
Abstract
Triage is a key principle in the effective management of major incidents and has traditionally been performed using an assessment of a casualty's physiology. However, it has become apparent from recent experiences of major incidents that physiological triage may practically not be possible, especially in the early stages of an incident. A key factor is the speed with which it is possible to perform triage, and subsequently, the speed at which key life-saving interventions (e.g., management of external haemorrhage and airway opening manoeuvres) are able to be performed simultaneously as part of the triage process. Addressing this issue was a priority for the review of major incident triage undertaken by NHS England and culminated in the development of the Ten Second Triage (TST) tool.
Triage is a key principle in the effective management of major incidents and is the process by which casualties are prioritised on the basis of their clinical acuity and need for life-saving interventions. 1 Historically, the triage process has been conducted using an assessment of the casualty's physiology and within the United Kingdom, a recent NHS England review of major incident triage culminated in the development of the new NHS Major Incident Triage Tool (MITT). 2
The introduction of the MITT represents the optimum method of triage based on physiological criteria at a major incident. However, it has become apparent from recent experiences of major incidents that in practice, the use of physiological triage may not be possible, especially in the early stages of an incident, where the casualties are likely to significantly outnumber responders. A key factor is the speed not only with which it is possible to perform triage, but subsequently, the speed at which key life-saving interventions, such as management of external haemorrhage and airway opening manoeuvres, are able to be performed simultaneously as part of the triage process. Furthermore, physiological triage can only realistically be performed by responders who have both the clinical training and equipment (if required e.g. Triage Sort) to do so. Additionally, the use of physiological assessments will add to the cognitive load of the provider on the scene, in what is likely to be an already incredibly stressful situation. The combination of these factors is likely to then compound the ‘care gap’, the term used to describe the period between an incident occurring and when emergency medical services (EMS) are on scene and able to provide casualty care; an issue which was specifically highlighted in the Manchester Arena Inquiry. 3 Addressing this issue became an additional priority for the NHS England review of major incident triage, culminating in the development of a quick and simple triage method, called the Ten Second Triage (TST) tool (Figure 1).
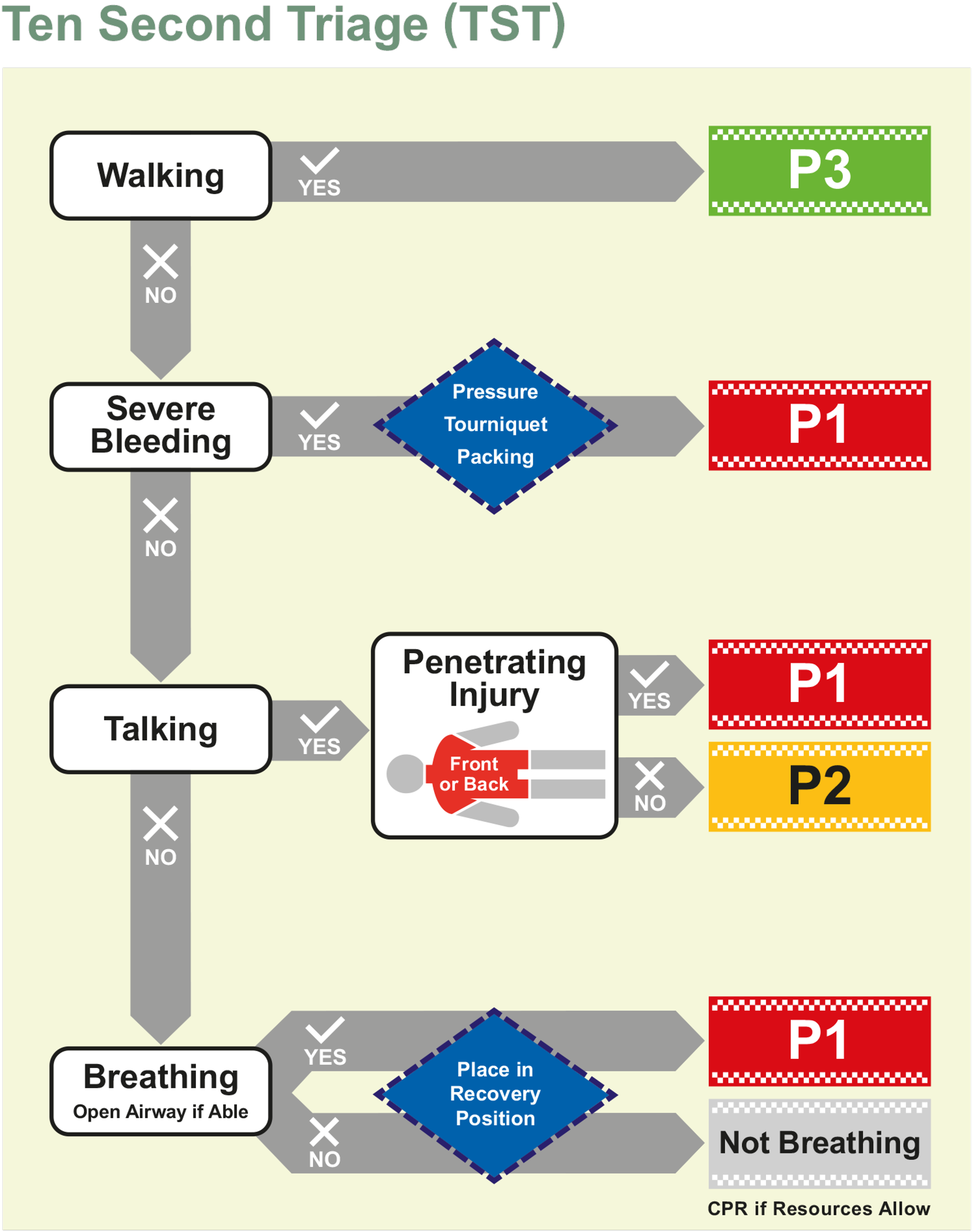
Ten Second Triage (TST) tool.
The development of the TST represents a collaborative approach incorporating academics and clinicians involved in pre-hospital care and major incident management from both the military and civilian sectors. Furthermore, it incorporated the extensive experience of responders involved in recent major incidents, from both Police and healthcare. The TST has subsequently been endorsed by NHS England, recommended to the Devolved Administrations and has been supported by both the National Fire Chiefs Council and National Police Chiefs Council. Thus, this is the first triage tool that can be used by first responders from all the emergency services and not just healthcare professionals.
This editorial provides an overview of the TST, describing its rationale ahead of its introduction into practice in Spring 2023.
Why physiology isn’t appropriate
There are several differences between the TST and existing major incident triage tools (including the MITT), the most notable of which is the lack of any formal physiological assessment. The use of a non-physiological initial triage tool has a number of key advantages. 2 The first is time to triage; even with responders experienced in triage, the use of the MITT still takes between 40 and 60 seconds to complete; by comparison, the TST takes approximately 10 seconds. 4 By reducing the time required to perform triage, we are able to deliver key life-saving interventions rapidly to a large number of casualties in the initial phase of a major incident, in order to optimise survivability. Lastly, by removing any arithmetic from the assessment, we reduce the cognitive burden on the triage provider. Instead of using actual physiological parameters, the TST follows a simple assessment of whether the casualty is walking, talking, breathing (but not talking), or not breathing in addition to looking for the presence of any central penetrating injury. These are all simple, surrogate end-organ assessments of cardiovascular status, with each category representing an increase in clinical acuity. The benefit of such a system is two-fold; the time taken to perform the triage process is rapid and additionally, it can be used by non-healthcare responders such as police and fire personnel. Increasing the availability and effectiveness of a triage system conveys huge benefits, as this begins to address the ‘care gap’. 3
Walking before bleeding
Major incident triage tools typically begin with the binary assessment of catastrophic haemorrhage 5 ; acknowledging that the distribution at an incident is typically skewed to the walking wounded, 6 the TST begins with ‘walking’ prior to the assessment of ‘severe bleeding’. This enables responders to rapidly deprioritise a large volume of casualties, allowing for efforts to focus on non-ambulant casualties.
The nomenclature has been changed in order to make it more accessible to those with limited clinical training; instead of ‘catastrophic’ bleeding, the terminology used is simply ‘severe’ bleeding. Very few ambulant casualties are expected to have severe external bleeding and be at risk of imminent clinical deterioration. The TST education package provides training in order to recognise and intervene in this small subset.
Life-saving interventions
The purpose of the TST is to rapidly triage casualties and simultaneously deliver basic life-saving interventions associated with improved survivability in the early injury phase (external haemorrhage control and airway opening). 7 The TST advocates basic measures to address external haemorrhage and for airway opening, no adjuncts are specifically described; the instruction is simply to open the airway as able, and to place the casualty in the recovery position. The rationale for this is speed and to increase applicability to be used by all responders.
Penetrating torso injury
A novel step in the TST is the assessment and prioritisation of non-ambulant casualties with penetrating torso trauma, who are not only at risk of rapid deterioration, but of non-compressible haemorrhage which may require urgent definitive care.8,9 A casualty diagram with the torso area shaded red, specifically including the junctional body areas at risk of significant haemorrhage together with the words ‘Front and Back’ is included. A non-ambulant talking casualty, with no severe external bleeding, but whom has a penetrating torso injury will be categorised as Priority 1.
Not breathing versus dead
Unlike classic triage tools, the TST categorises the apnoeic patient as ‘not breathing’ with a silver colour. The rationale for this is twofold; firstly, to allow non-healthcare responders to use the TST without the legal challenge of categorising casualties as dead. Secondly, salvageability, either in those in cardiac arrest, for example, from a crush injury or myocardial infarction, where resuscitation if resources allow may be appropriate, or in the event a casualty has a particularly slow (or shallow) respiratory rate that is not recognised, they will still receive the same life-saving intervention as a ‘breathing’ casualty (being placed in the recovery position).
Casualties will only be labelled as ‘Dead’ when sufficient healthcare resources are available to allow for the appropriate clinical consideration. This allows for formal declaration of death after a further assessment and consideration of any treatment options, thereby supporting families, responders, and subsequent legal enquiries.
Interaction with MITT
The TST will be the triage assessment employed by EMS and non-EMS responders initially attending a major incident, which will then be followed by a more detailed assessment (e.g., using the MITT) as and when sufficient EMS resources allow. From experience during simulated major incident training, time taken to triage using the MITT reduces by over 50% when it is used following the application of the TST.
Conclusion
Whilst the key principles of major incident triage are that it needs to be rapid, reliable and reproducible irrespective of whoever is performing it, it must also go further and allow for the delivery of timely life-saving interventions in order to optimise survivability of salvageable casualties. 7 The TST fulfils all of these principles and represents a significant change from traditional major incident triage tools in that it doesn’t include any formal physiological assessment. By adopting this approach, we have developed a triage tool that allows for a far quicker triage assessment and reduces the time to delivery of life-saving interventions across a large number of casualties. Additionally, the removal of physiological assessments increases its utility for all responders, creating a common triage language, enhancing interoperability and improving shared situational awareness. This helps to address the ‘care gap’ with the ultimate goal of reducing both morbidity and mortality associated with major incidents.
Footnotes
Author contributions
JV, PC, CP, SH, DB and JES designed the TST as part of a Triage Task and Finish group led by CM. JV wrote the initial draft of the manuscript which was updated following PC and JES review. Critical revisions were provided to the manuscript by CP, SH, DB and CM. CP and SH specifically provided significant revisions to the ‘why physiology isn’t appropriate’ and ‘penetrating torso’ sections. CM provided specific revisions with regard to the care gap concept, linking in with the Manchester Arena Inquiry and the areas relating to NHS England.
Declaration of conflicting interests
The author(s) declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JV, CP, JES are serving members of HM Armed Forces.
Funding
The author(s) declared receipt of the following financial support for the research, authorship, and/or publication of this article: Post-acceptance funding was provided by NHS England to enable the article to be published as Open Access.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Trial registration
Not applicable.
Acknowledgements
None.