
Abstract
The US National Survey of Residential Care Facilities was used to conduct cross-sectional analyses of residential care facilities (n = 2302). Most residential care facilities lacked computerized capabilities for one or more of these capabilities in 2010. Lacking computerized systems supporting electronic health information exchange with pharmacies was associated with non-chain affiliation (p < .05). Lacking electronic health information exchange with physicians was associated with being a small-sized facility (vs large) (p < .05). Lacking computerized capabilities for discharge/transfer summaries was associated with for-profit status (p < .05) and small-sized facilities (p < .05). Lacking computerized capabilities for medical provider information was associated with non-chain affiliation (p < .05), small- or medium-sized facilities (p < .05), and for-profit status (p < .05). Lack of electronic health record was associated with non-chain affiliation (p < .05), small- or medium-sized facilities (p < .05), for-profit status (p < .05), and location in urban areas (p < .05). eHealth disparities exist across residential care facilities. As the older adult population continues to grow, resources must be in place to provide an integrated system of care across multiple settings.
Introduction
Long-term care
More than 90 percent of older adults have one or more chronic health conditions. 1 Changing demographics among the older adult population include a dramatic rise in the number of individuals reaching older age groups and living longer, which may exacerbate the already present health care issues facing older adults in the United States.2–4 This rapidly aging group will likely need care from different sources and settings.
Long-term care, including residential care for the aging population, is an area expected to see a rise in utilization 5 as older adults become increasingly likely to receive long-term care in a residential setting. 6 Residential care settings are along the continuum between an individual’s private residence and nursing home facilities. Residential care facilities (RCFs) serve adults in need of assistance with activities of daily living, but they do not offer skilled care like what is provided to those residing in nursing homes. 7 RCFs include assisted living residences, board and care homes, congregate care, enriched housing programs, homes for the aged, personal care homes, and shared housing establishments. 7
eHealth capabilities and health care
Successful implementation of electronic health records (EHRs) provides a systematic approach to gather and maintain health information and improve the quality and continuity of communication between providers (i.e. physicians, nurses, pharmacies, and staff) within and between levels of care. 8 The implementation and adaption of EHRs will equip health care providers with timely access to the most updated patient records to make appropriate medical decisions.9–11 Such interoperability (e.g. ability to exchange and interpret shared data) 12 is especially critical for vulnerable or at-risk (e.g. having one or more chronic conditions) populations using long-term care who are often involved in complex, interdisciplinary cases, and experience frequent transitions. 13 Utilization of electronic health information exchange (EHIE) can potentially improve the quality and efficiency of long-term care by reducing the chances of errors and duplication of health care services and improve coordination of care between RCFs and other primary care facilities.9–11 For example, computerized capabilities facilitating exchange of patients’ prescription information between RCFs and medical professionals could be used as a safeguard against medication errors.14,15
Despite the potential benefits of EHR systems, implementation of the system is not always a feasible option in every RCF. A nationwide snapshot indicated that only about 17 percent of RCFs adopted EHRs as of 2010 16 and only increased to 20 percent in 2012. 17 EHR adoption rates in hospitals increased from about 10 percent in 2008 to 60 percent in 2013. 18 While hospitals and acute care facilities have shown exponential increases in EHR adoption, RCFs have lagged behind other health care settings in EHR adoption. Evidence surrounding EHR adoption in long-term care settings including RCFs is scarce, and past reports consist mainly of non-nationally representative cross-sectional snapshots at different time points in different states and different settings. For example, the 2007 report from California indicated that about 44 percent of RCFs (with more than 75 beds) fully or partially implemented EHRs, 19 while the 2008 report from Minnesota indicated 32 percent of nursing homes had EHRs, 20 and a 2010–2011 report from Texas indicated only about 15 percent of long-term care facilities had EHRs. 21
The initial adoption of an EHR may disrupt some aspects of usual business given the likelihood of errors in use due to changes in tasks and work flow, 22 but as discussed in the preceding discussion, the adaption and implementation of EHRs and other eHealth capabilities can improve cost and overall facility efficiency and quality of care for patients over time. 23 However, one of the key factors that determine EHR adoption and implementation in a RCF is the initial cost.22–24 There are mixed observations about the relationships between EHR implementation and facility characteristics. A cross-sectional study done in Texas showed that rates of EHR implementation in long-term care facilities were lower for rural facilities. 22 The study failed to show any significant association between EHR implementation rates and other facility characteristics (e.g. affiliation type, size, and ownership status), while other reports on the EHR utilization in long-term care facilities indicated a positive association between the EHR utilization rates and facility size and affiliation status.17,21,25
Thus far, we have presented evidence of changing demographics and needs among older adults. More specifically, the increasing population of older adults (age 65 and older), the relatively high potential need for health care resources among this group of older adults given the prevalence of chronic disease, and the potential benefits that eHealth can add in terms of improving health care transitions and daily living. While some research efforts have looked into the use of EHIE in long-term care facilities such as nursing homes, 24 little research has focused on their use in RCFs aside from limited descriptive analysis. 16
Objectives
It is hypothesized that facility characteristics such as size, chain affiliation, and ownership type will affect the implementation and utilization of eHealth capabilities in RCFs. Given the potential of eHealth capabilities to improve the delivery of care and communication between settings, the overall objective of this study was to identify the current utilization of eHealth capabilities among RCFs throughout the United States.
The aims of this study were as follows: (Aim 1) to ascertain whether computerized systems of RCFs across the United States supported one or more of the following five eHealth elements: (1) EHIE with pharmacies; (2) EHIE with physicians; (3) computerized capabilities for discharge and transfer summaries; (4) computerized capabilities for medical provider information; and (5) having an EHR; (Aim 2) to identify environmental and facility characteristics associated with these computerized capabilities.
While there is limited research regarding EHR utilization among RCFs on a national level, 26 our analyses are among the first to describe multiple components of these eHealth capabilities across different providers and care protocols.
Materials and methods
Data and design
Secondary data analysis was conducted using the most recent national-level public-use data on EHR adoption by RCFs in United States, the National Survey of Residential Care Facilities (NSRCF) public-use file (2010). The NSRCF public-use file is available from the Centers for Disease Control and Prevention (CDC) website. Our analyses used a nationally representative sample of RCFs (n = 2302) representing 31,100 facilities in all 50 US states. These facilities served over 700,000 residents in 2010. This survey used a two-stage probability sampling design (i.e. facilities were identified, and then RCF in-person interviews were conducted). This dataset has two components, the resident file and the facility file. In the public-use file (used in this analyses), facility surveys and resident surveys were not linked, preventing resident demographic information from being joined with the facility file. Because the facility was our desired unit of analysis, we used the facility file for all study analyses. The NSRCF dataset is the first national survey of RCFs and the NSRCF is only available for the 2010 calendar year. 27 The sample is weighted to reflect all RCFs throughout the United States allowing for greater generalizability.
Variables
Dependent variables
Our outcomes of interest included computerized capabilities of RCFs. We included five dichotomous outcomes in our analysis from five separate variables in the public-use file. The first two outcomes included: (1) having computerized systems for EHIE with pharmacies and (2) having computerized systems for EHIE with physicians. These variables were operationally defined in the NSRCF questionnaire using the following question: “Does this facility’s computerized system support EHIE with one or more specified providers?” 28 The third outcome included whether facilities had computerized systems for discharge and transfer summaries. A fourth outcome included whether a RCF had computerized capabilities for medical provider information. The third and fourth outcomes were operationally defined using the following question from the NSRCF questionnaire: “Does this facility have the following computerized capabilities?” Our fifth outcome of interest was the presence of EHRs, defined in the NSRCF questionnaire as “a computerized version of the resident’s health and personal information used in the management of the resident’s health care.” In all study analyses, these five dependent variables were treated dichotomously. Each of the outcomes chosen for our study plays a critical role in determining the quality of care transitions between care settings, especially for complex cases (e.g. patients with one or more chronic conditions).9–11,13 Care transitions in this context refer to the transition from one setting (e.g. RCF) to another care setting (e.g. hospital). 29 Thus, these five variables serve as a way to measure factors potentially associated with care transitions and thereby potentially affecting the receipt of high-quality health care and health outcomes of residents. We also created a variable to ascertain the depth of EHIE. This was a descriptive measure (range: 0–5) based on whether facilities had one, two, three, four, or all five of our outcomes of interest.
Control variables
We included facility characteristics and an environmental characteristic (i.e. rurality) in study analyses to explore factors that may be associated with whether a RCF had one or more of the five computerized capabilities under study. 26 Metropolitan Statistical Area (MSA) status, served as our geographic characteristic measuring rurality, coded as MSA (urban) versus non-MSA (rural). Details about these variables were taken directly from the CDC’s website. 16 Chain affiliation included those RCFs owned by a chain, group, or multi-facility system versus RCFs that were not chain-affiliated. Ownership type included private, for-profit versus private non-profit and state, county, or local government ownership. Facility sizes included small (4–10 beds), medium (11–25 beds), large (26–100 beds), and extra-large (over 100 beds). The percent of adults under age 55 years was also included as a measure of the age of the RCFs residents.
Statistical analysis
We used SAS 9.4 (Cary, NC) for all analysis. The complex survey design was incorporated using SAS survey procedures. Bivariate analyses were used to compare facility characteristics by our five dependent variables. A single binary logistic model was used to predict RCFs having any computerized capabilities defined as having 1–5 capabilities versus 0 computerized capabilities. A series of five binary logistic regression models were used to examine factors associated with RCFs’ computerized capabilities across each of the five eHealth capabilities individually. Adjusted analysis accounts for rurality, chain affiliation, ownership type, facility size, and the percent of adults under 55 years of age. By controlling for other variables, we have attempted to isolate the effect of each independent variable on EHR utilization. These inferential analyses can serve as stronger evidence for the message/assertion than a descriptive analysis based on frequencies.
Results
Overall, the majority of RCFs lacked any computerized capabilities in 2010 (54.9%). The percent of RCFs with one capability was 17.9 percent, followed by 16.1 percent for those with two capabilities, 6.9 percent for those with three, and 2.8 percent for those with four capabilities. Those facilities with all five computerized capabilities represented approximately 1.4 percent of all RCFs in the United States.
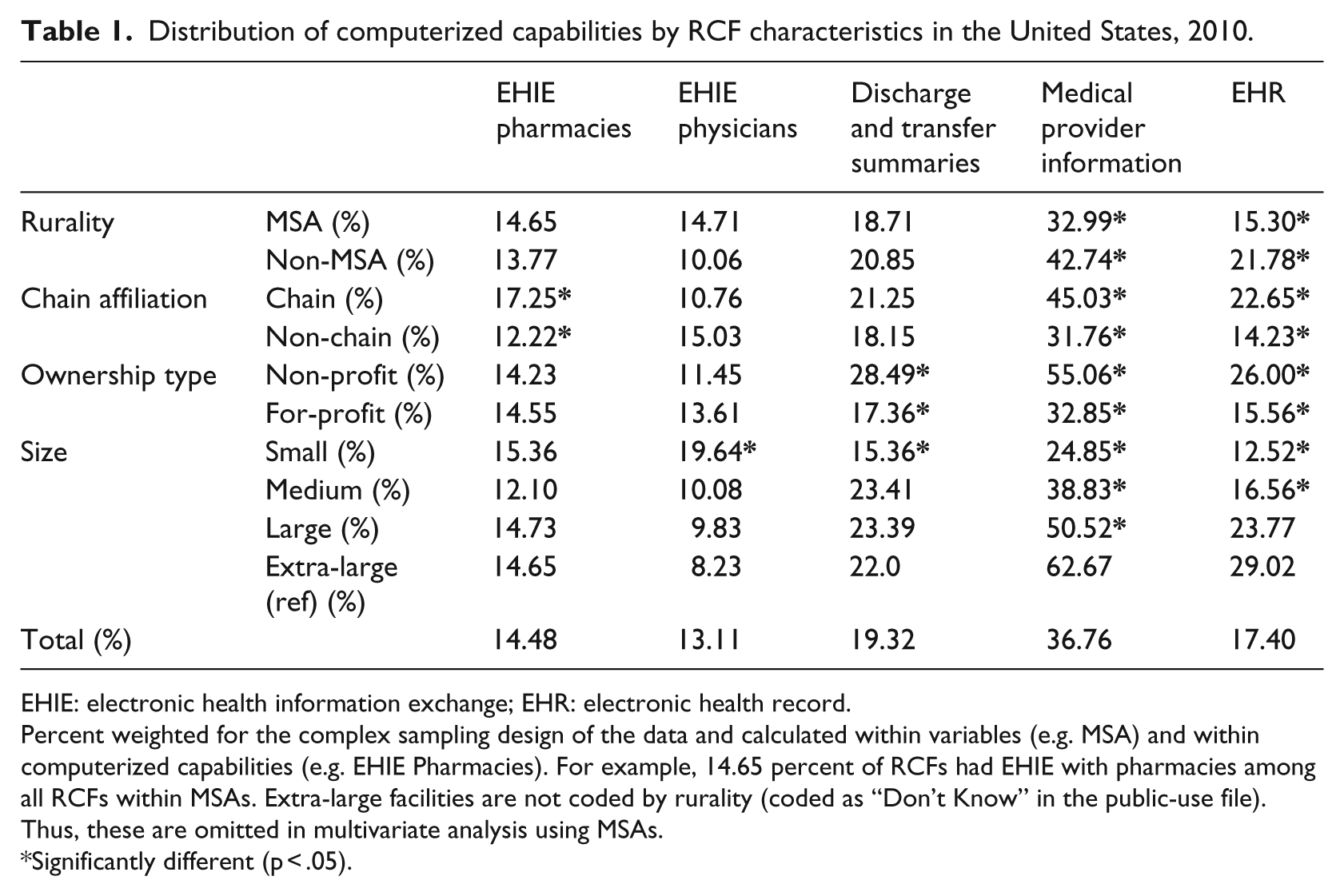
Across the United States, the number of RCFs with one or more of the five computerized capabilities under study varied by facility and geographic characteristics (Table 1).
Distribution of computerized capabilities by RCF characteristics in the United States, 2010.
EHIE: electronic health information exchange; EHR: electronic health record.
Percent weighted for the complex sampling design of the data and calculated within variables (e.g. MSA) and within computerized capabilities (e.g. EHIE Pharmacies). For example, 14.65 percent of RCFs had EHIE with pharmacies among all RCFs within MSAs. Extra-large facilities are not coded by rurality (coded as “Don’t Know” in the public-use file). Thus, these are omitted in multivariate analysis using MSAs.
Significantly different (p < .05).
EHIE with pharmacies
Nationwide, 14.5 percent of RCFs reported having computerized systems for EHIE with pharmacies. Having computerized systems for EHIE with pharmacies was higher for chain-affiliated RCFs (17.3%) than for RCFs that were not chain-affiliated (12.2%). Rates for this computerized capability did not vary significantly within MSA/rurality (14.7% for MSAs (urban); 13.8% for non-MSA (rural)), ownership type (14.2% for non-profits; 14.6% for for-profits), or facility size (rates from a high of approximately 15.4% in small facilities to a low of 12.1% in medium facilities, on average).
EHIE with physicians
Nationally, having computerized systems for EHIE with physicians was representative of approximately 13.1 percent of all RCFs. This was the lowest among all computerized capabilities under study. Rates for this computerized capability did not vary significantly within rurality (14.7% for urban RCFs; 10.1% for rural), chain affiliation (10.8% for chain-affiliated; 15.0% for RCFs that were not chain-affiliated), or ownership type (11.5% for non-profits; 13.6% for for-profits). On average, reporting computerized systems for EHIE with physicians was higher for small facilities (19.6%) when compared to extra-large facilities (8.2%).
Discharge and transfer summaries
Facilities with computerized systems for discharge and transfer summaries represented approximately 19.3 percent of all RCFs. Rates for this computerized capability did not vary significantly within rurality (18.7% for urban; 20.9% for rural) and chain affiliation (21.3% for facilities that were chain-affiliated; 18.2% for those that were not chain-affiliated). The rate of reporting computerized systems for discharge and transfer summaries was higher for non-profits (28.5%) with nearly double the rates of having these capabilities when compared to for-profits (17.4%). On average, the rate of reporting computerized systems for discharge and transfer summaries was lower among small facilities (15.4%) when compared to extra-large facilities (22.0%).
Medical provider information
Having computerized systems for medical provider information was the most common computerized capability reported among the five under study, with rates at 36.8 percent on average. The rate of reporting computerized systems for medical provider information was higher for rural areas (42.7%) when compared to urban areas (33.0%). The rate was also higher for chain-affiliated facilities (45.0%) versus facilities that were not chain-affiliated (31.8%). Rates were higher for non-profits (55.1%) when compared to for-profits (32.9%). On average, the rate of reporting computerized systems for medical provider information was highest for extra-large facilities (62.7%) than all other smaller-sized facilities (24.9% for small, 38.8% for medium, and 50.5% for large).
EHRs
Across the United States, RCFs reporting having EHRs represented approximately 17.4 percent in 2010. The rate of reporting having an EHR was higher for rural areas (21.8%) when compared to urban areas (15.3%). Rates were higher for chain-affiliated facilities (22.7%) versus facilities that were not chain-affiliated (14.2%). Across ownership type, rates were higher for non-profits (26.0%) when compared to for-profits (15.6%). On average, the rate of having EHRs was highest for extra-large facilities (29.0%) than both small-sized (12.5%) and medium-sized (16.6%) facilities.
Adjusted analysis
Table 2 presents results from the single binary logistic regression model predicting any (1+) versus none (0) computerized capabilities. After controlling for all other terms in the model, RCFs that were not chain-affiliated (odds ratio (OR) = 1.3), that were for-profit (OR = 2.0), and that were small versus large (OR = 2.5), or medium versus large (OR = 1.7) were more likely to lack a high number of computerized capabilities.
Adjusted analysis predicting a higher number of eHealth capabilities.
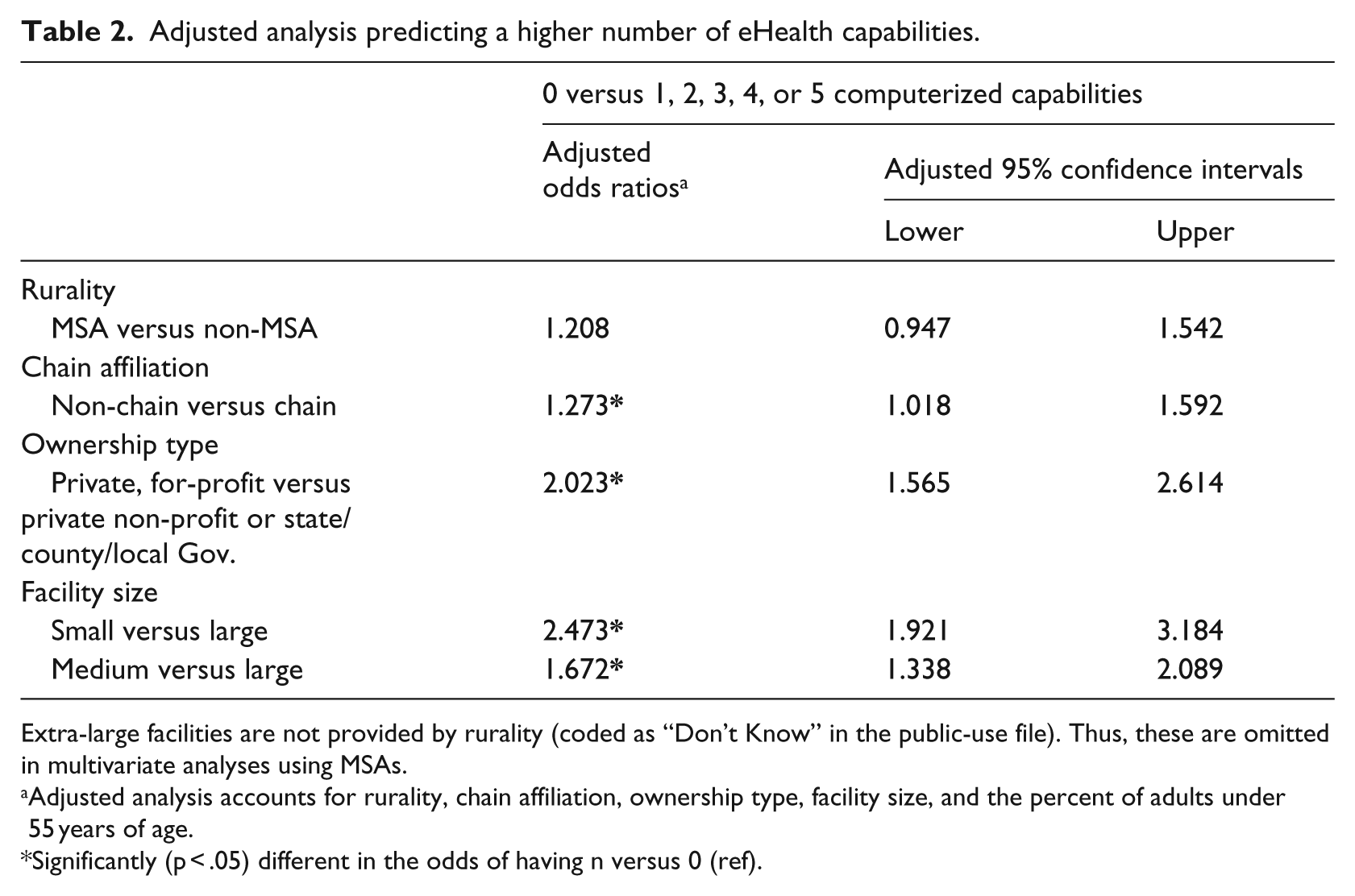
Extra-large facilities are not provided by rurality (coded as “Don’t Know” in the public-use file). Thus, these are omitted in multivariate analyses using MSAs.
Adjusted analysis accounts for rurality, chain affiliation, ownership type, facility size, and the percent of adults under 55 years of age.
Significantly (p < .05) different in the odds of having n versus 0 (ref).
Table 3 presents binary logistic regression analyses predicting the absence of the five individual computerized capabilities after adjusting for MSA status (rurality), ownership type, facility size, and the percent of adults under 55 years of age. EHIE pharmacies: The absence of computerized systems supporting EHIE with pharmacies was associated with chain affiliation. Facilities that were not chain-affiliated were more likely (OR = 1.7) to lack this capability. EHIE physicians: Absence of computerized systems supporting EHIE with physicians was associated with facility size. Facilities that were small-sized (versus large-sized) were less likely (OR = 0.4) to lack access to these computerized capabilities. Discharge and transfer summaries: Absence of computerized capabilities for discharge and transfer summaries was associated with facility size and ownership type. Facilities that were for-profit were more likely (OR = 1.6) to lack these computerized capabilities. Facilities that were small (versus large) were more likely (OR = 1.6) to lack access to these computerized capabilities.
Adjusted analysis predicting the absence of computerized capabilities.
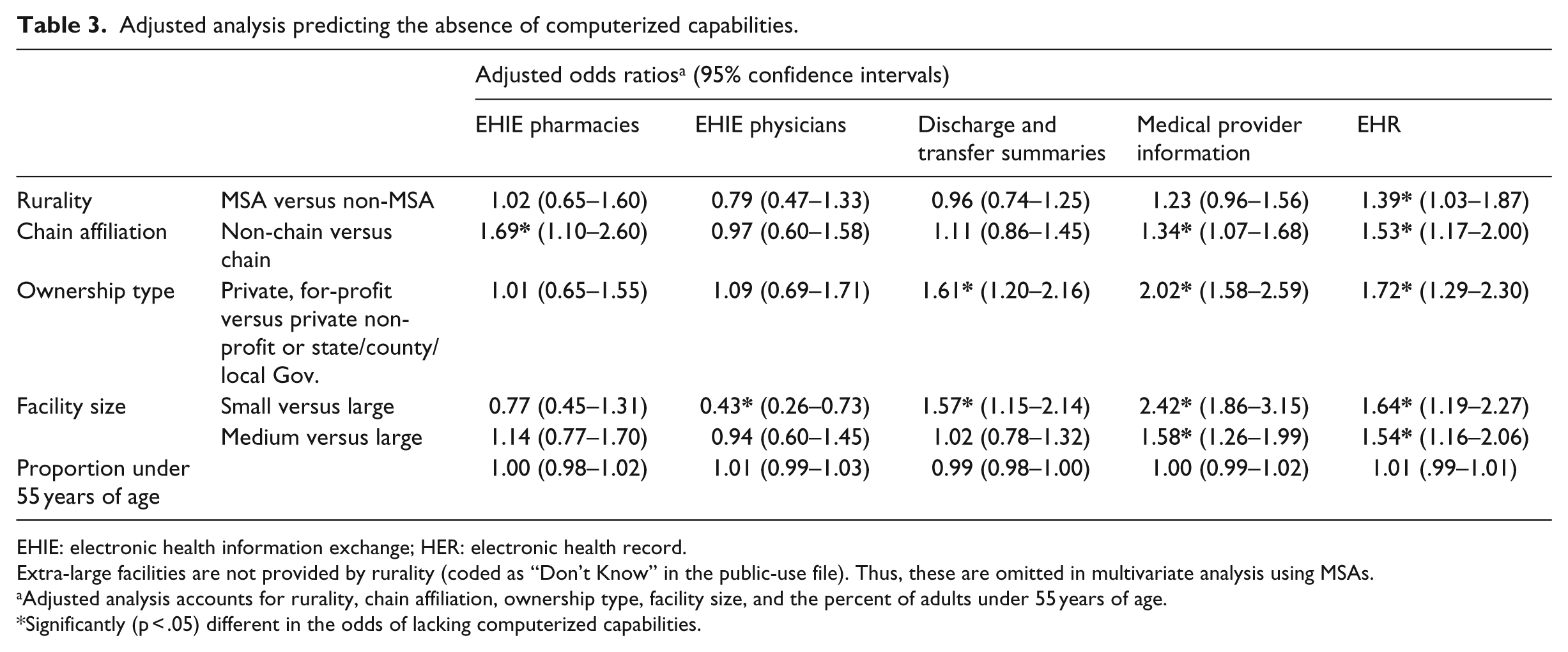
EHIE: electronic health information exchange; HER: electronic health record.
Extra-large facilities are not provided by rurality (coded as “Don’t Know” in the public-use file). Thus, these are omitted in multivariate analysis using MSAs.
Adjusted analysis accounts for rurality, chain affiliation, ownership type, facility size, and the percent of adults under 55 years of age.
Significantly (p < .05) different in the odds of lacking computerized capabilities.
Medical Provider Information: The absence of computerized capabilities for having medical provider information within facilities was associated with chain affiliation, ownership type, and facility size. Facilities that were not affiliated with chains (vs chain-affiliated) (OR = 1.3), that were for-profit (vs not-for-profit) (OR = 2.0), or that were small or medium-sized (vs large) (OR = 2.4; OR = 1.6, respectively), were more likely to lack these computerized capabilities. EHR: Absence of an EHR was associated with MSA status, chain affiliation, ownership type, and facility size. Facilities that were MSAs (vs non-MSAs) (OR = 1.4), not affiliated with a chain (vs chain-affiliated) (OR = 1.5), that were for-profit (vs not-for-profit) (OR = 1.7), that were small or medium-sized (vs large) (OR = 1.6; OR = 1.5, respectively) were more likely to lack an EHR.
Discussion
The purpose of this study was to examine RCFs computerized systems supporting eHealth capabilities including EHIE with health care professionals. The vast majority of RCFs lacked computerized capabilities for EHIE with pharmacies, EHIE with physicians, discharge and transfer summaries, medical provider information, or lacked an EHR. This may leave hundreds of thousands of residents of RCFs lacking access to these potentially quality improving and cost-effective technologies11,30 resulting in less continuity of care between care settings and within facilities. For example, these computerized capabilities may lead to more efficient communication between providers and others during care transitions. 8 This is especially worrisome for older adults, because evidence suggests nearly one in five experiences a care transition each year. 31 High-quality care is not completely dependent on having eHealth technological capabilities. However, as more older adults use these facilities and providers increasingly rely on EHIE, facilities without these computerized capabilities may face lower quality of care. 22
Comparisons over time
While we were restricted to currently available public-use files for 2010, we are able to make comparisons in the capabilities among RCFs using more recent data from 2012. Comparisons to the National Study of Long-term Care facilities were incorporated to allow for the inclusion of more recent evidence regarding the use of eHealth capabilities in residential care communities. 32 The percent of facilities reporting having an EHR rose to 20 percent in 2012 32 from 17 percent in 2010. In terms of reporting EHIE with pharmacies, there was an increase from approximately 15 percent in 2010 to approximately 20 percent in 2012. 32 In terms of EHIE with physicians, the rate was stable over time remaining at approximately 13 percent in 2012. 32 Although there has been an increase in EHRs and EHIE utilizations, the increment is relatively small in comparison with other health care facilities. Further research should be conducted to explore the secular trends in EHR and EHIE adoption as well as barriers and facilitators for adopting and utilizing the technologies.
Rurality did not play a major role in the likelihood that a RCF would report most computerized capabilities under study. In adjusted analysis, among the five computerized capabilities, only having an EHR varied by rurality. Rural RCFs were more likely to report having an EHR, which was surprising given the relative limited resources in rural areas throughout the United States. 33 This is inconsistent with previous findings in Texas, where rural long-term care facilities had lower rates of EHR implementation than urban long-term care facilities. 22 In the United States, states regulate RCFs, which may lead to variations in state and national data. 22
Having the capacity to use electronic health information and related computerized capabilities varied by characteristics of RCFs across the United States. Chain affiliation played a role in certain computerized capabilities, where not being affiliated with a chain served as a risk factor for lacking computerized capabilities to support having EHIE with pharmacies, medical provider information, and lacking an EHR. This is consistent with the previous findings in both RCFs and nursing homes.24,34 Chain-affiliated RCFs may have greater resources to pool in deciding whether to invest in these computerized capabilities; however, more research is needed to assess this in RCFs.
Similarly, differences were seen across ownership type, where being for-profit, served as a risk factor for lacking computerized capabilities to support having discharge and transfer summaries, medical provider information, and lacking an EHR. This is similar to other research comparing RCFs and nursing homes, where non-profit entities were more likely to have computerized capabilities for EHRs and other EHIE. 35 Ownership type plays a role in several organizational decisions and business plans, which may contribute to whether a facility decides to invest in these computerized capabilities. The funding source may also play a role as non-profits may be more likely to receive more from private donations or governmental assistance. More research is needed to understand why non-profits were more likely to have these computerized capabilities.
Small facility size (vs large) was a risk factor for lacking computerized capabilities to support having discharge and transfer summaries, medical provider information, and EHRs. This is consistent with previous findings indicating larger facilities were more likely to have computerized capabilities for discharge and transfer summaries. 36 In contrast, small facility size (vs large) was a protective factor for lacking EHIE with physicians. Thus, facility size may play a major role in whether a facility has access to certain eHealth computerized capabilities.
The successful implementation of eHealth systems in residential care settings is yet to be seen for the vast majority of RCFs. This study provides evidence to suggest that different facility characteristics are associated not only with EHR adoption but also with different dimensions (e.g. EHIE) of eHealth capabilities. This knowledge may aide in identifying particularly vulnerable facilities in terms of having access to eHealth technologies.
In addition to facility characteristics, previous studies identified cost, inadequate information management, and inter-agency cooperation as barriers37,38 to the successful implementation of these EHRs. High initial costs and maintenance cost is the most prevalent, primary barrier for EHR adoption.22–24 The successful implementation of EHRs and other eHealth systems not only involves the application of eHealth technologies, but also includes the supportive hardware/software environment and health professionals’ efforts. Existing EHR systems have been mainly designed for hospital and acute care settings, thereby posing greater challenges for EHR adoption in RCFs than in other health care settings. 39 Furthermore, user perception and other implementation issues (e.g. work flow change, additional work training, and cultural changes), and facility location were associated with EHR adoption in long-term care facilities including RCFs.17,23
Identifying potential facilitators in the adaption of eHealth capabilities is also critical to furthering the implementation of these capabilities. Factors that facilitate the successful implementation of eHealth services include health professional/patient relations and organizational support. 37 In addition, governmental support, having a clear implementation plan, and training programs have all been shown to be facilitators of the adoption of EHRs in long-term care facilities. 40 More research is needed to identify other facilitators that can further enable RCFs facing the most gaps in the implementation and adaption of these eHealth technologies. As EHR vendors design EHR systems for acute and non-acute care settings, they should keep in mind the broader implementation and adaption in different care settings (e.g. long-term care settings) and the unique needs of such settings. More research is also needed to both identify potential barriers and facilitators in EHR adoption and maintenance for RCFs in different contexts, and equally important, to identify potential recommendations or standardized guidelines in the successful implementation of eHealth capabilities throughout the United States.
Limitations
This study was a cross-sectional analysis and as such does not provide trends over time. However, because only the 2010 NSRCF dataset is available for public use, we were limited to using a cross-sectional study design. However, we were able to make comparisons with more recent data (2012) 32 in terms of changes in the use of eHealth capabilities over time. In addition, the level of analysis of interest for this study was at the facility level. Thus, inferences could only be made for facilities, not to individuals. The lack of geographic information for extra-large facilities prevented analyses across rurality and the inclusion of extra-large facilities in adjusted analyses; however, these data were not available in the public-use file. Additionally, our list of facility characteristics did not encompass the entirety of characteristics that may influence our outcomes. 26
The NSRCF dataset provides reliable data at the national level, which adds to the strengths of the study. However, these data were self-reported, and it is possible that the facility directors and their designated staff members could have over- or under-reported certain computerized capabilities. In addition, information on meaningful use was not specifically targeted with this survey preventing further comprehensive investigation into the quality of these eHealth capabilities.
Policy implications
Paying for long-term care is an issue that many individuals face, as having resources at later age or having long-term care insurance is not universal. 41 Policy makers are interested in finding ways to reduce the health care cost burden facing our aging population. Understanding what factors are associated with gaps in the availability of EHIE capabilities and other eHealth capabilities allows policy makers to understand where resources may be best allocated for those lacking these resources. Thus, initiatives aimed at increasing uptake of computerized capabilities may be targeted to RCFs.
The Patient Protection and Affordable Care Act (2010) included health information technology legislation and regulations specific to the promotion of EHRs and secure electronic exchange. 42 Several resources have been created to further this effort including the Health Information Technology for Economic and Clinical Health (HITECH) Act (2009) 43 and the Medicare and Medicaid EHR Incentive Program. In particular, the Medicare and Medicaid EHR Incentive Program is limited to physicians, nurse practitioners, certified nurse-midwives, dentists, and physician assistants working in Federally Qualified Health Centers or Rural Health Clinics. 44 Thus, RCFs with eHealth capabilities may only indirectly benefit from this legislation. More research will be needed to understand the full consequences of these efforts.
Finally, the largest public payer for long-term care is Medicaid; however, Medicare does cover limited skilled services or rehabilitative care. 45 State policy makers and other stakeholders have shown support of using Medicaid to cover residential care living services, where states can choose to do so through the Medicaid home and community-based services (HCBS) waiver program. 5 In 2002, 36 states expanded their scope of Medicaid services to cover older adults in RCFs. 5 In 2010, approximately 43 percent of RCFs had residents with at least some portion of their care paid through Medicaid. 16
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.