
Abstract
Introduction
Analgesia is key to successful conservative, nonsurgical management of patients admitted to the hospital with multiple rib fractures. Recently, new fascial plane regional anesthesia techniques have become widely available. We hypothesized that since the introduction of these new regional analgesia techniques, for patients over the age of 65 years, the effect of increasing numbers of rib fractures has been mitigated.
Methods
A retrospective study of patients admitted for the management of rib fractures between 2017 and 2020 was performed. Patients not admitted to the hospital, under the age of 65 years, or with chest trauma other than rib fractures were not eligible for inclusion. The primary outcome of interest was mortality. The secondary outcomes were the incidence of pneumonia and intensive care unit admission. Results were reported as the odds ratio and its 95% confidence interval and associated p-value. Statistical significance was set at
Results
Overall, 252 patients were included and 142 patients received a regional anesthesia. The mortality rate was 4% (n = 10) with no association between mortality and number of rib fractures (p = 0.215). Twenty-four patients (9.5%) developed pneumonia during their hospital stay, again with no association with an increasing number of rib fractures. The intensive care unit admission rate was 13.1
Conclusion
Management including liberal utilization of regional anesthesia for at-risk patients appears to mitigate the effect of increasing numbers of rib fractures on the incidence of mortality and pneumonia.
Introduction
Compared with younger patients, patients over the age of 65 years are twice as likely to die when admitted to the hospital with multiple rib fractures.1,2 Regardless of age, there is a strong correlation between an increasing number of rib fractures and mortality. 3 For patients over the age of 65 years, with four or more fractured ribs, the mortality rate is 34–38%.1,2 The primary cause of rib fracture-related morbidity and mortality is the associated respiratory complications, 4 which occur due to pain-related impairment of deep inspiration, as well as opioid-induced sedation and respiratory depression. 5
Recently, there has been a surge of literature demonstrating the benefits of surgical rib fixation on rib fracture-related morbidity and mortality, 6 although in many centers, this is not a common management technique for rib fractures, with a greater dependence on nonsurgical, conservative management strategies. When managing rib fractures nonsurgically, the key to prevent morbidity and mortality is the provision of high-quality analgesia and chest physiotherapy. 2 The best conservative analgesia for rib fractures involves the provision of neuraxial or regional anesthesia, in combination with other multimodal therapies.7–9 Unfortunately, the older populations have often been precluded from having thoracic epidural (TE) or paravertebral block (PVB) analgesia due to the frequent occurrence of contraindications, 10 leading to a higher reliance on opioid-based analgesia and associated respiratory complications.
In recent years, there have been significant advancements in the field of regional anesthesia. Fascial plane blocks such as the erector spinae plane (ESP) have been shown to be highly efficacious, safe blocks, even in the presence of contraindications to TE or PVB.11,12 These blocks are in superficial, compressible locations and based on a risk–benefit analysis can be utilized in patients with active infection or anticoagulation. 12 For this reason, the elderly population has particularly benefited from this new analgesic technique for rib fractures. 13 We hypothesized that since the introduction of these new regional analgesia techniques, for patients over the age of 65 years, the effect of increasing numbers of rib fractures has been mitigated. The primary aim of this study was to determine whether there is a correlation between an increasing number of rib fractures and mortality. The secondary aim was to determine whether there was a correlation between an increasing number of rib fractures with pneumonia and intensive care unit (ICU) admission.
Methods
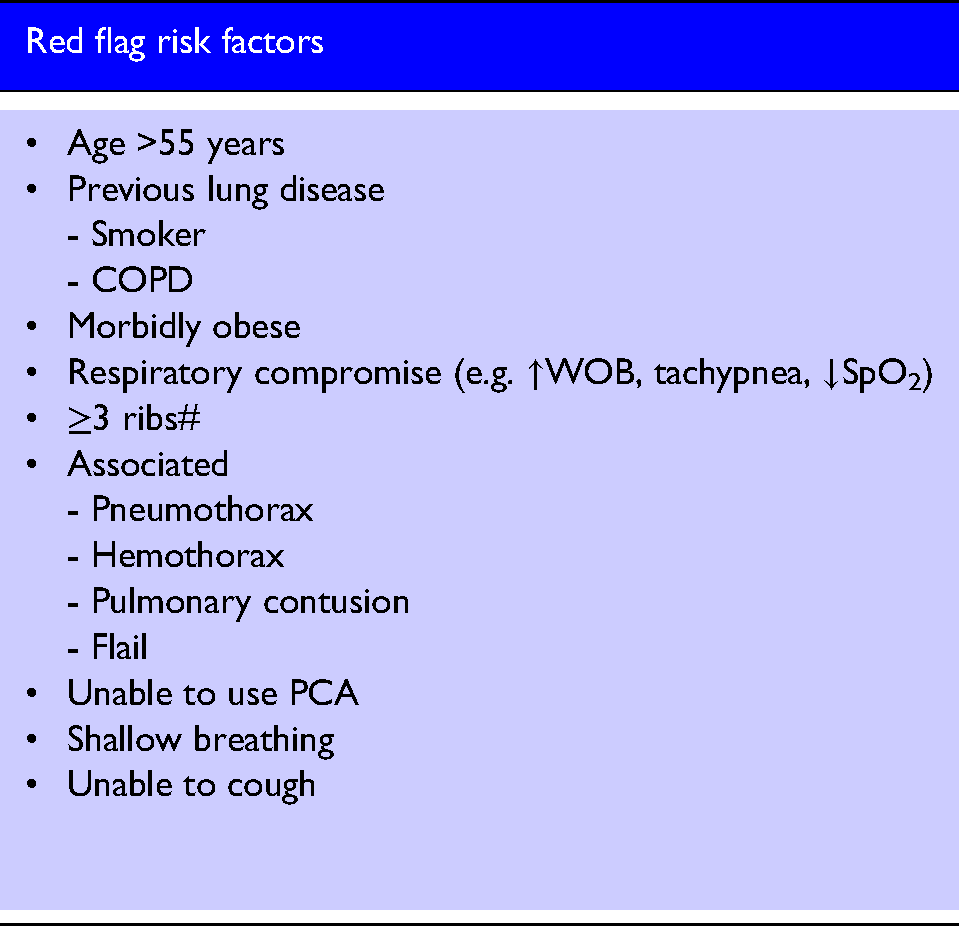
A retrospective study was performed with institutional review board (IRB) approval by The Prince Charles Human Research Ethics Committee (HREC: LNR/2018/QPCH/45155). Written informed patient consent was not required for this retrospective study as per the IRB. We analyzed electronic medical record data of patients aged 65 years and over, admitted for the management of rib fractures between February 2017 and September 2020. Patients not admitted to the hospital, under the age of 65 years, or with chest trauma other than rib fractures were not eligible for inclusion. Regional anesthesia was provided to patients according to red flag symptoms in our standardized blunt chest trauma algorithm (Box 1). Data collected included demographics, medical co-morbidities, mechanism of injury, injuries sustained, location of residence prior to admission, and utilization of regional anesthesia.
The primary outcome of interest was mortality. Mortality was defined as not surviving to discharge. The secondary outcomes were the incidence of pneumonia and ICU admission.
Data analysis was performed using Microsoft Excel 2016 (Microsoft Corp., Redmond, WA, USA) and STATATM (version 16.0) (StataCorp., College Station, Texas, USA). After checking for completeness, continuous data were assessed for normality using the Shapiro–Wilk test. Normally distributed data were summarized as mean (SD) with non-normal data either summarized as median (interquartile range (IQR)) or in the case of categorical or dichotomous data, number, and frequency (%). Binary comparisons were performed using a Student’s t-test with assumed unequal variance or Fisher’s exact test, where appropriate. Logistic regression was performed using mortality, ICU admission, or pneumonia as the outcome variables. Explanatory variables were selected on the basis of univariate significance with the final models constructed using a backward elimination technique. Results were reported as the odds ratio (OR) and its 95% confidence interval (95% CI) and associated p-value. Statistical significance was set at
Results
Overall, 252 patients were included in the final analysis. In total, 142 patients (56.3%) received a regional anesthesia technique, including 101 ESPs (Table 1). The mean age and number of rib fractures were 72.65 years (range: 65–95) and 5.4 (range: 1–18), respectively. The commonest mechanism of injury was a fall from less than 2m and comorbidities including obstructive sleep apnea, obstructive airway disease, ischemic heart disease, and a history of smoking were common.
Cohort baseline characteristics out of a cohort of 252 patients.
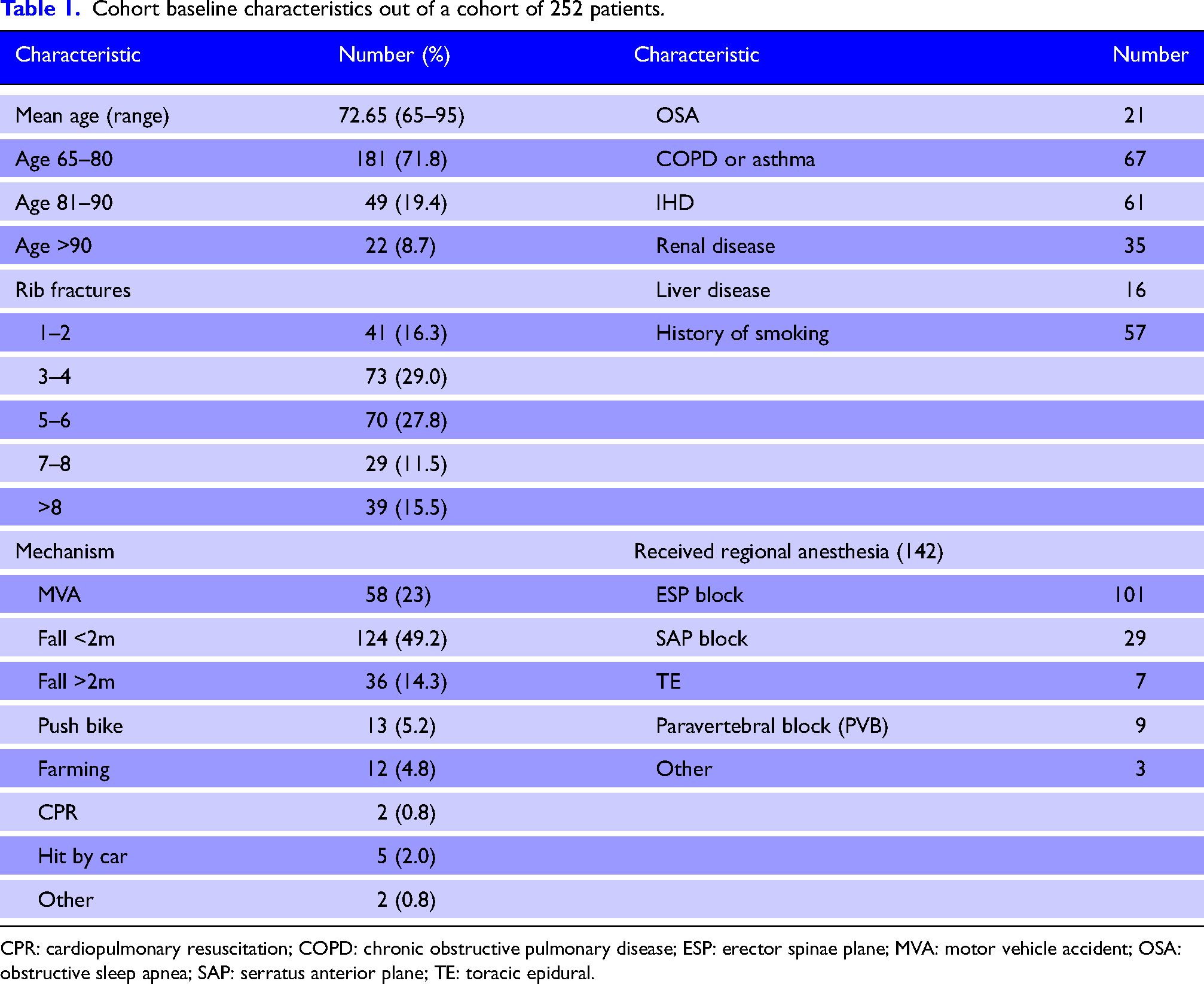
CPR: cardiopulmonary resuscitation; COPD: chronic obstructive pulmonary disease; ESP: erector spinae plane; MVA: motor vehicle accident; OSA: obstructive sleep apnea; SAP: serratus anterior plane; TE: toracic epidural.
There were 10 deaths in total with a mortality rate of 4%. On univariate analysis, there was no association between mortality and number of rib fractures (p = 0.215), the presence of pulmonary contusion (p = 0.107), pneumo/hemothorax (p = 0.332), or a chest drain (p = 0.451) (Table 2). Using logistic regression, independent predictors of mortality included pre-admission aged care residence (OR = 18.5; 95% CI = 3.6 to 95.2; p < 0.001), a past medical history of obstructive airway disease (OR = 6.3; 95% CI = 1.4 to 29.4; p = 0.19), the presence of a flail chest (OR = 5.1; 95% CI = 1.1 to 23.6; p = 0.036), and mechanism of injury (OR = 1.6; 95% CI = 1.1 to 2.5; p = 0.040). Although there was a higher incidence of mortality among patients who did not receive regional anesthesia (7/110; 6.4%) compared with those who did (3/142; 2.1%), this difference was not statistically significant (p = 0.083).
Patient characteristics by mortality given as number (%) unless otherwise stated.
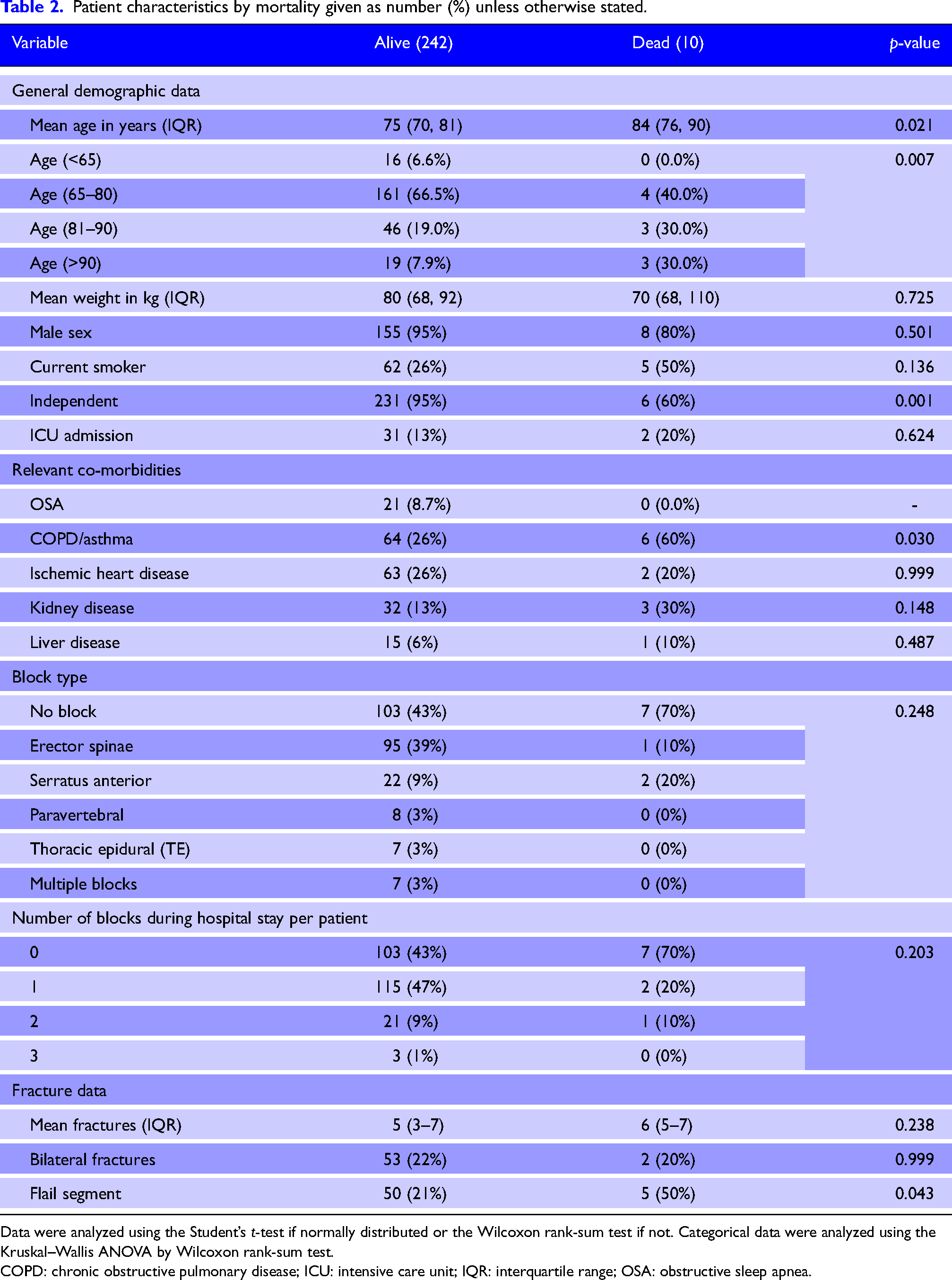
Data were analyzed using the Student’s t-test if normally distributed or the Wilcoxon rank-sum test if not. Categorical data were analyzed using the Kruskal–Wallis ANOVA by Wilcoxon rank-sum test.
COPD: chronic obstructive pulmonary disease; ICU: intensive care unit; IQR: interquartile range; OSA: obstructive sleep apnea.
A total of 24 (9.5%) patients developed pneumonia during their hospital stay. Predictors of pneumonia included past medical history of smoking (OR = 3.84; 95% CI = 1.34 to 10.96; p = 0.012) and liver disease (OR = 4.65; 95% CI = 1.20 to 18.10; p = 0.027). There was an increased odds of pneumonia with increasing age but this was not statistically significant (OR = 1.07; 95% CI = 0.999 to 1.137; p = 0.057). No other comorbidities or injuries, including number of rib fractures, were predictive of pneumonia.
The total ICU admission rate was 13.1% (n = 33). Predictors of admission to ICU included number of fractures (OR = 1.15; 95% CI = 1.01 to 1.31; p = 0.038) and the presence of bilateral fractures (OR = 4.10; 95% CI = 1.62 to 10.34; p = 0.003). A past medical history of asthma or COPD resulted in a nonsignificant increased odds of ICU admission (OR = 2.38; 95% CI = 0.98 to 5.80; p = 0.057).
Discussion
This study investigated the outcomes of patients aged over the age of 65 years admitted for conservative, nonsurgical management of rib fractures. As part of this study, 56.3% of patients received a regional anesthesia, the majority of which were ESP blocks. Of the 252 patients included in our cohort, there was a mortality rate of 4%. Furthermore, there was no correlation between the number of rib fractures and the incidence of mortality or pneumonia. These results differ significantly from previously published studies investigating outcomes of older patients managed conservatively following a rib fracture-related hospital admission. 3
Recently, there has been a large amount of literature published on the use of rib fracture fixation.6,14 Particularly in elderly patients, these studies have demonstrated significant morbidity and mortality benefits. 5 One limiting factor to these studies was potentially the regional anesthesia options available to the control group, as these studies took place prior to the widespread use of new fascial plane techniques. For this reason, future studies investigating the effect of rib fracture fixation versus regional anesthesia is unlikely to demonstrate such a profound benefit. Regardless of the benefits in favor of rib fracture fixation, this surgical technique is reasonably new and definitely not available to all patients admitted to the hospital with multiple rib fractures.
The positive results presented in our study are attributable to the initiation of a trauma pathway at the time of admission and the liberal use of regional anesthesia, particularly the utilization of newer chest wall blocks such as the ESP. This appears to have mitigated the effect of increasing numbers of rib fractures on mortality and pneumonia. Importantly, there was no significant difference in correlation in patients with regional anesthesia compared with those without regional anesthesia. We believe that this was attributable to careful patient selection for the provision of regional anesthesia techniques. Careful consideration of who needs a regional nerve block is important, as some patients with multiple rib fractures experience only mild pain. 15
The persisting correlation between number of fractures and ICU admission was likely based on admission for patient risk, rather than physiologic derangements requiring support. A key limitation of the present study was that we did not collect data on the reasons for ICU admission. Another limitation was the inability to compare the patients who received regional anesthesia with those who did not. This was due to the difference in patient populations and their associated injuries. Currently, there is reasonable efficacy data to demonstrate the effect of the various regional anesthesia techniques on pain scores and respiratory function post-rib fracture. Future randomized controlled trials need to be performed to investigate the effect of regional anesthesia on rib fracture-related morbidity and mortality. These studies should also compare regional anesthesia to both non-regional anesthesia-based management, as well as to rib fixation.
Conclusion
Management including liberal utilization of regional anesthesia for at-risk patients appears to mitigate the effect of increasing numbers of rib fractures on the incidence of mortality and pneumonia.
Declarations
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Prince Charles Hospital Human Research Ethics Committee and the Sunshine Coast Hospital and Health Service (HREC: LNR/2018/QPCH/45155).
Informed consent
This retrospective study did not require informed consent.
Trial registration
Not applicable.
Contributorship
All authors comply with the ICMJE recommendations. Leigh White: This author helped with study design, data curation, statistical analysis, writing—reviewing and editing. Brooke Riley: This author helped with study design, data curation, writing—reviewing and editing. Davina Siedel: This author helped with study design, data curation, writing—reviewing and editing. Keiran Davis: This author helped with study design, manuscript writing, reviewing, referencing, and editing. Andrew Mitchell: This author helped with study design, manuscript writing—reviewing and editing. Catherine Abi-fares: This author helped with study design, manuscript writing—reviewing and editing. Willem Basson: This author helped with study design, manuscript writing—reviewing and editing. Chris Anstey: This author helped with study design, statistical analysis, writing—reviewing and editing.
Acknowledgements
None.