
Abstract
Introduction
Blunt cerebrovascular injuries (BCVIs) are uncommon but associated with ischemic stroke and disability, particularly in younger adults. There is a paucity of literature on the incidence and risk factors for BCVI. The aim of this study was to report the incidence and clinical characteristics of patients diagnosed with BCVI at an adult level 1 trauma centre.
Methods
This was a registry-based cohort study. The accessible sample was all patients in the Alfred Hospital Trauma Registry (AHTR) who presented from January 2014 to June 2021 and were recorded to have BCVI. The diagnosis of BCVI was confirmed by independent, blinded neuroradiologists prior to study inclusion. Demographics, injury mechanism and associated injuries of patients were extracted from the AHTR and patient medical records.
Results
There were 20,954 blunt trauma patients in the AHTR during the study period, of which 300 patients were confirmed to have 428 BCVIs. The incidence of BCVI was 1.4% (95%CI: 1.3–1.6). The mortality rate was 14% with a median survival time of 86 h from the time of injury. More men (65%) were diagnosed with BCVI than women and motor vehicle crashes (n = 180; 60%) were the most common mechanism of injury. Younger age, high transfer mechanisms, high injury severity, brain and chest trauma were associated with carotid artery injuries, while vertebral artery injuries were associated with older age, higher presenting GCS and cervical spinal injuries.
Conclusion
The incidence of BCVI was low. The risk profile for patients with CAIs and VAIs were different. Consistent with the modified Denver criteria, high energy transfer mechanisms and cervical spinal injuries were identified to be high-risk features, but they impacted carotid and vertebral arteries differently. Any trauma involving these mechanisms should trigger investigation for the detection of BCVIs.
Introduction
Blunt cerebrovascular injury (BCVI) involving the carotid and/or vertebral arteries is thought to be secondary to stretching and shearing of the vessels during high-energy transfer. 1 BCVI is commonly associated with direct blows, hyperextension and/or rotation of the neck, facial injuries, base of skull (BOS) injuries and cervical spine injuries. 2
The incidence of BCVI is historically estimated to be low, around 0.24%–0.4%3–6 of major trauma admissions, and BCVI is therefore considered a rare complication of trauma. However, with increased awareness, advanced screening criteria and modern non-invasive imaging, the incidence of BCVI may be higher, with recent studies reporting the incidence at 1%–3%.7–16 Detecting BCVI is important, as it is associated with a high risk of ischemic stroke (IS) (reported 13%–26%), 17 high mortality (5%–40%)5,8,18,19 and worse long-term disability.6,20 Clinical examination to guide imaging is often limited in the setting of multi-trauma, particularly for patients with traumatic brain injury (TBI).
Different screening criteria have been developed to improve detection of BCVI, based on the mechanism of injury and high-risk symptoms.2–4,10,21–23 However, up to 20% of proven BCVI patients do not satisfy these criteria.20,24 Improved CT angiography techniques have increased the detection of BCVI, but routine use needs to be balanced against over-triage and unnecessary radiation exposure.
The objective of this study was to quantify the incidence and patient characteristics of adult trauma patients presenting to a Level 1 trauma centre with BCVI. Changes were made to the screening criteria during this time and were considered during analysis.
Methods
This was a single centre, retrospective, cohort study of all adult major trauma patients admitted to the Alfred hospital, an adult Level 1 trauma centre, one of the largest in the country that admits over 4700 patients annually. The study was reviewed and approved by the Alfred Hospital Human Research and Ethics Committee (IRB) (Project no. 445/19). The requirement to seek informed consent was waived.
All adult patients (age ≥18 years) registered in the Alfred Hospital Trauma Registry (AHTR) from 01 January 2014 to 30 June 2021 (‘study period’) were eligible for inclusion. The AHTR prospectively records pre-hospital and hospital data to chronicle trauma details. Criteria for inclusion in the registry include all major trauma (Injury Severity Score (ISS) > 12) admissions, those requiring admission for over 72 h, all trauma ICU admissions and all deaths after injury. Patients diagnosed with BCVI based on initial or subsequent vascular imaging were identified. Patients with injuries secondary to penetrating trauma were excluded.
From January 2014 to June 2016, the modified Denver screening criteria for BCVI was available to clinicians to screen trauma patients for further investigation with arch to vertex CT angiography. In 2016, the Alfred BCVI criteria were developed based on modified Denver criteria and included patients with 1st and 2nd rib fractures and sternal fractures. It was proposed that all patients who satisfied at least one of the Alfred BCVI criteria could undergo a CT angiogram of neck and intracranial vessels to assess for BCVI.
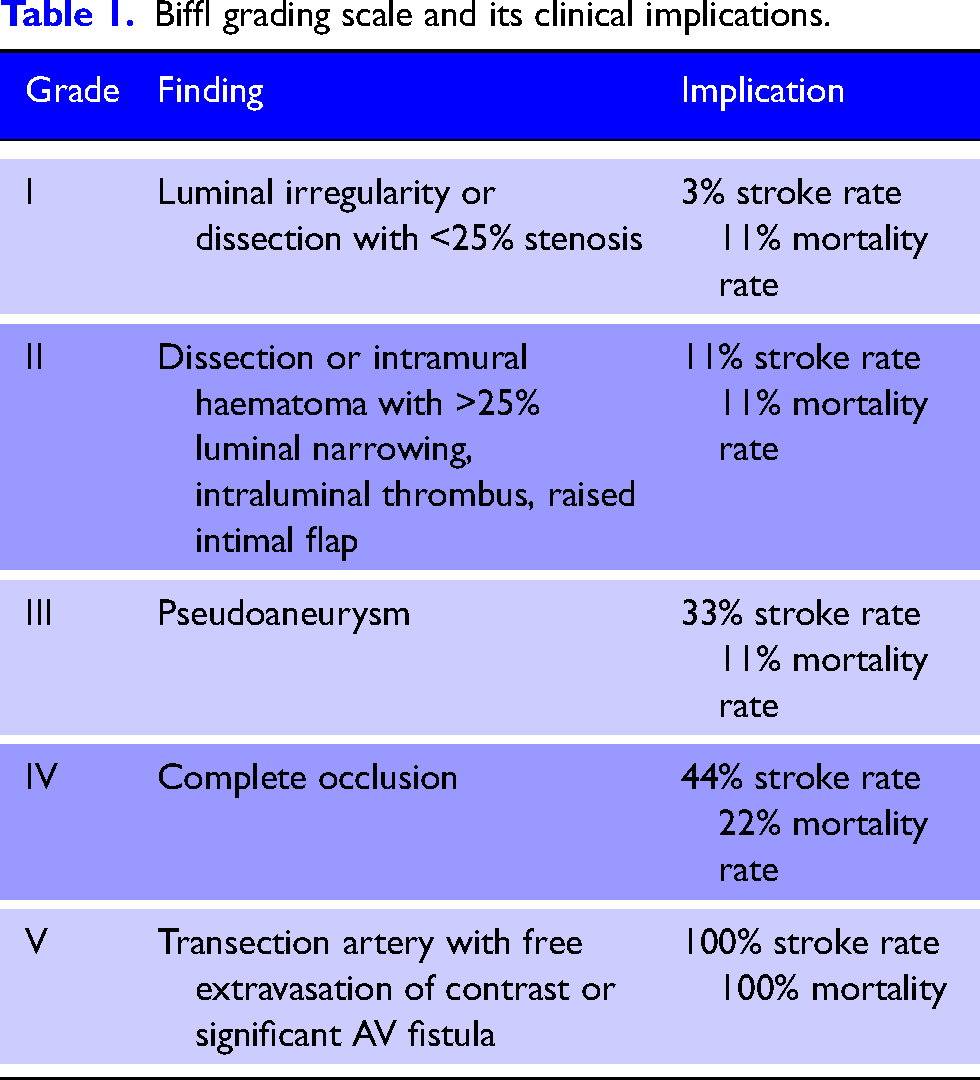
Prior to study inclusion, images of all patients recorded to have BCVI were re-reviewed and the diagnosis was confirmed by an independent specialist neuroradiology fellow, who was blinded to the original report. Where there was a disagreement, a consultant neuroradiologist provided the final adjudication. All vessel walls imaging including CT angiogram, magnetic resonance (MR) angiogram or digital subtraction angiography (DSA) were accepted. The severity of vessel injuries was classified by neuroradiologists according to the Biffl grading scale (Table 1). 21
Biffl grading scale and its clinical implications.
If the initial imaging was done externally and reported as BCVI, this was confirmed on the first follow up imaging performed on site within 3 days. Records in which the follow up imaging was not performed within 3 days were excluded, even if the original scan reported BCVI.
Data extracted from the AHTR included patient demographics, the time points of injury, mechanism of injury, injury details, length of stay in the hospital, time to CT and, presenting vital signs. Major complications during hospital admission including length of ICU stay and death were also included. Further data were extracted for each patient using an explicit medical record review. Variables associated with risk of BCVI as per the Denver criteria and later our BCVI criteria, were collected. Focal neurological symptoms, evidence of acute intracranial haemorrhage (ICH) and ischemic stroke (IS) on initial CT imaging were also extracted.
BCVIs were classified based on affected vessel (common carotid, internal carotid or vertebral), side (left or right) and cranial location (intracranial or extracranial). BCVIs were further sub-grouped as carotid artery injuries (CAIs) and vertebral artery injuries (VAIs) to determine associations with demographic and injury characteristics.
The overall incidence of BCVI was calculated across different patient population. Population-based incidence rates (95% confidence intervals (CIs)) were also calculated for each 6-month period based on the total population of blunt trauma patients at each time interval. A Poisson regression model was used to test for a change in increasing incidence. The incidence rate ratio (IRR) and 95% CIs were calculated. A p-value of <0.05 was considered statistically significant.
Results
During the study period of 6.5 years, there were a total of 23,775 major trauma presentations recorded in the AHTR, out of which 20,954 were due to blunt trauma. After removing initial coding errors, there were 360 patients found to have reported BCVIs on initial imaging. Following independent review by neuroradiologists, 300 patients were confirmed to have 428 BCVIs, with an institutional BCVI incidence of 1.4% (95%CI: 1.3–1.6, Figure 1). The overall incidence of BCVI, in each 6-month period, is displayed in Figure 2. The mean 6-monthly incidence of BCVI from January 2014 to June 2016 was 0.68 and from July 2016 to June 2021 was 1.33. However, this difference was not statistically significant (IRR 1.06; 95% CI: 0.95–1.19; p = 0.30).
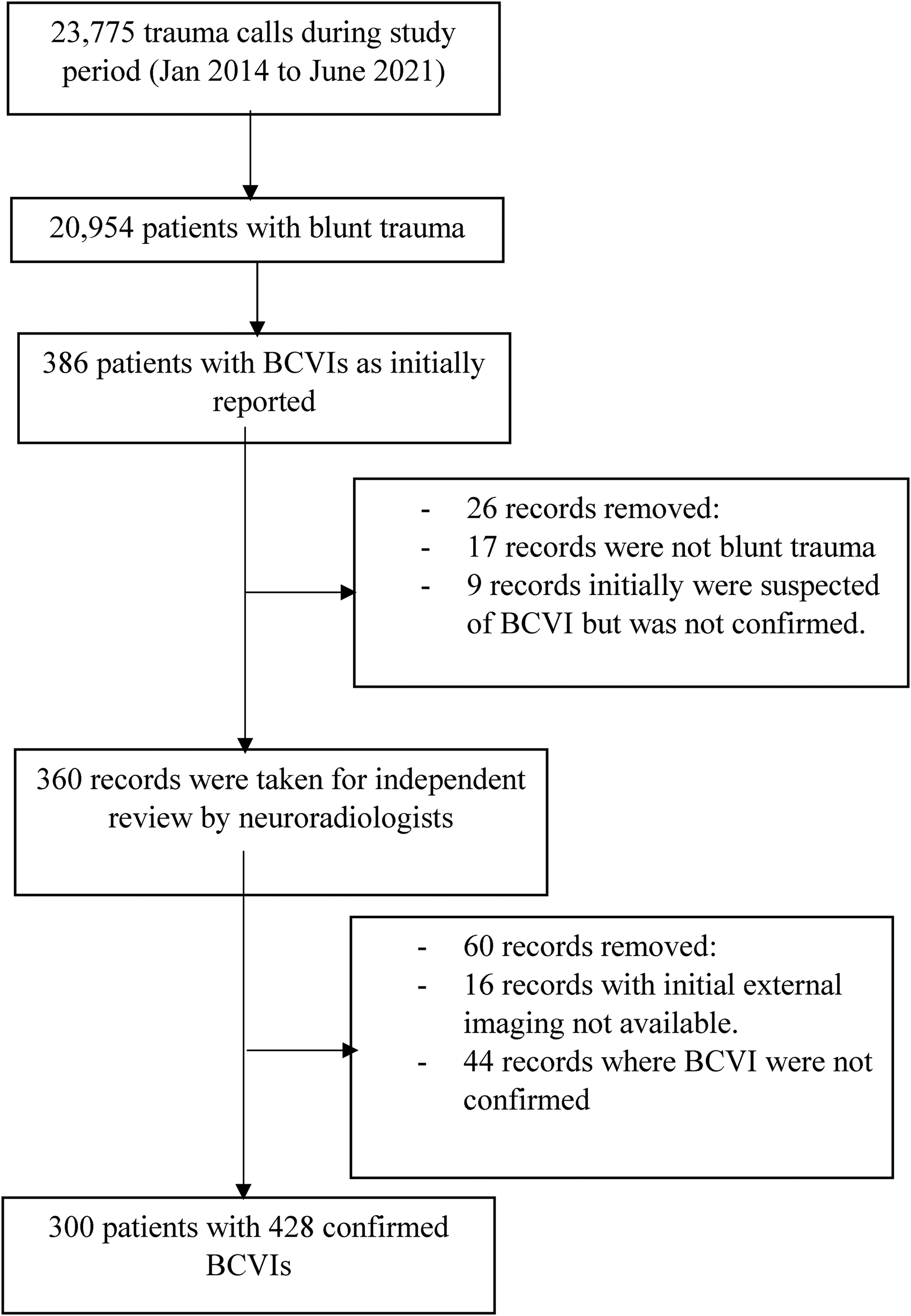
Flowchart demonstrating data collection and exclusion process.
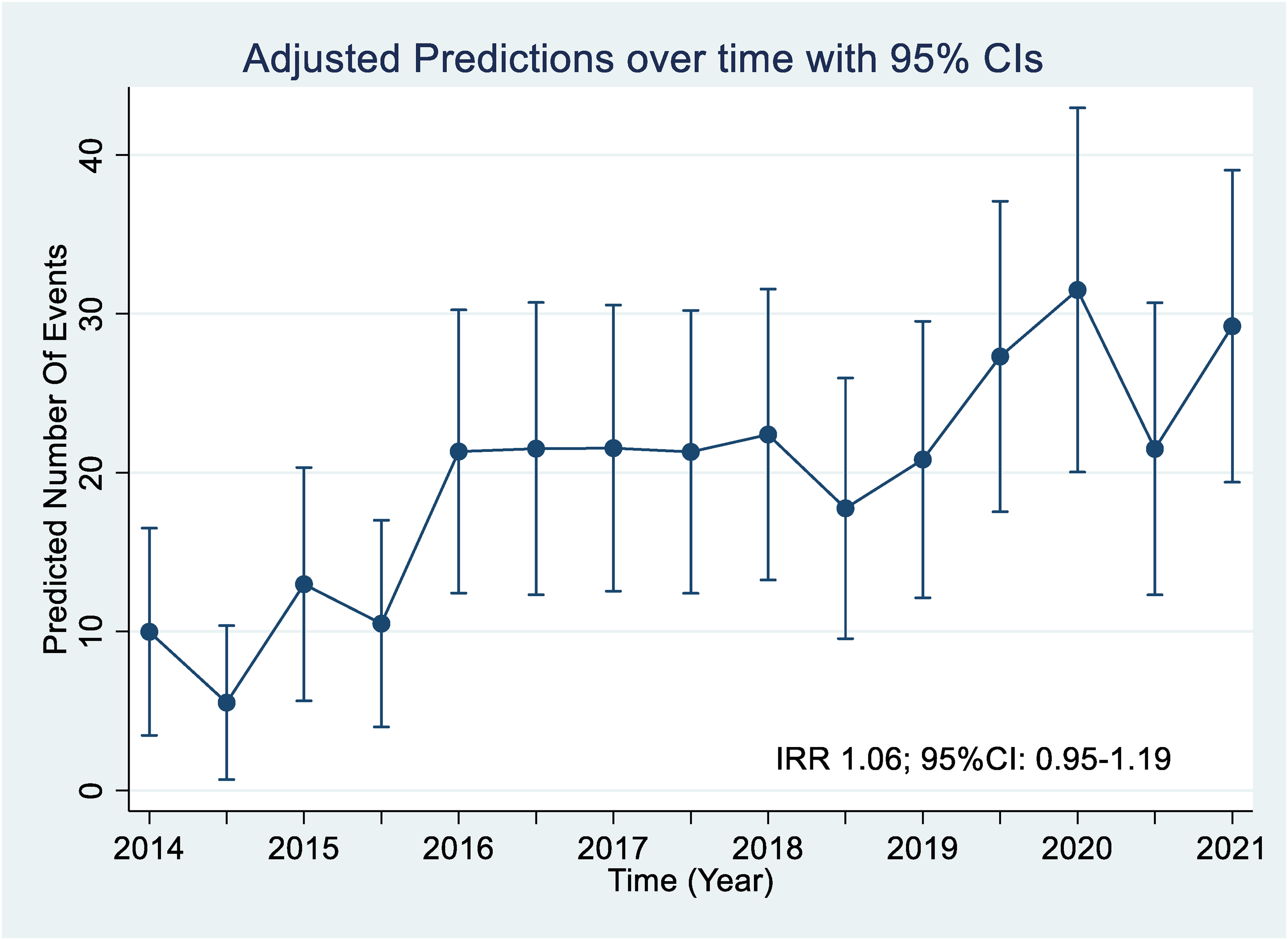
Incidence calculated for every 6 months during study period, with adjusted predictions with 95% confidence intervals (CIs).
Baseline demographics of the patients are listed in Table 2. Patients who sustained a BCVI had a median age of 50 (32–65) years; there were 194 men and 106 women. Forty-three patients (14%) died during admission, with a median interval of 86 (IQR 36–155) hours from the time of injury. The initial CT brain on arrival showed evidence of acute IS in 13 patients (4%) and intra-axial haemorrhage in 43 patients (14%). Eighty-seven patients (29%) had a Glasgow Coma Score (GCS) ≤ 8 on presentation and 94 (31%) patients had TBI, which included intra- and extra-axial haematomas. Six patients with IS (46%) and 16 patients with ICH (37%) were among those who died.
Baseline demographics of all BCVI patients.
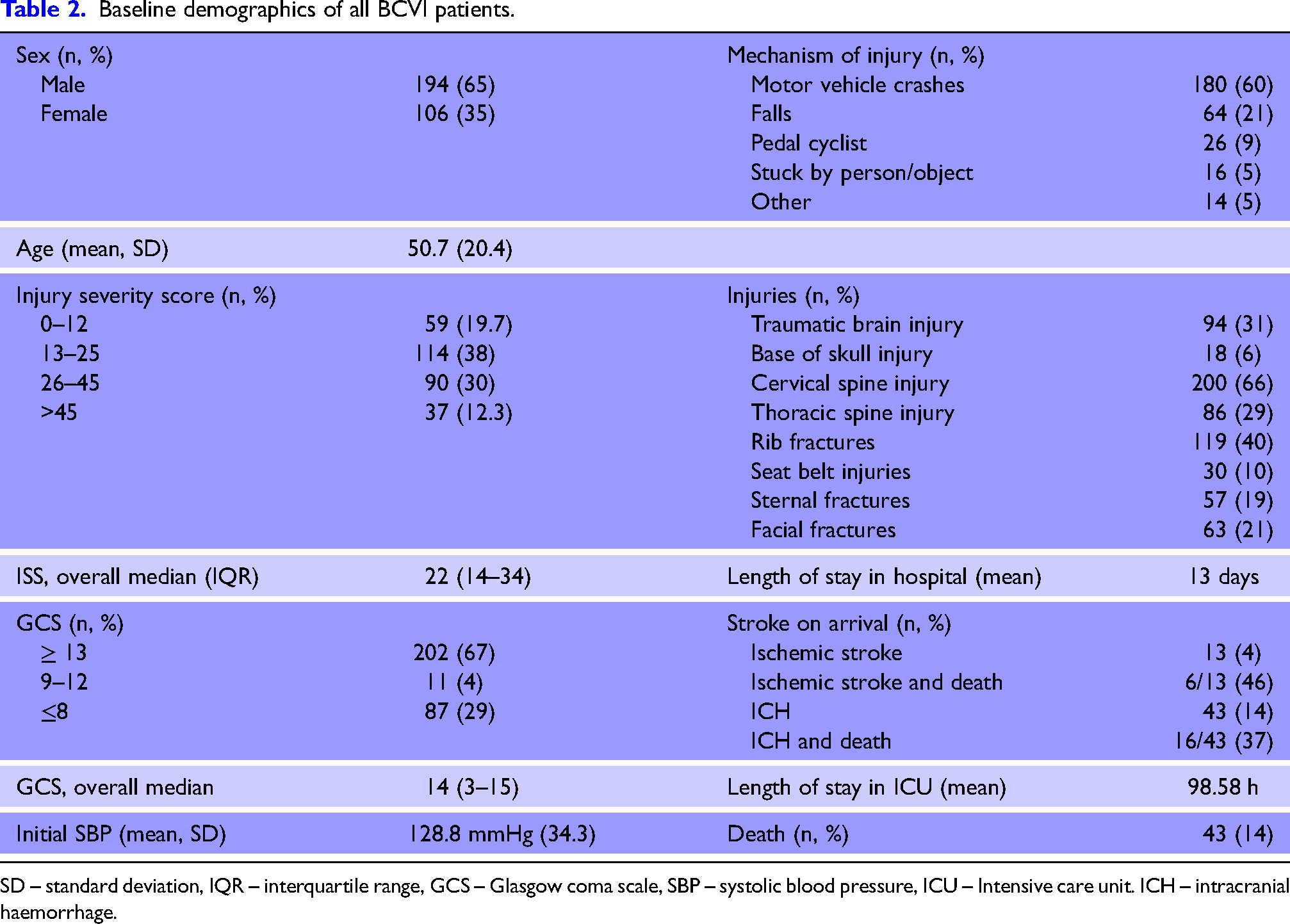
SD – standard deviation, IQR – interquartile range, GCS – Glasgow coma scale, SBP – systolic blood pressure, ICU – Intensive care unit. ICH – intracranial haemorrhage.
Motor vehicle crashes (MVC) were the most common cause of injury, occurred in 180 patients (60%), out of whom 120 (67%) were drivers/riders, 42 (23%) were passengers and 18 (10%) were pedestrians. Falls were the second most common mechanism and occurred in 64 (21%) patients. There were 26 (9%) cases related to pedal cyclists, 16 (5%) were struck by or had a collision with an object or person, and 14 patients (5%) had other external injuries.
Cervical spine injuries and rib fractures were the most frequently associated injuries, being present in 200 patients (60%) and 119 patients (40%) respectively. Thoracic spine injuries were the next most common, seen in 86 (29%) patients. Base of skull fractures were seen in 18 patients (6%), sternal fractures in 57 patients (19%), craniofacial fractures in 63 patients (21%) and seatbelt bruising in 30 patients (10%).
The number of BCVIs in each vessel studied is listed in Figure 3. There were 428 BCVIs in total of which 373 were extracranial injuries. Intracranial injuries were less common and accounted for 24 CAIs and 31 VAIs. There were 13 injuries to common carotid arteries.
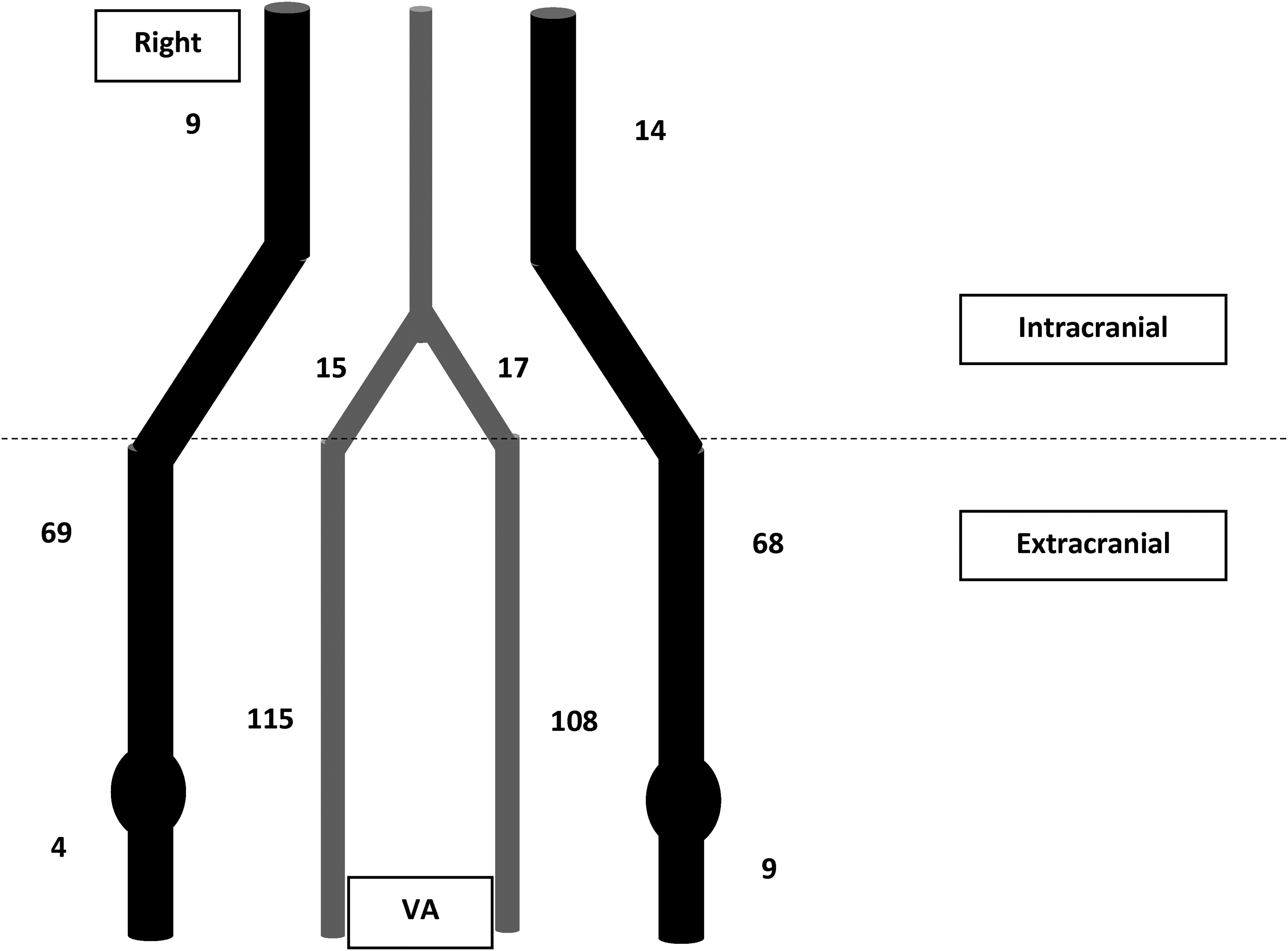
Number of BCVIs according to anatomical location.
Vessel injuries were classified according to their grades and grouped as CAIs and VAIs in Table 3. VAIs were the most common with 255 injuries (60%) while there were 173 CAIs (40%). Among CAIs, the median grade was 2 (IQR 2–2), while the median grade for VAI was 3 (IQR 2–4). Ninety-four vessel injuries were Biffl grade I minor injuries. There were 165 BCVIs with grade II, 23 with grade III, 144 with grade IV and 2 with grade V. For every grade, the number of BCVIs were similar between CAIs and VAIs except for Grade IV where there were 124 VAIs but only 20 CAIs.
BCVI severity is graded according to Biffl scale and grouped respective to the vessels.
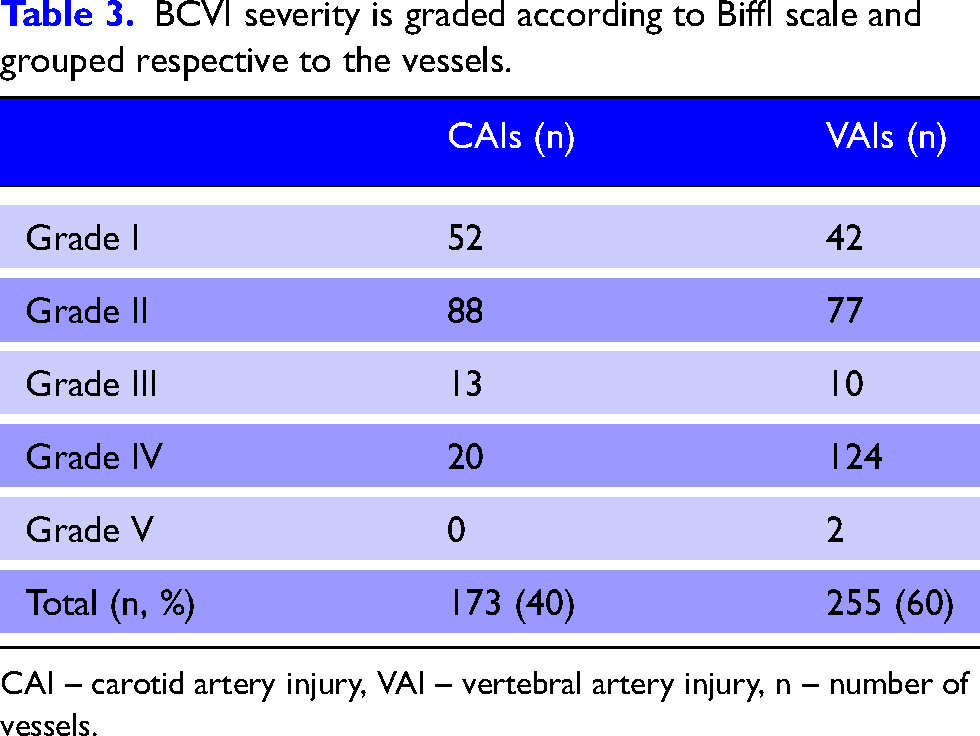
CAI – carotid artery injury, VAI – vertebral artery injury, n – number of vessels.
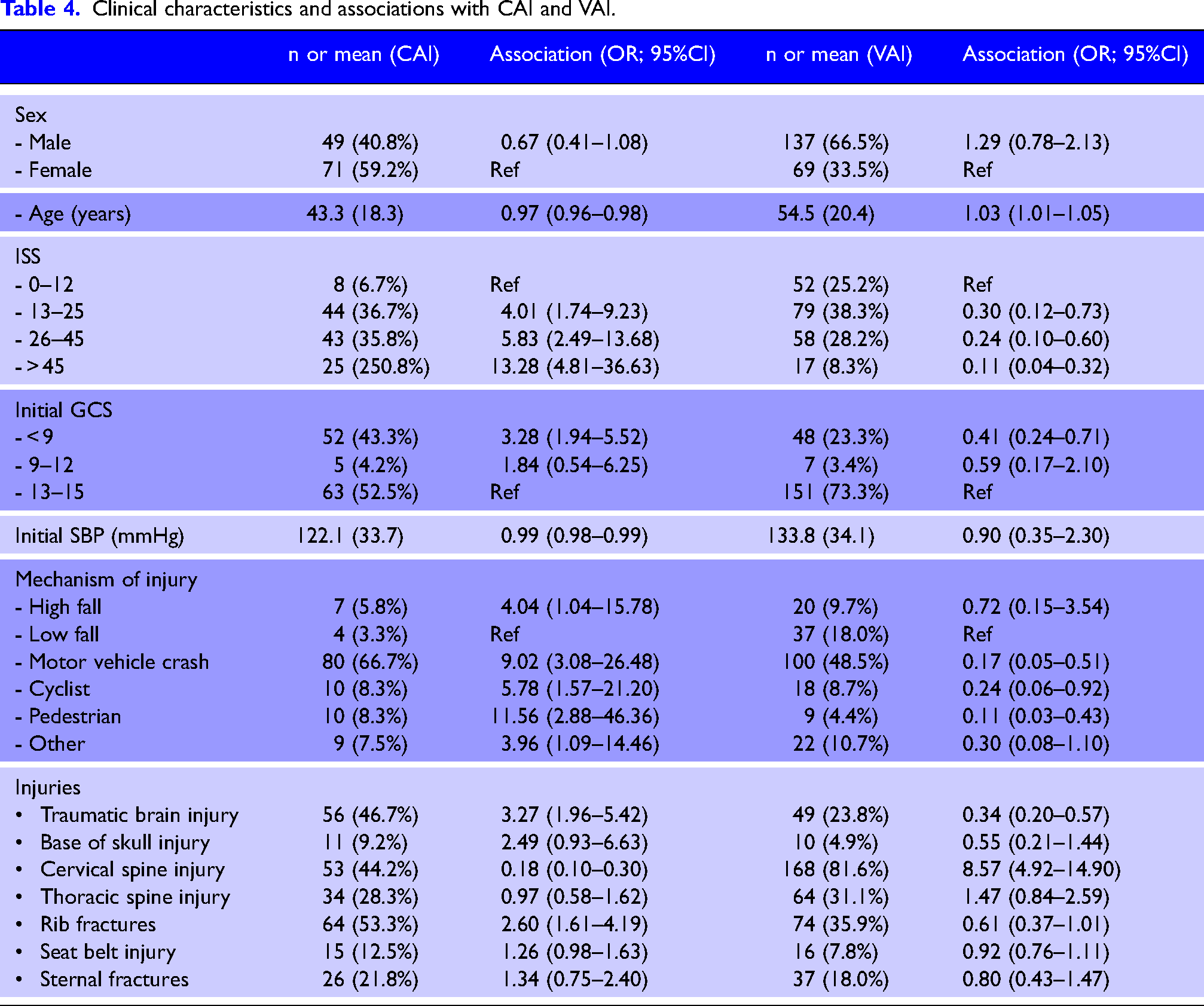
The association between clinical characteristics and BCVIs are listed in Table 4. There was no association with sex for either CAI or VAI. CAIs were associated with younger age (OR 0.97, CI 0.96–0.98), higher injury severity with lower GCS and lower initial systolic blood pressure. Mechanisms of injury among patients with CAI were more commonly after high energy mechanisms of motor vehicle crashes, high falls and cyclist crashes. TBI and rib-fractures were more commonly associated with CAIs. VAIs were associated with older age (OR 1.03; 95%CI: 1.01–1.05), and more frequently observed among patients with low injury severity and high GCS. VAIs were also more frequently present after low falls and associated with cervical spine injury.
Clinical characteristics and associations with CAI and VAI.
Discussion
Our cohort study of 300 BCVI patients with 428 vessel injuries collected over 6.5 years, represents one of the largest, single-centre, contemporary data on the incidence of BCVI in adult patients and provides an estimation of the incidence of BCVI after changes in screening processes. The incidence of BCVI diagnosed in our study was similar to previous reports. A similar study, published by Cothren et al. with a cohort of 301 adult BCVI patients with 422 BCVIs, collected between 1997 to 2007, reported similar incidence (1.6%) to our study. 25 More recently, Wu et al. from Seattle, USA published a retrospective cohort collected between 2005 and 2015, reported 1604 BCVIs on 1204 adult and paediatric patients and an incidence rate of 2.5%. 26 Wagenaar et al. from Denver, USA also published data from 582 patients with 829 BCVIs, collected over 16 years (1997 to 2013), however, the total number of blunt trauma patients was not reported in their study and hence the incidence is not known. 27
The current incidence of BCVI reported in this study was higher than previously reported from our centre (1.4% vs 0.69%) while the mortality rate was lower than before (14% vs 20%).18,28 This increase in incidence rate is likely due to increased awareness of BCVI over time, the development of more well-defined screening criteria and the advances in modern non-invasive imaging. While the increased detection rate of lesser severity BCVI may have contributed to the reduction seen in BVCI-associated mortality, increasing safety regulations and restraints introduced in the motor vehicle industry, particularly with speed limits and advanced safety technology may have aided as well.
Our study demonstrates that among patients with BCVIs, the clinical characteristics of patients with CAIs and VAIs were quite different. CAIs were most commonly observed in the setting of major trauma after high energy transfer mechanisms such as MVCs, high falls and trauma with high ISS. In contrast, VAIs were more commonly associated with older age, male gender, high GCS, low impact trauma such as low falls and trauma with low ISS. Associated injuries were also different between CAIs and VAIs. CAIs were more often seen with TBIs and chest injuries while VAIs were often associated with spine injuries. These results are quite interesting as BCVIs are traditionally seen as a complication of trauma involving high-velocity mechanism yet our data shows that this is not always the case, especially with VAIs.
Results of this study reaffirm that any screening criteria used to detect BCVIs should be adequate to cover as many risk factors as possible. As noted, the risk factors between CAIs and VAIs were very different for our patient group. A large portion of BCVI patients did not exhibit high-risk clinical characteristics, for example, 34% of patients did not have cervical spine fractures. Moreover, nearly 30% of our population were either asymptomatic or unexaminable (GCS ≤ 8). Having an effective screening criteria is, thus essential in order to optimise the detection of BCVIs and to identify patients at high risk of complications such as stroke whilst avoiding unnecessary radiation exposure. Modification of the existing modified Denver screening criteria, at the level of individual institutions, should be considered in order to address any specific characteristics of the local trauma patient population24,26,29 and to accommodate new developments in BCVI management. Our current screening criteria, with the inclusion of additional parameters into modified Denver criteria including sternal and rib fractures, showed numerically increased BCVI identification in our cohort, suggesting their inclusion in routine screening criteria is required to prevent under-diagnosis. The increase was not statistically significant, however, possibly due to the small sample size.
Within BCVIs, VAIs (255/428) were more commonly found to have higher Biffl grade injuries than CAIs (173/428), mainly accounted by the difference in Grade IV injuries (124/255 vs 20/173). This reflects the anatomical location of the vessels in relation to the blunt trauma and the transfer mechanism of high energy during trauma The VA at the skull base is particularly vulnerable to injury as it has a reduction in vessel wall thickness at this point. 30 In fact, cervical spine injuries were more commonly associated with VAIs than CAIs. Pre-existing, asymptomatic occlusion of vertebral arteries due to atherosclerosis could explain the difference in Grade IV injuries, however, longstanding atherosclerotic disease is more commonly seen in the elderly population with multiple cardiovascular risk factors. Our study population was predominantly young and likely with less cardiovascular risk factors as a group, making chronic atheromatic occlusion less likely. Similarly, Grade II injuries were seen more commonly than Grade I injuries. This could, at least partly be due to technical difference between imaging modalities. While Grade I can be clearly characterised using digital angiography, it can be challenging to visualise in other modalities.
Our study has a few limitations. Being a single-centre, retrospective study, our data relied on accurate medical records, and can be limited by inadequate documentation such as absence of potential confounding factors. Thus, the true overall incidence of BCVI is likely to be underestimated in this study. Although one of the largest studies, our sample size was not large enough to reliably conclude on risk factors for BCVI. Moreover, we did not have the data from the non-BCVI population during the same time to analyse outcome associations. It should be also noted that Biffl grading is validated only on DSA not in CTA. However, in our study, in line with similar, previously published studies, any vascular imaging available was used to grade vessel injuries.
Conclusion
A total of 428 BCVIs were diagnosed in 300 patients over a recent 6.5-year period with a steady yearly incidence. While CAIs were found to be associated with more severe trauma and high energy transfer mechanisms, VAIs were observed in low-impact injuries and associated with spinal fractures. VAIs were more common and more severely injured than the carotid arteries. Guidelines that promote liberal imaging and a high degree of clinical gestalt remain essential for early diagnosis of BCVI. Further work is required to identify BCVI patients at high risk of complications, including stroke and inform interventional study design to improve outcomes in this cohort.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Previous presentation
An abstract of this work was presented at the World Stroke Congress meeting in 2022.
Ethical approval
Ethics approval for this study was obtained from The Alfred Hospital Human Research and Ethics Committee (Approval no. 445/19).
Informed consent
Not applicable.
Trial registration
Not applicable.
Author contributions
GC, MF, JM, BM and AM devised the study and design. WZ, VS, TR and NN collected and organised the data. AM and BP analysed and reported the neuroimages as blind assessors. VS wrote the initial draft of the manuscript and all the authors edited the manuscript. BM assisted with the statistical analysis. The final version of the manuscript has been read and approved by all authors.
Acknowledgements
None.