
Abstract
Non-communicable disease rates associated with being overweight or obese are rising. Technologies warrant consideration as weight loss interventions. Cloudtag’s® Onitor® Track, a dual-position wearable plus smartphone application, monitors energy expenditure and provides tailored exercise programmes. This research aimed to undertake an experimental study of 20 overweight and obese women using the technology; explore its feasibility and acceptability through interviews; and investigate its behaviour change techniques. The primary outcome was decreased body weight (kg) at 4 weeks. Secondary outcomes were body mass index (kg/m2) and waist circumference (cm) changes. 15 overweight and obese women took part. Results indicated weight loss (median 2.7 kg, p < 0.05) and waist circumference decrease (median 4 cm, p < 0.05), but attrition was high (60%). Users reported dietary changes but few activity adjustments. They valued feedback. 27 behaviour change techniques were identified. The Onitor® Track shows potential for weight loss in overweight and obese women, but further work is needed.
Background
Healthcare systems worldwide continue to struggle with the growing prevalence of non-communicable diseases (NCDs), which are associated with being overweight or obese. 1 Treatment is available through various complex weight loss interventions, although high-risk patients and those with co-morbidities are given precedence due to limitations in resources. 2 The National Health Service (NHS) interventions are often practitioner-led and target diet and physical activity behaviours. 3 A number of systematic reviews have identified these interventions as successful in achieving ~10 per cent reduction in body weight within 6 months, but their long-term effectiveness and sustainability is variable;4–6 most regain around 40 per cent of their lost weight within the first 2 years. 7
Wearable devices (fitness and activity trackers, smart watches and so on) paired with smartphone applications (apps) have been considered platforms for delivering weight loss interventions. 8 They allow users to track and self-monitor multiple health outcomes, such as physical activity levels, steps and walking distance, energy expenditure and intake (diet) and along with sleep pattern analysis. 9 The accompanying applications can provide behaviour change strategies, such as goal setting and feedback provision, often including social support via push notifications and social media platforms. 10 Although widely available and increasingly fashionable among the general population, 8 wearables and apps are not rigorously tested for efficacy, and their ability to adopt evidence-based behaviour change techniques (BCTs) to motivate people to improve their health has been questioned. 11 They are not explicitly marketed for weight loss but are often adopted by women (35–54 years)12,13 who want to lose weight. 14 While there is an emerging body of research, the small number of preliminary studies to date comparing wearable technology to standard behavioural interventions7,15–18 has produced various results, with their ability to modify diet and physical activity behaviours still in question. Moreover, there is an absence of qualitative research in this area, both in terms of feasibility and acceptability, which is required to understand which components of these technologies are most promising and/or successful in promoting weight loss, and why. 19
Cloudtag® has developed a test unit Onitor® Track, which is a dual-position wearable, alongside a smartphone/tablet application (not yet available to the commercial market), which self-monitors energy expenditure and provides a tailored exercise programme, suitable for any environment. 20 The Onitor® Track can adjust with the user’s goals and adapts based on their progress, providing personalised feedback, coaching and guidance to encourage user engagement. To our knowledge, the Onitor® Track test unit is the first of its kind to target weight loss explicitly and to incorporate an exercise plan into its associated application (app). This unique programme, along with its use of self-monitoring, could help individuals achieve their weight loss goals, increase user adherence and help reduce attrition rates commonly found in other technology-based studies.21,22
This study aimed to develop a preliminary evidence-base around digital health technologies, that explicitly address weight loss through using a wearable/smartphone application, incorporating a personalised exercise plan, and to generate hypotheses for further detailed research. The objectives of this mixed methods exploratory study were to (a) undertake an experimental study of 20 overweight women using the Onitor® Track test unit and app for a 4-week period; (b) explore the feasibility and acceptability of the Onitor® Track test unit and app among those overweight women; and (c) investigate the presence of BCTs within the Onitor® Track test unit, app and study, relate them to known drivers of behaviour change and establish which ones are identified and engaged with.
Methods
Design
The study utilised a mixed methods exploratory design, as identified in phase I – modelling – from the Medical Research Council (MRC) Framework (MRC, 2010) (Supplemental Appendix 1).
Participants received a 4-week weight loss intervention using the Onitor® Track test unit (wearable and app), which included a personalised exercise programme and supplementary diet advice. There was a group launch event for participants, during which baseline measures were taken and technical set-up and support established. A private Facebook (social media) group was available for the duration of the study period as a platform for social support and discussion and to access technical support. Group participation was optional. If participants wanted to join and/or post, they could. They could interact with each other or access researcher and/or technical advice if they had questions or concerns about the intervention. At 4 weeks, participants were invited back individually to repeat measures and for a semi-structured interview to explore their experience of using the Onitor® Track. The primary outcome for weight loss was weight decrease at 4 weeks. The University of Aberdeen College Ethics Review Board approved all procedures (CERB/2017/4/1460; 16 May 2017).
Sampling and recruitment
The aim was to recruit 20 participants in the Aberdeen area and to invite them to a launch event (Supplemental Appendix 2). Individuals were eligible to attend the launch event if they were female; overweight or obese (body mass index (BMI) = 25–30 or ⩽30 kg/m2; waist circumference > 80 cm); 23 and aged between 25 and 54 years. Individuals also required access to an iOS Apple device (although a limited number were available to loan), Internet, USB power outlet and weighing scales. Exclusion criteria included significant weight loss in the past 6 months (>5% weight change); 24 those already following a weight loss programme; serious medical conditions or contraindication to the practice of physical exercise; or any medication that may affect body weight or blood pressure. Current physical activity levels did not determine eligibility. Potential participants were approached using a wide range of techniques, including an online press release, internal university emailing lists, university news page, Facebook and poster advertisements. They were asked to contact the researcher for more details, to check eligibility, receive an information sheet and to register for the launch event.
Intervention
Launch event
Pre-registered participants were checked into the group setting, screened using a Physical Activity Readiness Questionnaire (PARQ) (Supplemental Appendix 3) to ensure that there were no contraindications to exercise, 25 and were asked to provide their informed consent in writing. Baseline measures of height, weight, BMI and waist circumference 26 were obtained individually in a private room. To assess physical activity levels, a General Practice Physical Activity Questionnaire (GPPAQ) (Supplemental Appendix 4), 27 which is a validated screening tool, providing a simple 4-level physical activity index, 27 was administered. Quality of life was assessed using the Short Form (SF)-12 health survey (Supplemental Appendix 5), 28 which is a valid alternative to the SF-36 28 and provides mental and physical functioning scores, which are comparable at the population level. These questionnaires were not intended for comparison, therefore were only carried out at baseline. Participants were then (individually or in pairs/smaller groups) introduced to the Onitor® Track test unit by a company representative. Participants were presented with the Onitor® Track test unit (wearable, heart rate clip and application) and guided on the installation and utilisation of the app. A dietary advice sheet (Supplemental Appendix 6), recipe sheet (Supplemental Appendix 7) and summary checklist (Supplemental Appendix 8) were also provided. Participants were invited to join the private Facebook group before leaving.
Digital technology employed
The Onitor® Track test unit and app (Supplemental Appendix 9) used in this study is in development and has not yet been released to the commercial market. The Onitor® Track test unit comprises a worn sensor, which uses a three-axis accelerometer. It is a dual dual-position wearable (watch-style), consisting of a polymer wristband and heart rate clip (which can be attached to the underside of a bra), containing the sensor. When worn on the wrist, daily steps, distance, calories burned, active minutes and sleep duration are measured; these, plus the heart rate, are measured when using the heart rate clip. The sensor displays light-emitting diodes (LEDs) to indicate preferred progress towards the user’s daily goal (i.e. steps, calories burned) – more lights illuminate as progress towards the goal increases. All other feedback is available through a smartphone application that displays a real-time (within day) snapshot of user data (Supplemental Appendix 10).
Exercise intervention
Participants received a 4-week personalised exercise programme, delivered through the application (Supplemental Appendix 11), which was determined by the participant’s weight loss goal, target date of achievement (participant-led) and fitness level (not regularly exercising or currently exercising). The app uses a complex algorithm to continuously adapt the programme according to self-reported weight input data (minimum update weekly) and in response to the activity/heart rate recorded while wearing the device during exercise. The plan consists of body-weighted exercises, provides step-by-step instructions and allows the option of populating them within the user’s smartphone calendar. Each session lasts around 30–45 min, with 2-3 sessions per week. Participants were encouraged to wear the sensor within the heart rate clip during the exercise sessions, to provide a more accurate account of calories burned. They were also advised to record and update their weight on the application at the end of each week.
Dietary intervention
The dietary sheet provided (Supplemental Appendix 6) was designed by Onitor, with the intention of educating participants about best food choices while undertaking their weight loss journey and 4-week exercise plan. The initial aim was to make the body more sensitive to insulin, by encouraging a low-carbohydrate intake for the first 2 weeks, focusing on healthy fats (plant based and fish), vegetables and protein sources. At week 3, participants were recommended to slowly introduce carbohydrates on workout days. Portion sizes are used to control intake, with ‘hand’ size as a measuring tool, in place of calories or weight. The recipe sheet provided ideas suggested components above, for breakfast, lunch and dinner.
Facebook group
A private Facebook group was available for participants to share their experiences with each other, encourage each other and as a means of technical support. The group was monitored by both researchers, who replied to comments/questions, along with Onitor technicians, who provided technical assistance. Weekly reminders were posted by the lead researcher to prompt participants to record their weight and update it in the application.
Quantitative outcomes and analysis
Anthropometric measurements
The primary outcome was decrease in body weight (kg) at 4 weeks. Secondary outcomes were waist circumference (cm) and BMI (kg/m2). These, along with height, were obtained at the launch event, and again at 4 weeks. Body weight was self-reported for weeks 1, 2 and 3 through the Onitor® Track application. Procedures were as follows: body weight was assessed using the Home Treats digital scale (model KA229). Height was assessed using a stadiometer, employing the Frankfort Plane protocol 29 and recorded to the nearest centimetre. BMI was calculated as weight in kilograms divided by height in metre squared. Waist circumference was measured twice, using the World Health Organization (WHO) protocol, 26 with the measure taken midway between the highest point of the iliac crest and the bottom of the ribcage, at the end of expiration. 26 Where measurements were within 1 cm of each other, the average of the two was recorded. If >2, the measurements were repeated. 26
Process measures
Wearable compliance and application usage data were obtained from analytics software provided by Onitor. The days the test unit was worn were based on the days the Onitor® Track recorded energy expenditure. Actual activity monitored by the Onitor® Track, such as the step count and heart rate, was not available for analysis. Self-monitoring data for weight were also provided through this software.
Statistical analysis
The study aimed to recruit a sample size of 20. A formal sample size calculation was not appropriate, as this was not a phase III trial (MRC), but an exploratory study. All analyses were carried out using SPSS (v24). Descriptive statistics were used to describe and summarise all quantitative data. Statistical differences in distributions between pre- and post-outcome measures at 4 weeks were tested using the Wilcoxon matched pairs test. Significance was accepted at p < 0.05. Although this study was not powered to detect change in anthropometric measures, the results are displayed to provide information on effect size. Cohen’s Kappa was used to measure interrater reliability between the two coders in the first instance, ⩽0 indicates no agreement, where 1 suggests perfect agreement. 30 Percent agreement was obtained by calculating the number of item differences between coders divided by the total number of variables.
Qualitative outcomes and analysis
Participants were invited for repeat measures and a semi-structured interview (~30-min duration) at the end of the 4-week period. Interviews were audio-recorded with consent and transcribed verbatim for subsequent analysis. Interviews consisted of questions regarding experience of wearable technology and applications, and experiences, behaviours and preferences of using the Onitor® Track test unit and app. Although the interviewer followed a topic guide (Supplemental Appendix 12) drawn up in advance to maintain structure and flow, participants were encouraged to openly discuss their experiences. Where a semi-structured interview was not feasible, a telephone interview was carried out instead, which took the same format as the face-to-face interviews but were not recorded or transcribed verbatim, but in documented note-form. The transcribed data from the interviews were coded, followed by matrix analysis, 31 and key themes/patterns identified, using a framework analysis approach. 32 The same approach was taken with any key themes or patterns that emerged from discussion on the Facebook page.
BCTs
The Onitor® Track test unit (wearable, heart rate clip), application, including the supplementary material (dietary advice sheet, recipe sheet and user manual), and the study intervention (launch event, Facebook group and qualitative interviews) were coded separately, using the Behaviour Change Technique Taxonomy Version 1 (BCTTv1), 33 which is a standardised tool for assessing multiple behaviours targeted for change in complex interventions. Published definitions guide coding for each technique, which was independently undertaken by two researchers before comparing for interrater reliability. When consensus was not reached, a discussion and referral to the coding guidelines aided resolution of any differences in interpretation. Each technique was coded using a dichotomous score of 0 (not present) or 1 (present). Any information that was not immediately accessible through the application was not considered. The ‘behaviour’ considered when coding the Onitor® Track and study intervention was the adoption and use of the Onitor® Track test unit and app.
Results
In excess of 100 women expressed an interest in participating, 20 potential participants were formally invited and 15 participants subsequently attended the launch event, which took place on 26 May 2017, meaning that only 15 were eventually recruited to take part in the 4-week intervention (Supplemental Appendix 2). 9 participants (60%) dropped out of the study, with the majority (n = 6, 67%) leaving after the second week. 7 (78%) of those who dropped out reported recurring technical issues with the Onitor® Track test unit and/or application as the reason. Seven participants provided anthropometric data at week 4, of which one was self-reported. 7 qualitative interviews were carried out with 5 participants who completed the intervention, and 2 who dropped out. An additional telephone interview was carried out with one participant who dropped out. All 15 participants were invited to use the private Facebook group, of which 13 joined and all utilised, posting questions and supportive comments to other participants. We did not capture the number and nature of these posts.
Quantitative
Baseline characteristics
Baseline descriptive characteristics for all participants are shown in Table 1. As summarised, the median (interquartile range (IQR)) age was 42 (30–52) years; BMI was 32 (26.9–38.5 (g/m2) and waist circumference was 96 (88.5–115.5) cm. Although the exclusion criterion was explicit with BMI and age, only 33.3 per cent of participants were overweight, with the majority obese; one participant was 55 years old. The decision was made to include them in the study, due to time constraints and risk of reduced sample size. The self-reported physical activity level using the GPPAQ found that a higher percentage of participants consider themselves to be moderately inactive or inactive (60%). The median (IQR) self-reported physical and mental health composite scores (physical component summary (PCS) and mental component summary (MCS)) of the SF-12 questionnaire indicate good health (53.8 (51.7–54.7) and 53 (49–55), respectively).
Baseline characteristics of all participants (n = 15).
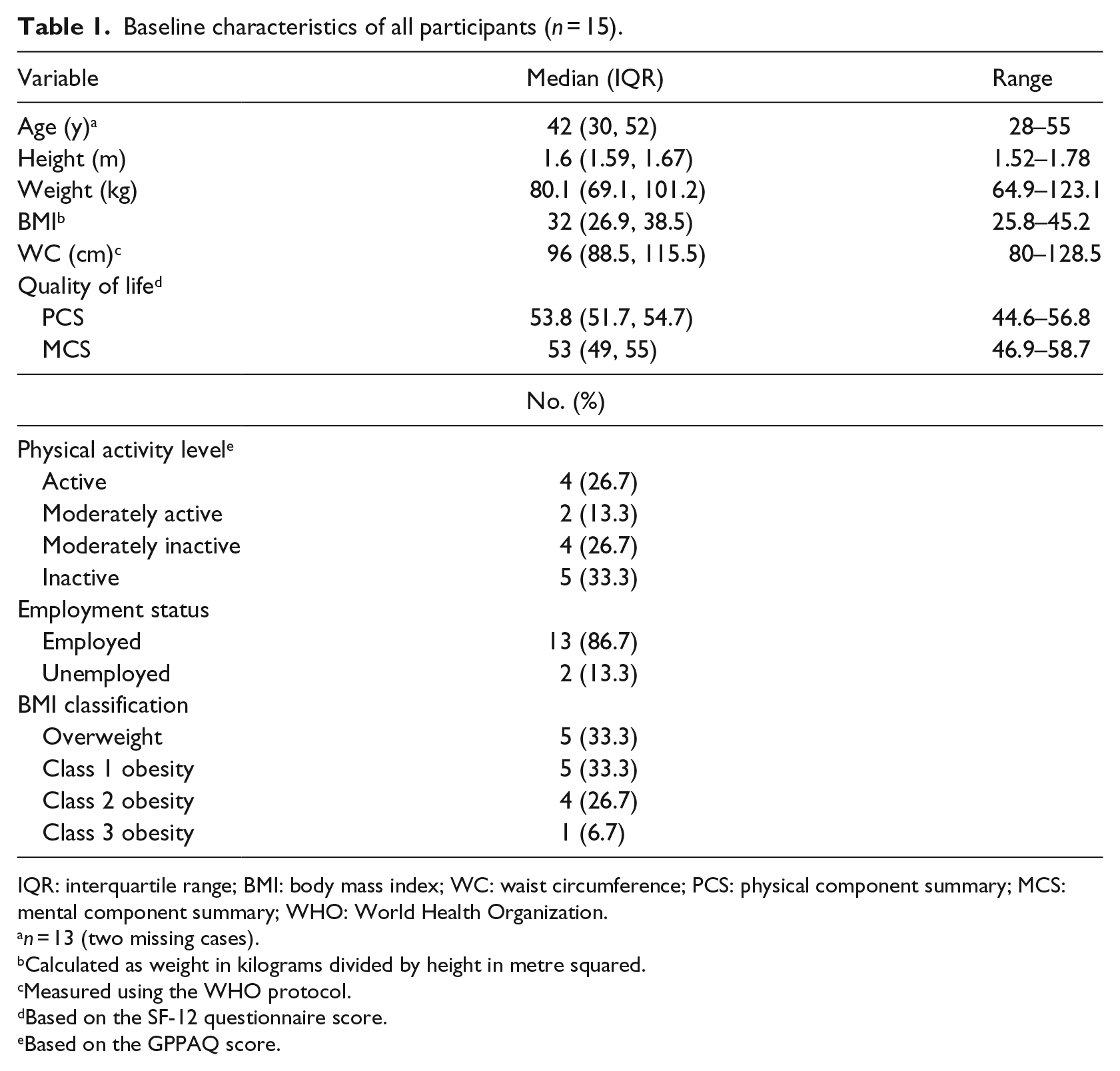
IQR: interquartile range; BMI: body mass index; WC: waist circumference; PCS: physical component summary; MCS: mental component summary; WHO: World Health Organization.
n = 13 (two missing cases).
Calculated as weight in kilograms divided by height in metre squared.
Measured using the WHO protocol.
Based on the SF-12 questionnaire score.
Based on the GPPAQ score.
Changes in anthropometric measurements
Weight loss data were available for only 47 per cent (n = 7) of the study sample (Table 2) due to dropout. The Wilcoxon matched pairs test showed differences in weight, BMI and waist circumference were found between baseline and week 4 (p < 0.05), with a median body weight reduction of −2.7 kg (IQR −1.6 to −3.3 kg). Weight and waist circumference change between baseline and 4 weeks can be seen for each individual in Figures 1(a) and (b).
Change in weight, body mass index and waist circumference in those who completed the study (n = 7).
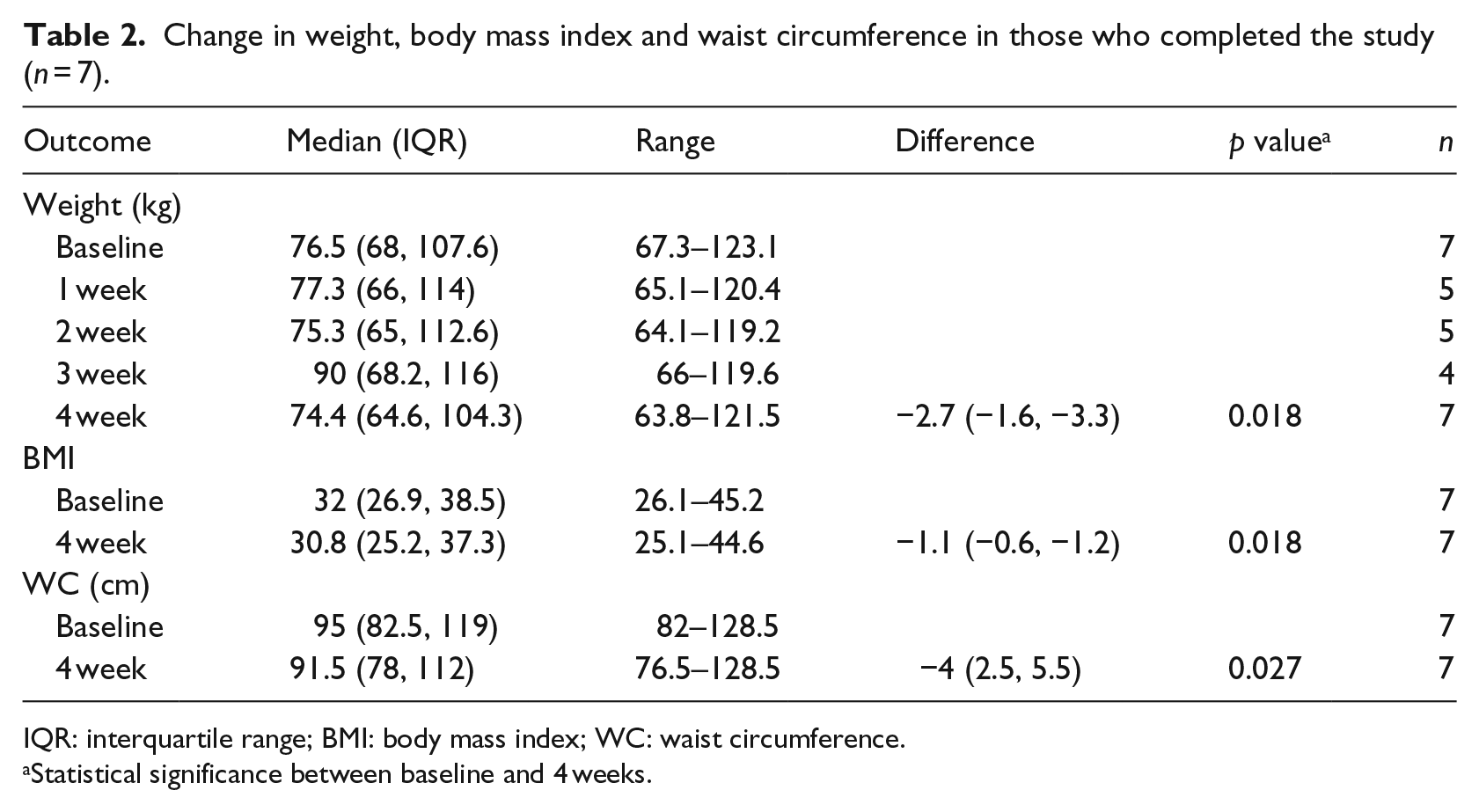
IQR: interquartile range; BMI: body mass index; WC: waist circumference.
Statistical significance between baseline and 4 weeks.
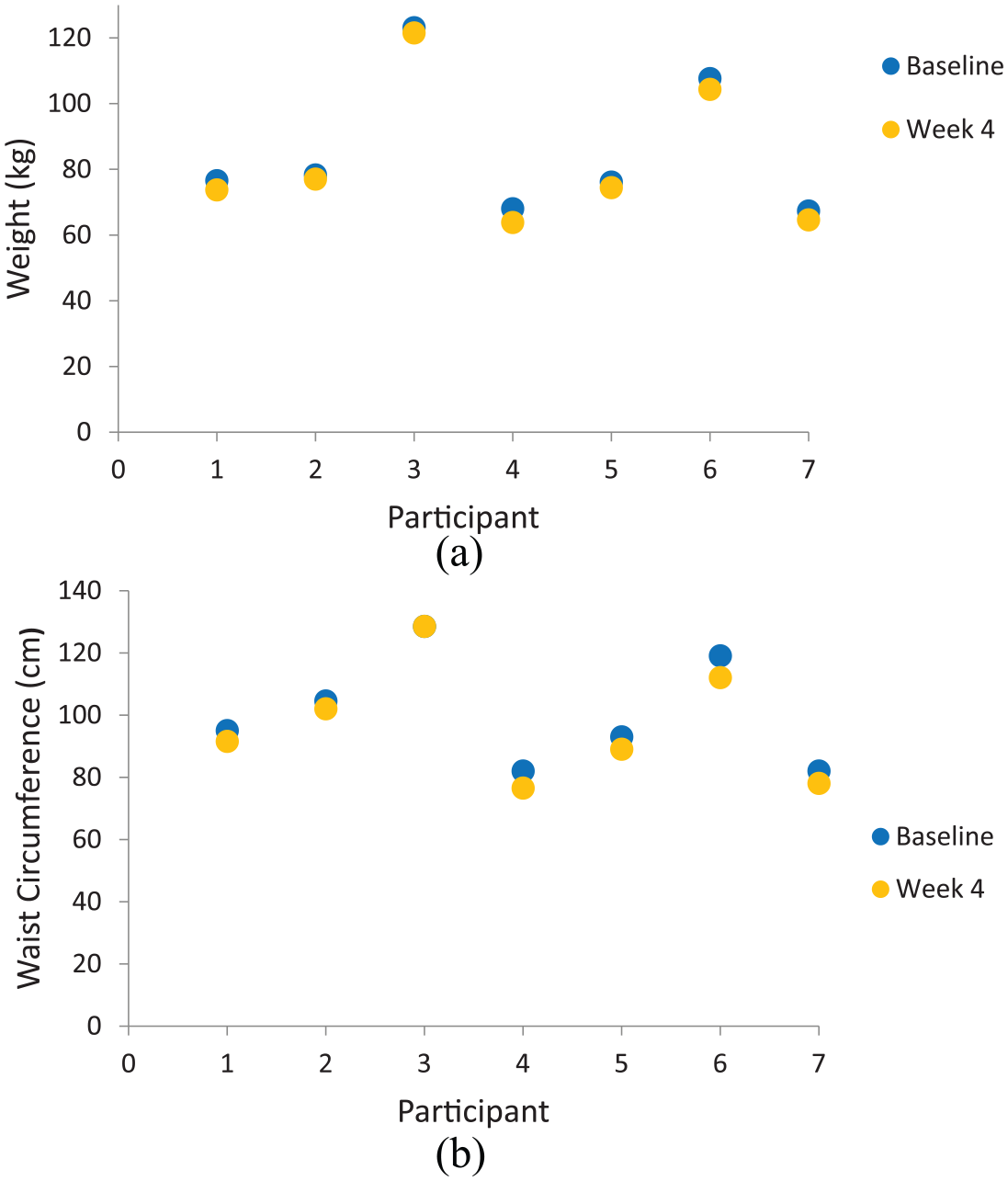
(a) Differences in body weight between baseline and week 4 for each participant and (b) differences in waist circumference between baseline and week 4 for each participant.
Analysis of process measures
Table 3 presents the process data for the last 3 weeks of the intervention period (n = 9). Data were not available to analyse for the first week. The data provided are not representative of all completers, as only 44 per cent of these participants provided anthropometric measures at 4 weeks, while the other 56 per cent dropped out. 2 participants who completed the 4 weeks were not represented here, as no data were available due to technical failure. Of the 21 possible full days of physical activity monitoring, the participants’ Onitor® Track readings showed median time worn to be 4 days (2–14.5 days). The hours of the Onitor® Track use was initially high but decreased each week, from 29.7 h worn (24.3–78.5 h) in week 2 to 0 h worn (0–13.6 h) in week 4. The median time the application recorded use over the 3 weeks was 126 h (42.5–169.5 h), which is 25 per cent of the potential 504 h. The recorded median number of times the application was opened was 25 (18–81 times) in 3 weeks, with 22 prolonged sessions (11–47 sessions). The total times the application was opened was initially high but decreased each week, from 16 times (11.5–30.5 times) in the second week to 0 times (0–17.5 times) in the last week. As seen in Figure 2(a) and (b), self-monitoring and application use decreased throughout the recorded 3-week period.
Process measures from week 2 to week 4 (n = 9).
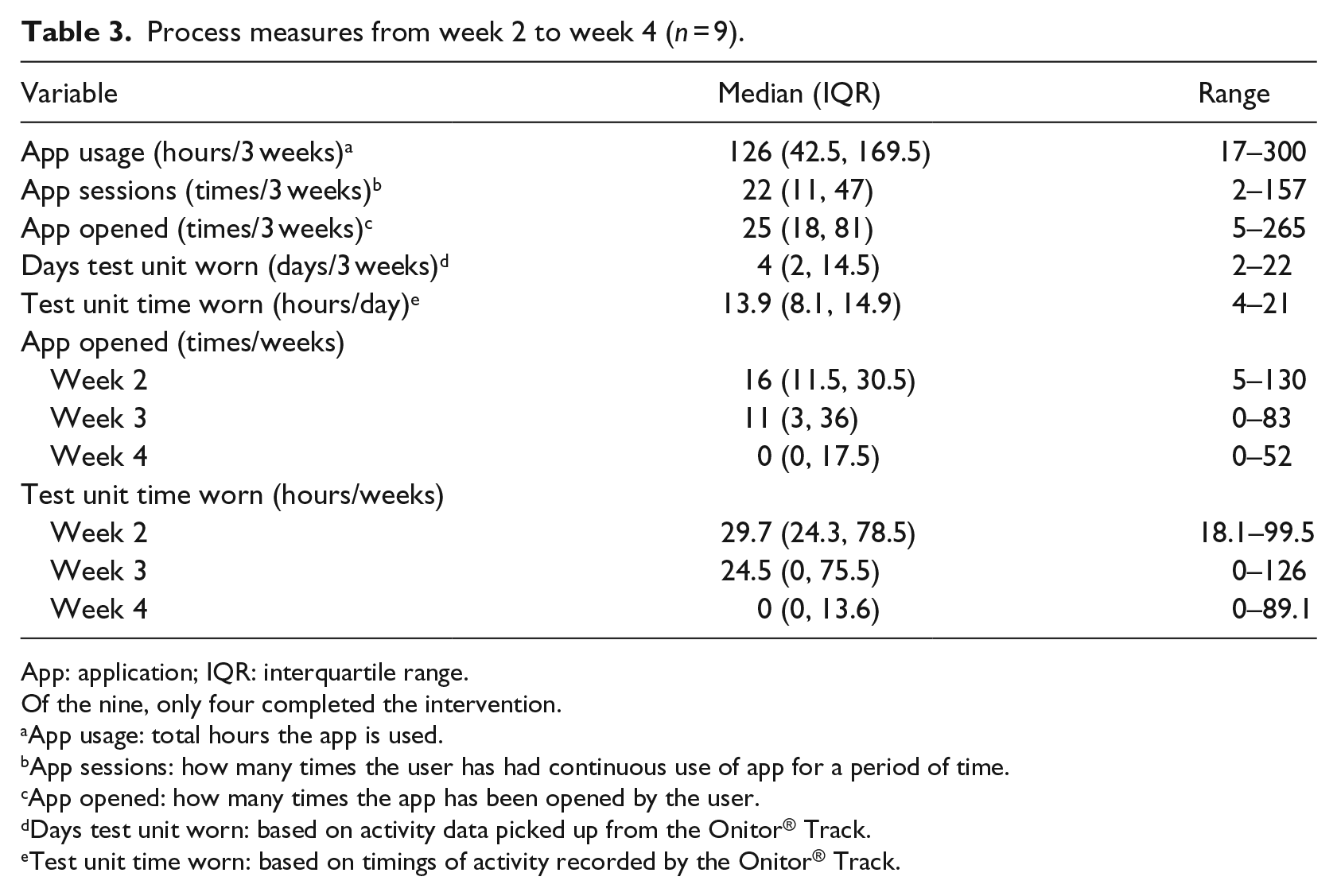
App: application; IQR: interquartile range.
Of the nine, only four completed the intervention.
App usage: total hours the app is used.
App sessions: how many times the user has had continuous use of app for a period of time.
App opened: how many times the app has been opened by the user.
Days test unit worn: based on activity data picked up from the Onitor® Track.
Test unit time worn: based on timings of activity recorded by the Onitor® Track.
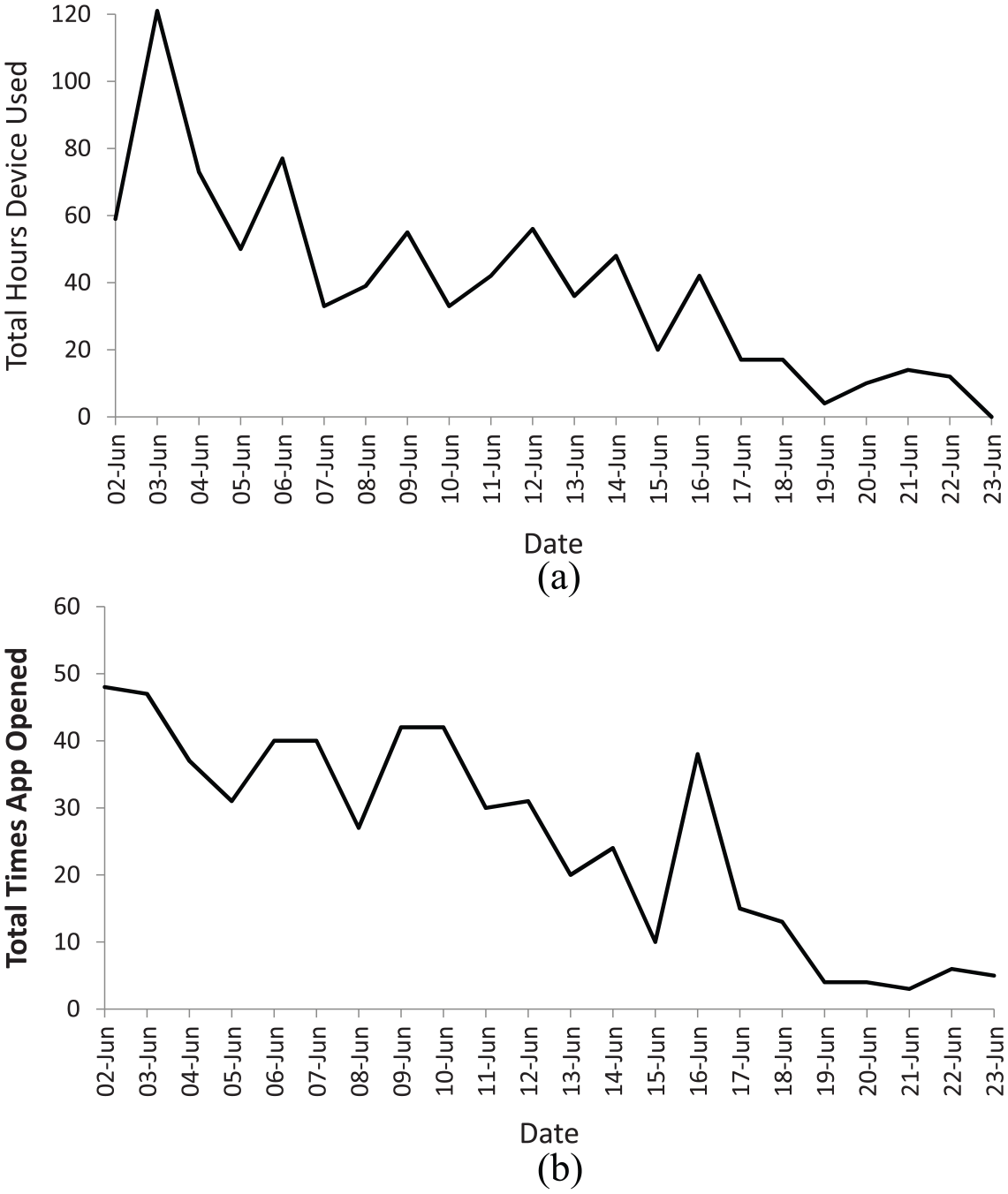
(a) Total hours device used over the last 3 weeks of the study intervention and (b) total times the application was opened over the last 3 weeks of the study intervention.
Qualitative
All participants were invited into the Facebook group, of which 13 joined and participated in conversations. Of the 8 participants interviewed, 5 were currently using a Fitbit, one had previously used a Fitbit (but nothing currently) and two were currently using various health and fitness applications. The interviews lasted between 25 and 45 min. Pseudonyms are used in place of the participant’s name to preserve anonymity. Three main themes emerged from the qualitative analysis: motivation to use wearables and applications; features of wearables and applications relating to ongoing engagement based on past experience and with the Onitor® Track; and behaviour change processes initiated by the Onitor® Track test unit, app and study intervention. The participants answered questions about their past experience/use of wearables and applications and their experiences of using the Onitor® Track test unit and app alongside Facebook.
What motivates people to use wearables and applications to achieve their weight loss goals?
Most participants wanted to lose weight and/or get fit. Motivation was often prompted by an upcoming event, or wearables/applications were used as a motivational tool. For example, I knew I’m going on holiday in a month, and the thing is, all of my clothes are not fitting. (Gemma) Probably to try and spur me on to lose that last sort of stone that I wanted. (Ann) I think maybe to help kick-start me to get into the mind-set to lose weight again. I thought that maybe it would help me to get myself going . . . it was a starting point for me. (Susan) Because I went off the wagon of losing weight . . . It’s just like a rough patch of unhealthy eating and not exercising, so I need to get back on track. (Taylor)
Step counting was a recurring reason for using wearables and applications. Most participants were concerned with recording and monitoring this, with feedback and goal setting frequently mentioned. For example, It’s more like counting the steps; I understood how long I went during the day. To me that is my main concern. I’ve got a target of 11k a day walking and running and that’s what keeps me motivated. (Gemma) When you go out for a walk, you can link it up like on your phone app. You can start it on a walk and it records your walk and you’ve got like a picture at the end showing you the area you have walked. (Ann)
Only 1 participant was primarily concerned with exercising and for using particular features within the wearable to facilitate weight loss: My heart rate when I exercise, and whether I have burned enough calories. (Taylor)
Which features are most used and enhance user satisfaction and engagement?
From previous experience and from using the Onitor® Track, 7 main factors were identified relating to satisfaction and engagement. These were the following: (a) accessibility, (b) flexibility, (c) accuracy, (d) design, (e) exercise plan, (f) food log and calorie counting and (g) challenges and social interaction.
Accessibility
Having access to instant feedback from the wearable is a preferred option, with many expressing that the Onitor® Track wristband lacks this. For example, You can’t really see anything. There’s nothing else to really look at. You need to log in, whereas with your Fitbit, you can push the button or tap it and it tells you how much steps you’ve done at a glance. (Ann) I would have preferred something on the device itself to just be able to have a quick check, rather than having to go into another device to have to see how I was doing. I don’t think I would have bought it if I had thought I’d have to look at my phone every time I wanted to check how I was doing. (Susan)
Flexibility
Most participants expressed their preference for a wearable and application that is flexible, in that there are enough options available for personalisation and ease of use. This was particularly true for dietary aspects within the applications: The only problem that I do find is really quite annoying is with the Fitbit, you have to measure how much food, like weight-wise and stuff you’re eating to get the accurate calories. (Eilidh) With the Fitbit one, I found that quite fiddley to use. It was quite restricted in how you recorded your food intake . . . you had to sort of chose from a drop-down menu . . . I was getting fed up trying to find out what went in. (Susan) [Regarding the Onitor® Track] To be honest, it is very basic the way it reports . . . it just shows you as a bar, but for e.g. my pacer, you could see some sort of statistical analysis, what’s happening, in a day, in a week, in a month and it gives you much more information compared to what you see there. (Gemma)
Accuracy
This was a big concern for most participants, especially with step counting and calories burned. Almost all participants compared the Onitor® Track to their current device and used that as a ‘gold standard’. For example, The fact that the steps were so far out compared to my other one, but then had I not had my other one, I wouldn’t have known any difference. (Ann) . . . I was going, ‘look at the difference in steps, this one’s saying 5,000 and this one’s 3,000 or something’, and he was like ‘yeah, but have you ever thought that that one might be accurate and it’s your Fitbit that’s really out?’. (Stephanie)
Design
The design, especially the security of the strap, was an issue for many of the participants. They preferred a lightweight, simple and secure wearable, which could also be used to record the heart rate instead of having to use another device. For example, I didn’t like the strap. I thought that was difficult to use, and clipping the sensor in and out – there are so many better devices that do it all in one go. (Susan) This is linked to your phone [test unit] so why do you need a removable? I didn’t find the clip thing easy to actually attach. That was a bit faffy having to wear that during exercise, and I didn’t like the strap on that at all – it’s not secure enough (Louise) I liked the fact that it was nice and lightweight. I didn’t feel like I had it on when it was on the wrist strap (Eilidh)
Exercise programme
All participants found the built-in exercise plan a very useful feature, with the fact that you do not need other equipment and it can be added into in your diary.
I think having that little workout and a sort of diary of when to do it, I thought that was really useful, in the device that you gave us. I think that it just motivated you to do something different, maybe from your regular activity, because I don’t really want to go to a gym. (Susan) I did like the exercise, how it was all in one thing, where you know that you could have gone anywhere and done it. It wasn’t like you had to do a DVD or download it from your iPad – I liked the fact it was all there. (Stephanie) I did like the fact that the exercise programme was built-in and it was different each time that you did it . . . Fitbit doesn’t have something like that built into their app . . . so I did really like that part . . . Can I still use the app? (Ann)
The intensity of the exercises and the rest periods were discussed on the Facebook page, with most users agreeing that they were too long: Workout wasn’t crazy hard. The rest periods are quite long. (Eilidh) Was a good workout but I do agree that the rest times were a tad too long. (Stephanie)
Food log and calorie counting
When asked about using applications for counting calories, there was a very mixed response. Some felt calorie counting was essential to help achieve their weight loss goal, where others found it time consuming and less of a concern: So, I don’t tend to weigh my food – life’s too short for that. How specific does it need to be? If you’re losing weight and you’re increasing your exercise, then how much do you really need to monitor that? (Susan) If something is a lot of calories then I wouldn’t have it rather than log it. (Fiona) With the calorie counting, I managed to lose weight, and that was helpful. (Gemma) I think for some people it doesn’t matter, but for me, if I really want to focus on my weight-loss and be serious about my nutrition and exercise, then it’s important. (Taylor)
Keeping track of which foods have been consumed is more important to some, rather than counting the actual calories/food components: I think keeping a food diary lets you see ‘oh my god, I ate all that today’ – it’s in your face, that’s what you did. Maybe that’s a bit clearer to you to reflect on. (Susan) I’ve used the Fitbit quite a few times to say to the GP sort of like . . . I didn’t realise that I was quite allergic to mustard and every time I found foods with mustard in it, I showed them my food diary and then because of that, they actually changed my medication that I was on. (Eilidh)
There were mixed responses about whether they felt the diet component was missing from the Onitor® Track application: I used the sheet – it doesn’t really come with the app. The other apps they help you with the nutrition. I think if you could have some sort of option in the app that you could enter it, then that’s helpful. (Gemma) I didn’t find that it was something lacking in the Onitor® Track. I didn’t feel that that was needed. (Stephanie)
Challenges and social interaction
Generally, most found that engaging in challenges, taking part in competitions and receiving ‘rewards’ was a motivation. Some did not find this useful however. For example, It gives you an email: a weekly update of what you’ve done that week, how many steps you’ve done. You get badges: you have walked the length of New Zealand; it does give you little challenges and you can use it as much or as little as you want and it is a motivator definitely. (Louise) The only thing that I would like to see gone would be the motivational kind of things. If you pick up your Fitbit, it goes ‘go Eilidh go, you can do it . . . one step more’, and it’s like, ‘shut up, I don’t need that motivational stuff, I’m walking’. (Eilidh) I think like you would get the email to say, ‘oh you’ve done so many miles’, but no, I didn’t find that a motivator. (Susan)
What behaviour changes occurred because of the Onitor® Track or study intervention?
Physical activity behaviours did not appear to change much because of the intervention. Those who reported change were generally inactive, whereas some participants reported that they were already active. It was evident that technical issues with the Onitor® Track impacted this behaviour: I was getting up in the mornings and doing some of the workouts in the house, so it has made me more active, whether I’ll continue it now that I won’t have the tracker [test unit] to use, I don’t know. I had my kids doing it with me as well. (Ann) When I noticed, I was like one dot left to make it full, and my day was over, I would go out just to make sure I could bring up the steps . . . it was like ‘yes, I must finish it, I must complete it’. Yeah, I think that changed, because it was not something I would usually do. (Taylor) I think because of the problems with the device, I didn’t keep going as much as I would have liked. (Susan) Maybe if the device had worked better, but I don’t think it increased my activity levels because I’m quite active anyway, so I don’t think it made any difference really. (Louise)
Some participants mentioned the challenges of sustaining exercise or physical activity due to the impact of the dietary plan: To be honest, it’s slightly reduced because I don’t have that much calorie to burn as I used to. I found that when I am doing exercising its kind of more challenging than it used to be. (Gemma) The day I did the kilt walk, there was no way I could just eat what was there [diet sheet] because I’d never have the energy to do 15.5 miles if I’d eaten what it said, so obviously that day I did about 40,000 steps so I had to eat because I needed the energy. (Ann)
Every participant reported a change in dietary behaviour as a result of following the diet advice on the sheet provided. Changes included reducing carbohydrate intake, replacing snacks with healthier options, mindful portion sizes, prompted learning and meal planning. For example, I found that I was probably eating different things, like I was eating nuts . . . not a lot of them, but I would never normally – that would never be a snack for me. (Stephanie) I invented like mushroom pizzas. The kids quite liked it actually because it was just new stuff that they were trying. (Eilidh) I went and googled it and I started to learn about what exactly is happening to your body. (Gemma) I would say over the last few weeks, I’ve definitely seen a reduction in what I’ve taken in. So, yeah, I’m starting to see improved habits. (Susan)
Some participants reported awareness of the consequences of eating certain foods and, in turn, evaluated their choices and intentions more readily: Sometimes at work, the last two weeks, making myself a coffee going, ‘I’m going to have a biscuit’. It was funny, I didn’t realise I did that until the third week when I was having a biscuit, I was like ‘now, I never did this that two weeks at all’. I then consciously was like ‘why am I needing it when I wasn’t having it?’. (Stephanie) It’s like my mental state has kind of changed a bit towards food and the food I put in my body. I’m more like, ‘should I really be eating this right now?’ I am more careful with what I put in my body instead of going straight for it. (Taylor)
There was some discussion around the diet component of the intervention, with very mixed views on the ‘low carbohydrate’ aspect: I find the diet too restrictive for my lifestyle/exercise routine. I feel hungry and miss carbs. My mood has definitely been affected by this too. (Ann) I haven’t felt hungry all week either, it’s really surprised me! I found that the things it told you not to have, were the things I wanted and I had on a daily basis. (Susan)
The online Facebook support was mentioned for providing social support and motivation and for reporting technical issues and receiving feedback: When we were putting our weight, some people was like ‘I’ve lost 2 kilograms’ – that was kind of motivating, because we were all losing weight and that was actually working, so seeing that was good. (Taylor) I wanted to make the people motivated, and also I think being part of a group doing something is helping, and when you’re communicating and saying things that you feel that you are struggling with. (Gemma) I did find it really helpful, because otherwise it would have been having to email or phone or something. (Ann) It works really well – people communicate on it and there is ongoing support throughout and feedback, and was great when things not doing so well. (Fiona)
However, some participants did not share the enthusiasm for group support and are perhaps more private. An artificially created group may be attributed to this. For example, I didn’t really like putting in how much weight I had lost or anything like that. I felt uncomfortable talking about my weight. I don’t know why. (Eilidh) I’ve got quite a lot of recipe ideas, but was just a bit nervous to share, because it’s a sort of artificially created group, you don’t actually know anyone – I wasn’t sure how much people would be into that, so I didn’t really offer. (Susan) . . . the launch, if everyone was there the same time, then I’m sure the Facebook group would have worked better than it did, and people would have been more interactive. (Taylor) It might have been better to get to know everyone, because you didn’t really get a chance to meet everyone. (Stephanie)
BCTs
Interrater reliability between the two coders was in good agreement (91%) for the Onitor® Track test unit and app, with a kappa statistic of .66, and in moderate agreement (82%) for the study intervention, with a kappa statistic of .55. 30 Discrepancies were discussed and final techniques present agreed between the two coders.
Table 4 displays the number of BCTs identified as present in the Onitor® Track (test unit, application and supplementary material) and study intervention (launch event and Facebook). The techniques were identified on the premise that they could potentially initiate the adoption and use of the Onitor® Track test unit and app. Techniques from the taxonomy that were not found were not included in the table. Of the possible 93 techniques, 27 were present in total: 14 were found in the Onitor® Track test unit and app, with 13 additional techniques found within the study intervention.
Behaviour change techniques present in the Onitor® Track and study intervention.
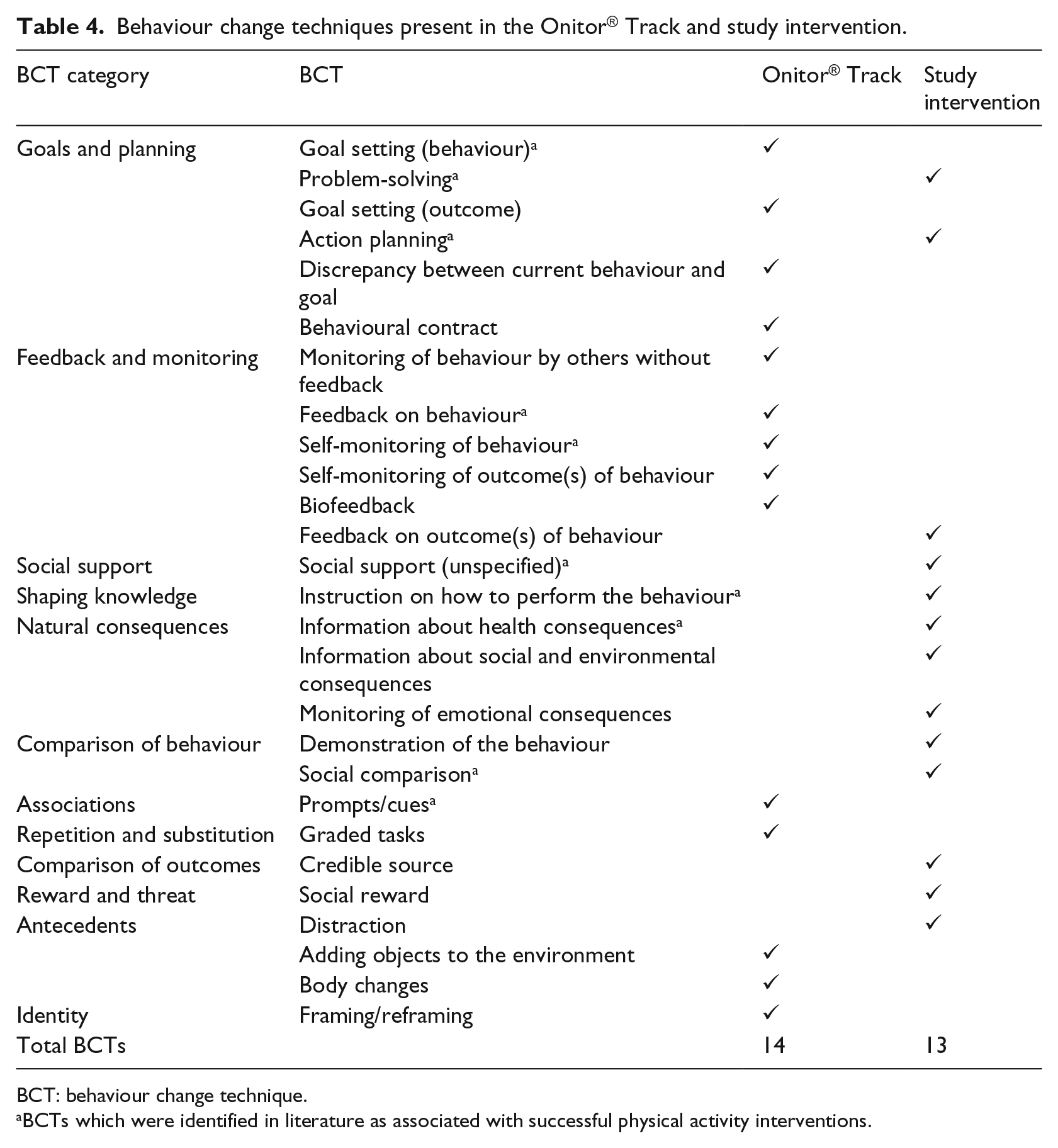
BCT: behaviour change technique.
BCTs which were identified in literature as associated with successful physical activity interventions.
Of the techniques identified, some were integral to the nature of the Onitor® Track: goal setting provided via the application; self-monitoring activity picked up by the Onitor® Track and stored within the application; feedback on progress and discrepancy between behaviour and goal provided by the Onitor® Track and application; and prompts/cues to engage in exercise received from the application. The study intervention added a social component, for social support and comparison, and provided relevant instruction and information.
Discussion
The objectives of this mixed methods exploratory study were to (a) undertake an experimental study of 20 overweight women using the Onitor® Track for a 4-week period; (b) explore the feasibility and acceptability of the Onitor® Track among those overweight women; and (c) investigate the presence of BCTs within the Onitor® Track and study, relate them to known drivers of behaviour change and establish which ones are identified and engaged with. We were only able to recruit 15 women. While the quantitative analysis revealed a change in body weight, BMI and waist circumference between baseline and study end (p < 0.05), with a median weight reduction of −2.7 kg (IQR −1.6 to −3.3 kg), statistical analysis of body weight change over the 4-week period should be treated with caution as it may be attributable to type 1 error. We included the results to provide information on effect size only. The few preliminary randomised controlled trials (RCTs) to date have used varying designs comparing and combining the use of wearables to standard behaviour weight loss interventions, which have shown some modest results.7,17,18 However, a recent RCT by Jakicic et al. 16 suggested that the addition of these technologies does not yield the desired quantitative results, questioning the effectiveness of wearables in modifying diet and physical activity behaviours. The Jakicic study reported that the addition of the wearable was less effective for weight loss compared to standard treatment at 24 months (p = 0.002), although no significant differences were observed between groups at 6 months (p = 0.29). In the same study, changes in BMI, body fat per cent, fat mass and lean mass were found over time (p < 0.01) but not between groups at any point (p > 0.05). Jakicic et al. also found that total calories and macronutrients as a percentage of calorie intake changed over time (p < 0.001), but did not differ between groups, which was the same for sedentary time (hours/day) and light physical activity (minutes/week). Therefore, it is difficult to understand the greater weight loss seen in their study’s standard group when there were no observed group differences for dietary intake or physical activity behaviour.
Although dietary intake was not monitored throughout this study, the 8 participants interviewed reported multiple changes in their dietary behaviours and advised that they cut out or reduced carbohydrate intake for the first 2 weeks. The diet provided in this study is very similar to the initial stages of the Atkins diet, although a complete elimination of carbohydrates was suggested, unlike the <20 grams/day commonly found in the Atkins diet. 34 The underlying concept was to bring the individual into ketosis and allow them to increase insulin sensitivity to better utilise their fat sources for energy, although higher intakes of fat were not necessarily encouraged. They were advised to re-introduce a ‘handful’ of carbohydrates around workout days in week 3, which provoked various responses from participants. Mostly, they were surprised that they did not miss carbohydrates during the first 2 weeks and were happy to continue excluding them, although some were clearly struggling due to the higher volume/intensity of physical activity and exercise. The relative contributions of fat and carbohydrate as a fuel source are dictated primarily by the relative intensity of exercise. 35 As the exercise programme is personalised, the intensity and difficulty increases with progress, which would be difficult to sustain on a low-carbohydrate diet. 35 The preliminary dietary recommendations designed by Onitor were based on the premise that individuals were already consuming a high level of carbohydrates and did not take physical activity levels or other individual differences into consideration. We cannot be sure of prior levels of carbohydrate consumption, other than from self-report within the qualitative component of the study; therefore, we cannot know whether this was the most appropriate intervention for participants. As preferred activity levels were not stipulated in the inclusion/exclusion criteria and there was no measure of current dietary habits, the tailoring of the intervention used baseline characteristics and behaviour change during the period of study, rather than before and after, so the reported differences among participants were not surprising. The weight loss observed in this study is comparable to that found in other studies with similar low-carbohydrate diets.34,36 Truby et al. 37 carried out an RCT comparing various diet types and found the Atkins diet to result in an initial higher weight loss during the first 4 weeks of the trial. The initial large restriction in carbohydrates seen in this study would likely result in a total kilojoule (Kcal) deficit and ultimately lead to weight loss. 34 Most benefits of weight loss programmes are seen in the first few weeks, 37 with weight loss gradually slowing down thereafter. 38 Water weight can also account for a majority of this initial weight and is usually regained once carbohydrates are re-introduced. 39 Some participants reported a weight gain at this time, although data were not available for all participants throughout the 4-week period, and body composition measurements were not taken, so week-to-week analysis could not be carried out.
A range of physical activity and dietary behaviour changes were evident. The majority of participants already engaged in a number of activities, such as walking, exercise classes and swimming and, therefore, did not find that the use of a wearable device necessarily helped increase their activity. However, all participants interviewed advised that they used the exercise programme. Some had technical issues with the application, as well as the Onitor® Track test unit, although a number of participants continued to engage with the exercise programme even without feedback. Although data were not available for exercise programme usage, or for specific physical activity behaviours (step count, energy expenditure and so on), data were provided for application and Onitor® Track engagement levels for the last 3 weeks of the study period. It must be noted that the data captured are unlikely to be a true reflection of the participants’ activity, as there were reported technical and wristband issues with the Onitor® Track, which would have prevented some participant’s data from being recorded. Moreover, only 4 of the 9 participants, for whom data were gathered, completed the 4-week intervention. Nevertheless, it is evident from Table 3 and Figure 2(a) and (b) that although initial use of the Onitor® Track and application was high, it fell over the subsequent weeks, to a median of 0 (0–13.6) for Onitor® Track use and 0 (0–17.5) for application use. However, the drop in engagement was found towards the end of the study rather than as a response to the technical issues experienced early on. We did not investigate this further in the qualitative interviews as quantitative data had not been analysed at that point. Pellegrini et al. 17 found that the technology group in their study wore the armband for 17.4 ± 5.9 h per day, with an average of 6.5 ± 0.6 days per week. The median (IQR) readings picked up from the participant’s Onitor® Track were 4 days/3 weeks (2–14.5 days/weeks). Although this is a poor result over the 3 weeks, it is evident from the skewed IQR that some individuals wore the Onitor® Track more than others. Moreover, Jakicic et al. 16 reported median test unit time worn to be 4 h per day (IQR = 1.7–9.7 h), whereas in this study, median test unit time worn was higher at 13.9 h per day (8.1–14.9). Continuous use of a wearable has been significantly associated with greater weight loss results than shorter intermittent use,7,18 as user engagement determines the intervention efficacy. 40 This is similar to that found in standard weight loss interventions, where successful weight loss has been associated with longer treatment periods. 41 It remains unclear as to which mechanisms limit weight loss, 42 although most studies now suggest that attrition rates,38,43 user engagement 44 and length of intervention 45 are all important factors. The attrition rates found in this study was 60 per cent, with the majority leaving after week 2, but was not dissimilar to the 40–60 per cent found in other studies,43,46 which highlights that only around half of those who undertake a weight loss programme complete it. The reason for these high attrition rates and programme adherence found in other studies is not clear, but within this study, 78 per cent reported leaving due to technical issues with the Onitor® Track test unit and/or app.
Despite the lack of reported changes in physical activity levels, participants expressed that they found the exercise programme motivating and convenient, and enjoyed the personalisation of the workouts themselves, noting the change in intensity as they progressed. Despite the technical issues experienced, some participants were happy to continue using the exercise programme, with 1 participant asking if they could continue to use it after the intervention period. This suggests that a built-in exercise programme is an appropriate tool to have within an intervention delivered by a wearable device and accompanying application. The built-in personalised exercise programme is a unique feature provided by the Onitor® Track, which, to our knowledge, is not a feature included within any other device on the commercial market. Other wearables have been designed to encourage a healthier, more active lifestyle, 47 where the Onitor® Track was designed specifically with weight loss in mind. There is usually little focus on physical activity and exercise in standard behavioural programmes, 2 even though there is a known association between being overweight/obese and sedentary behaviour, 48 with the ability to reduce the risk of obesity and its related diseases by increasing total physical activity over time.6,49,50 Interventions that include physical activity, along with diet and behaviour therapy, have shown to achieve around 8–10 per cent weight loss between 4 and 6 months.16–18,51 A systematic review by Fogelholm and Kukkonen-Harjula, 52 and a meta-analysis by Anderson et al., 6 also confirmed the importance of exercise in weight loss maintenance, with higher success rates in sustaining lost weight in those who exercise more. Another systematic review by Curioni and Lourenco 51 found that greater initial weight loss can result from a combination of diet and exercise, more so than diet alone. However, without calorie restriction, a high volume of exercise is required to achieve weight loss, which would not be sustainable for most. It is generally recommended that weight loss interventions should include both calorie restriction and exercise to achieve clinically significant weight loss.53,54
To date, there has been limited and mixed evidence provided for the effectiveness of wearable devices in facilitating weight loss. 16 Although these RCTs have discussed feasibility in relation to attrition and compliance among participants, practically no qualitative research has been carried out in terms of their acceptability among participants. 14 It is imperative to identify and understand which components of these wearable technologies, if any, can help facilitate weight loss, how they can be implemented into future weight loss programmes and whether they are acceptable to the participant.7,21 This study conducted exploratory research to gain an understanding into any underlying motivations, engaging features and BCTs implemented in the Onitor® Track that could potentially encourage user engagement and compliance, and ultimately weight loss. The study found that the predominant motivation for using wearable technology was to lose weight and get ‘fit’. Step counting was the main objective for participants, and therefore, whichever features facilitated this were the most preferred. Interestingly, when asked about motivations, many participants gave step count as their primary motivator to use a wearable, with weight loss being a secondary outcome. With that being said, it is unknown whether participants have purchased the device with weight loss in mind and used step count as a mediator. In Scotland, walking has been reported to be 3 times more popular than any other recreational activity, and a suitable mode of exercise. 55 Obtaining 8000–10,000 steps per day is suggestive of an active lifestyle, where anything below that is considered as sedentary behaviour. 53 Weight loss of <2 kg has been observed in participants using pedometers, who have increased their baseline step amount by 2000–4000 or succeeded the daily target of 10,000,56,57 although no clinically significant weight loss evidence exists as a result of pedometer-based programmes alone. 53 The recommended minimum levels of physical activity required to maintain health is 150 min/week of moderate or 75 min/week of vigorous physical activity. 29 However, there is a distinction between this and the required levels to induce weight loss, which the American College of Sports Medicine recommends is >255 min/week. 58 As only 63 per cent of Scottish adults have managed to meet the minimum requirements, it is unlikely that most would achieve the recommended amount for weight loss. 29
Accessibility, flexibility, accuracy and design were the four most commonly mentioned features that participants identified as being important when buying a device. Accessibility is receiving real-time feedback from the test unit itself, along with having the flexibility to personalise what is displayed on the test unit and on the application. Some participants expressed that the decision to buy a wearable would solely depend on this. Qualitative analysis by Tang et al. 14 and Yingling et al. 59 found both accessibility and personalisation to be two of the most valued features and that continued use would depend on the inclusion of these features. Accuracy 60 and design14,17 have been linked to the length of time test units are worn and whether there is continued use. Both have impacted the use of the Onitor® Track in this study, resulting in a high attrition rate, which is reflected in the comments. There were discrepancies in calorie counting/food logging, as some participants shared their distaste in this behaviour, while others embraced this feature, although complained about the lack of flexibility. Although calorie counting is usually perceived to be inconvenient and laborious, 61 it has also been shown to result in dietary changes and behaviours. 14 Software within applications can help reduce the burden of self-monitoring foods, if they include an extensive database and ensure flexibility for user preference. 62 Some participants in this study suggested that food diaries would be a better option, which would not only allow for self-monitoring of foods, but of feelings and situation-specific responses. 14 Although most smartphone applications offer social support through social media interaction and team challenges, the participants in this study did not generally consider these features to be important, with most not utilising them. However, the private Facebook group was generally considered motivational, encouraging and a useful place to obtain information. Group support schemes are usually the foundation of most commercial weight loss programmes37,63 and standard behavioural therapy 64 due to their association with motivation to maintain good health behaviour habits.65,66 Although the majority of participants liked being part of a group and were happy to engage, some felt less enthusiastic in sharing their personal experiences. Some participants mentioned the artificially created environment and advised that interaction would likely have been greater if they had had more time to get to know one another at the launch event. This mixed response is apparent in other studies, where a review by the National Institute for Health and Care Excellence (NICE) 67 provided some inconsistent evidence for group support schemes, showing the majority of studies to be in favour of it, while some find personalised support more desirable.
The feedback provided by these monitors and applications have been compared to that provided in a clinical study and is suggested to be similar, or more rich and individualised, as they provide charts and graphs, indicators and progress towards certain goals and options for social comparison and support. 10 Evidence-based BCTs are used within interventions to try and help people change health-related behaviours and have been adopted by developers of wearables and health and fitness applications. Although widely available, they have been questioned regarding their ability to endorse BCTs to motivate people to improve their health and are often reported as absent. 11 The Onitor® Track test unit and application contained 14 BCTs, including 4 important ones identified in literature, which are associated with successful physical activity interventions and increased self-efficacy.10,67,68 This is comparable to Lyons et al. 10 who also carried out the 93-item taxonomy on wearable devices, in which they found an average of 6/93 BCTs present and 9 from literature. Other studies have carried out analysis, but using different taxonomies, identifying 5–16 techniques.66,69,70 Of the evidence-based techniques identified, some were integral to the nature of the Onitor® Track: goal setting provided via the application; self-monitoring activity picked up by the Onitor® Track test unit and stored within the application; and prompts/cues to engage in exercise received from the application. These were identified and employed by the participants in this study and have also been valued in other studies.14,66,69–71 The study intervention provided an additional 13 BCTs, of which 6 were identified as successful in literature. This added a social element, for support and comparison, seen in most devices, 10 but also provided relevant instruction, and prompted problem-solving and action planning, which were not identified in other studies.10,66,69,70 Prompt practice, self-talk and self-rewards are identified as important, but they are generally absent in most devices, 10 including the Onitor® Track. The optimal number and combination of BCTs and features to increase retention and promote weight loss is unknown. Nevertheless, it has been postulated that the quality of the techniques present is more important than the absolute number 10 and that an abundance of these tools could in fact decrease efficacy. 40 NICE 67 also postulated that there is no evidence to suggest that greater use is associated with greater weight loss.
Strengths and limitations
Due to the 2-phase structure utilised, this study was able to identify important variables with the potential to influence weight loss outcomes, and explore the interaction between the effects and experiences to better inform future research. The study used a small convenience sample, which is not statistically powered to detect a difference in weight change, although clinical significance of the findings could be considered valid if applied to a larger sample, particularly as it captured free-living data. From a practical sense, the time frame was not sufficient to allow for the complexities of this research design, and future research should ensure they take this factor into consideration. From a commercial point of view, the quantitative results are disappointing, which are largely due to the technicalities experienced throughout. However, the Onitor® Track used in this study was a test unit, and so the issues that arose were unsurprising. Nonetheless, the qualitative research carried out provides a base to develop wearable technology and affiliated applications, and highlights the importance of engagement, user testing and collaborative working. It would have benefited our study to have captured the number and nature of engagements with the Facebook group to better understand its role.
Implications for future practice
From academic and commercial perspectives, this study will have a number of practical implications. Not only will it add knowledge to limited research on the efficacy and acceptability of wearables in facilitating weight loss but also it will highlight important implications for the development of said technologies and advance the understanding of important factors that influence weight loss. Commercial wearable technology on the market is not targeted towards weight loss, although it appears that this is one of the main reasons consumers purchase these devices. Therefore, developers should consider the main motivations when designing future wearables and apps around BCTs. Interventions should ensure qualitative work is carried out to create a body of evidence, and the collaboration between health professionals, researchers, developers and BCT experts is essential, as most tend to work in silo. 72 In order to achieve this, protocols need to be specific, further refined and standardised, to allow for easier interpretation and further applications.
Conclusion
The Onitor® Track shows promise as a tool to help facilitate weight loss in overweight women. The built-in personalised exercise programme was widely adopted and identified as being a key component to a weight loss intervention and should be considered for future interventions and by application designers. 2 key components missing from the Onitor® Track were tools to provide social support and to self-monitor nutritional intake. Further investigations are required to assess the feasibility of the Onitor® Track, due to the wide range of technical issues experienced, which hindered compliance and engagement. The Onitor® Track contained a number of important evidence-based BCTs, which was augmented by the social aspects provided throughout the study intervention. From a public health perspective, wearables and applications should be developed with the wider population in mind, although recognising individual needs, preferences and barriers, as the efficacy of BCTs may differ among individuals.
Supplemental Material
Supplementary_document – Supplemental material for Using the Onitor® Track for weight loss: A mixed methods study among overweight and obese women
Supplemental material, Supplementary_document for Using the Onitor® Track for weight loss: A mixed methods study among overweight and obese women by Kelly Buchan and Heather M Morgan in Health Informatics Journal
Footnotes
Acknowledgements
The authors thank the participants for their engagement with and significant contributions to this study. They also thank Cloudtag® for providing Onitor® Track test units, technical support (for the test unit and app) and comments on this paper.
Author contributions
K.B. researched the literature and was involved in finalising the methodology of the study; prepared the research materials (protocol and participant documents); gained ethical approval and co-ordinated participant recruitment; carried out data collection, analysis and interpretation of the data; and wrote the first draft of this paper. H.M.M. led the design of the study, undertook BCT coding and contributed to analysis and writing as supervisor of the project. Both authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study was carried out by a research team at the University of Aberdeen, in collaboration with Cloudtag®, who developed the Onitor® Track. None of the research team owns any shares in Cloudtag®. The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Informed consent was obtained from all participants, and all procedures were approved by the College of Life Sciences and Medicine Ethics Review Board at the University of Aberdeen.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Guarantor
H.M.M. is the guarantor of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.