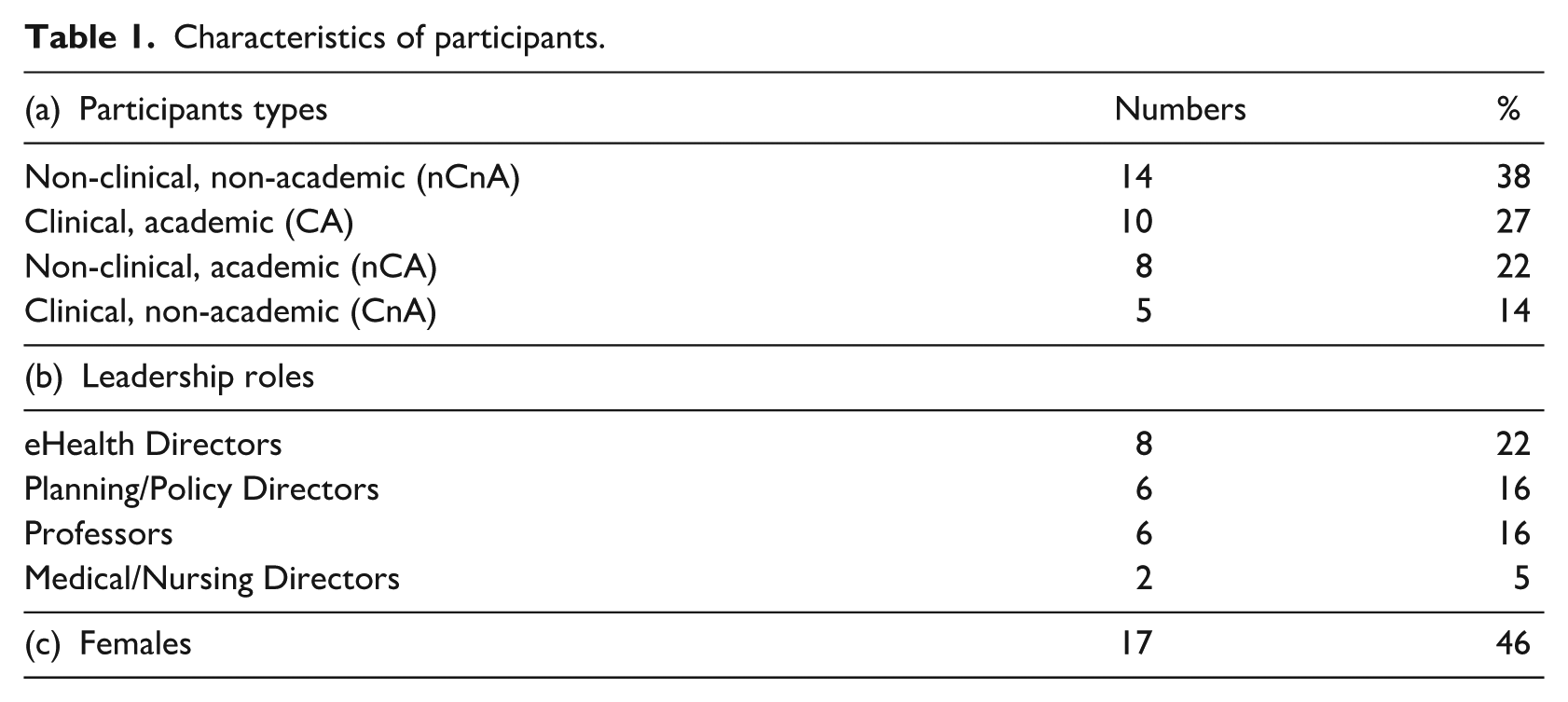
The participants who were not covered under the leadership roles were information analysts, research fellows, PhD students, clinicians in primary and secondary care, pharmacists, nurses, service managers, project managers, quality & safety assurance managers, research and development managers and data safe haven managers.
Syntheses
There were 121 codes/labels identified from the interviews, presented in the right column in Appendix 2. These labels were grouped into 37 categories, which were further grouped into 13 interrelated sub-themes (Appendix 2). The above mentioned process of refinement resulted in a final set of three main themes: (i) persistence of paper-based records and a variety of information systems, which in many cases lacked interoperability; (ii) the need for a standard, proportionate approach to managing IG; and (iii) the need for support structures to facilitate accrual, processing, linking, analysis and use and reuse of data for patient benefit. Codes which were closely related but constituted a different theme, were moved to the more pertinent theme, though keeping a note for the former theme. For example (a) ‘Understanding of what a data field means is different from what people put in’ was moved from theme iii to ‘Meaning of a data field means different things to different people’ in theme i, (b) ‘Researchers should be able to find and explore data from Safe Havens before writing grant or ethics applications’ was moved from Safe Havens to Virtualisation under ‘Researchers should be able to find and explore data before writing grant or ethics applications’, since the latter came earlier in the matrix and covered more than Safe Haven data. For each of the themes, respective sub-themes with quotations are presented in Tables 2 to 4 below each theme, with additional quotes by sub-themes and categories in Appendices 3-5.
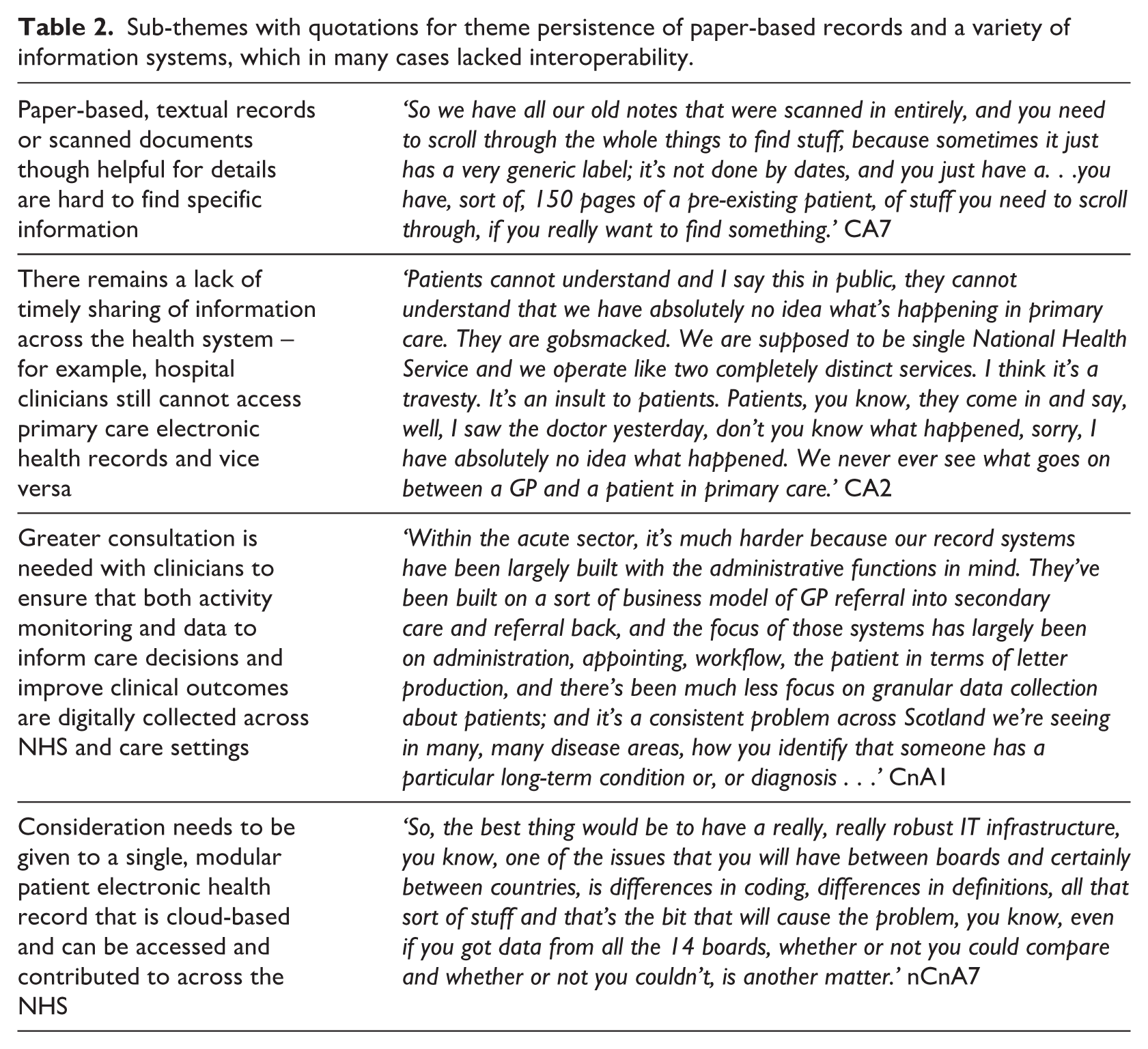
Sub-themes with quotations for theme persistence of paper-based records and a variety of information systems, which in many cases lacked interoperability.
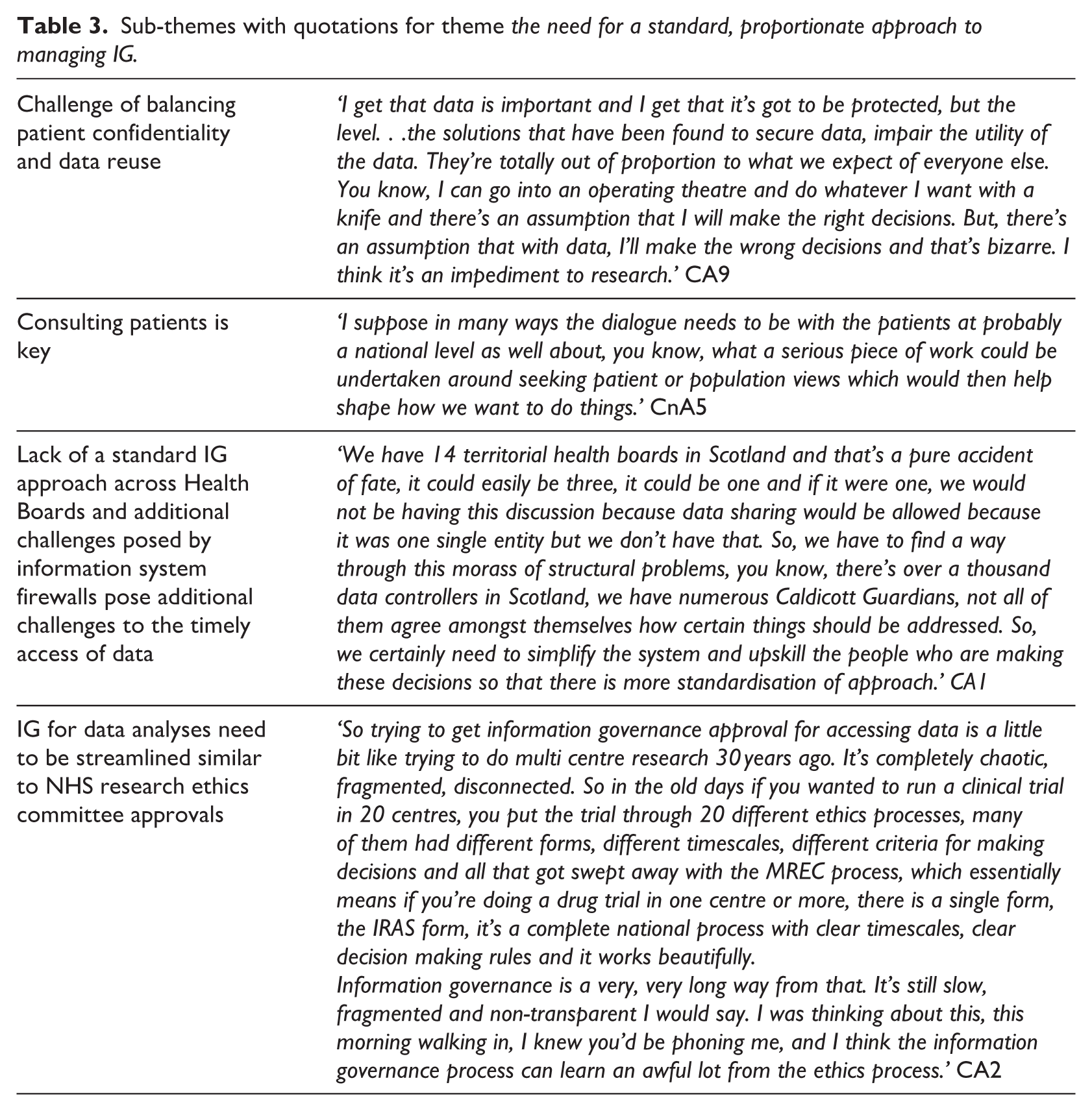
Sub-themes with quotations for theme the need for a standard, proportionate approach to managing IG.
Sub-themes with quotations for theme the need for support structures to facilitate accrual, processing, linking, analysis, use and reuse of data for patient benefit required.
Clinical notes in hospitals were mostly either handwritten on paper by clinicians or typed electronically by secretaries, with delays in coding after patients were seen. Handwritten notes were often scanned in, resulting in several pages of electronic documents, which were time consuming to access by clinicians during a patient consultation and resulted in ineffective use of clinician’s time. Clinicians reported that text-based records were helpful clinically; in contrast, scanned notes made it hard to rapidly find specific information.
Participants who worked in the NHS reported that information was stored in different information systems provided by different commercial providers on different aspects of care within/across Health Boards. These information systems remained as separate entities due to their different technologies, layouts, data structures, versions, application programming interface (API) and firewalls that prevented integrating patient records across all systems. Furthermore, different Health Boards and care providers considered themselves responsible for the upkeep of patients’ data and obtaining multiple agreements across multiple providers rendered data sharing challenging. Mainly NHS participants reported there was lack of willingness, leadership and collegiality to think and develop beyond local or disease-specific systems, to a national system.
Most participants reported lack of sharing of information across the health system, for example, many hospital clinicians were unable to access primary care electronic health records and vice versa. Clinicians unanimously vocalised that near real-time data were needed for personalised data interpretation across primary, secondary and social care to facilitate better individualised care and would help to generate quality performance indicators which are helpful for the decision makers. Interestingly, health informatics departments of a few Health Boards reported that near real-time patient administration data were available to them from within minutes to a few days after data entry into hospital information systems, but in some Health Boards coding of data could take up to 6 weeks, which delayed the entire national process.
Frustration was shared by clinicians that information systems are bestowed on them from Health Boards, without them being consulted, for business administration purposes, with good digital records on number of patient referrals, appointments, procedures carried out etc., but not with clinicians or patients in mind: since there were significant gaps in recording of granular data for example, diagnoses, outcome, thereby diminishing the quality of care provided to patients. Clinicians reported that unless Health Boards are mandated to record more clinical information they will not do so. Thus it would be helpful if there was intervention from the Scottish Government to address this issue. It was stated that greater consultation was needed with clinicians on what features they need in an information system, to ensure that both activity monitoring and data to inform care decisions and to improve clinical outcomes are digitally collected across the care settings.
Participants reported that differences in organisational culture, knowledge, specialities or hospitals, resources available, motivation, etc. affect the maturity and usability of an information system. Thus, it was suggested that data standards could be developed across specialities, based on inputs from highly interested teams who know their data needs. These could be scaled up for standardising clinical documentation and clinical practice, as was done for the Scottish Diabetes Network. 85 It was believed that such a convergence drive is needed nationally for interoperability and for reducing variability and inconsistencies between systems. Interviewees suggested that priority needs to be given to (i) identifying data items that are important to share, (ii) integrated systems targeted first to areas/specialities of highest need, (iii) including systems which were currently excluded in the integrated system, for example radiotherapy, chemotherapy, creating new ones, example hospital prescribing and improving current ones example adding diagnoses data in outpatient clinics data. Interviewees highlighted that consideration needs to be given to a single, modular patient electronic health record which can be accessed, and contributed to, across the NHS. The operations of the national sexual health system (NaSH) was mentioned as a good example to demonstrate that near real-time data access was possible when prioritised by national and local policymakers. 86
Regarding data sharing, almost all interviewees thought that there was risk aversion by data custodians, which ranged from preventing outright sharing of data to instituting numerous approvals and checks to greatly restrict access to data. Clinicians interviewed noted that there was potential for more harm to patients by not sharing their data at the appropriate level needed for patient care. They argued that patients would not be happy to find that their data were inaccessible to clinicians in other parts of the NHS. Researchers thought that data usage cannot be labelled as for ‘secondary use’ since it is for patient’s benefit and thus such distinctions were redundant. Data custodians in the study were keen to share data using innovative ways by shielding identifiable information. All researchers felt that the IG process was the biggest barrier, describing it as bureaucratic and slow, that it kept on being reinvented and renamed but the actual processing of applications did not get any better. NHS Safe Havens asked researchers for information on data curation, access procedures, data security measures in work place etc., which the researchers often had to find out from their employer’s IT department. This slowed down the application process and delayed submission of applications. A few researchers reported that it took them up to 2 years to get IG approval, whilst others reported that their study either changed or could not be delivered due to IG strictures. A majority of interviewees thought that the people who made decision on data access do so on imagining what the patients would like, but had never asked the patients. Suggestions were to consult patients using sampled focus groups, giving them honest information on the benefits and downsides of sharing data.
Some opined that whilst differences in IGs seem to hinder interoperability of information systems across/within Health Boards, these were manifestations of different technologies, vendors, firewalls and APIs of various information systems in use. Thus, besides IG, there needs to be discussions on information systems in place. Having a single information system framework across the country was repeatedly voiced by many participants. Towards interoperability, requirement of data standards was strongly recommended.
Some interviewees stated that conducting clinical trials on patients was risky yet getting permission to do trials had been streamlined, whereas doing population analytics using historical data was far less risky, but the IG for this was convoluted. Researchers thought that the current national IG panel decisions were not transparent to help researchers write better applications or for others to be guided by previous applications. It was thereby suggested that to streamline the IG process, it has much to learn from clinical trial processes and need to develop a similar integrated approach across Health Boards to reduce variation and avoid roundabout decision making. The approach needs to be agile, responsive and less resource intensive.
Numerous researchers questioned the research fitness of the data collected in secondary care, since sometimes they either had to design their study based on the data available or create a new study database when data were not available. But researchers reported that doing the latter was difficult since there was either no collective pursuit or there was resistance to create a new database or use a database which was unknown to the Safe Haven team. The common refrain was that researchers could have had more useful data if the data accrual process was informed and shaped by the articulated needs of data users. Thus, a data lifecycle approach in managing information was suggested, starting from specifying requirements at an early stage through to retirement. Most participants reported that what was needed was to pull data from different sources to one single data warehouse with adequate metadata. But such good data science exemplars should be disease specific and should be replicated across all places for that specific disease, as opposed to a one system for all diseases. Some participants reflected that there is need to think beyond data maintenance and analyses to understand the data and the processing involved, extract the value that is potentially obtainable, and disseminate findings also through visualisations and communicate back to the information system any feedback obtained in the process, so as to help develop and mature the patient information system. For example, although predictive models are available for high risk patients in Scotland, they are not adequately used by HCPs and patients are rarely aware that they are at high risk. Participants believed that the technology required was available, but the staff required to think through these myriad of obstacles and deliver ‘a system’ was currently lacking. It was mentioned that resources are needed to modernise the existing infrastructure, with additional spend to achieve changes. A network of people who can be called upon to help drive the information systems agenda forward was required. A dedicated paid time post needs to be given to individuals in this network who are tech-savvy, can liaise with people across Disciplines and who can create and nurture those relationships to translate their key information requirements as deliverables.
It was also reported that the level of knowledge required to fill the governance forms was sometimes not adequate for research managers in clinical teams and thus further help were required from data stewards who know the information systems, IG and the data, but such people were rarely available. Members involved with IG mirrored this view, when they opined that delays in a decision from governance panel could be because the application was not written appropriately in the first place by an experienced researcher or because of lack of time due to shortage of staff who review applications. Recognising the importance of data stewardship roles in research studies, which were largely invisible currently, was thought to be paramount.
Several interviewees suggested that trusted researchers could be fast-tracked with data access, or that if a competency framework could be created for data access to attain trustworthiness. Experienced researchers would find it helpful if they are as trusted as NHS Safe Haven employees and accredited periodically. All researchers would like to use data virtualisation of patient’s data hosted in NHS network for an initial insight for their study, by logging in remotely, using a query programme, wherein NHS has put in adequate measures to restrict extracting information that potentially should not be disclosed. That could speed up research and potentially save resources. There was also a recommendation for funders to adequately fund the development and maintenance of metadata, to facilitate greater understanding of the data.
Discussion
Main findings
This work has found that whilst there is considerable appetite to make better use of the data continuously generated by the NHS in Scotland, there are major barriers that prevent these data from being used in near real-time to drive forward service improvements. Key amongst these are the need to complete digitisation of the healthcare landscape, to develop standard data approval and management processes and the need to enhance technological and human capacity and capabilities to exploit these data for patient and public benefit.
Strengths and limitations
The key strengths of the study included the purposive sampling of a range of stakeholders from across Scotland, the fact that many of those recruited were in leadership roles with an appreciation of the opportunities for transformation of care provision, and the fact that we undertook iterative analysis and continued recruitment until we achieved saturation.
The main limitations were that we did not sample IT vendors or patients/carers and that the findings may not be transferable to the NHS in other UK nations or other health systems.
Integration with the current literature
The National Data Guardian’s report in England found that safety of care can be improved by better sharing of information across health and social care, that de-identified data are beneficial to commissioners, planners and researchers, and the case for data sharing needs to be made to the public. 76 Recent government reports have emphasised building interoperable information systems with user needs, giving improved access to data at point of care to health professionals, giving people more information about their care and data, considering multi-disciplinary care, building an ecosystem that supports researchers and innovators and building digital savvy workforce to support the initiatives,65,66,78,79,87,88 example Scotland’s National Digital Platform. 79 Our study also echoes with findings that essential local needs need to be prioritised and the key activity during implementation of both standalone and multi-modular systems should be information integration whilst maximising clinical benefit.67,74
Towards creating a LHS, participants voiced need for a common platform to collate, aggregate, link, protect, anonymise, analyse data to act on, with adequate metadata, with real-time interaction enabled with HCPs to make patient care better, enhance current data quality by adding data items currently missing for example, hospital prescribing, patient outcomes and include more details for example, diagnosis data in outpatients clinics, wherein data custodians can secure the data such that trusted analysts and researchers too can access near-real time data. A contemporary study in England also reported that data quality and accessibility as barriers to creating LHS. 33 Our study also found that a one-system might not suit all, thus there need to be disease-specific or local LHS exemplars. Current endeavours which are disease specific example BREATHE for respiratory diseases and local examplars example DataLoch in south-east Scotland are efforts towards this.89,90 But these are towards creating the infrastructure for a LHS. Since LHS is about health and not just healthcare, 16 the study found that there should also be scope for patients to add data that they think is important for their health. Registers of patients’ whether disease specific, example REACH for asthma or for all diseases, example SHARE, are moves towards patients being consulted to share their EHR.91,92 If a system is to be developed from scratch, studies found that it should be patient centric and HCPs should be consulted at an early or design stage.17,93 There was suggestion to move to a single information system framework across the region, through Open Data which requires the collection of standardised data that can be easily aggregated or harmonise existing data, towards deliberations for centralised definitions of systems and data items.93,94 Sharing of data and easy modes of communication were also suggested amongst HCPs and/for/with patients, so that decisions are not made based on piecemeal information and patient care is not fragmented. 95 A national study also found that information governance policies were found to be a hindrance to information sharing amongst HCPs and research purposes and suggested if local healthcare teams establish their own patient privacy procedures. 93 Requirement of a lead agency for cross-sectoral data linkage was suggested, which initiatives like Health Data Research UK (HDR UK) are suitably placed to address. 96 Besides training people, the importance of paid time and recognition of tech-savvy researchers/HCPs and data stewards who can bridge the gap between knowledge to practice and practice to data were also mentioned. 39
Implications for policy, practice and future research
There is a need to better understand our data assets to be able to enhance their usability and address the roadblocks in IG. Efforts have been put in place to improve the accessibility of data through initiatives such as the Scotland’s National Digital Platform, NHSX in England and Health Data Research UK’s Alliance, Innovation Gateway and Digital Innovation Hubs (HDR UK DIH), working on FAIR (Findable, Accessible, Interoperable, and Reusable) principles. 97 These are some very encouraging initiatives in the UK, which could accelerate digital transformation, progress in medicine and health and data reuse.79,96,98 To encourage good practice, we need to identify key user cases which can demonstrate innovative use of data, which could potentially lead to digital transformation. Some of the innovative data users are the HDR UK DIHs from specialised clinical/research areas, 89 as aspired by study participants. For future research, we need to add value to the existing and yet-to-be identified data assets before these can be scaled up to other areas.
Conclusions
The persistence of paper-based systems and the lack of pan-Scotland interoperable information systems and IG arrangements are major barriers to move towards creating a national learning health system. These challenges are compounded by the limited technical capacity to process, integrate, visualise, interrogate and use data to drive forward transformational change. There is a need to progressively replace paper-based systems with electronic health record infrastructures, move to a nationwide proportionate IG approach, decide whether a central data warehousing or a more federated approach is to be pursued across Scotland, and to invest in technical and human capabilities to make maximal use of Scotland’s rich data assets to enhance health care delivery and research across Scotland.
Supplemental Material
sj-docx-1-jhi-10.1177_1460458220977579 – Supplemental material for Identifying strategies to overcome roadblocks to utilising near real-time healthcare and administrative data to create a Scotland-wide learning health system
Supplemental material, sj-docx-1-jhi-10.1177_1460458220977579 for Identifying strategies to overcome roadblocks to utilising near real-time healthcare and administrative data to create a Scotland-wide learning health system by Mome Mukherjee, Kathrin Cresswell and Aziz Sheikh in Health Informatics Journal
Supplemental Material
sj-docx-2-jhi-10.1177_1460458220977579 – Supplemental material for Identifying strategies to overcome roadblocks to utilising near real-time healthcare and administrative data to create a Scotland-wide learning health system
Supplemental material, sj-docx-2-jhi-10.1177_1460458220977579 for Identifying strategies to overcome roadblocks to utilising near real-time healthcare and administrative data to create a Scotland-wide learning health system by Mome Mukherjee, Kathrin Cresswell and Aziz Sheikh in Health Informatics Journal
Supplemental Material
sj-docx-3-jhi-10.1177_1460458220977579 – Supplemental material for Identifying strategies to overcome roadblocks to utilising near real-time healthcare and administrative data to create a Scotland-wide learning health system
Supplemental material, sj-docx-3-jhi-10.1177_1460458220977579 for Identifying strategies to overcome roadblocks to utilising near real-time healthcare and administrative data to create a Scotland-wide learning health system by Mome Mukherjee, Kathrin Cresswell and Aziz Sheikh in Health Informatics Journal
Supplemental Material
sj-docx-4-jhi-10.1177_1460458220977579 – Supplemental material for Identifying strategies to overcome roadblocks to utilising near real-time healthcare and administrative data to create a Scotland-wide learning health system
Supplemental material, sj-docx-4-jhi-10.1177_1460458220977579 for Identifying strategies to overcome roadblocks to utilising near real-time healthcare and administrative data to create a Scotland-wide learning health system by Mome Mukherjee, Kathrin Cresswell and Aziz Sheikh in Health Informatics Journal
Supplemental Material
sj-docx-5-jhi-10.1177_1460458220977579 – Supplemental material for Identifying strategies to overcome roadblocks to utilising near real-time healthcare and administrative data to create a Scotland-wide learning health system
Supplemental material, sj-docx-5-jhi-10.1177_1460458220977579 for Identifying strategies to overcome roadblocks to utilising near real-time healthcare and administrative data to create a Scotland-wide learning health system by Mome Mukherjee, Kathrin Cresswell and Aziz Sheikh in Health Informatics Journal
Footnotes
Authors’ contribution
AS conceived the study and was the PI. MM conducted the study, analysed the data and wrote the drafts. All authors reviewed the drafts.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Chief Scientist’s Office of the Scottish Government (CGA1704). MM’s time to write the paper was supported by Health Data Research UK, which is funded by the UK Medical Research Council, Engineering and Physical Sciences Research Council, Economic and Social Research Council, Department of Health and Social Care (England), Chief Scientist Office of the Scottish Government Health and Social Care Directorates, Health and Social Care Research and Development Division (Welsh Government), Public Health Agency (Northern Ireland), British Heart Foundation and the Wellcome Trust. KC is funded by Chief Scientist’s Office of the Scottish Government.
Ethics and permissions
We sought relevant permissions from all Health Boards across medical, nursing, public health and eHealth directorates and obtained permissions from eight Health Boards and the Public Health Scotland (till recently known as Information Services Division (ISD)) Scotland. We obtained individual informed consent from all participants and anonymised their data to maintain confidentiality. All participants returned the consent form prior to the interview.
Data availability
The interviews, transcripts and datasets generated and analysed during the current study are not publicly available due to confidentiality of the provided information and in order to protect study participants’ privacy and anonymity but may be available from all authors on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.