
Abstract
Electronic health records are increasingly used in regional health authorities, healthcare systems, hospitals, and clinics throughout North America. The emergency department provides care for urgent and critically ill patients. Over the past several years, emergency departments have become more computerized. Tablet computers and Smartphones are increasingly common in daily use. As part of the computerization trend, we have seen the introduction of handheld computers, tablets, and Smartphones into practice as a way of providing health professionals (e.g. physicians, nurses) with access to patient information and decision support in the emergency department. In this article, we present a scoping review and outline the current state of the research using mobile devices in the emergency departments. Our findings suggest that there is very little research evidence that supports the use of these mobile devices, and more research is needed to better understand and optimize the use of mobile devices. Given the prevalence of handheld devices, it is inevitable that more decision support, charting, and other activities will be performed on these devices. These developments have the potential to improve the quality and timeliness of care but should be thoroughly evaluated.
Introduction
Electronic health records (EHRs) are becoming more widespread in regional health authorities, healthcare systems, hospitals, and clinics in North America. EHRs have afforded healthcare professionals (e.g. physicians, nurses) the opportunity to access patient information anytime and in many locations in a healthcare organization (where there is a computer available). Such rapid access to patient information has made EHRs a valuable tool and an aid to providers where patient care-related decision-making is concerned.
Historically, health professionals using desktop computers accessed EHRs. Desktop computers are located in specific areas of a healthcare organization (e.g. at the nursing station, at the end of a hallway) and cannot be easily moved from one location to another by a provider. With the development of varying types of mobile devices, EHRs and their components (e.g. provider order entry, medication administration systems, laboratory information systems) now allow providers to input and access patient information from any location in a healthcare facility.
Over the past few years, we have seen the introduction and use of not only desktop computers but laptops, handheld tablets, or other types of portable devices (e.g. Smartphones, Personal Digital Assistants—PDAs) into healthcare facilities for general use by providers to input, access, and review patient information. These devices have also been used as a source of information. They provide ubiquitous access to decision-support systems (DSS) such as UptoDate®. These DSS can be used in the process of care (if accessible via a mobile device).
Free access to the EHR within a healthcare organization can influence how healthcare professionals provide patient care. With current advancements in mobile devices and the introduction of new types of devices such as Smartphones and tablets, health professionals now have the ability and the opportunity to access EHRs and DSS in real time when caring for a patient (i.e. when there is a need to make a decision). Nowhere is such access to EHRs and DSS more important than in the emergency department (ED), where having rapid access to information is critical to being able to care for patients with life-threatening injuries or illnesses.
Therefore, the nature and structure of care in EDs is conducive to the use of mobile devices. In the ED, patients are treated by a variety of providers who physically move from one location to another (e.g. from one treatment room to another). Mobile devices that provide access to the EHR and DSS allow patients to be easily followed for the duration of their ED visit and for care decisions to be made at the bedside. Therefore, the purpose of this scoping review is to shed light on the current state of the research literature focusing upon the use of mobile devices in the ED.
Methods
Literature search
We conducted a search of the literature to identify articles that studied the impact of mobile devices in the ED. Studies were eligible for inclusion if they (1) examined mobile devices such as wireless mobile computers, mobile workstations, PDAs, handheld computers, tablets, or Smartphones and (2) evaluated an intervention in the ED. Studies were excluded if they (1) focused on the design of software alone; (2) lacked an evaluation component; (3) studied a clinician or patient educational intervention only; (4) were a case report, abstract, survey, editorial, or letter to the editor; (5) were in non-English language; or (6) focused on the use of a mobile device for only image-display purposes (e.g. radiology report reading). We excluded articles that did not evaluate the effectiveness of an application or device being actively used in ED practice.
The following electronic literature databases PubMed® (MEDLINE®), 1 OVID CINAHL®, 2 ISI Web of Science™, 3 and EMBASE®4 were searched from their respective inception to 18 July 2012. In MEDLINE, all search terms were defined as keywords and Medical Subject Headings (MeSH®) unless otherwise noted; in the remaining databases, the search terms were defined only as keywords. The search strategy was based on the concept “emergency medicine” combined with concepts representing any kind of mobile implementation. Search terms included “emergency medicine” and any combination of the terms “tablet computer,” “phone,” “medical informatics,” “mobile,” “tablet,” “iPad,” or “PDA” and relevant plurals. The exact PubMed query is shown below:
(emergency medicine OR emergency services, hospital) AND (tablet computer OR phone OR medical informatics OR mobile OR tablet OR iPad OR PDA).
An additional MeSH term search was performed and the results included in the title and abstract review:
(medical informatics AND emergency medicine AND computers, handheld).
Review of identified studies
Two reviewers reviewed the titles and abstracts of all articles identified using the keyword searches. All articles were reviewed by both reviewers and discussed. All disagreements between reviewers regarding the articles were resolved through discussion (i.e. consensus was reached about each article). Articles meeting the inclusion criteria outlined earlier in this article were pulled for full manuscript review. The studies were then examined for redundancy (e.g. findings of one study reported in two different reports) and duplicate results were removed. The full text of included articles was obtained. Following this, the two researchers then reviewed the full manuscripts. Again, disagreements were resolved through discussion until consensus was reached.
Analysis
The two reviewers extracted relevant themes and data from the included articles. Several themes emerged from the data extracted from the articles, which will be outlined in greater detail in the results section of this article.
Results
Included articles
The literature search produced 6672 articles during the time period, with 4280 coming from MEDLINE, 53 from CINAHL, 1922 from Web of Science, and 417 from EMBASE. After removing 1281 duplicate articles, 5363 were further excluded based on review of the titles and abstracts. Of the remaining 28 articles, 18 were excluded (see Figure 1). A total of 10 articles met the inclusion criteria set in the study. Table 1 shows the findings collected from the included studies. The articles had a median publication year of 2008 (range 2003–2012). No articles discussed the same intervention.
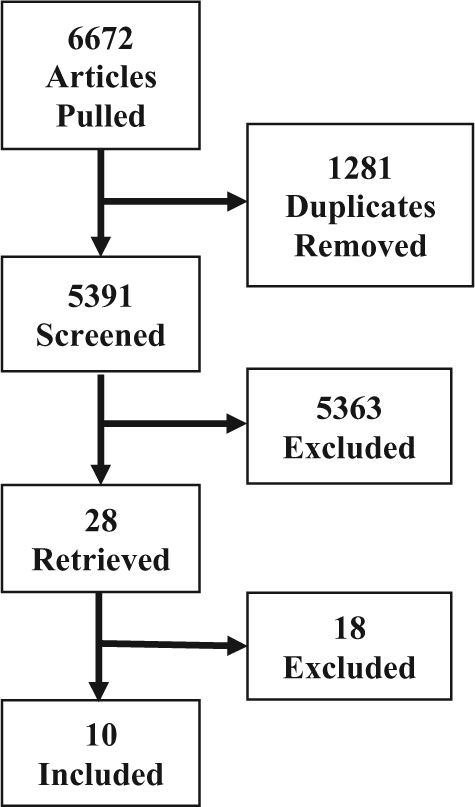
Consort diagram of included studies.
Included studies.
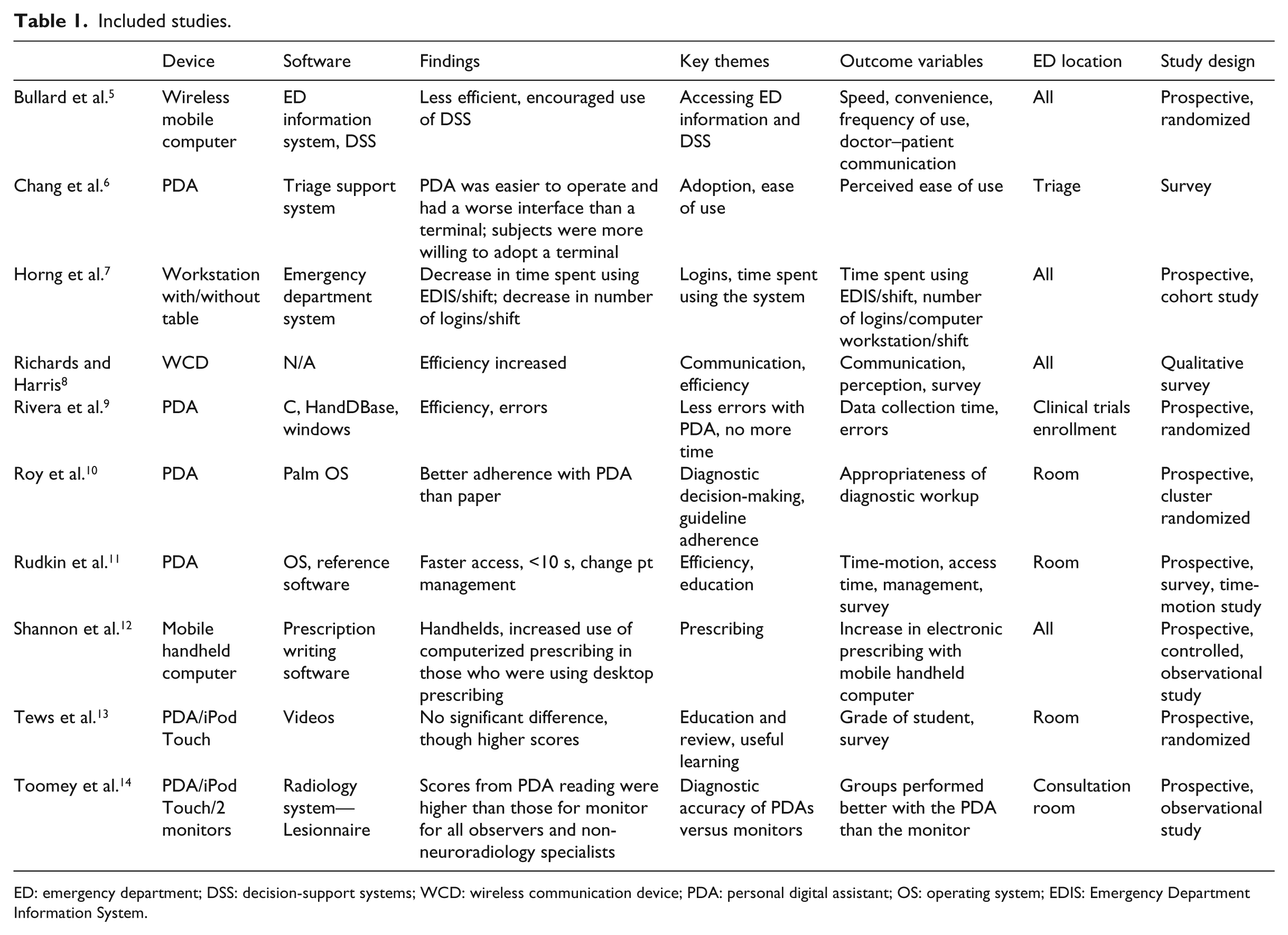
ED: emergency department; DSS: decision-support systems; WCD: wireless communication device; PDA: personal digital assistant; OS: operating system; EDIS: Emergency Department Information System.
Themes
Several key themes emerged from our review of the literature. These included (1) descriptions of the types of mobile devices and how they were used in the ED, (2) the use of prospective designs, (3) the type of software used, (4) a focus on improved efficiency and speed when using mobile devices, and (5) ED location of mobile device use. These themes were extracted post hoc after study inclusion. These themes are discussed below.
Theme 1: Descriptions of the types of mobile devices
Of the 10 studies, 7 employed handheld PDAs, with the remaining studies employing wireless mobile computers, wireless mobile workstations, and an iPod® device. Each of these devices was evaluated in terms of its ability to support effective and efficient work in the ED. It is interesting and worthy to note that the first Smartphone came on the market in 1994. 15 The first tablet launch occurred in the 1980s, 16 although it did not gain popularity until 2002. 16 Yet, no Smartphones or tablets were evaluated as part of this body of research. Instead, PDAs were primarily studied and evaluated for their ability to support provider work in the ED.
Although handheld devices are a useful technology, Smartphones and tablets have touch-screen technology that has not been fully evaluated in the ED, and it is unclear what the effects of this new generation of mobile devices would have upon health professional work (as compared to PDAs and mobile workstations). With the emergence and growth in popularity among both providers and healthcare consumers of touch-screen mobile devices such as the Apple® Smartphone and tablet (i.e. iPad®), it is important to study their impact upon ED settings as they are introduced to support patient care.
Although the early studies performed on PDAs6,9–11 provide some insights, they do not take into account the introduction of the more sophisticated and user-friendly features and functions of these mobile devices on work, workload, and patient outcomes in the ED.
There are significant differences between touch-screen mobile devices (e.g. iPhone®, iPad) and PDAs in terms of user interaction and the methodologies that were used to design and develop these new devices. These differences may influence the results of ED studies involving mobile device use, for example, more user-friendly touch-screen Smartphones may improve user efficiency.
Additionally, the limited black-and-white interface and data entry that involved either button-clicks or had to be performed with a stylus and a specific writing recognition system or stylus touch-typed keyboard that are part of PDA technology have been improved upon by technology designers as evidenced by the launch of a new generation of Smartphones and tablets that are easier to use and can do more.
Newer touch-screen Smartphones and tablets give users access to keyboards as part of the device. The user interface in new touch-screen devices is also far superior to the original handheld PDAs, allowing users to extend the nature of their work with application (such as viewing radiology images).
Despite the widespread adoption of this new generation of mobile devices by healthcare consumers and health professionals, research is needed to better understand the impacts of these new mobile devices on work, workload, and patient outcomes. Such work is critical to developing device implementation methods that ensure safe and effective adoption of these devices. Unfortunately, published research on the accuracy and usefulness of these mobile devices for medical care has not kept up with the hardware and software development (i.e. the development of Smartphones and tablets with touch-screen technology, access to a keyboard, and ability to access high-quality color images and videos).
Theme 2: The use of prospective designs
The study designs chosen to examine mobile device use in the ED include nine prospective studies and three surveys (one study was both prospective and a study component). The prospective studies include four randomized studies with physicians, 5 patients, 9 department, 10 and medical students 13 being the unit of randomization in the studies.
In this review of the literature, the researchers identified that many of the ED mobile device studies employ prospective, randomized control trial-type designs. Although these types of designs are considered the gold standard in the medical literature (evaluating the introduction of a new intervention such as a new drug), they have been shown to provide fewer insights as to how a technology is used in a given healthcare setting. 17
Researchers such as Kaplan and Shaw 18 have advocated the use of qualitative research methods in addition to quantitative methods in the fields of medical and health informatics. More recent research conducted19,20 outlines the importance of conducting qualitative studies in conjunction with quantitative studies when evaluating the introduction of a new device into a clinical setting. As Ash et al. 21 suggest, qualitative studies allow researchers to document the intended as well as the unintended consequences of introducing a technology (beyond what was intended to be studied) by the research designers. Understanding how a technology is appropriated or adopted is key to determining how the technology supports or detracts from patient care. For example, initial reports on technology-induced errors emerged from the qualitative research literature, which is now informing national-level policy-making bodies such as the Institute of Medicine. Other qualitative research has identified how technology can be used in positive ways to enhance care (not originally planned by technology designers or implementers).
Theme 3: Types of software
Figure 2 illustrates the generalized ED workflow. The patient is registered, then moves into a triage process, and is then placed in the appropriate room. In this simplified model of ED workflow, all of the ED care occurs in a room where the patient is located. As a final step, the physician determines the disposition of the patient and a decision is made regarding the patient for either admission or discharge.

General ED workflow.
In an electronic ED, software and hardware are frequently located throughout the department. In a fully integrated ED, patients may be initially registered in the EHR, and this information is passed into that patient’s visit information. Next, the triage nurse is able to access this basic information and clinical information such as a chief complaint and vital signs in the EHR. Here, a nurse may have one of the first targeted opportunities to use an informatics-based DSS in the care process. Once the patient has been moved to a room, a DSS can be used. Here, there is a need to fit the DSS and EHR appropriately into the ED workflow so that prompts or reminders are available at the time of documentation, placing orders, and decision-making. In examining the studies that were identified in this review, several types of software are used (e.g. prescription-writing software, ED information system software, triage support system, videos, and a radiology system). No one type of software is evaluated more than once in terms of its use with a mobile device in the ED setting.
In the last 1 to 2 years, vendors have made an increasing number of DSS tools available through informatics-based systems in conjunction with mobile devices for use in clinical settings such as the ED. Regulatory organizations have taken notice. The US Food and Drug Administration (FDA) approval is now required for mobile device software applications that are used for medical decision-making. This approval is required for mobile medical applications, 22 including Smartphones and other mobile communication devices (e.g. tablets) covering healthcare provider medical and personal use. Software applications that help a provider make a diagnosis, directly view medical information such as a radiographic image, and use a mobile device to deliver information and DSS are included in this software. The need for regulatory approval could impact development and adoption of software applications used with mobile devices. It may also lead to a need to fully evaluate the impact of mobile devices and their software upon clinician work before these technologies are released and approved for more common use. Increasing regulation adds to the urgency for additional research for effective devices and is relevant to the dearth of current published knowledge.
Theme 4: A focus upon improved speed and efficiency and speed when using mobile devices
Much of the research in the area of mobile device use in the ED has focused upon the effects of mobile devices upon the efficiency of health professionals (mainly physicians). First, we noted that many of the studies looked at the efficiency of the software and the providers. Access time was measured in one study, 11 although all three surveys addressed the user’s perceptions of the speed of their use in the system. Other types of efficiencies that were studied included efficiencies arising from improved communication, time spent accessing information, and organizational efficiencies arising from improved guideline accuracy and error reduction. It is interesting and worthy to note that much of his work has focused on efficiency rather than process changes arising from the use of the technology or improvements in patient outcomes. In Figure 2, we outline a general ED workflow. There are several points in the ED workflow where the use of a mobile device in conjunction with software that allows for access to EHR components or DSS to support decision-making would improve the quality of the work performed by providers while integrating this with the work they perform in the ED. No studies attempted to determine where and how the mobile devices and software were integrated so that efficiencies could be achieved beyond the time it took to access information. Such information would be valuable from an implementation perspective and a software design perspective. From an implementation perspective, such knowledge could be transferred to other organizations so that efficiencies could be immediately achieved rather than over time through organizational implementation. These studies focus on efficiencies sustained by an organization when introducing the devices. Little is known about the impacts of the devices on the quality of patient care and subsequent patient health outcomes. Such information is essential in determining if the technology provides any additional benefits beyond those of increasing speed of access to information and the ability to perform some medical and nursing tasks with greater speed.
Theme 5: ED location
Last, due to the nature of mobile devices, most of the interventions that were designed and studied in the ED that we identified in the research were designed and implemented for use throughout the ED. One study evaluated a triage support system, 6 two more were designed to use while in the patient’s room,10,11 and one was designed to be used only in the consultation room; 14 however, the four remaining studies evaluated devices wherever their use was most convenient to the provider. Mobile devices are designed to allow their users to be mobile and access/receive information anywhere and in any place. The strength of mobile devices is their ability to provide their users with access to information and DSS. With the introduction of mobile devices, individuals can have access to small reference books, the EHR, and DSS. Mobile devices can be carried and used anywhere. Handheld devices can function the same way by helping to improve efficiency, as studied, and providing information or decision support at the time the provider needs it. This in-time availability helps the handheld device interventions fit more seamlessly into the workflow. Although there are many hardware limitations such as battery life, screen real estate, and connectivity if the application relies on a wireless source of data, the ability for a provider to access it anywhere helps overcome the common workflow barrier of DSS available at the right place and the right time.
Discussion
Limitations
We focused our review on finding research articles that examined the use of mobile devices for activities such as decision support in the ED. As such, we did not find many eligible articles. While we do think it is important to report development of software, case reports, and displaying images on mobile devices, this was not the focus of our scoping review. We used “evaluation” as a broad term and kept that in mind while assessing articles for inclusion. The evaluation component was needed only to examine the implementation and use of the application or device as more than just a future plan or comment. We focused our review on the ED to show the need for further research. We had hoped to find more eligible studies, but it is certainly interesting to have found so few to show such a great need for additional research in this growing field.
Personal devices for healthcare
Smartphones are becoming more popular. An increasing number of providers are likely to be carrying their own personal device. Applications are currently available for providers and patients that provide medical reference information. It is likely that providers will prefer to use their own devices rather than those provided by the institution. This concept also benefits the institution since the price and mobility of handheld devices could become a burden. With this increasing trend toward personal use, more research is needed to help ensure that providers are able to provide the highest-quality and most reliable patient care and that personal devices maintain the safety and security standards that should be imposed on all devices containing personal health information.
New technology
Handheld devices are being used in new ways to help improve patient care. In the ED, Apple iPads have been used for child-life activities 23 as well as viewing radiology images. 24 While the latter was excluded from this review, the high-resolution screens provide a novel, portable, and convenient way to view these images. At this time, there is no literature on using them directly for decision support and clinical care in the ED.
Security
The security of handheld devices should also be considered when evaluating the new technology. Safeguards must exist to protect a potential breach of patient data. According to the National Information Technology Laboratory, there is a need to ensure that hardware, software, and firmware are designed and behave in a way that together they provide critical security functions. In addition to this, there is a need to have organizational policies that enable processing, management, and maintenance of mobile devices. Last, there is a need for “an application programming interface that allows operating systems and applications to use security functions.” 25
Future research directions
In a systematic review of the clinical decision-making literature, the authors found a dearth of literature relating to mobile devices by healthcare professionals. 26 Although the study was limited to randomized controlled trials, regardless, our review supports this scarcity without this limitation but still in a specialized area.
Given the provider’s desire for handheld devices and the prevalence of them throughout society, it is inevitable that more decision support, charting, and other informatics activities will be performed on handheld devices and not just on desktop computers. These developments have the potential to improve the quality and timeliness of care but should be thoroughly evaluated. As with any DSS, careful design and implementation should be undertaken to ensure that the systems produce the desired outcomes. Issues such as accessibility, human factors, patient privacy, and all others need to be explored in the realm of mobile devices.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.