
Abstract
Checklists are commonly used to structure the communication process between anesthesia nursing healthcare providers during the transfer of care, or handoff, of a patient after surgery. However, intraoperative information is often recalled from memory leading to omission of critical data or incomplete information exchange during the patient handoff. We describe the implementation of an electronic anesthesia information transfer tool (T2) for use in the handover of intubated patients to the intensive care unit. A pilot observational study auditing handovers against a pre-existing checklist was performed to evaluate information reporting and attendee participation. There was a modest improvement in information reporting on part of the anesthesia provider, as well as team discussions regarding the current hemodynamic status of the patient. While T2 was well-received, further evaluation of the tool in different handover settings can clarify its potential for decreasing adverse communication-related events.
Introduction
The patient handoff or transfer-of-care is a contemporaneous, interactive process of passing patient-specific information from one caregiver to another to ensure continuity and safety of patient care. It is well recognized that the transfer-of-care is a point of vulnerability where valuable patient information can be distorted and omitted.1,2 The Joint Commission has reported that communication breakdowns were the leading cause of reported sentinel events between 1995 and 2006. Similar studies have estimated that errors in communication at handoff or transfer of care may be implicated in as many as 80 percent of serious medical errors.3–5 To this end, multiple regulatory agencies have called for quality improvement measures to standardize handover processes and quickly identify handoff-related errors.
The post-operative transfer-of-care involves members of the anesthesia and surgery care teams providing a verbal report of the intraoperative patient course to the recovery room or intensive care unit (ICU) healthcare teams. However, the transfer-of-care occurs while there are competing clinical demands on attention, including the exchange of monitors, infusions, and their intravenous line attachments. A plethora of studies in the literature have identified a variety of problems associated with transfer-of-care, such as incomplete or inaccurate information exchange,2,6,7 unstandardized (or absent) tools to guide the order of the handover,8,9 interruptions, and lack of anticipatory guidance for subsequent care. 10
Use of standardized checklists to help structure the verbal communication process between the transferring operating room (OR) team and the receiving ICU team has been studied before.8–12 However, a checklist simply provides a structure for communication and in itself does not guarantee accurate and complete exchange of information during handoff. During handoff, providers are often forced to recall from memory information related to critical elements of clinical care. This process can be problematic due to incorrect or incomplete recollection of information. The problem is particularly serious during post-operative handoff because a surgical episode generates a large volume of critical data and multiple providers often care for patient during surgery. Hence, there is a critical need to have an information transfer tool in the context of a pre-existing handover checklist to facilitate handoff. Such a tool could summarize and present critical information such that clinical events and data need not be recalled from memory. The use of such a tool to supplement a handoff checklist has not been explored before. In this article, we describe the development and use of a novel electronic anesthetic information transfer tool (T2) for use in the transfer of intubated patients to the ICU. We also performed a pilot comparison of reported transfer-of-care information items with and without using T2 tool, utilizing a pre-existing OR-to-ICU checklist as a guide for comparison. Additionally, we also performed a usability survey to gauge user acceptance of the tool.
Methods
Study setting
This study was performed in an academic medical center from 27 October–12 December 2014. It was deemed exempt by our Institutional Review Board as a quality improvement project.
Electronic transfer tool (T2)
Our institution uses an anesthesia information management system (AIMS) (Merge AIMS; Hartland, WI, USA) to document anesthesia care in the ORs. To enhance the functionality of this system, we developed a decision-support software—Smart Anesthesia Manager (SAM). SAM acquires near real-time data from AIMS to provide real-time feedback and guidance to anesthesia providers on clinical care, billing, and compliance aspects. 13 For this study, we enhanced SAM by adding an informatics tool (transfer tool; T2) to facilitate handoff. The first component of T2 is an automatically generated transfer report that summarizes the anesthesia and surgery episodes into a concise and printable sheet. The second component is a communication module that notifies the recovery team of patient transport from the OR to recovery.
Content categories for the transfer tool (Figure 1) were derived from a review of previously studied tools in the literature2,6,7,10 and is comprised of the following main sections:
Patient/provider information. This section contains patient identifiers and demographics, American Society of Anesthesiologists (ASA) physical status, primary procedure and diagnosis, procedure duration, and anesthesia and surgery staff, and their contact information;
Anesthetic Information. Pertinent medical history and concerns noted by the anesthesia providers, intravenous and invasive line sites, airway management, regional blocks, and case-specific events such as cardiopulmonary bypass and emergence from anesthesia;
Medications. Total dose and time of last dose of bolus medications. Infusion medications and the latest infusion rate;
Labs. Categorized lab results during the intraoperative phase;
Vitals. The last set of hemodynamic parameters captured from the patient monitor.
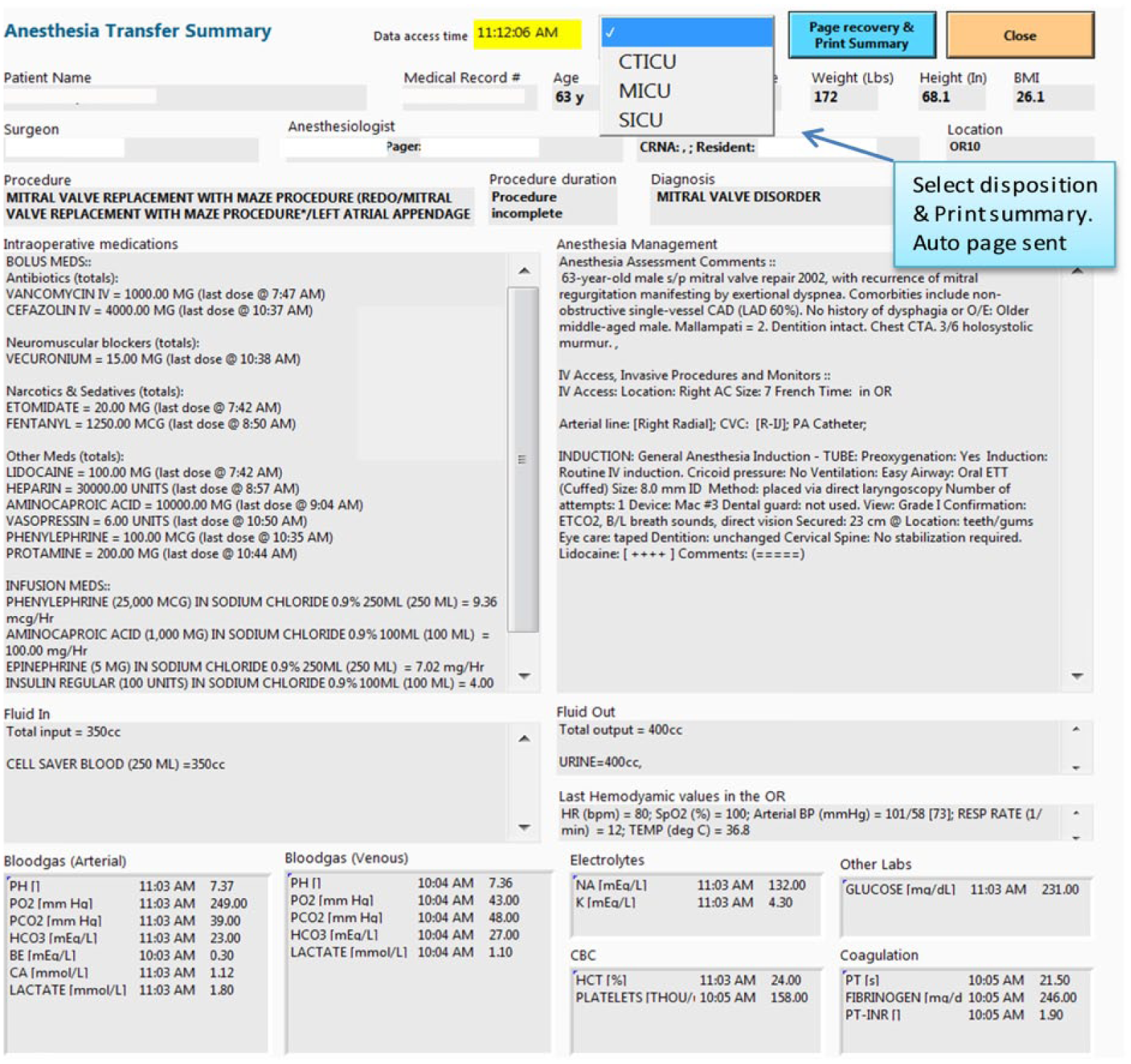
Electronic transfer tool (T2).
The transfer tool, T2, which embeds the transfer summary report can be evoked on an AIMS computer using a pre-assigned hot key on the keyboard. The report can be printed in designated recovery area printers using the “Print” button. The communication component is also embedded into T2, whereby a text message is sent to a designated recovery pager when the transfer summary report is printed.
Workflow integration
For this study, we piloted T2 to facilitate transfer of care of intubated surgery patients in an ICU for the cardiothoracic service (cardiothoracic intensive care unit (CTICU)) and other surgical services (surgical intensive care unit (SICU)). A flowchart describing the integration of T2 into the anesthesia and nursing workflow is shown in Figure 2. When the anesthesia provider is preparing to exit the OR with the patient, he/she evokes T2 on the OR AIMS computer with a simple keystroke. The anesthesia provider selects a disposition location from a drop-down menu and presses the “Print and Page Recovery” button. This initiates a text page to the ICU team resident, informing him/her about the imminent arrival of the patient. Concurrently, three copies of the transfer report are printed in two ICU printers. The ICU resident, bedside nurse, and anesthesia provider use the three copies during the handoff process. The ICU resident and an assigned nursing staff member bring copies of the transfer report to the patient’s bedside prior to patient arrival. Upon reaching the recovery bed, the OR team deposits patient in the ICU bed and initiates post-operative verbal handover process. During the handoff process, the anesthesia, ICU, and nursing providers use the transfer report as reference to communicate the relevant anesthesia and surgery information to the recovery team. Our ICUs use a visual checklist for the handoff process (Appendix Figure 4). The use of this checklist was continued during the pilot evaluation of T2.
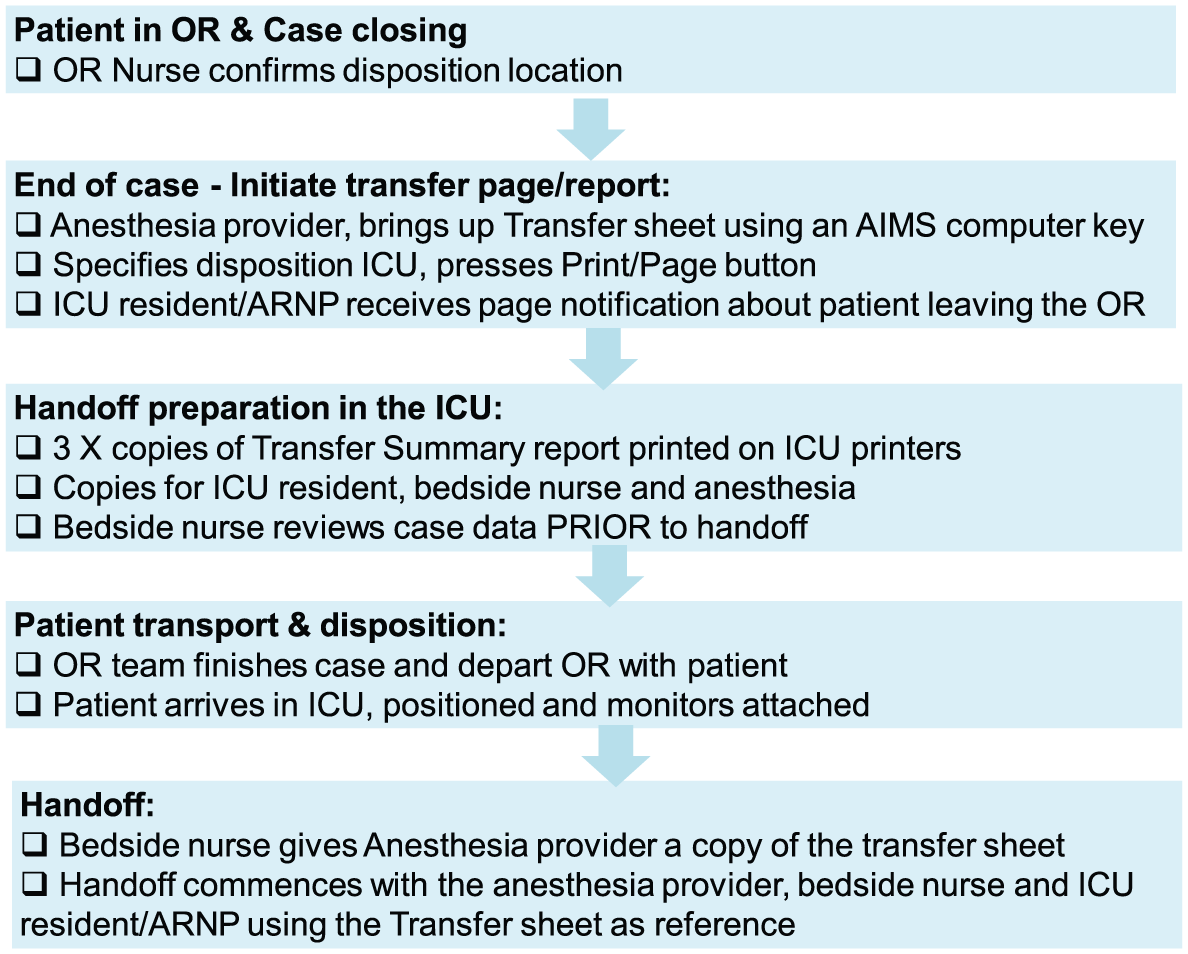
Transfer template (T2) workflow integration.
Education and activation of T2
A series of steps were undertaken over a 4-week period to educate all perioperative practitioners about the OR-to-ICU handoff protocol. Multiple methods and venues were used, including presentations at staff meetings and grand rounds, nursing in-services at shift changes, cognitive aids (workflow posters posted near anesthesia workstations), and informative emails. The educational steps emphasized the key points of the transfer report, initiation of the communication page, and collection of the printed transfer report. In addition, it was also emphasized that the providers continue to use the existing handoff checklist, with the new transfer report being used as a reference document. Subsequently, the T2 feature in SAM was activated for ICU patient transfers.
Data collection—audits
Two independent observers (medical students) were recruited and trained to observe the handoff in the ICU. Potential cases to be audited were identified from the OR schedule on the days when the observers were available. A structured observer audit form (Appendix Figure 5) was created to evaluate handover metrics. The metrics were derived from the data categories listed in existing handoff checklist. The observers completed the audit form for handoffs during both the pre-intervention period when T2 was not used and the post-intervention period when T2 was used.
Data collection—survey
A single two-item survey regarding frequency of use and helpfulness of T2 was separately distributed to all anesthesia providers, surgery residents, and attending physicians, as well as all ICU personnel engaging in the ICU transfer-of-care for patients during the time period of 1 July 2015 through 1 August 2015. E-mail distribution was utilized for all anesthesia and surgery personnel through program coordinators, while CTICU and SICU nurse administrators conducted paper distribution of the same survey. Survey results were tallied in August 2015. The 2-question survey was posed to obtain a subjective measure of comfort and satisfaction of using T2 by the end-user.
Statistical analysis
Handoff metrics were compared during the pre- and post-intervention periods. To test for statistical significance, we used a 2-sample t-test and Mann–Whitney U test, as applicable, for continuous variables and Fisher’s exact test for categorical variables. A p-value of <0.05 was considered statistically significant. Data were analyzed with SPSS software (Version 19.0, IBM Corp., Armonk, NY, USA).
Results
A total of 26 handoffs, 12 during pre-intervention (no T2 used) and 14 during post-intervention (T2 used) were observed. Patient demographics, location of ICU disposition, presence of service attendees during handoff, and handoff durations are presented in Table 1. Although most parameters were similar, there were a greater proportion of CTICU patients represented in the study during the post-implementation phase.
Patient demographics, disposition, service attendees, and handoff durations.
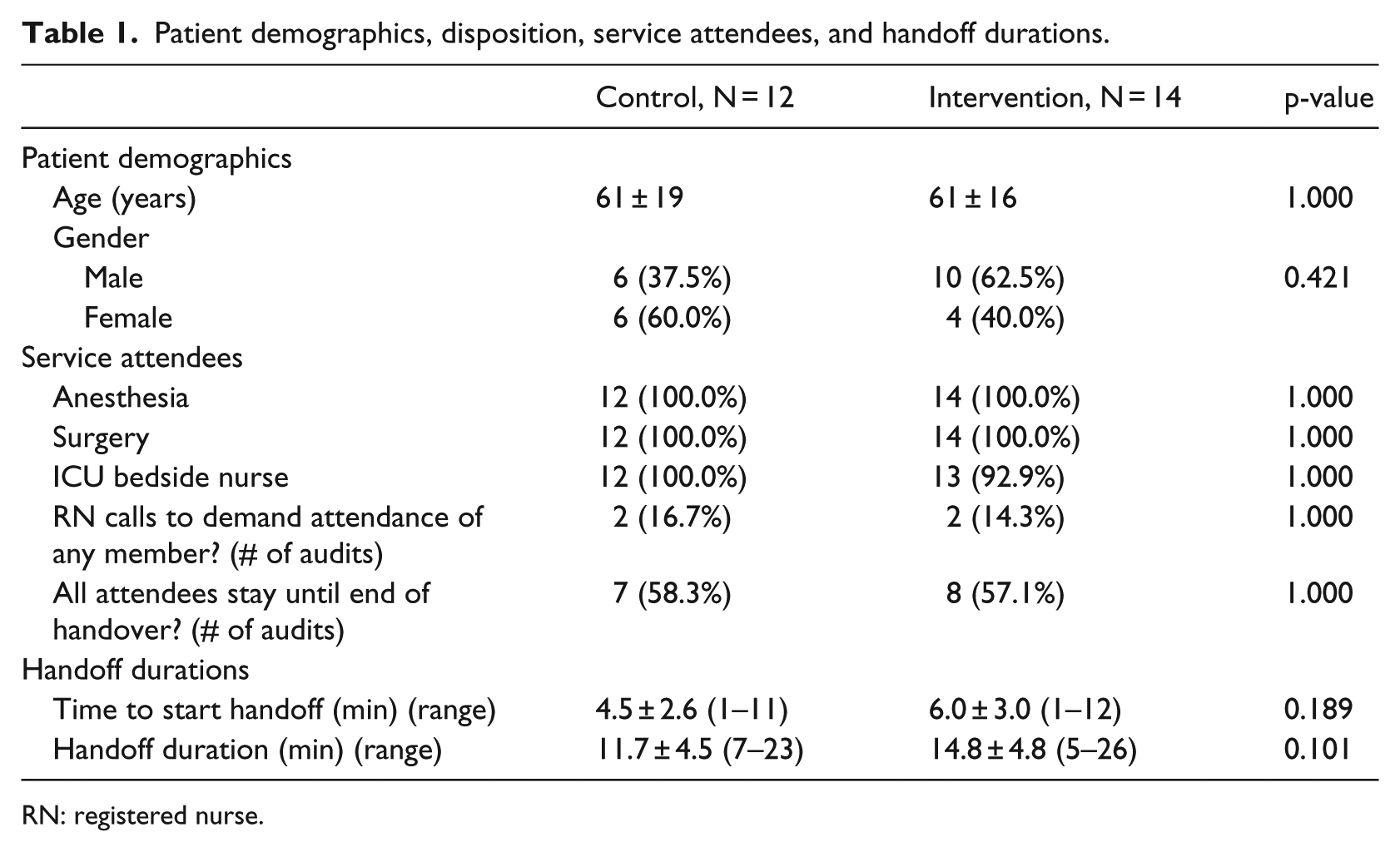
RN: registered nurse.
Comparison of critical elements communicated during handoff is shown in Table 2. There was a moderate improvement in the discussion of the intraoperative anesthetic plan, medications, blood products (or lack thereof), and intraoperative laboratory results with the post-implementation group. A similar increase in reporting airway concerns, antibiotic administration, and fluid losses (i.e. urine output and blood loss) was observed when using the T2 tool. Also, there was a greater proportion of handovers including a discussion about the current patient status, including hemodynamics and current infusions, in the post-implementation audit cohort. With the exception of the wound management plan (for which the discussion is typically led by the surgery team), the reporting rates for all items pertaining to current patient status were greater than 50 percent when using the T2 tool.
Comparison of critical elements communicated during handoff in control and intervention cases.
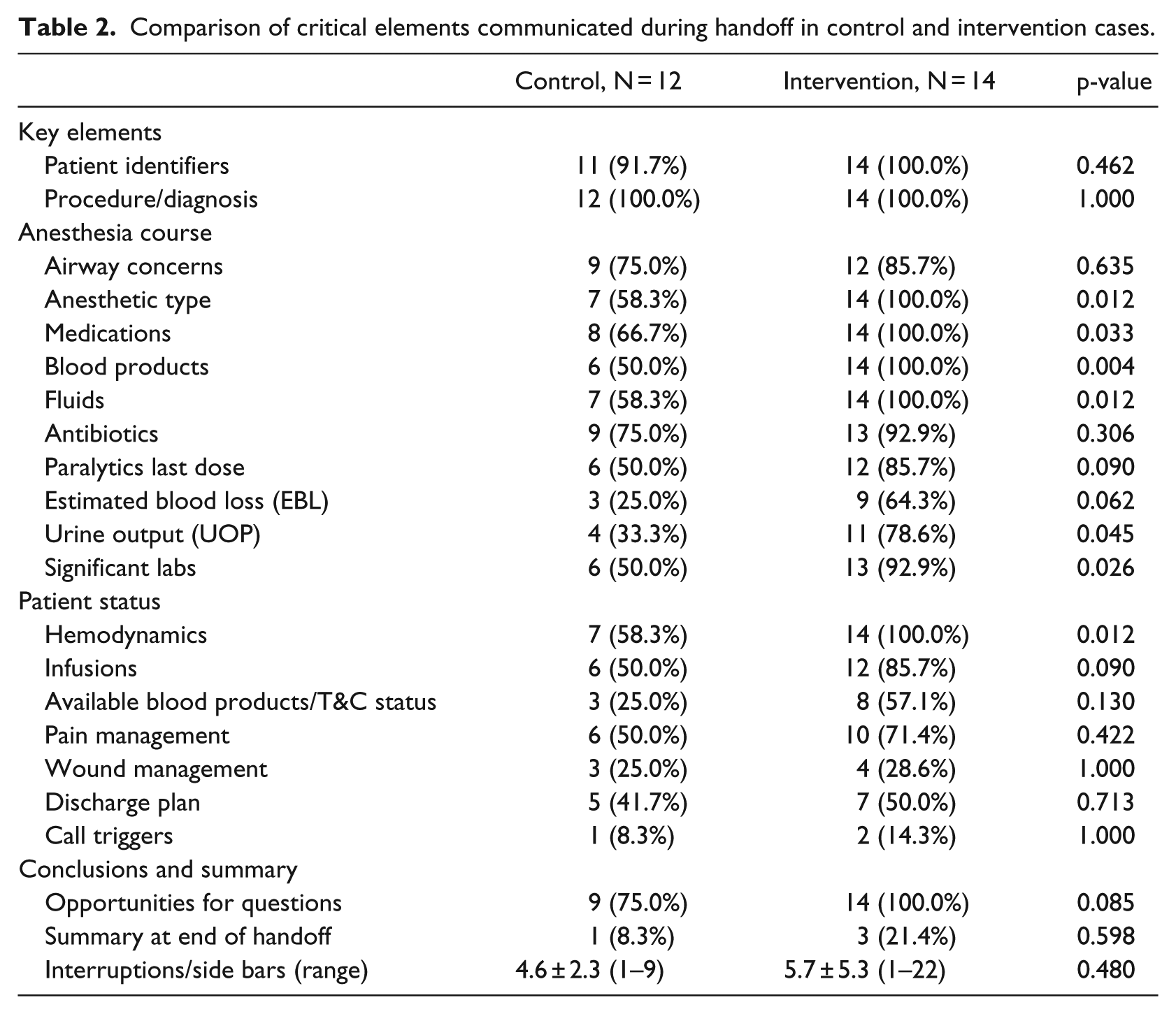
Table 2 also presents the conclusion summary and interruptions during handoff. During the post-implementation phase, all 14 audited handoffs (100%) contained a verbal acknowledgment of opportunities for questions, which represents a slight increase from the pre-implementation period when only 9 handoffs had this opportunity. There was no significant difference in the proportion of handoffs that included a clear intraoperative summary (by either the surgeon or anesthesiologist). The number of interruptions (as observed by the auditors) was also similar between the two study periods.
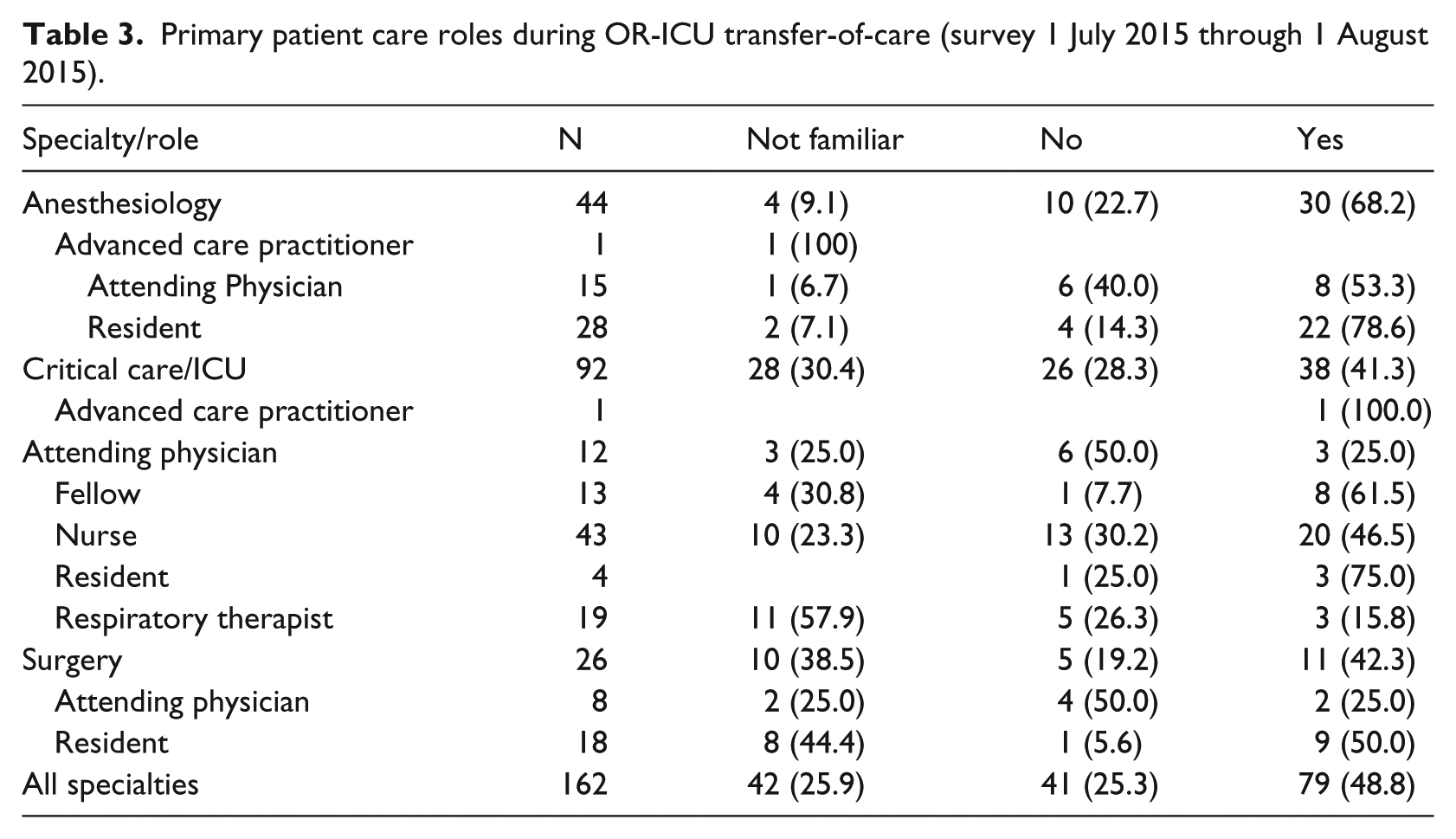
Table 3 presents the patient care roles for respondents to the three-item survey. Data are grouped by service category (anesthesia, surgery, and ICU) as well as specific job titles. At 6 months post-implementation, the T2 was utilized at least once by 79 of 162 respondents (49%). A significantly greater proportion of anesthesiologists reported use of the T2 compared to the remainder of the cohort (68% vs 41.5%; p = < 0.05). The “Resident” role, with respect to both the anesthesia and ICU care teams, reported the highest frequency use of the T2 template (Figure 3(a)). The “ICU Nurse” role was associated with the largest number of survey responses (N = 43). However, only 20 respondents (47%) reported using the T2, while 10 respondents (23%) were not familiar with the tool at all.
Primary patient care roles during OR-ICU transfer-of-care (survey 1 July 2015 through 1 August 2015).
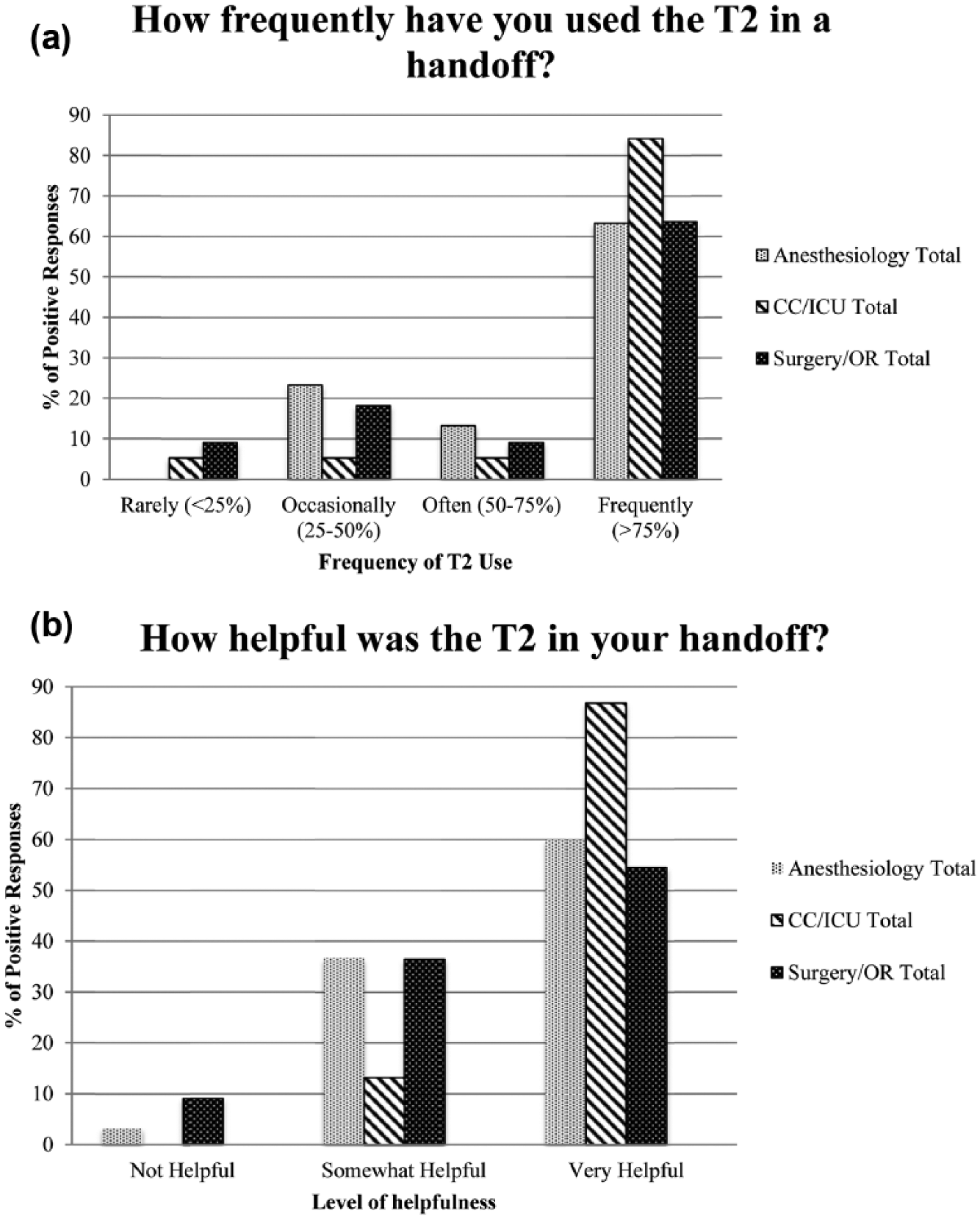
(a) and (b) Survey responses (1 July 2015 through 1 August 2015) (N = 162).
The vast majority of users who reported using the T2 at least once also rated the tool as being at least “somewhat helpful” (77 of 79 users; 97.5%) (Figure 3(b)). All but one respondent with the “ICU Nurse” job title found the T2 to be “very helpful” (19 of 20 users; 95.0%).
Discussion
The transfer of patient care between the OR and recovery teams at the end of surgery is an important juncture where critical and relevant information should be communicated for continued safe care of the patient. With the traditional paper anesthesia record, the anesthesia team had a reference document in hand when transferring patient to the nursing team in recovery. Furthermore, the finalized paper record is kept in the patient’s chart at the end of the case, which meant that the recovery nurses and other clinicians had a reference clinical record on intraoperative course for subsequent care. However, paper anesthesia records can be incomplete and illegible and have been largely replaced by electronic AIMS. Moreover, AIMS data often remain digitized in electronic databases not readily available to the OR and nursing teams at the time of handoff. This is particularly true when the anesthesia and nursing electronic medical records (EMRs) are not integrated. In our institution, we utilize an AIMS that is not integrated with the hospital-wide EMR used for nursing documentation in the recovery areas. Furthermore, the AIMS itself does not have a tool to facilitate handoff. For these reasons, as a quality improvement initiative, we developed a handoff tool to assist with patient handoff.
Our pilot investigation reveals that the overall quality of handoff, in terms of information exchange, was improved when using the T2 tool in conjunction with the pre-existing checklist. The quantitative improvements were mostly observed in reporting of elements related to anesthesia course and patient status. Specifically, the data elements that were presented in the transfer summary report were communicated more often when using T2. In addition, there was a trend toward improved communication of other elements related to handoff as well, although the difference did not reach statistical significance. The use of a handoff checklist throughout the evaluation period may have resulted in an overall improvement in the quality of handoff.10,11,14 Although the checklist was used for both control (no use of T2) and intervention (use of T2), it is unclear whether the differential improvements seen during the intervention period can be solely attributed to T2. Likely, the combination of using T2 with the handoff checklist contributed to improved handoff.
Observation of handoff using the T2 tool highlighted several qualitative improvements. The numerical data (e.g. medication and fluid totals) clearly presented in the T2 printout allowed more time and focus to be spent on other aspects of the handoff. The T2 tool changed the dynamics of the handover process by shifting time and attention from the receiving members documenting numerical details to the presenting team discussing the continuity of care for the patient (including anticipated complications and discharge, additional imaging/testing needed, etc.). This made the best use of time for the surgical/anesthesia staff as they could refer most questions regarding numerical details to the T2 printout. In addition, during the handoff process, both the anesthesia and nursing staff had copies of the T2 printout. Although the anesthesia provider initiated the transfer of information going through the handoff checklist while referencing the T2 printout, the receiving nursing staff also used the T2 printout as reference, verifying the received information. This process of concurrent communication and verification contributed to a better information exchange. Finally, having multiple participants with different roles using copies of the T2 printout allowed shared review and discussion of critical information. This encouraged a team approach and engagement of all parties during the handoff process diminishing communication barriers placed by role and seniority of different care personnel.
Improved information retention could be an indirect etiology of improved patient care. As the healthcare provider tasked with delivering or receiving a handover becomes more comfortable with the sequence of reporting (i.e. the purpose of the checklist) and their ability to report the correct information with high fidelity (i.e. the purpose of the T2), they will have more time to clarify information regarding the pre- or intraoperative care of the patient being transferred to the ICU. Questions posed will be focused on specialty-specific items not covered in a generic checklist (with concurrent decreased redundancies of information already reported) as well as the ultimate plan for the patient (i.e. a greater emphasis on the plan and relevant alerts for a patient). There is increased engagement of the handover team members that accompanies better information retention and reporting using the T2–checklist combination. Our outgoing hypothesis is that this greater engagement will improve anticipatory guidance by helping to decrease communication-related errors such as drug errors and improving care delivery by improved timeliness of time-sensitive tasks (labs, medications) in the immediate post-operative period.
Adoption and integration of T2 into the nursing workflow over the study period were fairly smooth, and both the ICU and OR teams generally welcomed the use of the tool. However, we initially encountered some practical challenges. At first, we printed only one copy of the summary report, which was reviewed by the ICU resident prior to patient arrival in the ICU and then used by the anesthesia team during handoff. However, feedback from the anesthesia, nursing, and ICU teams highlighted the need for multiple copies of the summary report, so that each group has a reference document during the verbal handoff. While a majority of anesthesia providers reported using the T2, a lower proportion of ICU nurses responded positively. We subsequently programmed T2 to print copies of the summary report in multiple printers, so that each of the anesthesia provider, bedside nurse, and ICU resident has a copy of the summary report. A second challenge was encouraging the anesthesia provider to remember all the steps in initiating the T2 (display on screen, setting physical disposition (CTICU vs SICU), and pressing “PRINT” button). In several cases, failure of one or more of these individual steps led to the failure of the transfer report to print at the destination. As a remedial step, we integrated T2 to be automatically launched when the provider presses the button in AIMS to document transport to recovery, thus unifying the processes associated with setting the physical location, paging the ICU team, and printing the transfer report. Transport to recovery is a routine documentation step that anesthesia provider performs in AIMS just as the patient leaves the OR.
Currently, the summary report of T2 comprises only information from the intraoperative phase. Future enhancements would include reporting preoperative information such as patient medical and medication history, allergies, and preoperative lab results. Another useful enhancement would be to present the summary report in a format similar to the handoff checklist which will allow the handoff teams to navigate the checklist while reviewing the corresponding data. A third enhancement would be to eliminate the printout of the summary report and instead have the data displayed on mobile platforms (mobile computers, electronic tables, and encrypted smartphones) during the handoff process.
Although our outcome measures were focused on handover accuracy and quality metrics, a larger-scale study is necessary to evaluate the effect of T2 on adverse communication-related events and hospital quality-of-care metrics. This objective may be approached by extending the use of the T2 to the recovery room setting, which is frequented by a larger number of post-operative patients. Bittner et al. 15 demonstrated an association between improved handover scores and a decreased length of stay in the recovery room. In spite of possible improvements that can be made to T2, it still provides a helpful reference for anesthetic management information for the delivering and receiving healthcare teams during the transfer-of-care.
Conclusion
In summary, we developed a transfer tool that summarizes and presents pertinent information on anesthetic management to be used concurrently with a checklist during ICU handoff after surgery. This tool obviated the need for information to be recalled from memory, thus minimizing the risk of omission of critical data and incorrect exchange of information during handoff. A workflow that utilizes multiple copies of the transfer summary printout encouraged concurrent communication and verification of information and a team participation of surgical, anesthesia, and nursing personnel during the handoff process.
Footnotes
Appendix 1
Acknowledgements
We thank Kellie Garth-Green, RN, and Kimberly Yeary, RN, for their educational initiatives to familiarize the ICU nursing staff with the Transfer Template (T2) intervention. This report was previously presented, in part, at the Society for Technology in Anesthesia (STA) meeting (26 January 2015). A.C.S. helped to prepare the manuscript and execute statistical tests. D.C.O. helped with data analysis and study execution. A.H.X. helped with study execution. J.D.L. helped with study execution and preparation of the manuscript. B.G.N. helped with study execution and manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.