
Abstract
Health-based electronic games present an innovative tool to deal with mental and behavioral disorders as well as physical. An appropriately designed game can optimize health care. The aim of this study was to establish a design for health-based electronic games model and to develop a sample game in diabetes. This study was carried out in two phases: first, the design of a health-based electronic game framework and second, the design and production of sweet care game. There were two intended information prerequisites: determination of effective components in models of behavior change and validation of these components on health topics and structural formation of a game. The game framework design was presented. In the second phase, a sample of the game was developed in the field of diabetes. Important components to empower people were ranked using the Friedman test in the following order: self-learning, treatment, mental empowerment, condition management, healthy eating and physical activity. The axis of self-learning received the highest rating from the perspective of the subjects with an average of 3.93 percent. Another part was the game framework with components as follows: application areas, educational content for change behavior, resources, game structure and game production. Finally, the sweet care game was designed on diabetes with educational, technological and clinical content. The health-based electronic game designed on a systematic framework could be applied as a tool to expanding the knowledge base on how to create effective health-based digital games that entertain while promoting behavior change.
Background
Today, extensive advances in medicine and health care have somewhat diverted physicians’ attention from communicating with their patients through providing modern equipment and techniques, strong and aggressive treatment and effective drugs. Research had highlighted the importance of effective communication with patients and training for successful treatment. 1 Health education is achieved by promoting physical, social, spiritual and psychological well-being in various social groups through training and practical skills. Applied scientific approaches to e-learning can direct people toward adopting healthy behavior and lifestyle. Avoidance of high-risk behaviors such as inactivity, obesity, unhealthy recreational pursuits and an individuals’ attitude to their own health is largely dependent on their level of health literacy. Enhancing health literacy among a wide range of people requires a scientific and rational approach to health education. This type of training can have a significant effect on an individuals’ self-efficacy as a self-empowerment indicator of success in the field of physical and mental health. Therefore, innovative methods and new technologies should be adopted to facilitate health education.2,3
Unfortunately, health among populations in many countries is changing rapidly due to changes in dietary patterns; particularly related to people’s tendency to consume high-calorie and low-value food and to partake in minimal physical activity and consume more tobacco and alcohol; these unhealthy lifestyle choices make communities vulnerable to future epidemics of non-communicable diseases. 4 One of the most important of disease is diabetes. Diabetes is a global health problem. Its prevalence is increasing worldwide at an alarming rate, and according to the World Health Organization’s report, by 2030, diabetes will be the seventh leading cause of death. The number of people with diabetes has been estimated to grow from 171 million in 2000 to 366 million by 2030. 5 Currently, over 4.5 million people are diabetic in Iran in 2015. 6
Therefore, to empower individuals, policy makers and researchers have increasingly focused on management of chronic diseases such as diabetes and are currently researching interventions and strategies for chronic disease management in different classes of society. Application of health-based games has been applied as a new digital media tool to empower patients. Health-based electronic games are innovative tools that deal with mental and behavior disorders as well as physical factors in order to optimize health care. This technology is presented as an interactive software program and has been designed with the main aim of entertaining individuals; it could get widespread attention and gain popularity among socioeconomic groups. The benefit of this tool is not limited to entertainment. These games are presented in variety of styles depending on the purpose for which they are designed. Health-care games are among the most widely used digital games. This type of game is designed to transfer values and generate ideas. Such games train the mind in an optimum fashion to improve behavioral, physical, cognitive and emotional functioning.7,8
There is an obvious need to design and create technology that clearly defines the design process of this modern and effective tool. Research also needs to focus on how electronic games can help people learn to make healthy lifestyle choices and optimize disease management. Since the information framework cannot be used by itself for game development, an operational framework must be provided for evaluation in conjunction with the key points of design process.
Issel 9 maintains that a project designed primarily with subjective evaluation is more likely to result in useful performance of data in the development process. Anderson states that the basis for an effective operational framework is accurate, and appropriate understanding of the program was developed as well as application of the necessary resources. Clarity about the objectives and targets is also important. 10 In the conceptual model designed by Thompson for a serious video game for diabetics, entertainment was considered as the main factor promoting change to healthy behavior in the input component of the model, and behavioral change was considered as the core of the model in the process section. Other considerations were knowledge, skills, self-efficacy and motivation as axes in this model that formed the main framework along with other design principles of the game. 11 In a theoretical model in the field of designing Packy and Marlon Game, Brown considered the mechanism of behavioral change as the fundamental platform; self-concept (self-esteem, self-efficacy), social support (consultation, public relations), knowledge (information, skills, intelligence) and self-care (diet, self-control, self-medication) as intermediate variables; input of this framework as game characteristics (entertainment, role-playing, interaction, learning) and output as results affecting health. Packy and Marlon is an action-adventure side-scrolling Nintendo console game for children and adolescents with type 1 diabetes. Other example of research and development with game system to address childhood disorders can be seen in the development of a Glymetrix Diabetes Game that has been used for testing attention processes in children with diabetes. In Glymetrix Diabetes Game, researcher provides quiz games and card games that test players’ knowledge about diabetes self-management. The games are integrated into an extensive clinical system that supports patients and clinicians in the management of diabetes. 12 “GRIP” is a Dutch language diabetes self-management game designed to connect health information from the patient’s personal electronic medical record file to a game in which players learn to make decisions and develop skills based on their current personal health information. The game enables parents and clinicians to monitor the patient’s condition over time. Players observe how daily activities and food choices influence blood glucose levels.13,14
Jianhong’s framework was also based on a mechanism of behavior change by designing a game for asthma management. There were positive results of this game for its players, and these included a significant increase in knowledge about asthma, self-efficacy in disease self-management, self-efficacy in social communication in spite of suffering from the disease and improved relationships with family members and peers. 15 Amri Yusoff combined learning and training theories presented with game requirements in a conceptual framework for serious games. The study aimed to develop an operating model for use by game designers, clinicians and behaviorists. The report suggested that learning could occur at any part of model through playing. 16 In a study titled “Conceptual framework for designing games for cognitive rehabilitation traumatic brain injury,” ElakLouke provides guidance for practical and effective design of cognitive rehabilitation games. The proposed framework consists of four parts: conditions, processes, activities and results .In his opinion, each component played a significant role in effective design based on cognitive interventions. The general objective of all these efforts was to engage individuals in interactive games aimed at empowerment of their players. Serious digital games have been developed to promote a positive attitude in users by instilling information aimed at chancing behavior. Despite considerable research in the field, there remains a lack of theoretical support for behavioral sciences, including poor game assessment by designers during the construction phase and a lack of attention to the operational framework prior to design. This has been a challenge for game design in recent years. 17 Finally, it can be argued that without a clear framework as a guideline for developers, it is very difficult to justify the claim that a game can meet its objectives. But a health-based game designed according to appropriate considerations has the potential to improve self-management in various diseases. Nowadays, games have been designed on systematic frameworks that aim to change user behavior. However, more research attention is needed in planning for new technologies, such as appropriate health-based electronic games and identification and management of games technologies in order to maximize their potential. Accordingly, the researcher aimed to provide a collection game framework by considering the needs appropriate to and health structure in a country. In order to make the design operational and to evaluate its technical performance, the technology was applied to diabetes by designing a sweet care game.
Methods
This study was conducted in two phases: (1) design of health-based electronic game framework (three steps) and (2) development of the sweet care game (Figure 1).
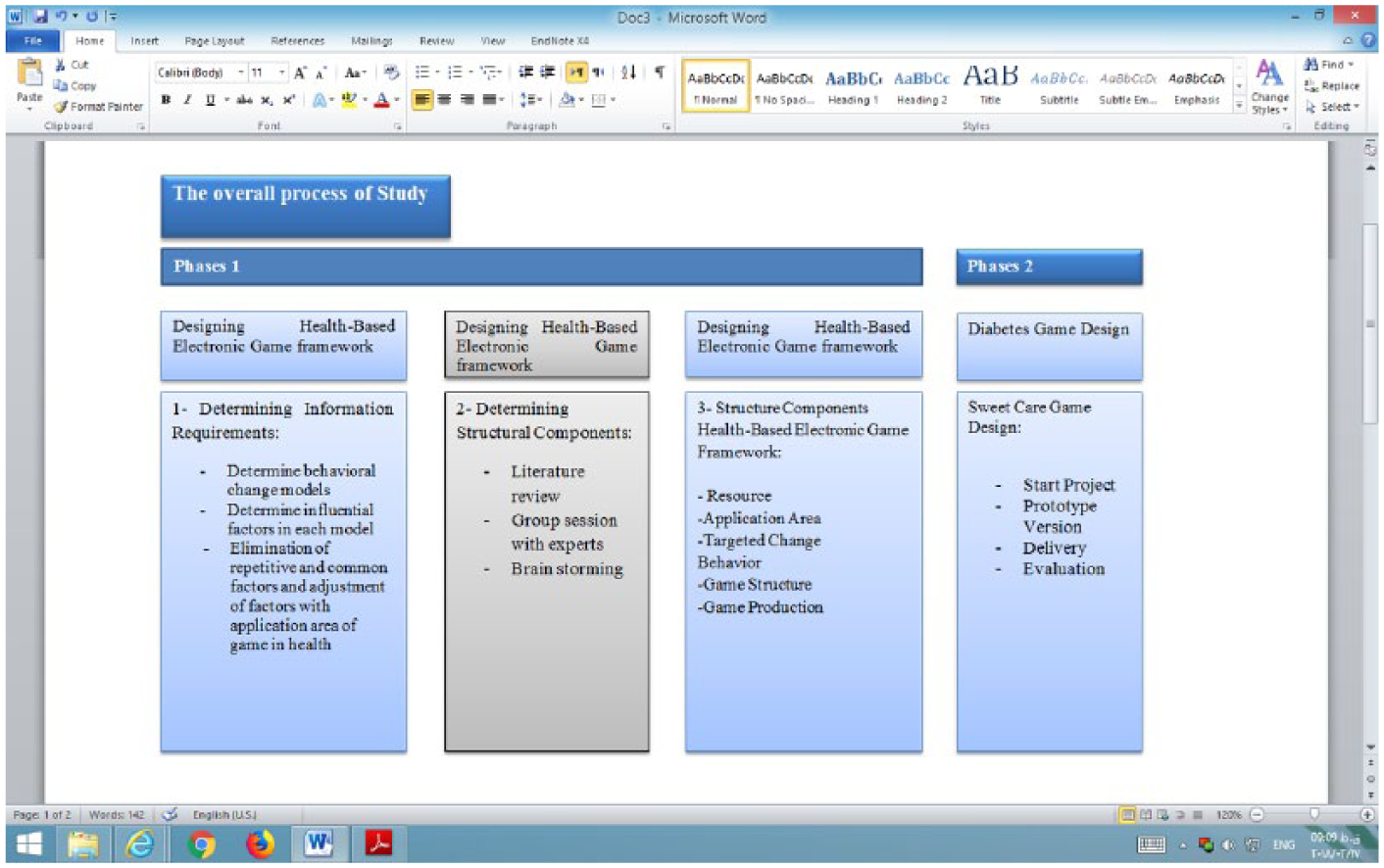
Study method.
Designing health-based electronic game framework
Determining information requirements
Health information content constituted the conceptual framework of the game model. This framework helped to explain the components that empowered individuals by enabling them to protect themselves and to determine the key points of intervention and the best strategies for achieving the goal. The most fundamental goal of health education is to change human behavior or to promote continuity of preferential behavior. Therefore, the goal of health education is defined as the way in which goals, progress and success can be achieved in public health through medical innovations 2 and learning principles, theories of human behavior and models in a comprehensive framework of how people learn and how and why they behave in certain ways. In addition, theories can provide a framework for effective intervention to change behavior. A person’s behavior plays an important role in management, prevention, treatment and a person’s ability to cope with disease. To reach the ultimate goal, which is to maintain and improve health, achieving behavioral change is the start of a process that automatically promotes health. 18 In this study, after identification of sources of information and according to the research team’s opinion based on Delphi technique, the following nine common models were investigated: health belief model and behavior change, 19 behavioral intention model, 20 PRECEDE model, 21 Simon’s model, 22 BASNEF model, 23 planned behavior model, 24 protection motivation model, 25 social recognition 26 and trans theoretical model. 27
At this stage, a set of behavior change models within the framework of the Delphi framework was provided for a group of experts (research population). At the first stage of Delphi process and within relevant questionnaire, research population was asked in addition to determining the relative importance of each of the proposed models (on five-point Likert-type scale) to provide their desired models that were not mentioned in the stated model. The criteria for deciding on indicators were determined as follows (Table 1).
The criteria for deciding on indicators.

As according to the experts’ view, all the proposed models have the median score of 4 or 5 (score 1 = marginal importance, 2 = low importance, 3 = moderate importance, 4 = very important and 5 = very high importance), and the second stage of Delphi was not done and the results of the first stage were sufficed. After confirming the content validity of the questionnaire with the help of five members of experts’ team, reliability of the questionnaire was confirmed with Cronbach’s alpha measurement (91%).
After confirming the validity and reliability of the questionnaire, questionnaire was provided for experts via email; 67 percent of questionnaires (equivalent to 62 questionnaires) were returned. Accordingly, it was concluded that based on the views of the experts’ team, all proposed models had high or very high importance.
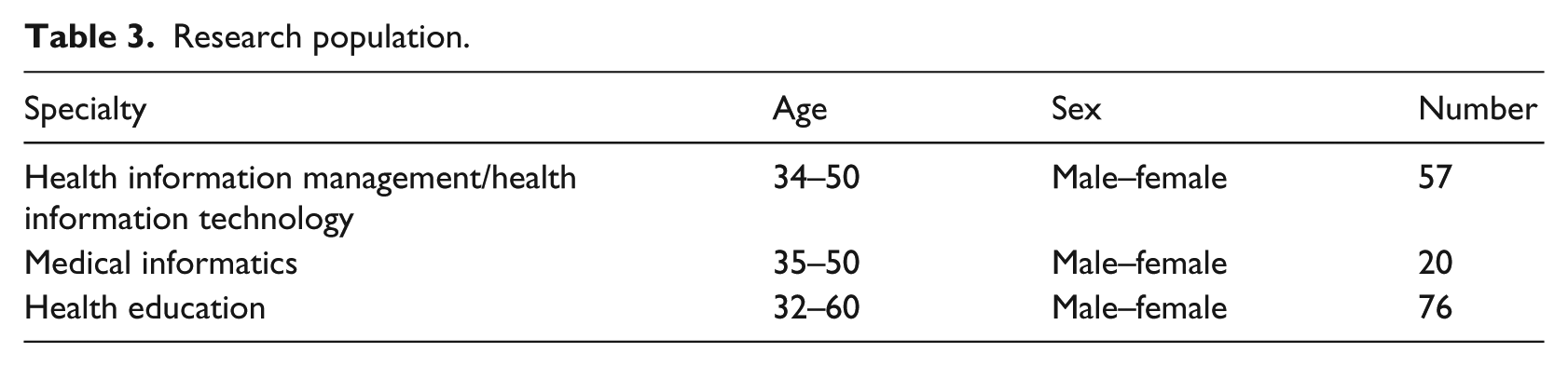
The next stage was to determine factors for each model; according to the research team, researcher eliminates duplicates and adjusts factors according to practicalities for producing the specific game (Table 2). Health-based electronic games have various areas of application depending on the goal for which the game has been designed. Among the topics studied, mental empowerment, healthy eating, condition management, education and physical activity were appropriate for application in the field of health.7,8,28–30 In the next stage, 153 professionals (Table 3) were identified on the basis of relevant departments in Iranian medical universities across the country and selected as the research population, and census was conducted accordingly.
Components of change behavior models.
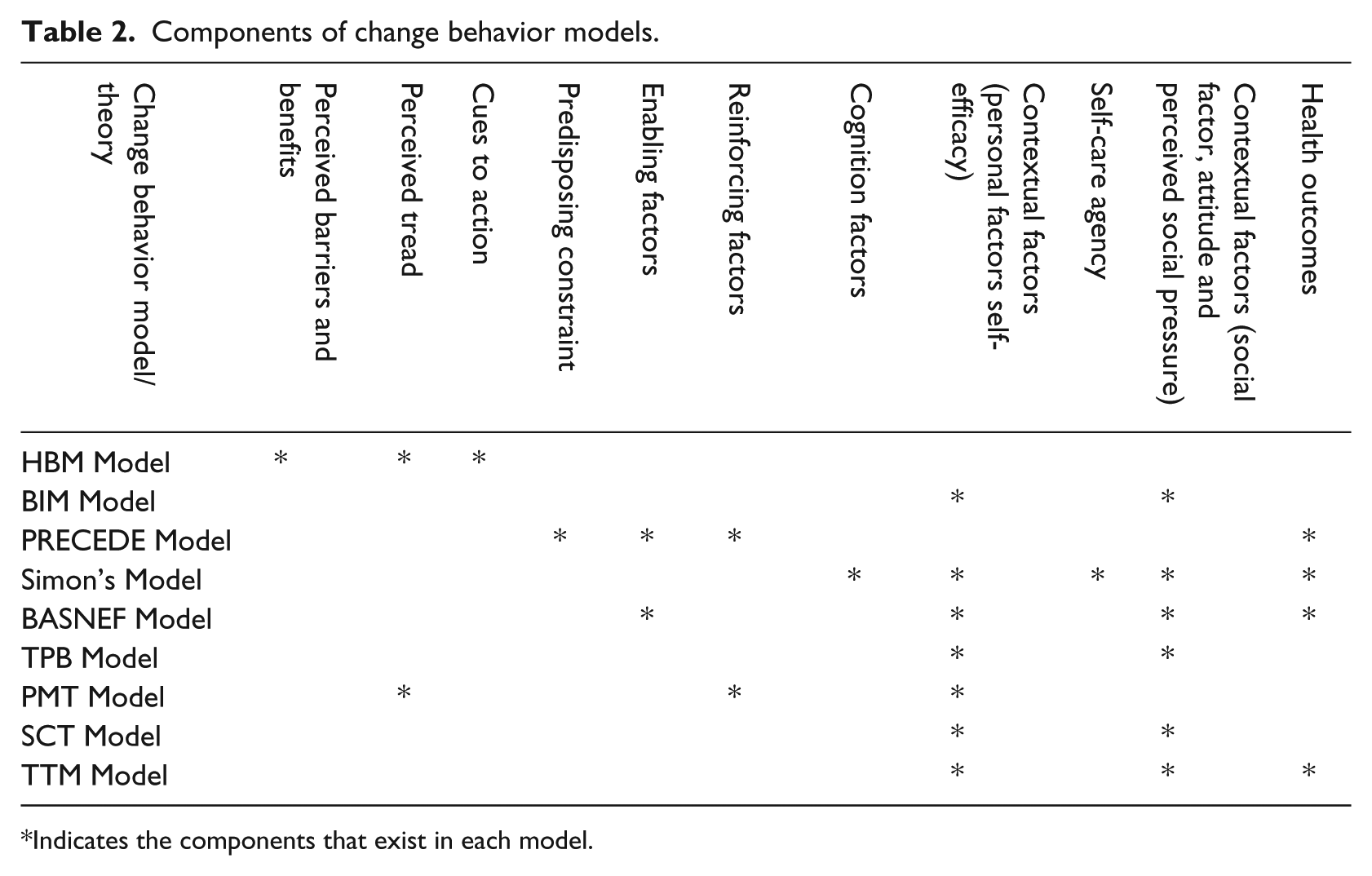
Indicates the components that exist in each model.
Research population.
The data collection tool at this stage was a researcher-made questionnaire; it had 150 questions and consisted of two criteria on two distinct areas of application; these were health-based games application area in vertical axis (healthy diet, physical activity behaviors, mental empowerment, education and condition management) and components extracted from the model of behavior change (Table 2) in horizontal axis. The degree of importance was determined as (0–5; 0 = unimportant and 5 = utmost importance). Validity of the instrument included content and face validity. Responses received from the team of experts were evaluated. Any necessary changes were made to the content later, and questions in which there were no different understandings among the individuals were corrected. After confirming content validity of the questionnaire, its reliability was measured using Cronbach’s alpha (0.97).
A period of 14 days was allowed for completion of the questionnaire; while sending the questionnaire, subjects were asked to complete and inform researchers when it was completed by sending it via e-mail. A number of subjects were excluded because they expressed unwillingness to complete the questionnaires; some sent it back after the period of 14 days. The return rate of questionnaires was 48 percent (equivalent to 73 cases).
To achieve the research question that “which of the applied areas is preferred in determining the information requirements in game model design,” the components of mentioned models in the area of behavior change were examined in six proposed applied axes. With regard to our objective, to rank the components, nonparametric test of Friedman was used. This test compares several applied groups in terms of mean and determines the rank of groups (Tables 5–8).
Determining structural components
In order to extract the structural components affecting the design of electronic game, a review of the academic literature was undertaken. Accordingly, the electronic databases such as PubMed, Web of Science, ProQuest, Scopus, ScienceDirect and Google Scholar were searched. The search strategy interchangeably used the terms “Game,” “Video Game,” “Digital Games” and “Electronic Game” in combination with the term “Technical Infrastructure,” “Technical Structure” and “Technical Content” combined with Boolean operator “AND.” Furthermore, six group sessions were held by a group of seven experts (Project Manager, Designer, Content Provider, Programmer, Animator, Graphic and Modeler) in the field of games. Different methods (Delphi group interview, brainstorming and informal interviews on the field of study) were proposed for group meetings. Here, brainstorming technique was used. Finally, the framework was presented.
Designing health-based electronic game framework
Information on key components obtained from the questionnaire was used to design the game framework, and the game structure was derived from sources and group sessions (Figure 2).
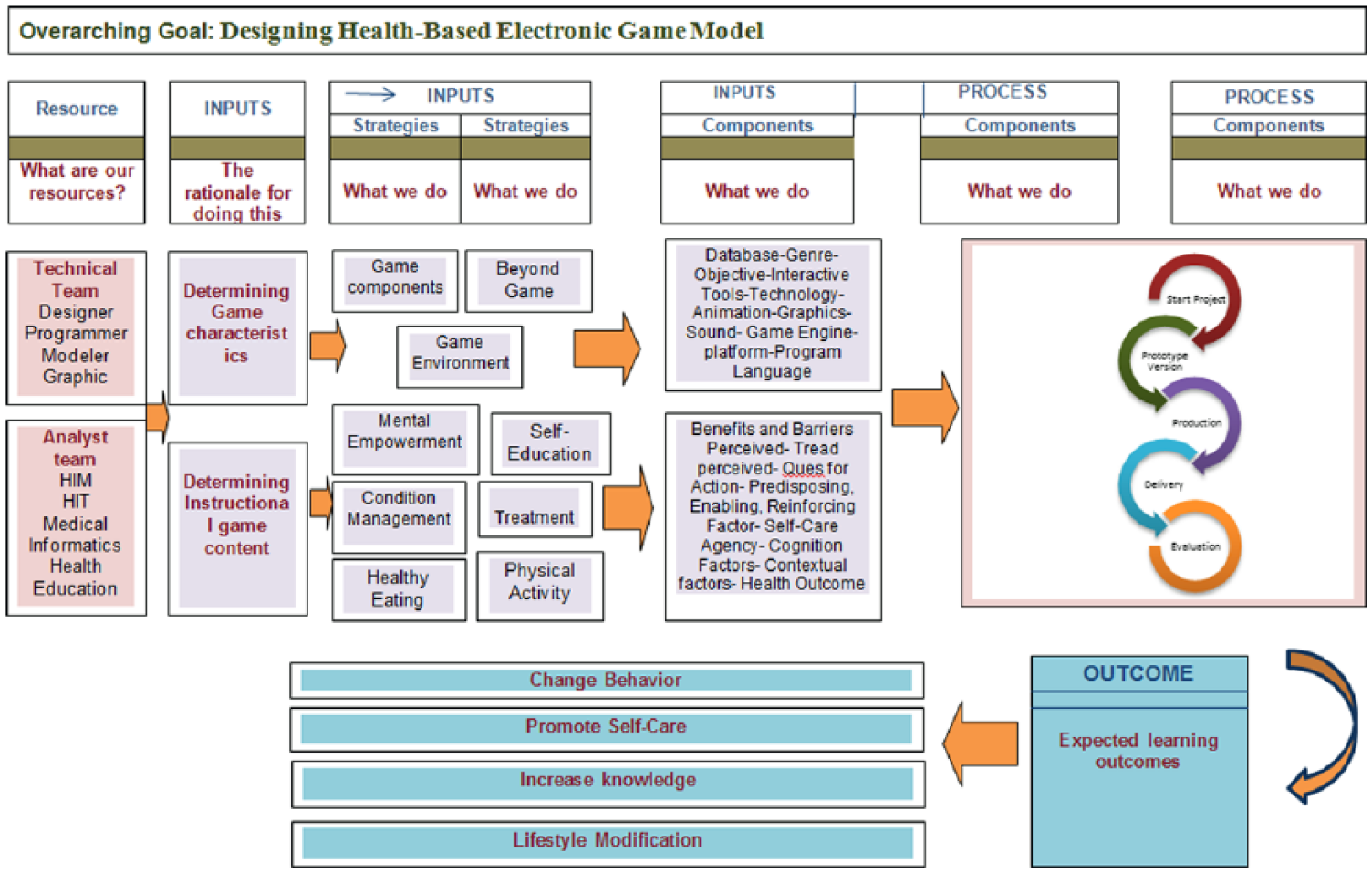
Designing health-based electronic game model.
Diabetes game design
Clinical content (non-behavioral components), educational content (expected behavioral changes) and technologic content of the game made up different parts of the game. Health content was extracted by reviewing academic texts and resources, and educational and technologic contents were derived from a health-based game model. According to analysis of data obtained from surveying information requirements in health-based electronic game model, the self-learning axis (3.93%) was the most important component and obtained the highest average rating; this explains why in the diabetes model, the self-learning sub-axes were used according to professors’ opinions.
To design health-based electronic game, mobile platform (iPhone 6 and newer/Android phones 5 and newer with at least 1 GB of RAM, ARM Cortex A5/Snapdragon 810/1.5 GHz Speed/Adreno 305 and Higher) was selected; however, it was possible to use a personal computer for displaying C++and C# programming languages for scripting. Microsoft Visual Studio–Construct 2 was the environment, in which the code was development and graphics tools included such as Adobe Photoshop, 3DS Max, Maya, Mudbox and Particle Illusion in this project. Smart SVN Source Control software was used for managing content and data inside the game and sorting them into different computer systems on which the project has been worked. Hardware and software requirements for this project were Windows Vista or newer, CPU Core 2 Duo 1.5 GHz, 100 MB of free space and 1 GB of RAM. Game experts (gameplay and game designer, animator and modeler, programmer and graphic artist) worked with the team during the design phase. Game design process was conducted in three phases: the conceptual phase, pre-production and finally prototype and production. After the formation of the basic idea of game, a draft of plan was recorded in the paper form (Figures 3 and 4)
Initial draft of plan.
Draft of plan.
According to the basic design, Game Maker Engine Construct was selected to run the game. Providing technical document of game was the next step in making the game. In this document, all the necessary information to make the diabetes game was explained.
The name and story of the game, designing the mechanics and artistic information necessary to design the characters and game environments along with details consisted of different parts of this document. Output of this part was prototype version of work.
After examining the version of the prototype, game components were run in order of priority according to the game design in the construct environment.
Figures 5 and 6 show the coding and development of menus available in the game. In Figure 5, we referred to writing the events and codes required to design the game environment (game mechanic), and in Figure 6, right menu (Table 4) information of game (store and list of purchasable items), Diabo animation, graphics and sound were added.
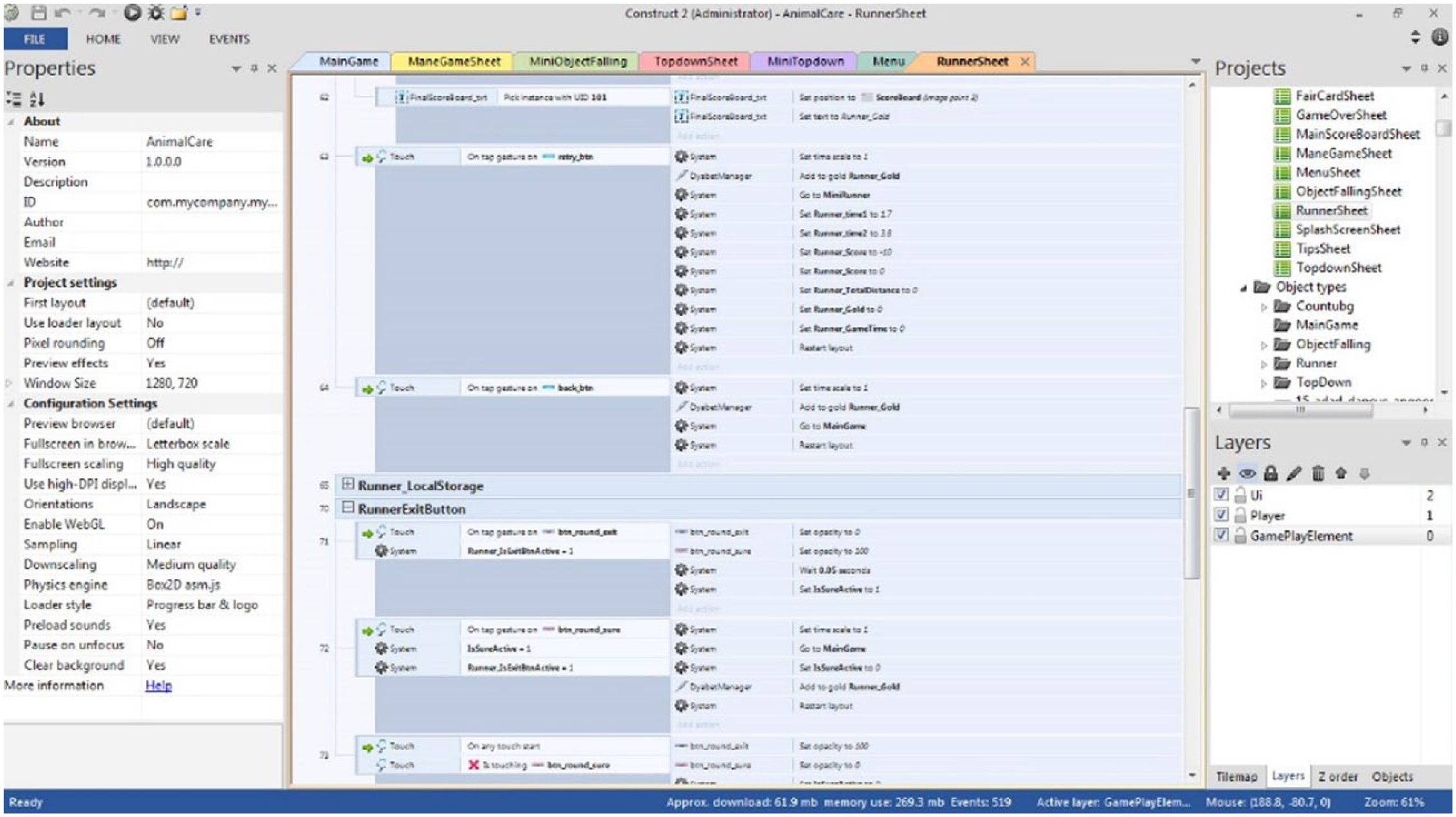
Coding and development of menus available in the game.
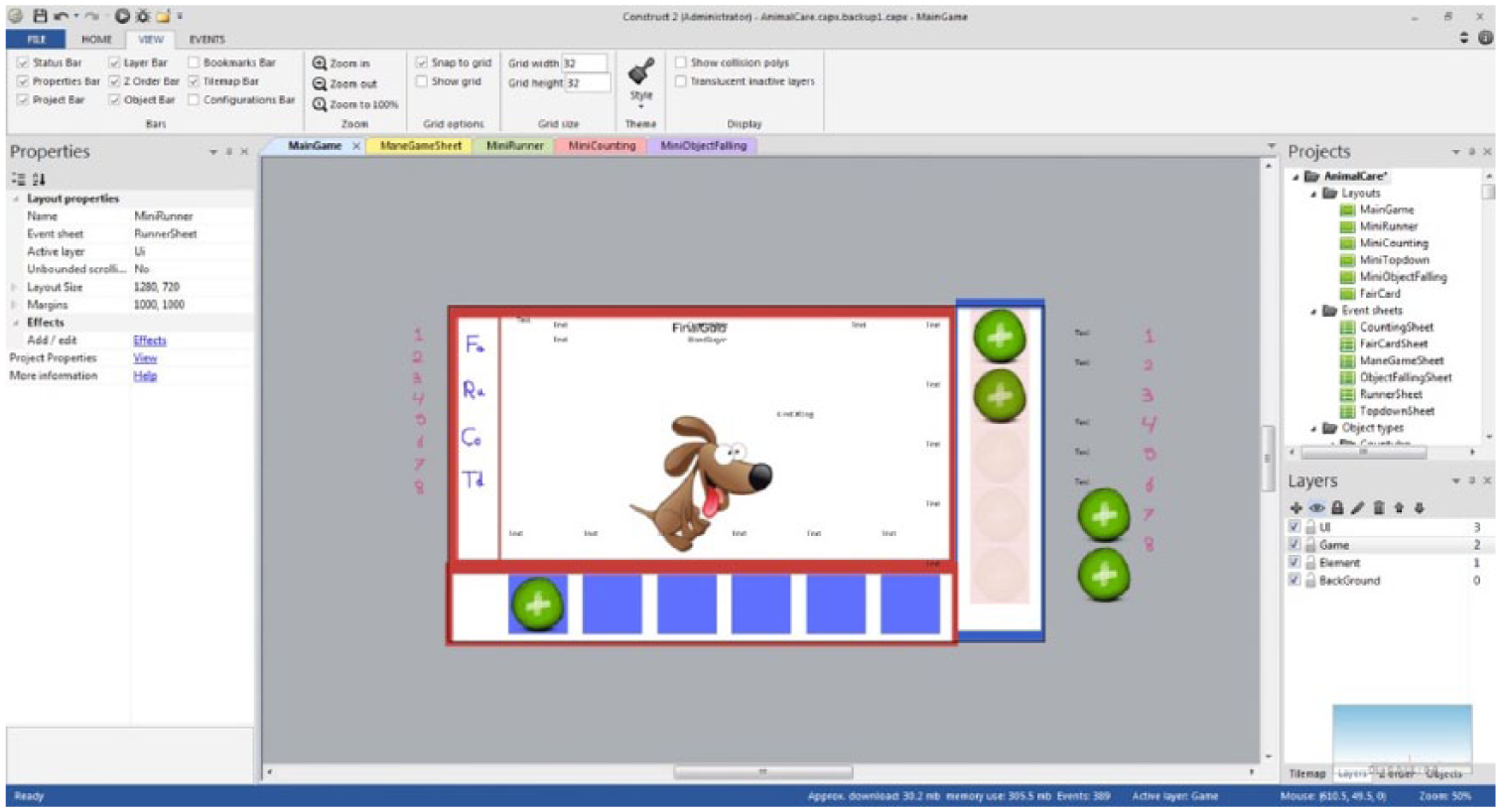
Main menu information of game.
Right menu of the game.
After running the store menu, the part related to backpack to be prepared is required, so that the process of purchasing and use of items to store to be done properly. This part is at the bottom of main page of game. Development of mini game menu is the next part of development. One of the most important cases in the diabetes game is designing the process to earn money. For this purpose and to access the entertaining mini games that have educational goal, the need to allocate space for the presentation of mini games was felt (Table 5).
Description of mini games.
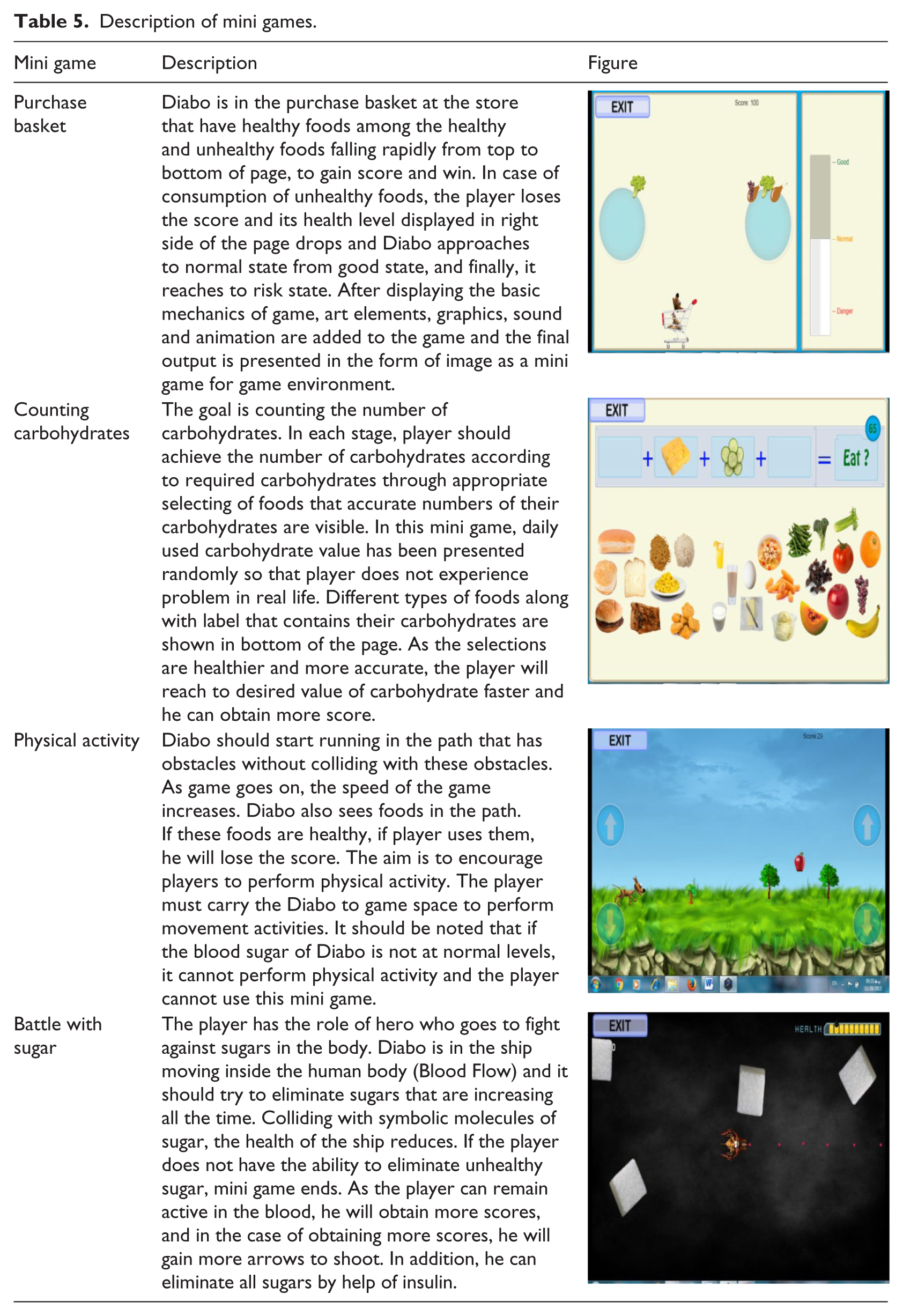
Proper running of functions, establishing relationship between mini games and creating balance with main page were considered in the next stage of game. According to the diversity of mini games and their difference in terms of running, there was need for log in and log out system, since mini games are run beside main game and their result (obtained scores) is transferred to main game.
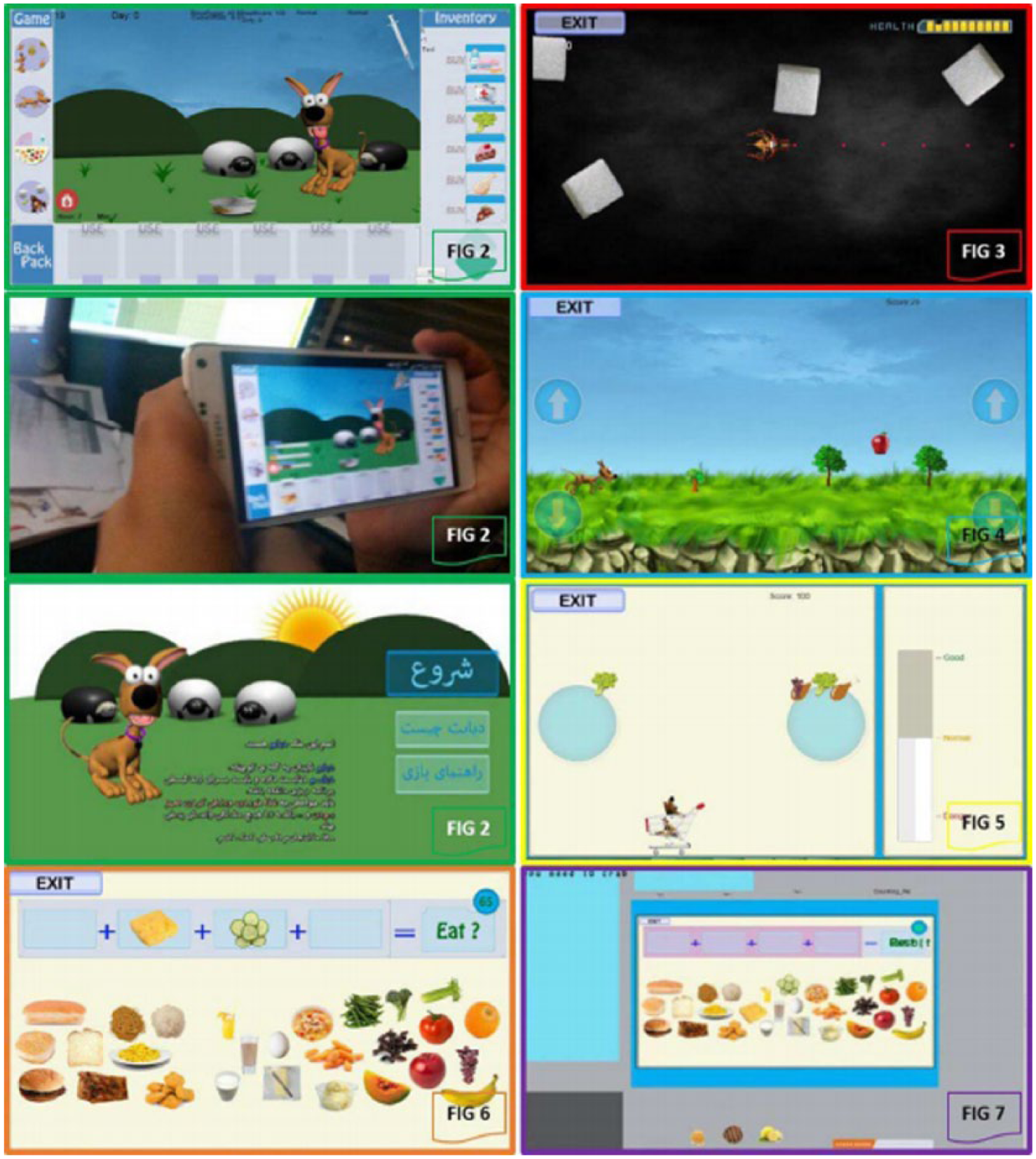
Beside design of the game and mini games (Figure 7; different parts of game design), part of the time was allocated to design the main character of game. “Diabo” was the name of a dog that has diabetes in this game. Its design is in the form of a three-dimensional model. In the first step of run, it was needed that animation to be designed as a prototype. After final testing and approval, its production stage was completed so that its output to be desirable for audience.
Development of special effects (particle), sounding, designing day and night cycle and determining scoring element were other details that they were addressed. For completion of the work, all main elements were replaced with basic mechanics. Another point is the balance of numbers system and math game that is an integral part of the game and almost everything semi-hidden of game is in the math language. Finally, game was tested frequently by testers, so that in addition to evaluation, probable shortcoming of it to be manifested and resolved before presentation and game releasing.
Results
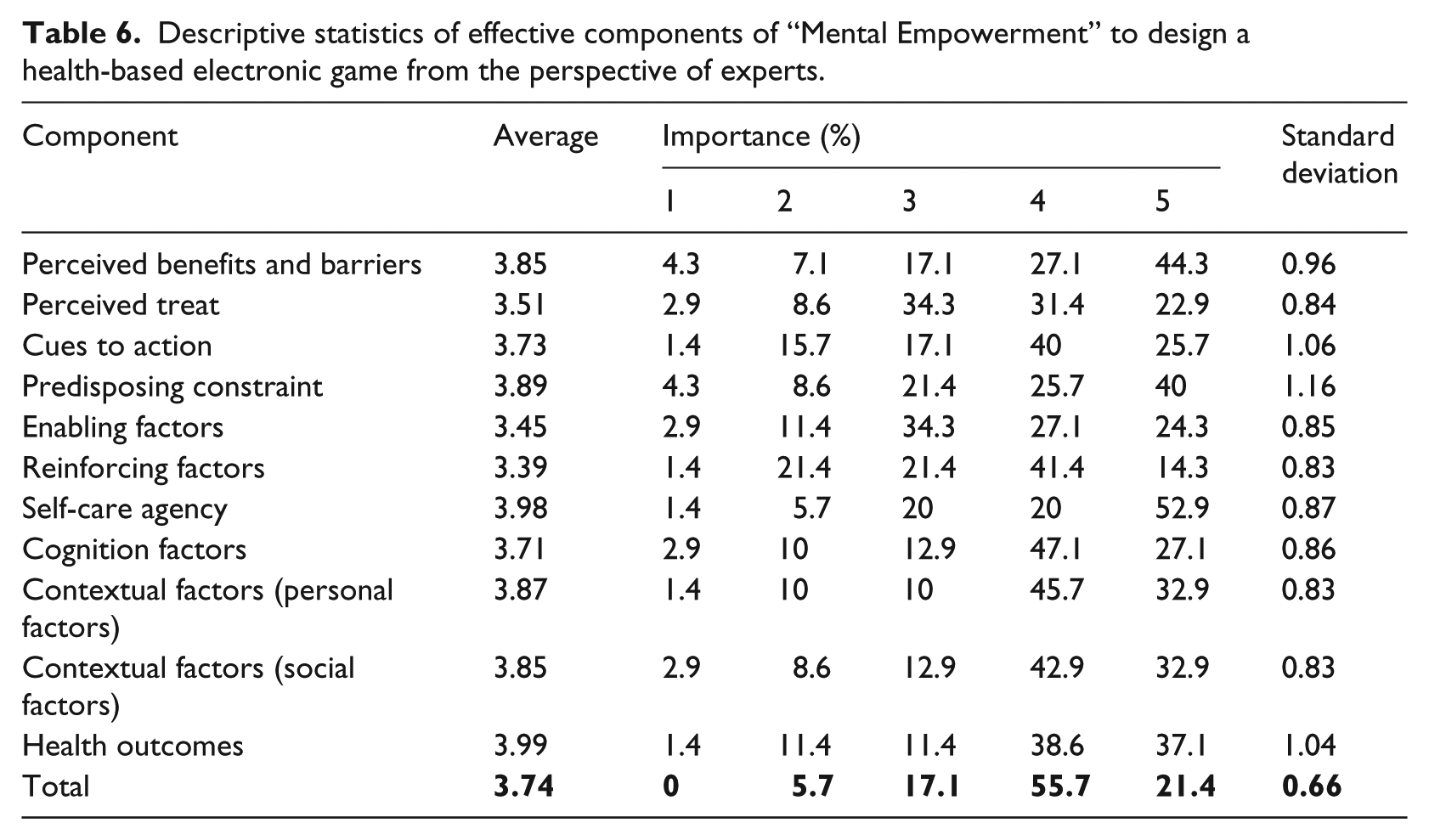
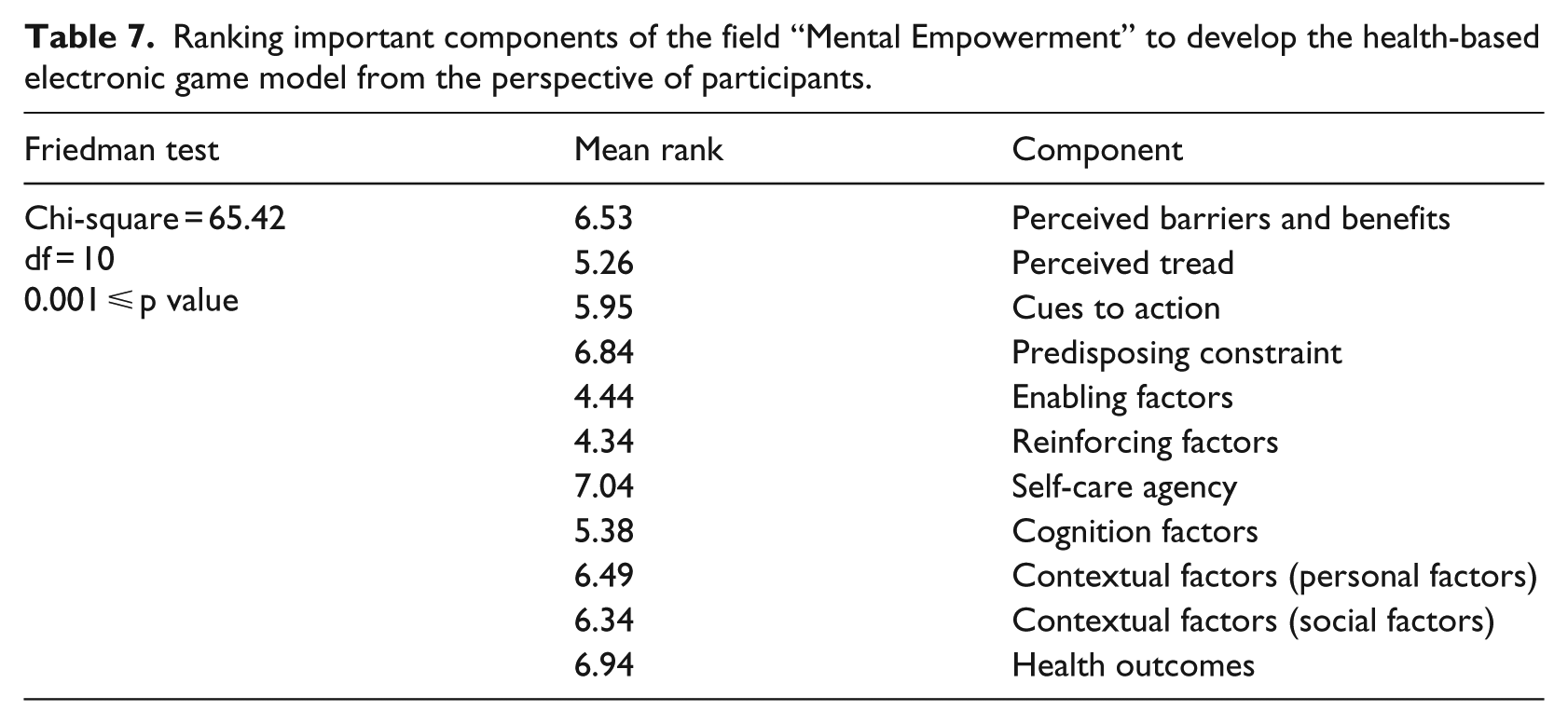
According to data obtained from the information content section of the game design of the research questionnaire, percentage distribution, average of subjects’ comments and standard deviation for responses are presented in the tables for each axis. For example, in the mental empowerment axis, due to the output of this test (p value ⩽0.001), which was lower than 0.05 level, there was a difference between the average rating of these 11 components (Table 1) at the confidence interval of 95 percent. Considering the average rating of the 11 components, “self-care agency” and “reinforcing factors” were the most and least important components, respectively (Tables 5 and 6).
Descriptive statistics of effective components of “Mental Empowerment” to design a health-based electronic game from the perspective of experts.
In the self-learning axis, the self-care agency component and reinforcing factors were the most and least important components, respectively. In the treatment and physical activity axis, according to the test output (p = −0.197), which had a higher level of significance at 0.05, here there was no significant difference between the average rating of these 10 components of the treatment domain (individual or with the help of team care).
With regard to the condition management axis, considering the resulting average for these 10 components, “self-care agency” component and “enabling factors” were the most and the least important components, respectively. With regard to healthy eating, considering the resulting average rating for these eight components, “self-care agency” component and “perceived threat” were the most and least important, respectively. According to analysis of data obtained from the research questionnaires, percentage distribution and the average of subjects’ comments in the six areas involved in the health-based electronic game design model as well as the standard deviation of their responses are presented in Table 7.
Ranking important components of the field “Mental Empowerment” to develop the health-based electronic game model from the perspective of participants.
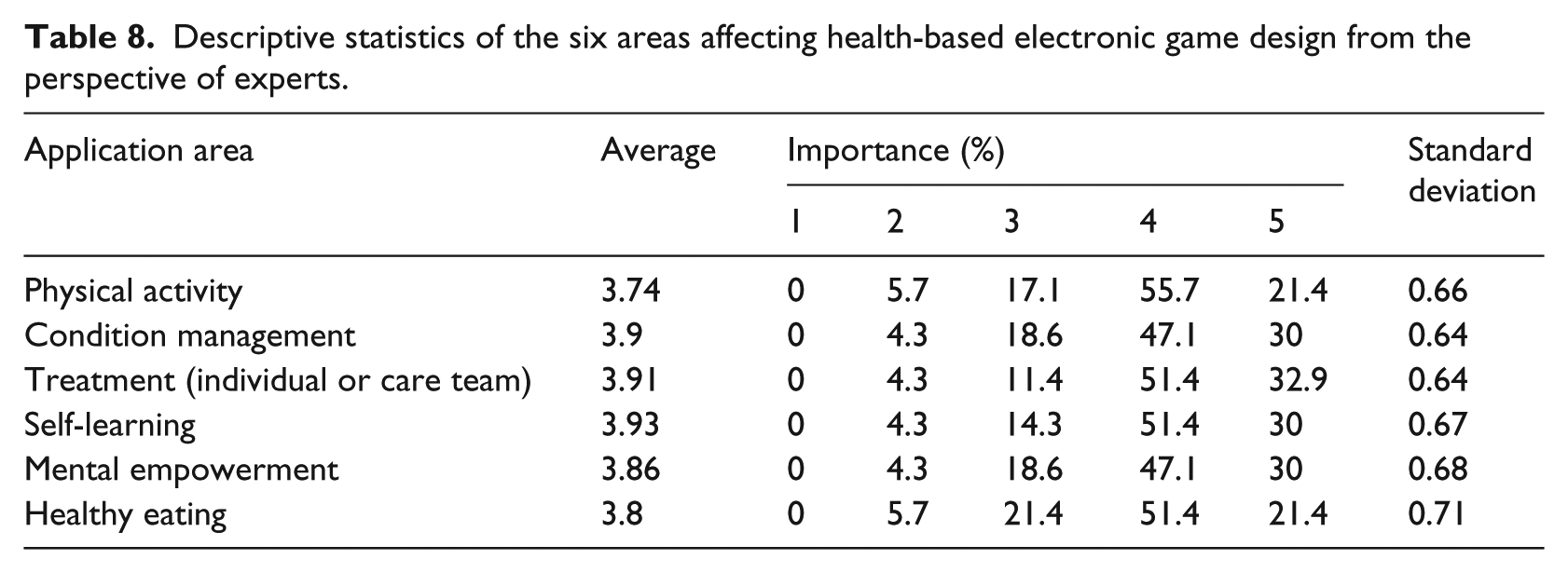
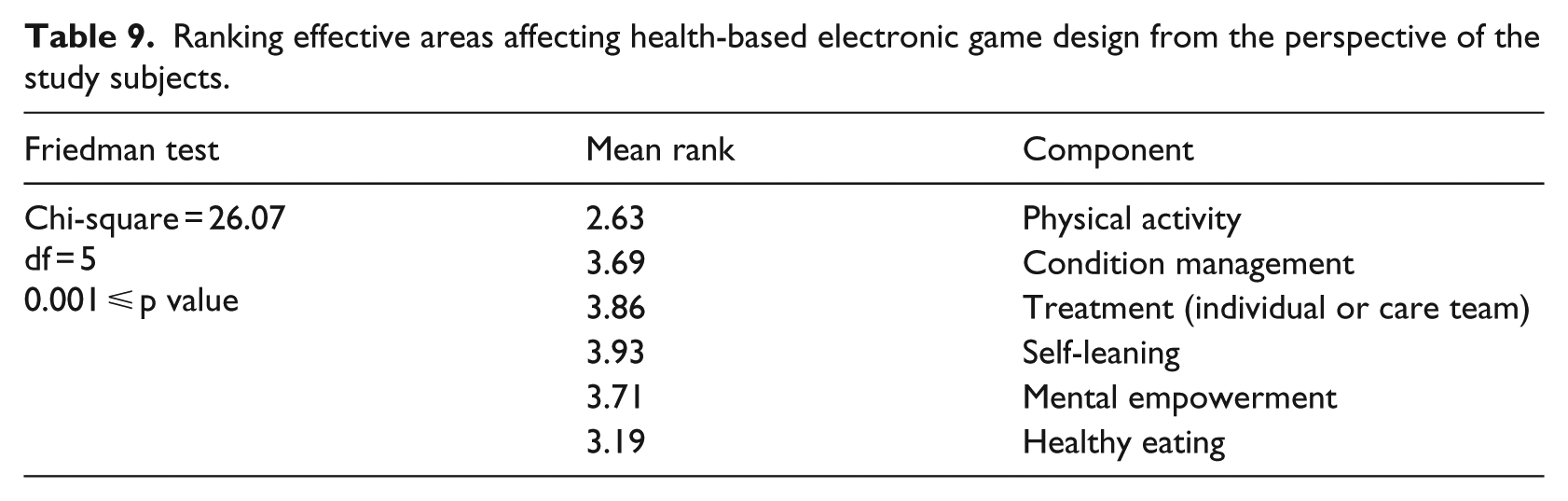
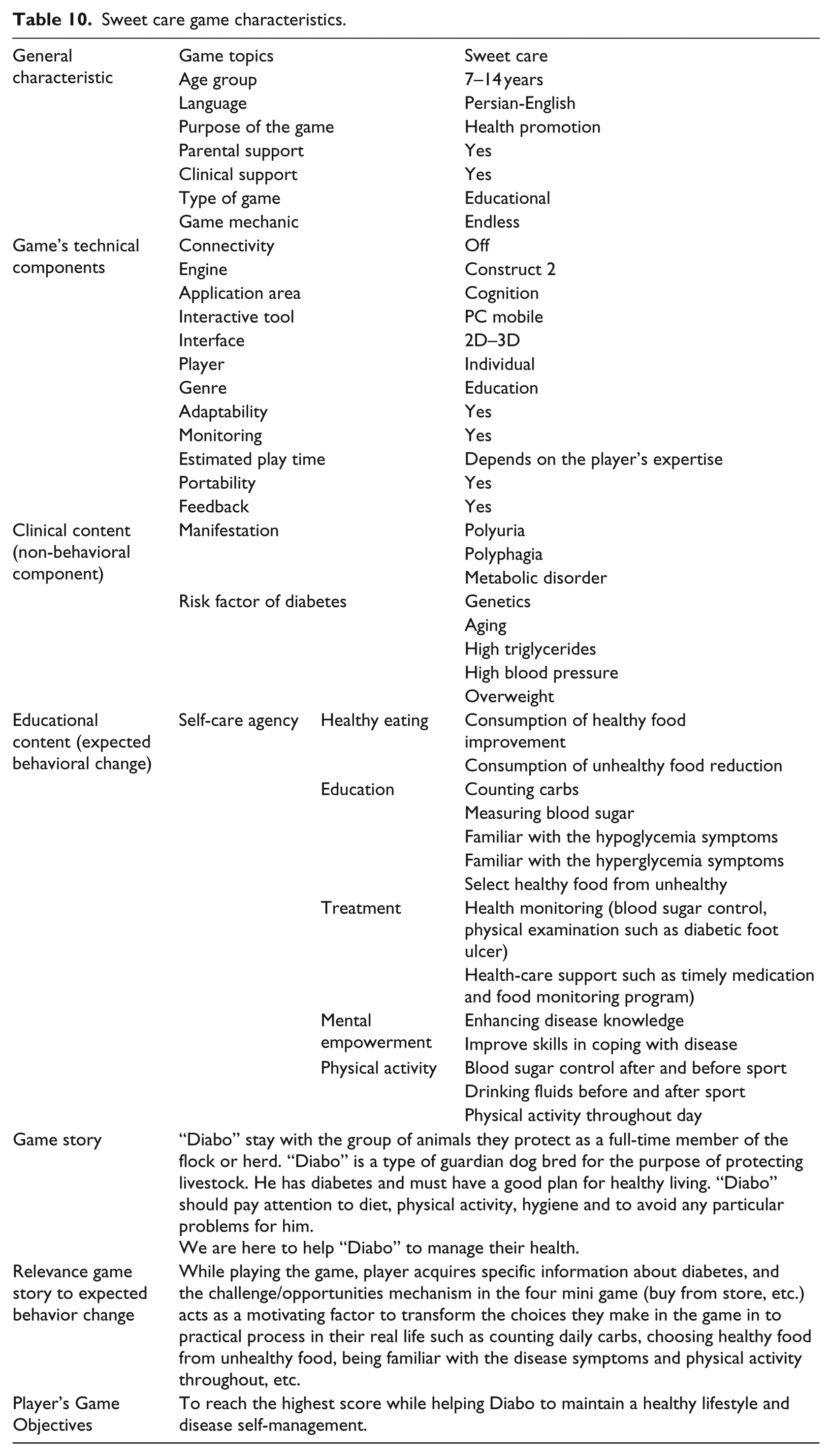
According to the analysis of data obtained from the research questionnaires, percentage of distribution and average of subjects’ comments on the six areas involved in the health-based electronic game design model as well as the standard deviation of responses are presented in Tables 8 and 9. Table 10 provides the game’s ID and details of the designed sweet care game constituted.
Descriptive statistics of the six areas affecting health-based electronic game design from the perspective of experts.
Ranking effective areas affecting health-based electronic game design from the perspective of the study subjects.
Sweet care game characteristics.
Discussion
It is evident that human behavior is influenced by a number of factors. Behavior can be modified or changed through education provided by innovative technologies such as electronic games. This approach requires an understanding of behavior and factors that can affect change or modification of existing behavior and lead to new behavior. Therefore, behavioral models and theories have a role in education.
The goal of this study was to change behavior in order to empower people, to implement learned behavior, to inform and to take selective and targeted action in order to secure, to maintain and to promote the health status of individuals and their families. As a media tool, digital games can be effective in health education, but this requires a structure framework to deliver information. The goal was to change behavior in order to empower people, to inform, to implement acquired knowledge and to stimulate selective and targeted action and behaviors in order to maintain and promote health in individuals and families. So, theories on behavior change were accepted as a guide for designing messages related to good health (content) embedded in the game.
Here, there were three reasons that led to the use of several models of games to supply information. This required components on which to present the health education content. This study was consistent with Peng’s study on whether the medium of a computer game could educate people and promote health in individuals. He believed that successful computer games required effective content in terms of health information. The operational strategy presented by “Peng” was based on theories of behavior change in the structure and game content. 31 Marchetti’s theoretical framework was also based on the model of behavior change. He introduced transtheoretical model (TTM), social cognitive theory (SCT) models and self-care theory as content components and considered five transtheoretical theories in the game design. He also used “self-efficacy,” “self-monitoring skill development” and “intrinsic motivation” to exchange messages within the context of the game. 32
The second reason for using several models relates to the fact that it did not seem right to assign the duty of selecting behavior change in models for different health behaviors to service providers at the early stages of the program due to diversity of the models. Third, the types of goal behaviors directed at patients in the health education system were almost the same and perhaps all of them could be placed as goal behavior related to self-management of the disease; thus, it seemed rational to use health behavior change components in practical aspects of the game in the field of health. All factors mentioned in each behavior change model were divided into smaller components in the presented study so that all factors with a significant effect on changing behavior were entered into the design checklist; so, it was possible to plan for every single component and to select for inclusion in the health-based game design process. However, there are always challenges for setting game components. These challenges can be solved by the design team’s judgment and by the purpose of playing the game as well as elements of its content. Harman and Ten state that it is very difficult to design a game that satisfies all the needs of all its users, and the paper argues that the only solution, prior to design, was to create a practical framework of the game’s content, which ultimately meets some needs of some individuals. 33
During the design of the product, and to facilitate achievement of learning outcomes, identification of the concept structure has a fundamental role. Information components of most of the studied models were divided into three parts: input, process and output. Most of the information content was derived from the theory of behavior change. 34 What distinguishes the model presented in this study with those in other studies is that both the technical structure and the information content of the game design were determined in the present model. In determining the information content of a health-based game, it is better to consider both information and technical components and to plan for them in the form of a framework to avoid any being missed. Among the presented models, the logic model can provide the basis for developing a more detailed management in the design field that helps track to and control activities in order to apply a rigorous program. The proposed model provided the basis for a blueprint of the budget and an outline of the work. Also, it can be a valuable tool for planning and developing games. This structure helps focus on a strategic plan and thereby to clarify what consumers wants to achieve. The proposed design model, if it is accurate and appropriate, can be a powerful communication tool for various beneficiaries in the field of health.
This model can inspire other applications to develop games in different areas of health. A model developed according to these interpretations and by these components can be used at any time for any purpose or for any disorder or health problem or in cases that require a small picture of the health program. Also, in relation to management of sweet consumption, this model was made operational with the goal of empowering and improving self-care behavior among diabetics. In a study on designing games for diabetes, “CopperQ,” states that blood glucose monitoring, insulin administration, diet planning and physical activity constituted only some of the daily tasks in routine for someone with diabetes. However, he believed that many environmental and personal factors affected whether or not a person performs these tasks. For this reason, he believed that individuals with insulin-dependent diabetes needed to receive proper training, appropriate to the maturity of the individual and his or her personal preferences for different levels of learning through the context of a game. 35 Definition of character and setting in the context of the game was devised to deepen, enrich and create a memorable experience. Diabo, a dog with diabetes, was our main character in this game. Also, we tried to take advantage of appropriate graphics, professional animations and sound for the character in the original environment.
In the self-care axis, Diabo’s health status was protected by monitoring healthy eating (introduction of healthy and unhealthy food groups, counting daily carbohydrate intake), physical activity and pharmacotherapy (the amount of insulin needed) and health monitoring (control of blood sugar level; Figure 2).
Attempts were made to encourage Diabo to participate in physical activity (Figure 2). With this goal in mind, mini games, for sale in the store, were embedded in the game as menus and extra points could be earned by playing these games (Figure 2).
Prensky believed that each game should receive the same reward. He asserted that players are motivated by rewards. Also, punishment was indirectly considered in the game. If a player earned a low rating, rather than dying or losing points, then he or she would have to restart the game in this study. Also, Prensky believed that players should benefit from a negative feedback strategy so that once a player lost at a particular stage of the game, then the game should become easier. Conversely, the game should be designed such that if a player plays well, then obstacles should appear to make the game more difficult. 36
Song maintained that patients learn from experimental behavior. For example, if a player is presented with dangers in a game, the game should require the player to make the right decision for promoting good health. 37 In a mini game, players were made sensitive toward the goal of the game and then achieving the goal was made harder. Studies have shown that the game should be fun for a wide range of players. For this reason, we tried to use challenges in the mini games such that the level became more difficult as the game progressed. In support of this, Tai stated that the best games are those that are learned by players at the beginning. In other words, the game is easy to learn but players need more time to overcome its challenges. However, this must occur within the allocated time period. 38 In sweet care, Diabo was fed with three meals between 9:00 a.m. and 7:00 p.m. (Figure 2). Classification of meals per day was clearly reminiscent of a user’s meals in the real world. Days were endless in the game, and players could enter the second day only after completion of the first day of the game. Chamberlain believed that a good game is one that gives players training tips during the game. In this way, the game links narrative aspects of the story—the education necessary for a child or adolescent with diabetes in the real world. Chamberlain suggested that the educational information should be repeated in different categories in various locations in a game. 39 In sweet care, self-care training tips, as well as stages of the game, were taken into consideration. In the shopping mini game, dual healthy and unhealthy queuing formed the user’s mind set while confronting visual signs, objects and different situations in the game. Also, it created a sort of mental preparedness and desire in the user to create similar dual categories in terms of healthy and unhealthy foods in the real world. Creating this type of duality in the user’s mind can help persuade a user to visit a doctor or to get advice from parents on an issue. In the game setting, users enter the game world, and in order to succeed in their mission, they should skillfully follow their diet program step by step. This line of narrative, in which success depends on strict adherence to the diet, clearly links the game’s context with the reality of health education in the real world for a child or adolescent with diabetes, “Your health is contingent upon compliance with an appropriate diet.” Finally, in favor of the transfer of the goals of health education, the design of the game’s procedures was so simple so that a user was able to review the least essential information about diabetes as a childish hobby without spending too much time and energy. The game procedures had simple appeal.
In fact, they strengthened positive and negative logic systems, through which they generate the necessary charm to continue the game and transfer text related to health and education in the same logical two-value system to the game user. Information technologies, aside from information transfer, can have a constructive influence on mental health, cognitive function and social activity. Children and adolescents with diabetes also fill their time with these games; they learn from them and are affected by them. These effects can be positive or negative depending on the game’s design and its purpose, game type and the amount of time devoted to playing it. Positive effects that can be expected from these games include behavioral evolution and creativity and developing attention span increased IQ, learning complex concepts, improving and developing cognitive skills, intuitive intelligence and other skills. 40 However, if such games are not selected appropriate to age, culture and content, then there are possible risks such as social isolation, decreased academic performance, increased levels of risky behavior and aggression and exacerbation of problems related to attention, concentration and other such conditions.
Future research directions
This study is important to expanding the knowledge base on how to create effective health-based digital games that entertain while promoting behavior change. In addition to electronic games for health offer a promoting platform for reducing risk of developing disease and enhancing self-management by promoting healthy diet, physical activity behaviors, mental empowerment, education and condition management. However, this field is in its infancy. To reach its full potential, sweet care game is needed to effective evaluation, but unfortunately due to lack of time and lasting game design process, this work was not done. In future research, this work is carried out.
Conclusion
Health-based electronic games, as a type of serious game, are extensive efforts that use the expressive capacity of a game, as media that take advantage of the appeal of computer games to communicate essential health-care education. Utilizing an electronic game on health is a novel tool that can empower people. It is introduced as a way to develop a better quality of life and to promote public welfare. Empowerment is an approach that supports patients with chronic diseases such as diabetes. Diseases and the effects of diseases can be controlled by developing the approach of electronic health-based games for empowerment. Application of this technology can help people control their diabetes and by presenting individuals with a learning tool to change their behavior. Digital games offer promise as an engaging and entertaining approach for enhancing self-management among youth with diabetes, especially when guided by a framework informed by behavioral theory. Considering the increasing use of electronic games in different classes of society, more emphasis must be placed on the need to develop strategies and policies that optimize the potential of this technology as a new media for education as well as to develop games with an educational approach that foster creativity and problem-solving skills in the user. Furthermore, as educational tools that promote good health, these games can be presented in an attractive way. Future research is needed to test the efficacy of sweet care game as a new approach for self-care improvement in management of diabetes, as well as its effectiveness under real-world conditions.
Footnotes
Acknowledgements
The personnel of the Red Cap Company are also thanked for their cooperation in development of this important project. At the end, the author’s acknowledge Mr Syed Ahmad Moosavi and Mr Mustafa Movahedian for the essential scientific and technical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was supported by grant from Studies and Research Management Center, Tehran Universities of Medical Science.