
Abstract
Emerging adults have been raised in the digital age and are therefore prime candidates for using a patient portal to manage chronic conditions. The limited body of research both identifies the underutilization of the patient portal and suggests increased use of the portal for the chronically ill as a tool to alleviate caregiver stress, as well as a potential modality to assist emerging adults to manage their chronic illnesses. This qualitative study was completed to obtain an understanding of emerging adults familiarity with the electronic patient portal and to elicit the perception of the usefulness of the portal to support self-management of type I diabetes. Findings provide a preliminary understanding of how a sampling of emerging adults with type I diabetes uses, perceives the benefits of, and wants to improve technology for diabetes self-management.
Keywords
Introduction
Transition from pediatric to adult care between ages 18 and 30 years, which is also called emerging adulthood, requires emerging adults (EA) to start taking primary responsibility for key tasks associated with adulthood. It is a high-risk period for EAs with chronic disease, that is, type 1 diabetes mellitus (T1DM) since the transition is generally from a multidisciplinary, family-based approach to care, with long-standing relationships, to a decentralized approach.1,2 Although patient portals are increasingly common, there is little information regarding their use in this transition to engage EA patients, caregivers, and the health-care team as partners in EA care. The limited body of research, conducted primarily in academic health-care settings among parents of children with chronic conditions, both identifies the underutilization of the patient portal within the pediatric population and suggests increased use of the portal for the chronically ill may be a mechanism to alleviate caregiver stress, as well as a potential modality to help EA learn to manage their chronic illnesses.3–8 Considering EA familiarity with daily electronic communication on mobile devices, it is reasonable to assume that the portal provides a viable opportunity to engage this vulnerable patient group in the health-care system. Digital technology is an appealing and relevant modality,9–11 although the deployment of portals has occurred with limited patient involvement, especially with EA. 12 This qualitative study was designed to explore EAs’ patient portal knowledge, perceived barriers, and successes, with the goal of improving EA portal access and engagement in chronic disease self-management.
Background
Children with chronic illnesses are experiencing fulfilling and extended life spans; 1 nonetheless, the transition from pediatric to adult care is a high-risk period for EAs with chronic disease.2,13 Health-care transition for individuals with complex conditions has been identified in Healthy People 2020 public health goals, as a high priority for action and transition planning.14–17 Technological applications may provide needed monitoring and support systems as EA makes this transition with the opportunity to go online to medically sound resources rather than exclusively having to speak to a provider.1,18–20 Adding the ability to communicate electronically with health-care practitioners may be of substantial benefit. An integral first step is EAs with T1DM have stated that they are willing to share personal information about their condition. 21
The Society for Adolescent Health and Medicine 2003 transition statement proposed identification of transition coordinators who reach out to adolescents using multiple technologies, including telephone, text messages, and social media.22,23 Huang et al. 24 argued that the portal provides a one-stop electronic location for scheduling, communication with providers, and an opportunity to begin to develop independent disease self-management as part of the transition from pediatric to adult-oriented care system. Most health-care systems have the needed technology infrastructure, but are poorly prepared in the one-on-one care needed for EAs to transition into receiving continuity-of-care into adulthood. 22 One of the limitations to providing access has been the challenge of children maturing, requiring updated data feeds to the portal ensuring both easy and appropriate access, while maintaining confidentiality and privacy for both adolescent patients and their parents.6,25–28 To ensure all EAs are able to use the portal, access disparities among those with fewer resources, less education, low health literacy, and who are already ill must be addressed.29–32 Prior to designing and implementing strategies to ensure portal use, the purpose of this study was to gather qualitative information to gain a preliminary understanding of EA familiarity with the electronic patient portal and to elicit their perceptions of the usefulness of the portal to support self-management of T1DM.
Methods
This study used a qualitative design via individual semi-structured interviews (see Appendix 1), lasting 35–55 min, to gain an understanding of EA familiarity with the electronic patient portal and to elicit their perception of the usefulness of the portal to support self-management of chronic illness, specifically T1DM. All study procedures, including protocols for recruiting participants and obtaining informed consent, were reviewed and approved by the appropriate administrative and university Institutional Review Boards for the protection of human subjects prior to study initiation. All participants provided written informed consent prior to participation in the interview.
Participants were recruited through two channels. First, a purposive sample of young adults volunteering at a day camp for young people with T1DM in San Diego County during the summers of 2016 and 2017 was identified. Second, additional snowball recruitment took place among friends and acquaintances of the research assistant (RA) for the study. The RA is a type 1 diabetic and reached out to her own networks through word of mouth and social media. All participants were required to be English speaking and aged 18–26 years.
Data were collected through individual semi-structured interviews, comprising questions developed by the primary researcher based on a review of patient portal and transitioning literature. With the goal of understanding how EAs with T1DM learn about and use the portal, an interview guide was comprised of questions developed by the primary investigator (PI) based on a review of patient portal and transitioning literature. The interview guide focused on the following four areas: (1) how the patient learned about the portal, (2) the type and frequency of their portal use, (3) how they are using the portal to manage their health, and (4) what changes and modifications they would like to make to the portal. Before the interview, participants listened to an explanation of the study, were instructed to answer questions openly and honestly, and told they could skip any question. The open-ended questions were designed to encourage participants to describe their experience with a patient portal system, as well as feedback about potential modifications. Interviews were conducted both in-person and over the telephone by the PI and the RA (data collection team).
Data analysis
Each interview was transcribed verbatim and then independently analyzed by two of the investigators (R.A.B. and K.K.M.) to identify themes that emerged from the transcripts. Digital recordings were transcribed verbatim by a professional transcriptionist. All transcribed recordings were then compared to the digital recording to ensure accuracy. Identifying information (i.e. names of people or places) were removed while the recordings were checked for accuracy. The coding process began with two independent researchers highlighting exact words from the text that appeared to capture key thoughts or concepts during line-by-line review. The two researchers then established preliminary themes. A third researcher reviewed the initial codes and themes, aggregated themes into categories, and created a codebook. The preliminary codebook and transcribed interviews were reviewed by the lead investigator. After her review, all themes were approved and no additional consistency checks were required. Four broad themes were identified.
Results
Participants
A total of 29 participants were enrolled in this study, with 27 completing the interview. Of the total participants completing the study, 19 self-identified as female and 8 self-identified as male. At the time of enrollment, seven participants were aged 20 years and another seven participants were aged 22 years. The remainder of the participants’ ages were between 18 and 25 years. No participants were aged 23 years. A breakdown of participants by recruitment channel is provided in Table 1.
Participants by demographic information and portal usage (n = 27).
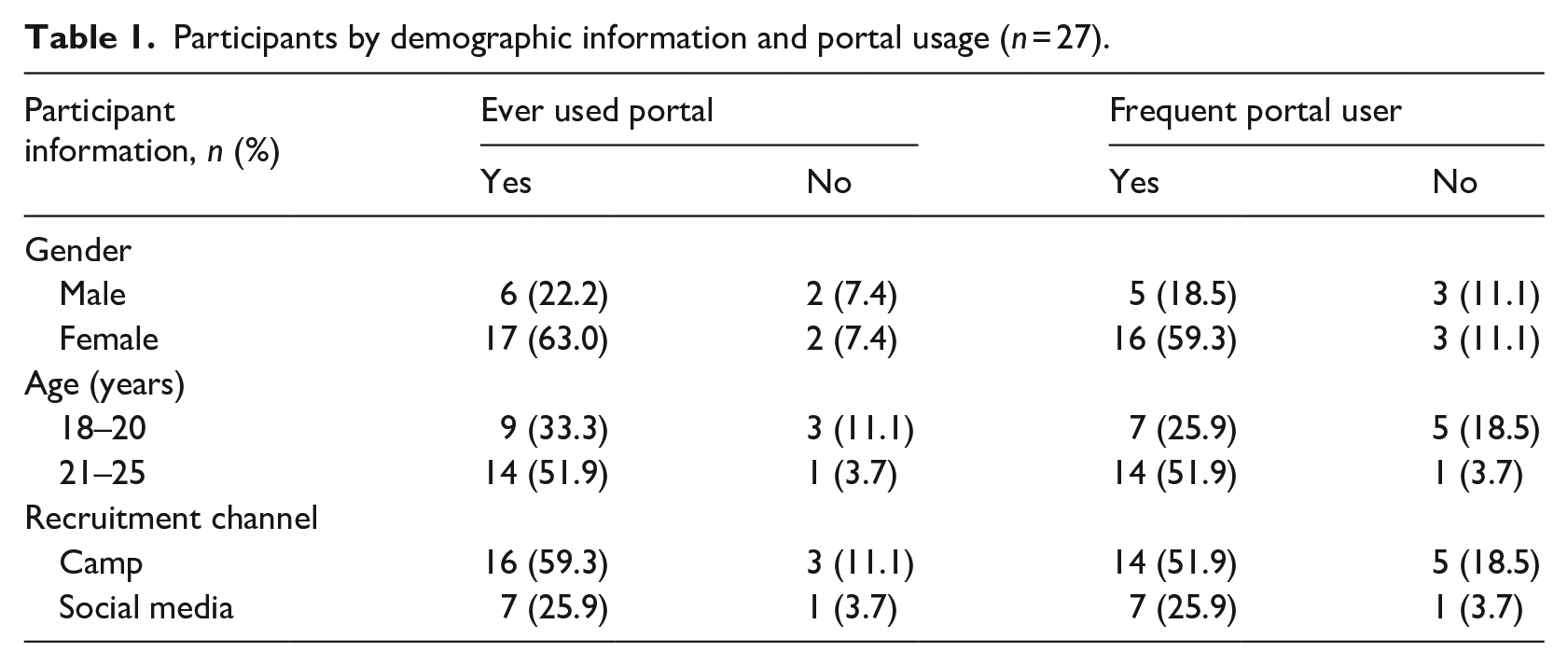
Participants typically obtained their health information from a variety of sources, including conversations with providers, printed materials, insurance company reminders, school, Instagram, and the patient portal. Twenty-three of the 27 (85%) participants reported that they have ever used the portal, and 21 (78%) participants reported that they were active users of the portal, which was defined by having used the portal greater than one time in the past 6 months. Since participants were recruited from community sites and social channels, as opposed to in-clinic recruitment, participants represent a variety of different health-care systems, and thus use a variety of patient portals such as MyChart or Kaiser’s patient portal.
Themes
Participants commented on a number of issues relating to their portal usage and using the analysis discussed in section “Methods,” the research team arrived at the themes presented in Table 2.
Counts of themes.

Health information is obtained via myriad of modalities
Twenty-three participants reported that they receive their health information from their providers (both physicians and nurse practitioners); others reported that they receive health information from their parents (n = 3), the Internet (n = 5), and using the portal (n = 8). Fifty-five percent of participants reported that they obtained health information from one or more sources, for example, using their health-care provider to obtain information in conjunction with using the portal to seek out information. Conversely, 45 percent reported that they only receive health information through one source. When a participant reported only having one source for health information, they specified their provider as the place they went for answers. It is important to note not all the participants who prefer to access health information through the Internet are using the portal. For example, one participant commented, I do a lot of research on my own via the Internet. Additionally, my NP (nurse practitioner) and I have in depth discussions about my diabetes when I go in for a clinic visit. (Participant 1, 19 July 2016)
Three participants (11%) also responded that they rely on their mothers for information about their health, although they are adults. Specifically, one participant commented, I am happy to receive information from my doctor, my NP, or my mom. I am really not ready to take on all that is needed to manage my health. Diabetes is a big deal. I need all the help I can get. Most people want to be on their own with their life at this age (22 years) but I have to say diabetes changes everything. If I didn’t have diabetes, I think I would be a lot more independent but quite frankly, I am worried about not waking up at night due to a low bs (blood sugar) and I need my mom to help me manage my diabetes. (Participant 2, 19 July 2016)
Participants (n = 15) also commented on the importance of using the portal to access health information ranging from general questions about their health to information about appointments, lab results, and prescription/supplies. One participant said, I use the portal system to message my doctor. I probably went in to talk to my provider more frequently in the beginning [of my diagnosis] but now, with my smaller questions, I’ll just send a message. Most often it’s not worth coming in for [getting the answers to my questions]. (Participant 12, 2 January 2017)
Given the age range of study participants, it is interesting to note that only one participant mentioned using social media or social networking platforms to obtain health information.
Participants would like a more comprehensive, user-focused health portal
When asked about how they currently use the patient portal or factors that would lead to increased portal usage, 20 participants indicated that they are looking for a platform that presents a more comprehensive picture of their health in concert with having the strategies to help them manage their care, rather than only being able to receive results from one doctor or only results about diabetes. These data suggest that patients want their health to be viewed holistically and not segmented based on provider, diagnosis, or illness. For example, I think I have the tools and apps I need. I use the Dexcom app, which is not through provider but helps me manage and view how I’m doing with my diabetic health. An “all in one app” where my doctor could view my Dexcom app may be helpful but if I want my provider to view my numbers from my Dexcom I can give him code that he can go to the Dexcom website and view my numbers for the past month or two months. I have never used this when emailing my provider but once a provider pulled up my numbers online while I was in the visit so she could check how I had been doing. If I have a problem and they could view it automatically that may be helpful. (Participant 6, 22 July 2016)
The critique that the portal only presents information related to their T1DM may indicate several different situations for the participants. One is the participants are seeing an endocrinologist who is not part of their primary care system so their portal only has specialty information. Another is the participants have not received a great deal of information about the portal and do not realize they have access to all of their medical information, not just the visits and data related to their T1DM management.
Two participants commented on how the portal could be improved to support a more positive user experience that could potentially lead to increased usage: I think it would be great if it could be even more user friendly. For example, I have to go in to the portal to see something is updated, I’d like it if there is a notification that I get when said test result comes in/uploaded [so I don’t have to check in as frequently when waiting for result]. It would nice if you saw provider that wasn’t your usual provider like urgent care that that information would be documented on my portal. Might be complicated to manage but that would be ideal if possible. (Participant 13, 16 December 2016) I tried the portal once and frankly, it was too confusing. I must tell you and am a big techy guy so if the patient portal is too confusing for me then it is too confusing for most people. (Participant 6, 22 July 2016)
The patient portal facilitates access to providers and medical history, which support diabetes self-management
The third and most commonly cited theme emerging from the data is the patient portal facilitates access to providers and medical history, which support diabetes self-management. The two features capturing EA portal users are the ability to view lab/health results and the ability to message with providers. The ability to message their health-care provider through the portal was mentioned 66 times by participants. Participants enjoy messaging providers with small questions because it helps them avoid calling their provider or making an unnecessary appointment. This feature may be particularly helpful for recently diagnosed patients because they can ask quick questions between visits and know they will receive an accurate and timely response: Overall, I really like it. For some things it is definitely easier to go in person-like if it is an issue that takes a lot of words to describe or need to show them something. But usually mine is the short one question type, so this [messaging/emailing] has made it a lot easier to get a hold of my doctors. (Participant 12, 2 January 2017)
Participants (n = 24) indicated that they value the ability to access their medical history, including lab results and notes from previous visits with their providers. Specifically, participants appreciated the ability to track test results over time so they can see changes in their overall health and diabetes management. For example, participants reported that they like to open the portal and see their previous HbA1c before they go to the provider again, so they can understand how their self-management has changed since the last visit. One participant also reported that the ability to view past lab results has empowered her to be more accountable for her health: I think I am more aware of my diabetes because of the portal. It makes me be more accountable. (Participant 23, 2 September 2017)
Participant 2 affirmed this notion of empowerment and accountability: I use the portal to check on my scheduled visits, as well as following up on different goals such as decreasing my A1C. It’s is really convenient to be able to see my A1C in a graph form. It kind of gives me a reason to work harder on my diabetes care. (Participant 2, 19 July 2016)
Participant 13 validated and expanded upon this sentiment by describing how the portal provided a critical step in their ability to take control of their health by making it easier to access their health results in a way they had not been able to before: Prior to the portal I didn’t know a lot about my results unless I went into the doctor’s office to ask directly. “I don’t really like being in the dark about my health care so I think the portal has really helped with that.” (Participant 13, 16 December 2016)
There is information asymmetry around existing technology
Twenty-four participants reported that they use other technology apps to manage their health, for instance, CalorieKing or MyGlu. They use these apps to keep track of carbohydrates and calories, and obtain answers about diabetes management, respectively. Nine mentioned that they are aware other technology exists, but do not have the time to look into using it or they had not heard of other technology from their provider. At least one participant shared an expectation that the provider had responsibility for being aware of available apps and disseminating this information to patients: There are a lot of good apps out there, but my doctor really doesn’t know about them. (Participant 29, 4 August 2017)
Another participant commented that her health-care team could do more to bridge the gap between offering tools to patients and educating patients on how to use them to access specific information: There really needs to be more information about the portal and how to transition from child to adult healthcare. Maybe a sign at the NP office or in the health center at college. (Participant 1, 19 July 2016)
These responses contrast to other participants who reported that they feel they have all the tools and technology needed to manage their own health: I have the tools at my fingertips to navigate my health. Durable medical equipment has my back, I have access to the care I need with my parents insurance . . . I like the Dexcom Facebook page as a community to post questions/concerns, tips, accessories parents use it for their kids etc. I don’t feel I am missing any technology—I feel complete and competent with what I got. (Participant 16, 9 May 2017)
These data suggest that all providers should take a more active role in educating patients on all tools and technology available to patients with chronic diseases. In addition, these data may indicate that providers need to receive training throughout their course of practice to ensure they are adequately skilled to advise patients on how to manage their health outside the office of the provider.
Discussion
Organizations ranging from the Institute of Medicine, Healthy People 2020, and Maternal and Child Health Bureau have published statements highlighting the vulnerability and urgency to implement comprehensive transition systems.15,16,33 Ideally, transition should be a process rather than a one-time transfer. 34 This qualitative study found that EAs obtain their health information from myriad sources, are interested in using technology to help manage their T1DM, and have had mainly positive but limited experiences with the patient portal, but do not appear to be part of a coordinated transition approach. In addition, participants raised issues about provider knowledge of and ability to share information about health apps and the portal as part of their clinical care.
The majority of participants were aged either 20 or 22 years and mainly female. Although a convenience sample, the participants in this study—EAs with a chronic condition making the transition from coordinated pediatric care to an adult health-care system—provide important insight into a key group whose attitudes and approach to transition are not well-documented. The knowledge gained contributes to the limited body of research exploring the role of the portal in this transition. 4 Given the majority of participants were volunteers at a diabetes camp, they are likely a sample of people with T1DM who have greater degree of health agency and increased capacity for self-management of blood glucose. As such, these participants’ ability and desire to interact with the portal may be increased.
With respect to portal usage, some EAs appear not to have sufficient understanding of information available within their records, while others appreciate the longitudinal ability to track their data over time, which empowers them to manage their health. This finding is particularly important, given that EAs often fall through the cracks in the health system during times of transition. If health-care providers and health systems can find ways to leverage technology to empower young people to play a more active role in their care, then perhaps this can lead to fewer EA falling out of care during a transition period. Participants provided concrete examples of the ways in which they interact with their own data. EAs also indicated that they expected to receive information about available technology from their providers, indicating an important modality for portal activation and retention. This study provides the framework to implement focused prospective approaches with more EA participants and providers to study the longitudinal impact of the patient portal on transitional care and clinical outcomes. Participants’ observations and suggestions were largely congruent with the recent Commonwealth Fund report indicating that effective care management programs used care coordination in combination with technology to target EA. 35
Despite the fact saturation of themes occurred within this sample, the study has several limitations. This was a convenience sample and did not represent geographical, racial/ethnic, or socioeconomic diversity. Important factors—including type of health-care coverage, having a primary care provider, and access to specialty providers—were not addressed. Specific types of patient portal, portal recruitment, or Internet access were also not explored. Despite these limitations, this qualitative research has been useful for generating preliminary hypotheses, and analysis of the use of the patient portal on enhancement of transition of care for emerging youth will need to be tested.
Conclusion
The purpose of this qualitative descriptive study was to gain an understanding of EA with T1DM knowledge of the electronic patient portal, whether they used the portal for self-management of their condition, perceived barriers, and suggestions for improved use. Structured interviews resulted in the emergence of the following four themes: obtaining health information from a variety of sources, limited portal use, desire for a more comprehensive portal, and expectations of provider responsibility for technology familiarity and dissemination. These findings indicate that technology could play an essential role in the needed continued attention to a successful transition from pediatric to adult care for individuals with a chronic condition.
This research provides a preliminary understanding for how a sample of EAs with T1DM uses, perceives the benefits of, and wants to improve technology for diabetes self-management. Further studies are needed to examine how improved technology can be integrated and standardized for transitions to adult care with targeted implementation.
Footnotes
Appendix 1
Author contributions
The authors alone are responsible for the content and writing of this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.