
Abstract
Many studies have shown that women’s experiences, feelings and opinions during their infertility treatment play an important role in treatment outcomes. This qualitative study aimed to reveal the experiences, feelings and opinions of Turkish women with infertility. The data were collected from two Internet forums between October 2016 and November 2016, and the writings of 26 women were explored. The key words “woman with infertility,” “feelings, opinion, experience and blogs” and “infertility and blogs” were browsed. The obtained data were analyzed using the method of content analysis. Those expressing feelings, opinions and experiences were underlined and codes, subthemes and themes were created by three researchers separately. Then they came together, discussed the codes and agreed on the thematic statement. The themes which emerged were psychological changes, changes in social life and changes related to treatment themes. Holistic approach and patient-specific interventions can help turn the abovementioned vicious cycle into positive.
Introduction
One out of every seven couples throughout the world experiences infertility. 1 From a psychological point of view, not having a child means an inability to give birth (functional disorder), loss of control (my body does not fulfill my wishes), psychological deficiency (inability to experience motherhood), feeling isolated by society, feeling lonely (lack of support from children), insufficient social support (no one to take care of me during old age) and not having defined social roles (mother, pregnant woman, lactating woman, mother-in-law and grandmother).2,3 Women with infertility have been reported to be more depressed than men with infertility.4–6 However, women talk about their problems, while men act as if they have fewer problems. In addition, whether they are infertile or not, women suffer more from feelings of guilt and take more responsibility. 7 In a qualitative study on the experiences of couples with infertility from North Ghana, all the women felt responsible for not having a child, and the theme “infertility is the guilt of women” emerged. 8 Infertility causes financial difficulties because medications and treatment for infertility are quite expensive. Since clinics are open during working hours, working women are often required to obtain permission from their employer when they go to treatment. 8 These researches have shown that high costs and long durations of treatment increase anxiety in women with infertility. 7
In a study by Kocyigit (2012), 48.3 percent of Turkish women were found to face social pressure after getting married with the question, “When will you have a child?” 9 In a study by Kirca, 10 57.8 percent of women with infertility were negatively affected by conversation related to children, 63.7 percent were bothered by questions about having a child, 55.4 percent felt understood only by other women with infertility, 56.9 percent experienced anger during their menstrual period and 51.5 percent had financial difficulties and failed to pay for treatment.
Many researchers have shown that infertile women’s experiences, feelings and opinions during their infertility treatment play an important part in treatment outcomes.11–14 It is of great importance that women feel well physically, psychologically and socially during their treatment even if fertility treatment fails. Therefore, health professionals should be aware of the feelings, opinions and experiences of women with infertility and design appropriate interventions based on a holistic approach. This qualitative study aims to identify experiences, feelings and opinions of Turkish women with infertility.
Method
Sample and study design
A qualitative design was used, and data were obtained from two Internet forums by passive analysis technique. We used an online search engine, Google, and performed a search utilizing the terms “woman with infertility,” “feelings, opinion, experience and blogs” and “infertility and blogs” between October 2016 and November 2016 to determine the sample. After three iterations, no additional unique and relevant threads were found. As a result of search, 14 blogs were reached. All blogs were viewed independently by three authors, and two blogs were selected as most related to topic. In these blogs, there were headings related to feeling, opinions and experiences that were parallel to our purpose. In other blogs, the shares were generally under the headings related to techniques of infertility treatment. At the same time, selected blogs were most frequently used blogs by infertility women in Turkey. Besides in this discussion boards, women can post a message or comment related to the topic at hand. On this platform, women could create new headings or could write under available headings. After the blog selection, the feelings, opinions and experiences expressed by 26 women who have received or are currently receiving treatment for infertility were included in the analysis.
Data analysis
Obtained data were screened using directed qualitative content analysis. Comments taken from the blogs were carefully read through several times to get a general sense of the information and to ensure the accuracy of the data analysis. When evaluating the data, we paid attention to the fact that our beliefs and values did not affect the interpretations of the data. During the thematic analysis, three researchers independently read all transcripts and determined codes. After this evaluation, the codes and subthemes were combined to form themes. The researchers carried out the analysis steps themselves independently. Then they came together, discussed the codes and agreed on the thematic statement that best described the findings. 15
Ethical considerations
The ethical evaluation was determined by the Dokuz Eylul University’s Non-interventional Ethics Committee (Decision number: 2016/29-03, protocol number: 2997-GOA). Women included in the study used a nickname to make comments. We used numbers instead of nicknames when we demonstrated the expressions in the text. In this research, only the numbers that were given by researchers were supplied, and no other information about the participants was provided. According to the passive analysis, there was no need for informed consent because no registration was required for women to take part in these public forums. These forums were online and openly accessible. Since shared comments are open to the public, it has been accepted as implied consent.
Results
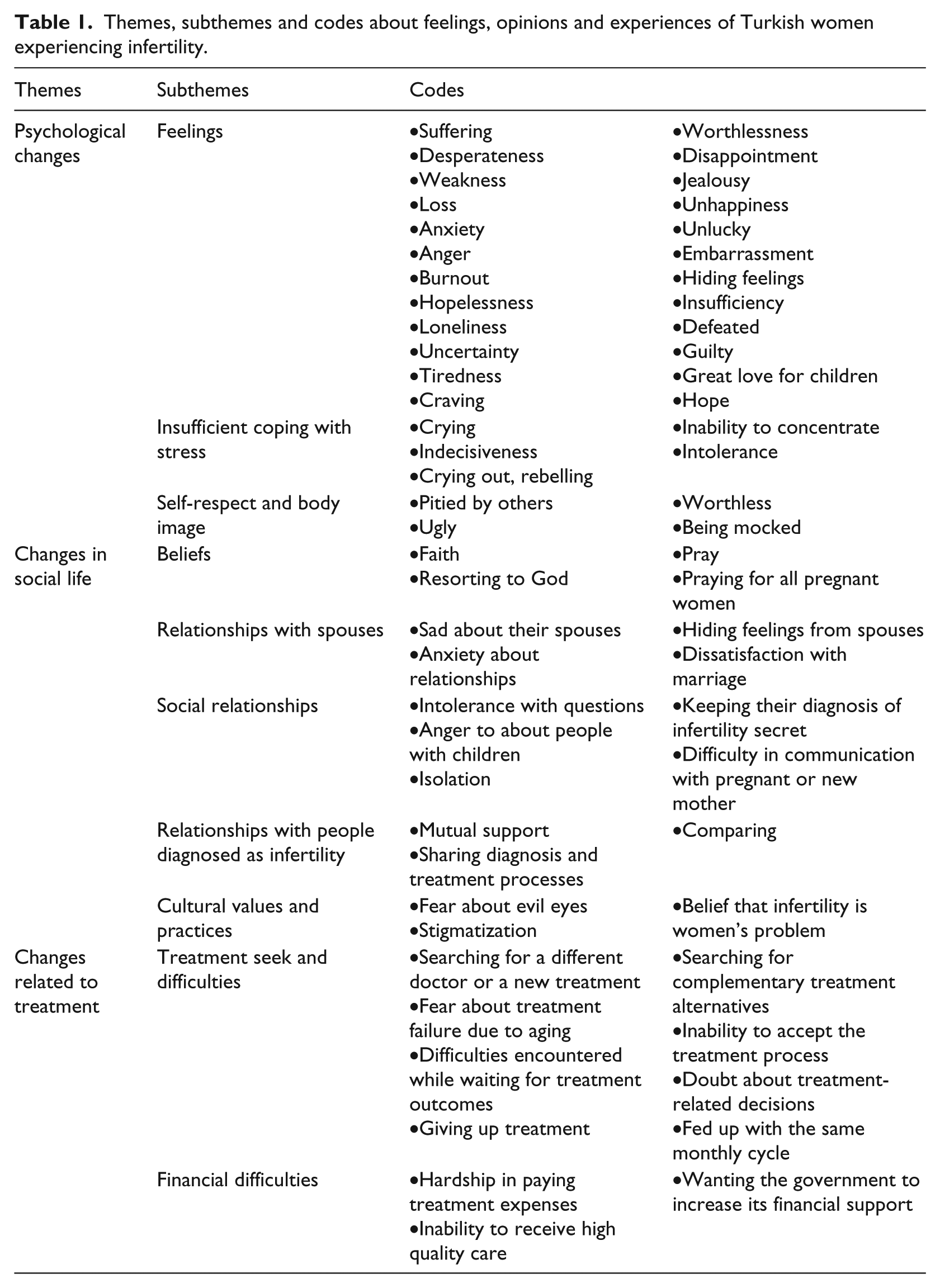
The content analysis revealed 3 themes, 10 subthemes and 63 codes (Table 1).
Themes, subthemes and codes about feelings, opinions and experiences of Turkish women experiencing infertility.
Psychological changes
Feelings
Women expressed both positive and negative feelings during the process with infertility. Subtheme feelings included the following codes: suffering, desperateness, worthlessness, weakness, disappointment, loss, jealousy, anxiety, hiding feelings, guilty, uncertainty, tiredness, unhappiness, anger, feeling unlucky, burnout, hopelessness, embarrassment, loneliness, insufficiency, defeated, craving, great love for children and hope: … most of the time I feel weak and I say I’ll never have a child. I can’t find a solution; it’s a vicious cycle. (4) All women around me are pregnant. Frankly, I’m jealous of them. (8) I have no friends or relatives left without children anymore; I feel lonely. (16)
Insufficient coping with stress
The subtheme “insufficient coping with stress” included crying, inability to concentrate, indecisiveness, intolerance and crying out and rebelling: I’ve been fed up with nonsense questions for eight years. People haven’t stopped asking those questions. I would like to cry and shout at them. (20)
Self-respect and body image
The women reported decreased self-respect and negative body image. The subthemes for self-respect and body image involved the codes of feeling pitied by others, worthless, ugly and being mocked: I feel as if people pitied me. I feel as if they (pregnant women) were the luckiest people in the world and very precious, but I were miserable. (5) Now four of my close friends are pregnant. I feel terrible when they are around. Even their praying makes me feel as if they pitied me. (21)
Changes in social life
Beliefs
Fertility problems are sometimes considered by women as a part of faith, or women expect God to find a solution to infertility. The subtheme “beliefs” included the codes faith, prayer, resorting to God and praying for all pregnant women: I’m going through a period I have no hope. I hope God gives me the best. I expect that I and other infertile women will feel content one day. (9)
Relationships with spouses
Some women blamed their spouses, whereas others felt guilty—hiding feelings from spouses, sad about their spouses, dissatisfaction with marriage and anxiety about relationships: Men do not experience anything bad because nobody insinuates that they can’t have children. (11) I’ve stopped worrying about myself; I’m worried about my husband. (10)
Social relationships
Women reported that they tried to stay away from their social network. Subtheme included intolerance with questions, isolation, anger toward people with children, difficulty in communication with pregnant people or new mothers and keeping their diagnosis secret: I don’t call my friends who I haven’t seen for a long time. I’m worried that they might be pregnant. (5) … My husband has told me the wife of a friend is pregnant (I don’t understand why he gives this news to me!!!) We’re attending a wedding ceremony at the weekend. She will definitely be at the ceremony. I can’t stand seeing pregnant women … (5)
Relationships with people diagnosed as “infertile.”
The women admitted that they felt more comfortable when they shared their infertility with other women having the same problem. Mutual support, comparing experiences and sharing diagnosis and treatment processes were codes determined in the relationships with people diagnosed as “infertile” subtheme: I wish all childless women would have a positive pregnancy test result. (1) … Same here. We, childless women, understand each other. Others cannot understand us. (13)
Cultural values and practices
This subtheme comprised the codes fear about evil eyes, stigmatization and the belief that fertility is the women’s problem: … We met after she became pregnant, but she didn’t tell me she was pregnant. I’m not sure, but she might have fear about evil eyes. (23) My mother-in-law has always called me childless. Now I know that she is right (looks upset). (9)
Changes related to treatment
Treatment seeking and difficulties
This subtheme included searching for complementary treatment alternatives, searching for a different doctor or a new treatment, inability to accept the treatment process, doubt about treatment, fear about treatment failure due to aging, difficulties encountered while waiting for treatment outcomes, giving up treatment and being fed up with the same monthly cycle: First, why did he prescribe Klomen? How did he know whether I had ovulation or not? (18) I was really fed up with this sad period every month. (11) I searched for a lot of information about inability to become pregnant. I tried many cures such as onion juice and figs. (2)
Financial difficulties
Hardship in paying treatment expenses, wanting the government to increase its financial support and inability to receive high-quality care were expressed as financial difficulties: I would like to ask the authorities to provide infertile women with discounts in private clinics … (14)
Discussion
Discussion of the findings will be considered in three main themes: psychological changes, changes in social life and changes related to treatment.
Psychological changes
The research results indicated that women with infertility experience both positive (craving and hope) and negative feelings (guilt, disappointment and insufficiency). Although some literature reviews present positive feelings of women (hope), 8 many of them confirmed negative emotions (hopelessness, disappointment, worry, anger, sadness, pessimism, loneliness and burnout).8,10,16,17 As infertility persists, the abovementioned emotional states turn into a vicious cycle.
Women with infertility also expressed that they use crying, inability to concentrate, indecisiveness, intolerance, crying out and rebelling as methods for coping with stress. Tabong and Adongo 8 reported that women preferred overcoming stress by being away from things that reminded them of childlessness. In the Turkish culture, women are considered responsible for becoming pregnant and having children; the inability to have a child is thought to be the women’s fault. Motherhood is compulsory in many developing countries, and many girls are trained for this role; therefore, there are direct psychosocial consequences for infertile women. This is believed to increase women’s stress. Women cannot ask for help in dealing with stress because they hide fertility problems. They often resort to ineffective coping methods due to a lack of support.
One of the important findings was lower self-respect and disrupted body image due to changes in psychology and social life. In a study on Canadian couples presenting to an in vitro fertilization (IVF) center, both women and men defined their senses of self and bodies as a broken machine. 18 In a study by Kohan et al., 19 women unable to become pregnant were found to suffer from distorted body images due to their impaired reproductive functions. Behboodi-Moghadam et al. 20 stated that women felt incompetent and had decreased self-respect. In Turkish culture, womanhood is identified as the capacity to have children. Therefore, women unable to have children cannot consider themselves women. They may feel that they cannot fulfill their roles and therefore dislike themselves.
Changes in social life
Women in this study associated the problem of fertility with faith, and they expected God to solve this problem. The most important tendency in Islam is to trust God without questioning; both well-being and health come from God. Women mostly think that they have infertility because it is the will of God. They depend not only on medical treatment, but also on religious and non-religious aspects such as faith, luck, fortune, magic, amulets, oblations and visiting shrines. 9 All of these are thought to originate from Islam and Turkish culture.
In the present study, women sometimes blame themselves, and at other times, they accuse their spouses. As they identified marriage with having children, the inability to have a child caused changes in their relationships with their spouses. Kocyigit 9 reported that the most important difficulty experienced by more than half of the infertile women (54%) was the feeling of incompetency when they saw their spouses showing affection for other people’s children. Another research revealed that it is the women who felt guiltier and more responsible for not having a child, whether they themselves were infertile or not. 7 Kirca 10 reported that 75.5 percent of the women studied expected their spouses to understand their feelings and that 80.9 percent of the women wanted their spouses to be tactful. Tabong and Adongo 8 stated that women were not happy with their marriage, as they could not have a child. They also mentioned that all the women found themselves guilty of infertility. 8 In a study by Ranjbar et al., 21 the women felt guilty because they could not give birth. Steuber and Solomon, 22 in their study on online blogs, found that women either blame themselves or couples accused each other. Jedrzejczak et al. 23 reported that infertility created a serious problem in marriages among 25 percent of the couples. In Behboodi-Moghadam et al.’s 20 study, most of the participants commented that their spouses did not trust them any longer and did not show interest in them. They were also worried that their spouses might get married to another woman to have children. 20 Although having a child is supposed to be achieved by couples together, women shoulder the responsibility by themselves. Therefore, they hold either themselves or their spouses responsible for infertility. Since they identified marriage with having children, they thought that infertility caused changes in their relationships with their spouses.
In the present study, infertility was found to have a negative impact on the women’s social relationships. They wanted to be away from their social network. Behboodi-Moghadam et al. 20 reported that most of the women were not willing to participate in social activities and wanted to be alone. In a study in South Africa, the women commented that they felt stigmatized and mocked by their spouses’ families. 8 Kocyigit 9 revealed that nearly half of the women (48.3%) were exposed to social pressure and that the first step of this pressure was to answer the question of when they would have a child. In addition, more than half of the women (54%) admitted that the most important part of infertility was social pressure. They explained that they had to tell other people why they could not have children, felt stressed out when there were children around, had a burning desire for having children when they saw parents showing affection and love for their children and felt terrible when their peers had children and when their mothers-in-law threatened that they might have to get divorced, or might have to live with a “kuma” (a woman with whom married men can live in the same home with their wives without having a formal marriage in some parts of Turkey). 9 In Turkish culture, giving birth is considered the first responsibility of the women. People start to ask questions about having children after couples get married. Women who are unable to have children are incriminated for incompetence and unproductiveness and treated as if they were inferior to other women. They are treated as if they were a broken machine that has to be replaced.
In the current study, women were found to contact other women to talk about their diagnosis and treatment, as they felt more comfortable with them. They provided support for each other, compared their experiences and shared their diagnosis and treatment experiences. In general, women themselves start medical treatment, and they are more determined during treatment. 24 In a study by Kirca, 10 55.4 percent of the women felt that other infertile women could more easily understand what they experienced. In view of the results of the present study and the literature, women seem to feel more responsible and attempt to search for treatment alternatives more often than men. As a consequence, it is not surprising that they play a more active role in diagnosis and treatment of infertility.
We revealed that the women who were worried about evil eyes felt responsible for infertility and stigmatized. Women had difficulty accepting the outcomes of treatment and attributed their inability to have a child to medical treatment’s insufficiency. They also incriminated evil eyes for infertility. It is believed that people with evil eyes or malicious intentions may cause women to have bad experiences. These women may resort to traditional practices or religious leaders to get rid of evil eyes.
Changes related to diagnosis and treatment
In the present study, the women commented that they sought complementary treatment alternatives, different doctors and new treatment alternatives, had doubts about treatment-related decisions, had fears about treatment failure due to aging, sometimes gave up treatment and were fed up with the same treatment cycle every month. Kamaci 16 found that 28 percent visited religious leaders and shrines to ask for help and that 7 percent of the women took herbal medicines. The researcher also discovered that half of the couples hoped to benefit from traditional practices. 16 In a study by Engin and Pasinlioglu, 25 all the women knew about traditional medicine used to treat infertility, 71 percent of the couples applied them and 61 percent of the women using these methods experienced health problems. Kilic et al. 26 revealed that infertile women were recommended to perform some alternative treatment methods. Among them were eating or drinking mixtures of various plants, vegetables and fruit, sitting over vapors of some mixtures, having a rest for a minimum of 30 min after sexual intercourse, using vacuum therapy on their backs, bathing in thermal hot springs and putting raw meat or vegetables on their abdomens. One example of mixtures recommended contains hot water, milk, kale, straw, dead nettle and/or onions. Half of the women were found to use these methods before and during medical treatments for infertility. One woman admitted that she fried an egg with olive oil, covered it with a piece of thin, cotton cloth and put it on her underwear just before medical treatment. Some of the abovementioned treatment alternatives can jeopardize the biological well-being of women with gynecological problems. It is clear that women can try a wide variety of alternative traditional methods to find a cure for infertility. 26 Since treatment for infertility is usually given to women, they think that they are the only person who can solve the problem. When medical treatment fails, they try every method they hear about. Lee et al. 27 showed that time from transfer and implantation of embryos to conception was the most stressful stage of IVF and embryo transfer (IVF/ET) treatment. Women can have conflicting feelings such as anxiety and happiness during this period. Those going through this period and then experiencing treatment failure feel incompetent, empty, guilty, sad and unsuccessful and have severe mourning reactions. 27 Ranjbar et al. 21 emphasized that the women tried many treatment alternatives including ovulation induction, intrauterine insemination and intracytoplasmic sperm injection and found it difficult to wait for test results. Peddie et al. 28 commented that the women had difficulty in deciding to continue or discontinue treatment and often searched for information about treatment. They make many sacrifices, are eager to receive treatment and endure many difficulties during diagnosis and treatment. When they experience treatment failure, they get tired, but they restart their treatment because they think that having a child is their duty and that inability to achieve it is their fault. They do everything they can to compensate this guilt.
Infertility has not only physiological and psychological effects, but also financial effects on women. In the current study, the women mentioned hardship in paying treatment expenses, inability to receive high-quality care and an expectation for authorities to provide them with financial support. Kirca 10 also reported that 51.5 percent of the women experienced financial difficulty in paying treatment costs. Working women also must take off from work for their treatment. 29 They may have to stop working or following their career paths. High costs and long durations of infertility treatment may play a role in the financial difficulties experienced. 7 Ranjbar et al. 21 mentioned that unemployed women could not afford to pay treatment expenses and depended on their spouses. Tabong and Adongo 8 underlined the high costs of treatment for infertility and revealed that some women had to give up treatment due to these high costs. Similarly, in a study by Peddie et al., 28 one reason for stopping treatment was financial difficulties. In Turkey, these treatment costs are paid by couples. If they fulfill criteria determined by the state insurance system, including age and intrauterine insemination, only a small amount of the expenses is paid by the government. Work leaves for treatment also cause some deductions in wages. Women living in small towns have to travel to big cities where they can access treatment facilities and have to pay for transportation and accommodation.
The results of the study show that women need holistic approach. The holistic approach embraces individual’s psychological, sociological and mental needs. 30 Because of that in clinics, health professionals should not forget that as a whole psychological, sociological and mental support is needed.
Conclusion
We suggest that women with infertility mostly experience negative feelings, opinions and experiences during diagnosis and treatment for this condition. Conversely, diagnosis and treatment processes may increase negative feelings, opinions and experiences. Holistic approach and patient-specific interventions can help turn the abovementioned vicious cycle into a positive experience. Women with infertility should be provided with environments where they can express and convert their negative feelings, opinions and experiences into positive ones. More detailed qualitative studies are needed because infertility is a person-specific problem that is difficult to express. This study was performed only on women. Since fertility problem affects both women and men, further qualitative studies are needed that involve couples.
Footnotes
Authors’ contributions
S.M., S.F. and M.A.T. contributed to the study design. S.F. contributed to the data collection. S.M., S.F. and M.A.T contributed to the data analysis. S.M., S.F. and M.A.T. contributed to the article preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.